-
Pneumonia
For other uses, see Pneumonia (disambiguation).
Pneumonia (nu-mo'ne-a) is an inammatory conditionof the lung
aecting primarily the microscopic air sacsknown as alveoli.[1][2]
It is usually caused by infec-tion with viruses or bacteria and
less commonly othermicroorganisms, certain drugs and other
conditions suchas autoimmune diseases.[1][3]
Typical symptoms include a cough, chest pain, fever, anddiculty
breathing.[4] Diagnostic tools include x-rays andculture of the
sputum. Vaccines to prevent certain typesof pneumonia are
available. Treatment depends on theunderlying cause. Pneumonia
presumed to be bacterial istreated with antibiotics. If the
pneumonia is severe, theaected person is generally
hospitalized.Pneumonia aects approximately 450 million
peopleglobally per year, seven percent of population, and resultsin
about 4 million deaths, mostly in developing countries.Although
pneumonia was regarded by William Osler inthe 19th century as the
captain of the men of death,[5]the advent of antibiotic therapy and
vaccines in the 20thcentury has seen improvements in survival.[6]
Neverthe-less, in developing countries, and among the very old,
thevery young, and the chronically ill, pneumonia remains aleading
cause of death.[6][7] In the terminally ill and el-derly,
especially those with other conditions, pneumoniais often the
immediate cause of death. In such cases, par-ticularly when it cuts
short the suering associated withlingering illness, pneumonia has
often been called theold mans friend.[8]
1 Signs and symptomsPeople with infectious pneumonia often have
a productivecough, fever accompanied by shaking chills, shortness
ofbreath, sharp or stabbing chest pain during deep breaths,and an
increased respiratory rate.[10] In the elderly, confu-sion may be
the most prominent sign.[10] The typical signsand symptoms in
children under ve are fever, cough, andfast or dicult
breathing.[11]
Fever is not very specic, as it occurs in many other com-mon
illnesses, may be absent in those with severe dis-ease,
malnutrition or in the elderly. In addition, a coughis frequently
absent in children less than 2 months old.[11]More severe signs and
symptomsmay include blue-tingedskin, decreased thirst, convulsions,
persistent vomiting,extremes of temperature, or a decreased level
of con-
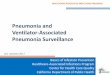
Main symptoms of infectious
PneumoniaSystemic: - High fever - Chills
Lungs: - Cough with sputum or phlegm - Shortness of breath -
Pleuritic chest pain - Hemoptysis
Skin: - Clamminess - Blueness
Central: - Headaches - Loss of appetite - Mood swings
Vascular - Low blood pressure
Heart: - High heart rate
Muscular: - Fatigue - Aches
Gastric: - Nausea - Vomiting
Joints: - Pain
Main symptoms of infectious pneumonia
sciousness.[11][12]
Bacterial and viral cases of pneumonia usually presentwith
similar symptoms.[13] Some causes are associatedwith classic, but
non-specic, clinical characteristics.Pneumonia caused by Legionella
may occur with ab-dominal pain, diarrhea, or confusion,[14] while
pneumo-nia caused by Streptococcus pneumoniae is associatedwith
rusty colored sputum,[15] and pneumonia caused byKlebsiella may
have bloody sputum often described ascurrant jelly.[9] Bloody
sputum (known as hemoptysis)may also occur with tuberculosis,
Gram-negative pneu-monia, and lung abscesses as well as more
commonly withacute bronchitis.[12] Mycoplasma pneumonia may occurin
association with swelling of the lymph nodes in theneck, joint
pain, or a middle ear infection.[12] Viral pneu-monia presents more
commonly with wheezing than doesbacterial pneumonia.[13] Pneumonia
was historically di-vided into typical and atypical based on the
belief thatthe presentation predicted the underlying cause.[16]
Evi-dence; however, has not supported this distinction, thus itis
no longer emphasized.[16]
2 CausePneumonia is due to infections caused primarily
bybacteria or viruses and less commonly by fungi andparasites.
Although there are more than 100 strains of
1
-
2 2 CAUSE
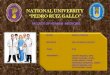
The bacterium Streptococcus pneumoniae, a common cause
ofpneumonia, imaged by an electron microscope.
infectious agents identied, only a few are responsiblefor the
majority of the cases. Mixed infections with bothviruses and
bacteria may occur in up to 45% of infectionsin children and 15% of
infections in adults.[6] A causativeagent may not be isolated in
approximately half of casesdespite careful testing.[8]
The term pneumonia is sometimes more broadly appliedto any
condition resulting in inammation of the lungs(caused for example
by autoimmune diseases, chemicalburns or drug reactions); however,
this inammation ismore accurately referred to as
pneumonitis.[17][18]
Conditions and risk factors that predispose to pneu-monia
include smoking, immunodeciency, alcoholism,chronic obstructive
pulmonary disease, chronic kidneydisease, and liver disease.[12]
The use of acid-suppressingmedicationssuch as proton-pump
inhibitors or H2blockersis associated with an increased risk
ofpneumonia.[19] The risk is also increased in old age.[12]
2.1 Bacteria
Main article: Bacterial pneumonia
Bacteria are the most common cause of community-acquired
pneumonia (CAP), with Streptococcus pneu-moniae isolated in nearly
50% of cases.[20][21] Othercommonly isolated bacteria include
Haemophilus in-uenzae in 20%, Chlamydophila pneumoniae in 13%,and
Mycoplasma pneumoniae in 3% of cases;[20]Staphylococcus aureus;
Moraxella catarrhalis; Legionellapneumophila and Gram-negative
bacilli.[8] A number ofdrug-resistant versions of the above
infections are becom-ing more common, including drug-resistant
Streptococcuspneumoniae (DRSP) and methicillin-resistant
Staphylo-coccus aureus (MRSA).[12]
The spreading of organisms is facilitated when risk fac-tors are
present.[8] Alcoholism is associated with Strep-tococcus
pneumoniae, anaerobic organisms, and My-cobacterium tuberculosis;
smoking facilitates the eects
of Streptococcus pneumoniae, Haemophilus inuenzae,Moraxella
catarrhalis, and Legionella pneumophila. Ex-posure to birds is
associated with Chlamydia psittaci;farm animals with Coxiella
burnetti; aspiration of stom-ach contents with anaerobic organisms;
and cystic bro-sis with Pseudomonas aeruginosa and Staphylococcus
au-reus.[8] Streptococcus pneumoniae is more common in
thewinter,[8] and should be suspected in persons aspirating alarge
amount anaerobic organisms.[12]
2.2 Viruses
Main article: Viral pneumonia
In adults, viruses account for approximately a third[6]and in
children for about 15% of pneumonia cases.[22]Commonly implicated
agents include rhinoviruses,coronaviruses, inuenza virus,
respiratory syncytialvirus (RSV), adenovirus, and
parainuenza.[6][23]Herpes simplex virus rarely causes pneumonia,
exceptin groups such as: newborns, persons with cancer,transplant
recipients, and people with signicantburns.[24] People following
organ transplantation orthose otherwise-immunocompromised present
high ratesof cytomegalovirus pneumonia.[22][24] Those with
viralinfections may be secondarily infected with the
bacteriaStreptococcus pneumoniae, Staphylococcus aureus,
orHaemophilus inuenzae, particularly when other healthproblems are
present.[12][22] Dierent viruses predom-inate at dierent periods of
the year; during inuenzaseason, for example, inuenza may account
for overhalf of all viral cases.[22] Outbreaks of other virusesalso
occasionally occur, including hantaviruses andcoronavirus.[22]
2.3 Fungi
Main article: Fungal pneumonia
Fungal pneumonia is uncommon, but occurs morecommonly in
individuals with weakened immune sys-tems due to AIDS,
immunosuppressive drugs, or othermedical problems.[8][25] It is
most often caused byHistoplasma capsulatum, blastomyces,
Cryptococcus ne-oformans, Pneumocystis jiroveci, and Coccidioides
immi-tis. Histoplasmosis is most common in the MississippiRiver
basin, and coccidioidomycosis is most common inthe Southwestern
United States.[8] The number of caseshave been increasing in the
later half of the 20th centurydue to increasing travel and rates of
immunosuppressionin the population.[25]
-
3.2 Bacterial 3
2.4 Parasites
Main article: Parasitic pneumonia
A variety of parasites can aect the lungs, includingToxoplasma
gondii, Strongyloides stercoralis,Ascaris lum-bricoides, and
Plasmodium malariae.[26] These organ-isms typically enter the body
through direct contact withthe skin, ingestion, or via an insect
vector.[26] Exceptfor Paragonimus westermani, most parasites do not
af-fect specically the lungs but involve the lungs sec-ondarily to
other sites.[26] Some parasites, in partic-ular those belonging to
the Ascaris and Strongyloidesgenera, stimulate a strong
eosinophilic reaction, whichmay result in eosinophilic
pneumonia.[26] In other infec-tions, such as malaria, lung
involvement is due primar-ily to cytokine-induced systemic
inammation.[26] In thedeveloped world these infections are most
common inpeople returning from travel or in immigrants.[26]
Aroundthe world, these infections are most common in
theimmunodecient.[27]
2.5 Idiopathic
Main article: Idiopathic interstitial pneumonia
Idiopathic interstitial pneumonia or noninfectiouspneumonia[28]
are a class of diuse lung diseases. Theyinclude diuse alveolar
damage, organizing pneumonia,nonspecic interstitial pneumonia,
lymphocytic inter-stitial pneumonia, desquamative interstitial
pneumonia,respiratory bronchiolitis interstitial lung disease,
andusual interstitial pneumonia.[29]
3 MechanismsPneumonia frequently starts as an upper respiratory
tractinfection that moves into the lower respiratory tract.[30]
3.1 Viral
Viruses may reach the lung by a number of dierentroutes.
Respiratory syncytial virus is typically contractedwhen people
touch contaminated objects and then theytouch their eyes or
nose.[22] Other viral infections oc-cur when contaminated airborne
droplets are inhaledthrough the mouth or nose.[12] Once in the
upper air-way, the viruses may make their way in the lungs,
wherethey invade the cells lining the airways, alveoli, or
lungparenchyma.[22] Some viruses such as measles and her-pes
simplex may reach the lungs via the blood.[31] Theinvasion of the
lungs may lead to varying degrees of celldeath.[22] When the immune
system responds to the in-fection, even more lung damage may
occur.[22] Primarily
Pneumonia lls the lungs alveoli with uid, hindering
oxygena-tion. The alveolus on the left is normal, whereas the one
on theright is full of uid from pneumonia.
white blood cells, mainly mononuclear cells, generate
theinammation.[31] As well as damaging the lungs, manyviruses
simultaneously aect other organs and thus dis-rupt other body
functions. Viruses also make the bodymore susceptible to bacterial
infections; in this way, bac-terial pneumonia can arise as a
co-morbid condition.[23]
3.2 Bacterial
Most bacteria enter the lungs via small aspirations of
or-ganisms residing in the throat or nose.[12] Half of nor-mal
people have these small aspirations during sleep.[16]While the
throat always contains bacteria, potentially in-fectious ones
reside there only at certain times and un-der certain
conditions.[16] A minority of types of bac-teria such as
Mycobacterium tuberculosis and Legionellapneumophila reach the
lungs via contaminated airbornedroplets.[12] Bacteria can spread
also via the blood.[13]Once in the lungs, bacteria may invade the
spaces be-tween cells and between alveoli, where the macrophagesand
neutrophils (defensive white blood cells) attempt toinactivate the
bacteria.[32] The neutrophils also releasecytokines, causing a
general activation of the immunesystem.[33] This leads to the
fever, chills, and fatigue com-mon in bacterial pneumonia.[33] The
neutrophils, bacte-ria, and uid from surrounding blood vessels ll
the alve-oli, resulting in the consolidation seen on chest
X-ray.[34]
-
4 4 DIAGNOSIS
4 DiagnosisPneumonia is typically diagnosed based on a
combinationof physical signs and a chest X-ray.[35] However, the
un-derlying cause can be dicult to conrm, as there is nodenitive
test able to distinguish between bacterial andnon-bacterial
origin.[6][35] The World Health Organiza-tion has dened pneumonia
in children clinically basedon either a cough or diculty breathing
and a rapid res-piratory rate, chest indrawing, or a decreased
level ofconsciousness.[36] A rapid respiratory rate is dened
asgreater than 60 breaths per minute in children under 2months old,
50 breaths per minute in children 2 monthsto 1 year old, or greater
than 40 breaths per minute inchildren 1 to 5 years old.[36] In
children, increased respi-ratory rate and lower chest indrawing are
more sensitivethan hearing chest crackles with a
stethoscope.[11]
In general, in adults, investigations are not needed in
mildcases:[37] There is a very low risk of pneumonia if allvital
signs and auscultation are normal.[38] In persons re-quiring
hospitalization, pulse oximetry, chest radiogra-phy and blood
testsincluding a complete blood count,serum electrolytes,
C-reactive protein level, and possiblyliver function testsare
recommended.[37] The diagnosisof inuenza-like illness can be made
based on the signsand symptoms; however, conrmation of an inuenza
in-fection requires testing.[39] Thus, treatment is frequentlybased
on the presence of inuenza in the community or arapid inuenza
test.[39]
4.1 Physical exam
Physical examination may sometimes reveal low bloodpressure,
high heart rate, or low oxygen saturation.[12]The respiratory rate
may be faster than normal, and thismay occur a day or two before
other signs.[12][16] Ex-amination of the chest may be normal, but
it may showdecreased chest expansion on the aected side.
Harshbreath sounds from the larger airways that are
transmittedthrough the inamed lung are termed bronchial breath-ing
and are heard on auscultation with a stethoscope.[12]Crackles
(rales) may be heard over the aected area dur-ing inspiration.[12]
Percussion may be dulled over the af-fected lung, and increased,
rather than decreased, vocalresonance distinguishes pneumonia from
a pleural eu-sion.[10]
4.2 Imaging
A chest radiograph is frequently used in diagnosis.[11]In people
with mild disease, imaging is needed only inthose with potential
complications, those not having im-proved with treatment, or those
in which the cause isuncertain.[11][37] If a person is suciently
sick to requirehospitalization, a chest radiograph is
recommended.[37]Findings do not always match the severity of
disease and
CT of the chest demonstrating right-side pneumonia (left side
ofthe image).
do not reliably separate between bacterial infection andviral
infection.[11]
X-ray presentations of pneumonia may be classied aslobar
pneumonia, bronchopneumonia (also known as lob-ular pneumonia), and
interstitial pneumonia.[40] Bac-terial, community-acquired
pneumonia classically showlung consolidation of one lung segmental
lobe, which isknown as lobar pneumonia.[20] However, ndings
mayvary, and other patterns are common in other types
ofpneumonia.[20] Aspiration pneumonia may present withbilateral
opacities primarily in the bases of the lungsand on the right
side.[20] Radiographs of viral pneumoniamay appear normal, appear
hyper-inated, have bilateralpatchy areas, or present similar to
bacterial pneumoniawith lobar consolidation.[20] Radiologic ndings
may notbe present in the early stages of the disease, especiallyin
the presence of dehydration, or may be dicult to beinterpreted in
the obese or those with a history of lungdisease.[12] A CT scan can
give additional information inindeterminate cases.[20]
4.3 Microbiology
In patients managed in the community, determining thecausative
agent is not cost-eective and typically does notalter
management.[11] For people that do not respond totreatment, sputum
culture should be considered, and cul-ture forMycobacterium
tuberculosis should be carried outin persons with a chronic
productive cough.[37] Testingfor other specic organisms may be
recommended dur-ing outbreaks, for public health reasons.[37] In
those hos-pitalized for severe disease, both sputum and blood
cul-tures are recommended,[37] as well as testing the urine
forantigens to Legionella and Streptococcus.[41] Viral infec-tions
can be conrmed via detection of either the virusor its antigens
with culture or polymerase chain reaction(PCR), among other
techniques.[6] The causative agent isdetermined in only 15% of
cases with routine microbio-logical tests.[10]
-
5.2 Other 5
4.4 Classication
Main article: Classication of pneumonia
Pneumonitis refers to lung inammation; pneumo-nia refers to
pneumonitis, usually due to infectionbut sometimes non-infectious,
that has the additionalfeature of pulmonary consolidation.[42]
Pneumonia ismost commonly classied by where or how it wasacquired:
community-acquired, aspiration, healthcare-associated,
hospital-acquired, and ventilator-associatedpneumonia.[20] It may
also be classied by the area oflung aected: lobar pneumonia,
bronchial pneumoniaand acute interstitial pneumonia;[20] or by the
causativeorganism.[43] Pneumonia in children may additionally
beclassied based on signs and symptoms as non-severe, se-vere, or
very severe.[44]
4.5 Dierential diagnosis
Several diseases can present with similar signs and symp-toms to
pneumonia, such as: chronic obstructive pul-monary disease (COPD),
asthma, pulmonary edema,bronchiectasis, lung cancer, and pulmonary
emboli.[10]Unlike pneumonia, asthma and COPD typically presentwith
wheezing, pulmonary edema presents with an abnor-mal
electrocardiogram, cancer and bronchiectasis presentwith a cough of
longer duration, and pulmonary embolipresents with acute onset
sharp chest pain and shortnessof breath.[10]
5 PreventionPrevention includes vaccination, environmental
measuresand appropriate treatment of other health problems.[11]
Itis believed that, if appropriate preventive measures
wereinstituted globally, mortality among children could be re-duced
by 400,000; and, if proper treatment were univer-sally available,
childhood deaths could be decreased byanother 600,000.[13]
5.1 Vaccination
Vaccination prevents against certain bacterial and vi-ral
pneumonias both in children and adults. Inuenzavaccines are
modestly eective against inuenza A andB.[6][45] The Center for
Disease Control and Prevention(CDC) recommends yearly vaccination
for every person6 months and older.[46] Immunizing health care
work-ers decreases the risk of viral pneumonia among
theirpatients.[41] When inuenza outbreaks occur, medica-tions such
as amantadine or rimantadine may help pre-vent the condition.[47]
It is unknown whether zanamiviror oseltamivir is eective due to the
fact that the com-
pany that manufactures oseltamivir has refused to releasethe
trial data for independent analysis.[48]
Vaccinations against Haemophilus inuenzae andStreptococcus
pneumoniae have good evidence to supporttheir use.[30] Vaccinating
children against Streptococcuspneumoniae has led to a decreased
incidence of these in-fections in adults, because many adults
acquire infectionsfrom children. A Streptococcus pneumoniae vaccine
isavailable for adults, and has been found to decrease therisk of
invasive pneumococcal disease.[49] Other vaccinesfor which there to
support for a protective eect againstpneumonia include pertussis,
varicella, and measles.[50]
5.2 OtherSmoking cessation[37] and reducing indoor air
pollution,such as that from cooking indoors with wood or dung,are
both recommended.[11][13] Smoking appears to be thesingle biggest
risk factor for pneumococcal pneumoniain otherwise-healthy
adults.[41] Hand hygiene and cough-ing into ones sleeve may also be
eective preventativemeasures.[50] Wearing surgical masks by the
sickmay alsoprevent illness.[41]
Appropriately treating underlying illnesses (such asHIV/AIDS,
diabetes mellitus, and malnutrition) can de-crease the risk of
pneumonia.[13][50][51] In children lessthan 6 months of age,
exclusive breast feeding reducesboth the risk and severity of
disease.[13] In those withHIV/AIDS and a CD4 count of less than 200
cells/uLthe antibiotic trimethoprim/sulfamethoxazole decreasesthe
risk of Pneumocystis pneumonia[52] and may also beuseful for
prevention in those that are immunocomprisedbut do not have
HIV.[53]
Testing pregnant women for Group B Streptococcusand Chlamydia
trachomatis, and administering antibiotictreatment, if needed,
reduces rates of pneumonia ininfants;[54][55] preventive measures
for HIV transmissionfrom mother to child may also be ecient.[56]
Suctioningthe mouth and throat of infants with
meconium-stainedamniotic uid has not been found to reduce the rate
ofaspiration pneumonia and may cause potential harm,[57]thus this
practice is not recommended in the majority ofsituations.[57] In
the frail elderly good oral health caremaylower the risk of
aspiration pneumonia.[58]
6 ManagementOral antibiotics, rest, simple analgesics, and uids
usu-ally suce for complete resolution.[37] However, thosewith other
medical conditions, the elderly, or thosewith signicant trouble
breathing may require more ad-vanced care. If the symptoms worsen,
the pneumoniadoes not improve with home treatment, or
complica-tions occur, hospitalization may be required.[37]
World-wide, approximately 713% of cases in children result
-
6 7 PROGNOSIS
in hospitalization,[11] whereas in the developed world be-tween
22 and 42% of adults with community-acquiredpneumonia are
admitted.[37] The CURB-65 score is use-ful for determining the need
for admission in adults.[37]If the score is 0 or 1, people can
typically be managed athome; if it is 2, a short hospital stay or
close follow-up isneeded; if it is 35, hospitalization is
recommended.[37]In children those with respiratory distress or
oxygen sat-urations of less than 90% should be hospitalized.[59]
Theutility of chest physiotherapy in pneumonia has not yetbeen
determined.[60] Non-invasive ventilation may bebenecial in those
admitted to the intensive care unit.[61]Over-the-counter cough
medicine has not been found tobe eective[62] nor has the use of
zinc in children.[63]There is insucient evidence for
mucolytics.[62]
6.1 BacterialAntibiotics improve outcomes in those with
bacterialpneumonia.[64] Antibiotic choice depends initially on
thecharacteristics of the person aected, such as age, un-derlying
health, and the location the infection was ac-quired. In the UK,
empiric treatment with amoxicillinis recommended as the rst line
for community-acquired pneumonia, with doxycycline or
clarithromycinas alternatives.[37] In NorthAmerica, where the
atypicalforms of community-acquired pneumonia are more com-mon,
macrolides (such as azithromycin or erythromycin),and doxycycline
have displaced amoxicillin as rst-lineoutpatient treatment in
adults.[21][65] In children withmild or moderate symptoms,
amoxicillin remains therst line.[59] The use of uoroquinolones in
uncom-plicated cases is discouraged due to concerns aboutside-eects
and generating resistance in light of therebeing no greater
clinical benet.[21][66] The durationof treatment has traditionally
been seven to ten days,but increasing evidence suggests that
shorter courses(three to ve days) are similarly eective.[67]
Recom-mended for hospital-acquired pneumonia include third-and
fourth-generation cephalosporins, carbapenems,uoroquinolones,
aminoglycosides, and vancomycin.[68]These antibiotics are often
given intravenously and usedin combination.[68] In those treated in
hospital, more than90% improve with the initial
antibiotics.[16]
6.2 ViralNeuraminidase inhibitors may be used to treat
viralpneumonia caused by inuenza viruses (inuenza A andinuenza
B).[6] No specic antiviral medications are rec-ommended for other
types of community acquired vi-ral pneumonias including SARS
coronavirus, adenovirus,hantavirus, and parainuenza virus.[6]
Inuenza A maybe treated with rimantadine or amantadine, while
in-uenza A or Bmay be treated with oseltamivir, zanamiviror
peramivir.[6] These are of most benet if they arestartedwithin 48
hours of the onset of symptoms.[6] Many
strains of H5N1 inuenza A, also known as avian in-uenza or bird
u, have shown resistance to rimanta-dine and amantadine.[6] The use
of antibiotics in viralpneumonia is recommended by some experts, as
it is im-possible to rule out a complicating bacterial
infection.[6]The British Thoracic Society recommends that
antibi-otics be withheld in those with mild disease.[6] The useof
corticosteroids is controversial.[6]
6.3 AspirationIn general, aspiration pneumonitis is treated
conserva-tively with antibiotics indicated only for aspiration
pneu-monia.[69] The choice of antibiotic will depend on sev-eral
factors, including the suspected causative organismand whether
pneumonia was acquired in the commu-nity or developed in a hospital
setting. Common op-tions include clindamycin, a combination of a
beta-lactamantibiotic and metronidazole, or an
aminoglycoside.[70]Corticosteroids are sometimes used in aspiration
pneu-monia, but there is limited evidence to support
theireectiveness.[69]
7 PrognosisWith treatment, most types of bacterial pneumonia
willstabilize in 36 days.[71] It often takes a few weeks be-fore
most symptoms resolve.[71] X-ray nding typicallyclear within four
weeks and mortality is low (less than1%).[12][72] In the elderly or
people with other lung prob-lems, recovery may take more than 12
weeks. In per-sons requiring hospitalization, mortality may be as
highas 10%, and in those requiring intensive care it may
reach3050%.[12] Pneumonia is the most common hospital-acquired
infection that causes death.[16] Before the adventof antibiotics,
mortality was typically 30% in those thatwere hospitalized.[8]
Complications may occur in particular in the elderlyand those
with underlying health problems.[72] Thismay include, among others:
empyema, lung abscess,bronchiolitis obliterans, acute respiratory
distress syn-drome, sepsis, and worsening of underlying
healthproblems.[72]
7.1 Clinical prediction rulesClinical prediction rules have been
developed to more ob-jectively predict outcomes of pneumonia.[16]
These rulesare often used in deciding whether or not to
hospitalizethe person.[16]
Pneumonia severity index (or PSI Score)[16]
CURB-65 score, which takes into account the sever-ity of
symptoms, any underlying diseases, and
-
7age[73]
7.2 Pleural eusion, empyema, and ab-scess
A pleural eusion: as seen on chest X-ray. The A arrow
indicatesuid layering in the right chest. The B arrow indicates the
widthof the right lung. The volume of the lung is reduced because
ofthe collection of uid around the lung.
In pneumonia, a collection of uid may form in the spacethat
surrounds the lung.[74] Occasionally, microorgan-isms will infect
this uid, causing an empyema.[74] Todistinguish an empyema from the
more common simpleparapneumonic eusion, the uid may be collected
witha needle (thoracentesis), and examined.[74] If this
showsevidence of empyema, complete drainage of the uid isnecessary,
often requiring a drainage catheter.[74] In se-vere cases of
empyema, surgery may be needed.[74] If theinfected uid is not
drained, the infection may persist,because antibiotics do not
penetrate well into the pleuralcavity. If the uid is sterile, it
must be drained only if itis causing symptoms or remains
unresolved.[74]
In rare circumstances, bacteria in the lung will forma pocket of
infected uid called a lung abscess.[74]Lung abscesses can usually
be seen with a chest X-ray but frequently require a chest CT scan
to conrmthe diagnosis.[74] Abscesses typically occur in
aspirationpneumonia, and often contain several types of
bacteria.Long-term antibiotics are usually adequate to treat a
lungabscess, but sometimes the abscess must be drained by asurgeon
or radiologist.[74]
7.3 Respiratory and circulatory failurePneumonia can cause
respiratory failure by triggeringacute respiratory distress
syndrome (ARDS), which re-sults from a combination of infection and
inammatoryresponse. The lungs quickly ll with uid and becomesti.
This stiness, combined with severe diculties ex-tracting oxygen due
to the alveolar uid, may require long
periods of mechanical ventilation for survival.[22]
Sepsis is a potential complication of pneumonia butoccurs
usually in people with poor immunity orhyposplenism. The organisms
most commonly involvedare Streptococcus pneumoniae, Haemophilus
inuenzae,and Klebsiella pneumoniae. Other causes of the symp-toms
should be considered such as a myocardial infarctionor a pulmonary
embolism.[75]
8 EpidemiologyMain article: Epidemiology of pneumoniaPneumonia
is a common illness aecting approximately
Age-standardized death rate: lower respiratory tract
infectionsper 100,000 inhabitants in 2004.[76]
450 million people a year and occurring in all parts ofthe
world.[6] It is a major cause of death among all agegroups
resulting in 4 million deaths (7% of the worldstotal death)
yearly.[6][64] Rates are greatest in childrenless than ve, and
adults older than 75 years.[6] It occursabout ve times more
frequently in the developing worldthan in the developed world.[6]
Viral pneumonia accountsfor about 200 million cases.[6] In the
United States, as of2009, pneumonia is the 8th leading cause of
death.[12]
8.1 Children
In 2008, pneumonia occurred in approximately 156 mil-lion
children (151 million in the developing world and5 million in the
developed world).[6] In 2010, it resultedin 1.3 million deaths, or
18% of all deaths in those un-der ve years, of which 95% occurred
in the developingworld.[6][11][77] Countries with the greatest
burden of dis-ease include India (43 million), China (21 million)
andPakistan (10 million).[78] It is the leading cause of deathamong
children in low income countries.[6][64] Many ofthese deaths occur
in the newborn period. The WorldHealth Organization estimates that
one in three newborninfant deaths is due to pneumonia.[79]
Approximately halfof these deaths can be prevented, as they are
caused by thebacteria for which an eective vaccine is
available.[80] In2011, pneumonia was the most common reason for
ad-mission to the hospital after an emergency departmentvisit in
the U.S. for infants and children.[81]
-
8 10 SOCIETY AND CULTURE
9 History
WPA poster, 1936/1937
Pneumonia has been a common disease throughouthuman history.[82]
The symptoms were described byHippocrates (c. 460 BC 370 BC):[82]
Peripneumonia,and pleuritic aections, are to be thus observed: If
thefever be acute, and if there be pains on either side, or inboth,
and if expiration be if cough be present, and thesputa expectorated
be of a blond or livid color, or like-wise thin, frothy, and orid,
or having any other char-acter dierent from the common... When
pneumoniais at its height, the case is beyond remedy if he is
notpurged, and it is bad if he has dyspnoea, and urine thatis thin
and acrid, and if sweats come out about the neckand head, for such
sweats are bad, as proceeding fromthe suocation, rales, and the
violence of the diseasewhich is obtaining the upper hand.[83]
However, Hip-pocrates referred to pneumonia as a disease named
bythe ancients. He also reported the results of surgicaldrainage of
empyemas. Maimonides (11351204 AD)observed: The basic symptoms that
occur in pneumo-nia and that are never lacking are as follows:
acute fever,sticking pleuritic pain in the side, short rapid
breaths, ser-rated pulse and cough.[84] This clinical description
isquite similar to those found in modern textbooks, andit reected
the extent of medical knowledge through theMiddle Ages into the
19th century.Edwin Klebs was the rst to observe bacteria in the
air-
ways of persons having died of pneumonia in 1875.[85]Initial
work identifying the two common bacterialcauses, Streptococcus
pneumoniae and Klebsiella pneumo-niae, was performed by Carl
Friedlnder[86] and AlbertFrnkel[87] in 1882 and 1884, respectively.
Friedlndersinitial work introduced the Gram stain, a
fundamentallaboratory test still used today to identify and
categorizebacteria. Christian Gram's paper describing the
proce-dure in 1884 helped to dierentiate the two bacteria,
andshowed that pneumonia could be caused bymore than
onemicroorganism.[88]
Sir William Osler, known as the father of modernmedicine,
appreciated the death and disability causedby pneumonia, describing
it as the captain of the menof death in 1918, as it had overtaken
tuberculosis as oneof the leading causes of death in this time.
This phrasewas originally coined by John Bunyan in reference
toconsumption (tuberculosis).[89][90] Osler also describedpneumonia
as the old mans friend as death was oftenquick and painless when
there were many slower morepainful ways to die.[8]
Several developments in the 1900s improved the out-come for
those with pneumonia. With the advent ofpenicillin and other
antibiotics, modern surgical tech-niques, and intensive care in the
20th century, mortal-ity from pneumonia, had approached 30%,
dropped pre-cipitously in the developed world. Vaccination of
infantsagainst Haemophilus inuenzae type B began in 1988 andled to
a dramatic decline in cases shortly thereafter.[91]Vaccination
against Streptococcus pneumoniae in adultsbegan in 1977, and in
children in 2000, resulting in a sim-ilar decline.[92]
10 Society and cultureSee also: List of notable pneumonia
cases
10.1 Awareness
Due to the high burden of disease in developing countriesand a
relatively low awareness of the disease in devel-oped countries,
the global health community has declared12 November as World
Pneumonia Day, a day for con-cerned citizens and policy makers to
take action againstthe disease.[93]
10.2 Costs
The global economic cost of community-acquired pneu-monia has
been estimated at $17 billion annually.[12]Other estimates are
considerably higher. In 2012 theestimated aggregate costs of
treating pneumonia in theUnited States were $20 billion;[94] the
median cost
-
9of a single pneumonia-related hospitalization is
over$15,000.[95] According to data released by the Centers
forMedicare and Medicaid Services, average 2012 hospitalcharges for
inpatient treatment of uncomplicated pneu-monia in the U.S. were
$24,549 and ranged as high as$124,000. The average cost of an
emergency room con-sult for pneumonia was $943 and the average cost
formedication was $66.[96] Aggregate annual costs of treat-ing
pneumonia in Europe have been estimated at 10billion.[97]
11 References[1] McLuckie, A., ed. (2009). Respiratory disease
and its
management. New York: Springer. p. 51. ISBN
978-1-84882-094-4.
[2] Leach, Richard E. (2009). Acute and Critical CareMedicine at
a Glance (2nd ed.). Wiley-Blackwell. ISBN1-4051-6139-6. Retrieved
2011-04-21.
[3] Jerey C. Pommerville (2010). Alcamos Fundamentalsof
Microbiology (9th ed.). Sudbury MA: Jones & Bartlett.p. 323.
ISBN 0-7637-6258-X.
[4] Ashby, Bonnie; Turkington, Carol (2007). The encyclo-pedia
of infectious diseases (3rd ed.). New York: Facts onFile. p. 242.
ISBN 0-8160-6397-4. Retrieved 2011-04-21.
[5] Osler, William (1901). Principles and Practice ofMedicine,
4th Edition. New York: D. Appleton and Com-pany. p. 108.
[6] Ruuskanen, O; Lahti, E; Jennings, LC; Murdoch,
DR(2011-04-09). Viral pneumonia. Lancet 377 (9773):126475.
doi:10.1016/S0140-6736(10)61459-6. PMID21435708.
[7] George, Ronald B. (2005). Chest medicine : essentials
ofpulmonary and critical care medicine (5th ed.). Philadel-phia,
PA: Lippincott Williams & Wilkins. p. 353.
ISBN9780781752732.
[8] Eddy, Orin (Dec 2005). Community-Acquired Pneumo-nia: From
Common Pathogens To Emerging Resistance.Emergency Medicine Practice
7 (12).
[9] Tintinalli, Judith E. (2010). Emergency Medicine: A
Com-prehensive Study Guide (Emergency Medicine (Tintinalli)).New
York: McGraw-Hill Companies. p. 480. ISBN 0-07-148480-9.
[10] Hoare Z; Lim WS (2006). Pneumonia: update on diag-nosis
andmanagement (PDF). BMJ 332 (7549):
10779.doi:10.1136/bmj.332.7549.1077. PMC 1458569. PMID16675815.
[11] Singh, V; Aneja, S (March 2011). Pneumonia man-agement in
the developing world. Paediatric respiratoryreviews 12 (1): 529.
doi:10.1016/j.prrv.2010.09.011.PMID 21172676.
[12] Nair, GB; Niederman, MS (November 2011).Community-acquired
pneumonia: an unnishedbattle. The Medical clinics of North America
95 (6):114361. doi:10.1016/j.mcna.2011.08.007. PMID22032432.
[13] Pneumonia (Fact sheet N331)". World Health Organi-zation.
August 2012.
[14] Darby, J; Buising, K (October 2008). Could it be
Le-gionella?". Australian family physician 37 (10): 8125.PMID
19002299.
[15] Ortqvist, A; Hedlund, J; Kalin, M (December
2005).Streptococcus pneumoniae: epidemiology, risk factors,and
clinical features. Seminars in respiratory and criti-cal care
medicine 26 (6): 56374. doi:10.1055/s-2005-925523. PMID
16388428.
[16] Murray and Nadel (2010). Chapter 32.
[17] Lowe, J. F.; Stevens, Alan (2000). Pathology (2nd ed.).St.
Louis: Mosby. p. 197. ISBN 0-7234-3200-7.
[18] Snydman, editors, Raleigh A. Bowden, Per Ljung-man, David
R. (2010). Transplant infections (3rded.). Philadelphia: Wolters
Kluwer Health/LippincottWilliams & Wilkins. p. 187. ISBN
978-1-58255-820-2.
[19] Eom, CS; Jeon, CY; Lim, JW; Cho, EG; Park, SM; Lee,KS (22
February 2011). Use of acid-suppressive drugsand risk of pneumonia:
a systematic review and meta-analysis. CMAJ : Canadian Medical
Association jour-nal = journal de l'Association medicale canadienne
183(3): 3109. doi:10.1503/cmaj.092129. PMC 3042441.PMID
21173070.
[20] Sharma, S; Maycher, B; Eschun, G (May 2007). Ra-diological
imaging in pneumonia: recent innovations.Current Opinion in
Pulmonary Medicine 13 (3): 15969.doi:10.1097/MCP.0b013e3280f3b4.
PMID 17414122.
[21] Anevlavis S; Bouros D (February 2010). Community ac-quired
bacterial pneumonia. Expert Opin Pharmacother11 (3): 36174.
doi:10.1517/14656560903508770.PMID 20085502.
[22] Murray and Nadel (2010). Chapter 31.
[23] Figueiredo LT (September 2009). Viral pneumo-nia:
epidemiological, clinical, pathophysiological, andtherapeutic
aspects. J Bras Pneumol 35 (9): 899906.
doi:10.1590/S1806-37132009000900012. PMID19820817.
[24] Behera, D. (2010). Textbook of pulmonary medicine (2nded.).
New Delhi: Jaypee Brothers Medical Pub. pp. 391394. ISBN
8184487495.
[25] Maskell, Nick; Millar, Ann (2009). Oxford desk refer-ence.
Oxford: Oxford University Press. p. 196. ISBN9780199239122.
[26] Murray and Nadel (2010). Chapter 37.
-
10 11 REFERENCES
[27] Vijayan, VK (May 2009). Parasitic lung infections.Current
Opinion in Pulmonary Medicine 15 (3): 27482.
doi:10.1097/MCP.0b013e328326f3f8. PMID19276810.
[28] ed. in chief Richard K. Root. Eds. Francis Waldvogel(1999).
Clinical infectious diseases : a practical approach.New York, NY
[u.a.]: Oxford Univ. Press. p. 833. ISBN978-0-19-508103-9.
[29] Volume editors, Ulrich Costabel (2007). Diuseparenchymal
lung disease : ... 47 tables ([Online-Ausg.]ed.). Basel: Karger. p.
4. ISBN 978-3-8055-8153-0.
[30] Ranganathan, SC; Sonnappa, S (February 2009).Pneumonia and
other respiratory infections. Pe-diatric clinics of North America
56 (1): 13556, xi.doi:10.1016/j.pcl.2008.10.005. PMID 19135585.
[31] editors, Gary R. Fleisher, Stephen Ludwig ; associate
edi-tors, Richard G. Bachur [et at.] (2010). Textbook of pedi-atric
emergency medicine (6th ed.). Philadelphia:
WoltersKluwer/Lippincott Williams & Wilkins Health. p. 914.ISBN
1605471593.
[32] Hammer, edited by Stephen J. McPhee, Gary D.
(2010).Pathophysiology of disease : an introduction to
clinicalmedicine (6th ed.). New York: McGraw-Hill Medical.pp.
Chapter 4. ISBN 0071621679.
[33] Fein, Alan (2006). Diagnosis and management of pneu-monia
and other respiratory infections (2nd ed.). Caddo,OK: Professional
Communications. pp. 2829. ISBN1884735630.
[34] Kumar, Vinay (2010). Robbins and Cotran pathologicbasis of
disease. (8th ed.). Philadelphia, PA: Saun-ders/Elsevier. pp.
Chapter 15. ISBN 1416031219.
[35] Lynch, T; Bialy, L; Kellner, JD; Osmond, MH;Klassen, TP;
Durec, T; Leicht, R; Johnson, DW(2010-08-06). Huicho, Luis, ed. A
systematic re-view on the diagnosis of pediatric bacterial
pneumo-nia: when gold is bronze. PLoS ONE 5 (8):
e11989.doi:10.1371/journal.pone.0011989. PMC 2917358.PMID
20700510.
[36] Ezzati, edited by Majid; Lopez, Alan D.; Rodgers, An-thony;
Murray, Christopher J.L. (2004). Comparativequantication of health
risks. Genve: Organisation mon-diale de la sant. p. 70. ISBN
978-92-4-158031-1.
[37] Lim,WS; Baudouin, SV; George, RC; Hill, AT; Jamieson,C; Le
Jeune, I; Macfarlane, JT; Read, RC; Roberts,HJ; Levy, ML; Wani, M;
Woodhead, MA; Pneumo-nia Guidelines Committee of the BTS Standards
ofCare, Committee (October 2009). BTS guidelines forthe management
of community acquired pneumonia inadults: update 2009. Thorax 64
(Suppl 3): iii155.doi:10.1136/thx.2009.121434. PMID 19783532.
[38] Saldas, F; Mndez, JI; Ramrez, D; Daz, O (April
2007)."[Predictive value of history and physical examinationfor the
diagnosis of community-acquired pneumonia inadults: a literature
review]". Revista medica de Chile 135(4): 51728. PMID 17554463.
[39] Call, SA; Vollenweider, MA; Hornung, CA; Simel,
DL;McKinney, WP (2005-02-23). Does this patient have in-uenza?".
JAMA: the Journal of the AmericanMedical As-sociation 293 (8):
98797. doi:10.1001/jama.293.8.987.PMID 15728170.
[40] Helms, editors, William E. Brant, Clyde A.
(2012-03-20).Fundamentals of diagnostic radiology (4th ed.).
Philadel-phia: Wolters Kluwer/Lippincott Williams & Wilkins.
p.435. ISBN 9781608319114.
[41] Mandell, LA; Wunderink, RG; Anzueto, A; Bartlett,
JG;Campbell, GD; Dean, NC; Dowell, SF; File TM, Jr;Musher, DM;
Niederman, MS; Torres, A; Whitney, CG;Infectious Diseases Society
of America; American Tho-racic Society (1 March 2007). Infectious
Diseases So-ciety of America/American Thoracic Society
consensusguidelines on the management of
community-acquiredpneumonia in adults. Clinical infectious diseases
: an o-cial publication of the Infectious Diseases Society of
Amer-ica 44 (Suppl 2): S2772. doi:10.1086/511159. PMID17278083.
[42] Stedmans medical dictionary. (28th ed.).
Philadelphia:Lippincott Williams & Wilkins. 2006. ISBN
978-0-7817-6450-6.
[43] Dunn, L (June 29 July 5, 2005). Pneumonia: clas-sication,
diagnosis and nursing management. Nursingstandard (Royal College of
Nursing (Great Britain) : 1987)19 (42): 504.
doi:10.7748/ns2005.06.19.42.50.c3901.PMID 16013205.
[44] organization, World health (2005). Pocket book of hospi-tal
care for children : guidelines for the management ofcommon
illnesses with limited resources. Geneva: WorldHealth Organization.
p. 72. ISBN 978-92-4-154670-6.
[45] Jeerson, T; Di Pietrantonj, C; Rivetti, A; Bawazeer,GA;
Al-Ansary, LA; Ferroni, E (2010-07-07). Jeerson,Tom, ed. Vaccines
for preventing inuenza in healthyadults. Cochrane Database of
Systematic Reviews (7):CD001269.
doi:10.1002/14651858.CD001269.pub4.PMID 20614424.
[46] Seasonal Inuenza (Flu)". Center for Disease Control
andPrevention. Retrieved 29 June 2011.
[47] Jeerson T; Deeks, JJ; Demicheli, V; Rivetti, D;Rudin, M
(2004). Jeerson, Tom, ed. Amanta-dine and rimantadine for
preventing and treating in-uenza A in adults. Cochrane Database
Syst Rev (3):CD001169. doi:10.1002/14651858.CD001169.pub2.PMID
15266442.
[48] Jeerson, T; Jones, MA; Doshi, P; Del Mar, CB;Heneghan, CJ;
Hama, R; Thompson, MJ (18 January2012). Jeerson, Tom, ed.
Neuraminidase inhibitorsfor preventing and treating inuenza in
healthy adultsand children. Cochrane Database of Systematic
Reviews1: CD008965. doi:10.1002/14651858.CD008965.pub3.PMID
22258996.
[49] Moberley, SA; Holden, J; Tatham, DP; Andrews,
RM(2008-01-23). Andrews, Ross M, ed. Vaccines forpreventing
pneumococcal infection in adults. Cochrane
-
11
Database of Systematic Reviews (1):
CD000422.doi:10.1002/14651858.CD000422.pub2. PMID18253977.
[50] Pneumonia Can Be Prevented Vaccines Can Help.Centers for
Disease Control and Prevention. Retrieved 22October 2012.
[51] Gray, DM; Zar, HJ (May 2010). Community-acquiredpneumonia
in HIV-infected children: a global perspec-tive. Current Opinion in
Pulmonary Medicine 16 (3):20816. doi:10.1097/MCP.0b013e3283387984.
PMID20375782.
[52] Huang, L; Cattamanchi, A; Davis, JL; den Boon, S; Ko-vacs,
J; Meshnick, S; Miller, RF; Walzer, PD; Worodria,W; Masur, H;
International HIV-associated Opportunis-tic Pneumonias (IHOP),
Study; Lung HIV, Study (June2011). HIV-associated Pneumocystis
pneumonia. Pro-ceedings of the American Thoracic Society 8 (3):
294300. doi:10.1513/pats.201009-062WR. PMC 3132788.PMID
21653531.
[53] Green H, Paul M, Vidal L, Leibovici L (2007).Green,
Hefziba, ed. Prophylaxis for Pneumocys-tis pneumonia (PCP) in
non-HIV immunocompro-mised patients. Cochrane Database Syst Rev
(3):CD005590. doi:10.1002/14651858.CD005590.pub2.PMID 17636808.
[54] Taminato, M; Fram, D; Torloni, MR; Belasco, AG;Saconato, H;
Barbosa, DA (NovemberDecember 2011).Screening for group B
Streptococcus in pregnantwomen: a systematic review and
meta-analysis. Re-vista latino-americana de enfermagem 19 (6):
14708. doi:10.1590/s0104-11692011000600026. PMID22249684.
[55] Darville, T (October 2005). Chlamydia trachoma-tis
infections in neonates and young children. Sem-inars in pediatric
infectious diseases 16 (4): 23544.doi:10.1053/j.spid.2005.06.004.
PMID 16210104.
[56] Global Action Plan for Prevention and Control of Pneumo-nia
(GAPP). World Health Organization. 2009.
[57] Roggensack, A; Jeeries, AL; Farine, D; Basso, M;Delisle,
MF; Hudon, L; Mundle, WR; Murphy-Kaulbeck,LC; Ouellet, A; Pressey,
T (April 2009). Management ofmeconium at birth. Journal of
obstetrics and gynaecologyCanada : JOGC = Journal d'obstetrique et
gynecologie duCanada : JOGC 31 (4): 3534, 3557. PMID 19497156.
[58] van der Maarel-Wierink, CD; Vanobbergen, JN;Bronkhorst, EM;
Schols, JM; de Baat, C (6 March 2012).Oral health care and
aspiration pneumonia in frail olderpeople: a systematic literature
review. Gerodontology30 (1): 39.
doi:10.1111/j.1741-2358.2012.00637.x.PMID 22390255.
[59] Bradley, JS; Byington, CL; Shah, SS; Alverson, B;
Carter,ER; Harrison, C; Kaplan, SL; Mace, SE; McCrackenGH, Jr;
Moore, MR; St Peter, SD; Stockwell, JA; Swan-son, JT (2011-08-31).
TheManagement of Community-Acquired Pneumonia in Infants and
Children Older Than
3 Months of Age: Clinical Practice Guidelines by the Pe-diatric
Infectious Diseases Society and the Infectious Dis-eases Society of
America. Clinical infectious diseases :an ocial publication of the
Infectious Diseases Society ofAmerica 53 (7): e2576.
doi:10.1093/cid/cir531. PMID21880587.
[60] Yang, M; Yuping, Y; Yin, X; Wang, BY; Wu,T; Liu, GJ; Dong,
BR (2010-02-17). Dong, BiRong, ed. Chest physiotherapy for
pneumonia inadults. Cochrane Database of Systematic Reviews
(2):CD006338. doi:10.1002/14651858.CD006338.pub2.PMID 20166082.
[61] Zhang, Y; Fang, C; Dong, BR; Wu, T; Deng, JL(14 March
2012). Dong, Bi Rong, ed. Oxy-gen therapy for pneumonia in adults.
CochraneDatabase of Systematic Reviews 3:
CD006607.doi:10.1002/14651858.CD006607.pub4. PMID22419316.
[62] Chang CC, Cheng AC, Chang AB (2012). Chang,Christina C, ed.
Over-the-counter (OTC) med-ications to reduce cough as an adjunct
to antibi-otics for acute pneumonia in children and adults.Cochrane
Database Syst Rev 2: CD006088.doi:10.1002/14651858.CD006088.pub3.
PMID22336815.
[63] Haider, BA; Lassi, ZS; Ahmed, A; Bhutta, ZA (5 Oc-tober
2011). Bhutta, Zulqar A, ed. Zinc sup-plementation as an adjunct to
antibiotics in the treat-ment of pneumonia in children 2 to 59
months ofage. Cochrane Database of Systematic Reviews
(10):CD007368. doi:10.1002/14651858.CD007368.pub2.PMID
21975768.
[64] Kabra SK; Lodha, R; Pandey, RM (2010). Kabra, SushilK, ed.
Antibiotics for community-acquired pneumo-nia in children. Cochrane
Database Syst Rev 3 (3):CD004874.
doi:10.1002/14651858.CD004874.pub3.PMID 20238334.
[65] Lutyya MN; Henley, E; Chang, LF; Reyburn,SW (February
2006). Diagnosis and treatment ofcommunity-acquired pneumonia
(PDF). Am FamPhysician 73 (3): 44250. PMID 16477891.
[66] Eliakim-Raz, N; Robenshtok, E; Shefet, D; Gafter-Gvili,A;
Vidal, L; Paul, M; Leibovici, L (12 September2012). Eliakim-Raz,
Noa, ed. Empiric antibioticcoverage of atypical pathogens for
community-acquired pneumonia in hospitalized adults.
CochraneDatabase of Systematic Reviews 9:
CD004418.doi:10.1002/14651858.CD004418.pub4. PMID22972070.
[67] Scalera NM; File, TM (April 2007). How longshould we treat
community-acquired pneumonia?". Cur-rent Opinion in Infectious
Diseases 20 (2): 17781. doi:10.1097/QCO.0b013e3280555072.
PMID17496577.
[68] American Thoracic Society; Infectious Diseases So-ciety of
America (February 2005). Guidelines forthe management of adults
with hospital-acquired,
-
12 11 REFERENCES
ventilator-associated, and healthcare-associated pneu-monia. Am
J Respir Crit Care Med 171 (4):
388416.doi:10.1164/rccm.200405-644ST. PMID 15699079.
[69] Marik, PE (May 2011). Pulmonary aspiration syn-dromes.
Current Opinion in Pulmonary Medicine 17 (3):14854.
doi:10.1097/MCP.0b013e32834397d6. PMID21311332.
[70] O'Connor S (2003). Aspiration pneumonia and pneu-monitis.
Australian Prescriber 26 (1): 147.
[71] Behera, D. (2010). Textbook of pulmonary medicine (2nded.).
New Delhi: Jaypee Brothers Medical Pub. pp. 296297. ISBN
9788184487497.
[72] Cunha (2010). Pages6-18.
[73] Rello, J (2008). Demographics, guidelines, and clin-ical
experience in severe community-acquired pneumo-nia. Critical care
(London, England). 12 Suppl 6 (Suppl6): S2. doi:10.1186/cc7025. PMC
2607112. PMID19105795.
[74] Yu, H (March 2011). Management of pleural eusion,empyema,
and lung abscess. Seminars in interventionalradiology 28 (1): 7586.
doi:10.1055/s-0031-1273942.PMC 3140254. PMID 22379278.
[75] Cunha (2010). Pages 250251.
[76] WHO Disease and injury country estimates. WorldHealth
Organization (WHO). 2004. Retrieved 11Novem-ber 2009.
[77] Liu, L; Johnson, HL; Cousens, S; Perin, J; Scott, S;Lawn,
JE; Rudan, I; Campbell, H; Cibulskis, R; Li,M; Mathers, C; Black,
RE; Child Health Epidemiol-ogy Reference Group of WHO and, UNICEF
(Jun 9,2012). Global, regional, and national causes of
childmortality: an updated systematic analysis for 2010 withtime
trends since 2000. Lancet 379 (9832):
215161.doi:10.1016/S0140-6736(12)60560-1. PMID 22579125.
[78] Rudan, I; Boschi-Pinto, C; Biloglav, Z; Mulholland,
K;Campbell, H (May 2008). Epidemiology and etiology ofchildhood
pneumonia. Bulletin of the World Health Or-ganization 86 (5):
40816. doi:10.2471/BLT.07.048769.PMC 2647437. PMID 18545744.
[79] Garenne M; Ronsmans, C; Campbell, H (1992). Themagnitude of
mortality from acute respiratory infectionsin children under 5
years in developing countries. WorldHealth Stat Q 45 (23): 18091.
PMID 1462653.
[80] WHO (1999). Pneumococcal vaccines. WHO positionpaper. Wkly.
Epidemiol. Rec. 74 (23): 17783. PMID10437429.
[81] Weiss AJ, Wier LM, Stocks C, Blanchard J (June
2014).Overview of Emergency Department Visits in the UnitedStates,
2011. HCUP Statistical Brief #174. Rockville,MD: Agency for
Healthcare Research and Quality.
[82] Feigin, Ralph (2004). Textbook of Pediatric
InfectiousDiseases (5th ed.). Philadelphia: W. B. Saunders. p.
299.ISBN 978-0-7216-9329-3.
[83] Hippocrates On Acute Diseases wikisource link
[84] Maimonides, Fusul Musa ("Pirkei Moshe").
[85] Klebs E (1875-12-10). "Beitrge zur Kenntniss der
patho-genen Schistomyceten. VII Die Monadinen" [Signs
forRecognition of the Pathogen Schistomyceten]. Arch. Ex-ptl.
Pathol. Parmakol. 4 (5/6): 40488.
[86] Friedlnder C (1882-02-04). "ber die Schizomycetenbei der
acuten brsen Pneumonie". Virchows Archpathol. Anat. U. Physiol. 87
(2): 319324.doi:10.1007/BF01880516.
[87] Fraenkel A (1884-04-21). "ber die genuine
Pneumonie,Verhandlungen des Congress fr innere Medicin".
DritterCongress 3: 1731.
[88] Gram C (1884-03-15). "ber die isolierte Frbungder
Schizomyceten in Schnitt- und Trocken-prparaten".Fortschr. Med 2
(6): 1859.
[89] edited by J.F. Tomashefski, Jr. [] et al. (2008).
DailandHammars pulmonary pathology (3rd ed.). NewYork:Springer. p.
228. ISBN 978-0-387-98395-0.
[90] William Osler, Thomas McCrae (1920). The principlesand
practice of medicine: designed for the use of practi-tioners and
students of medicine (9th ed.). D. Appleton.p. 78. One of the most
widespread and fatal of all acutediseases, pneumonia has become the
Captain of the Menof Death, to use the phrase applied by John
Bunyan toconsumption.
[91] AdamsWG; Deaver, KA; Cochi, SL; et al. et al.
(January1993). Decline of childhood Haemophilus inuenzaetype B
(Hib) disease in the Hib vaccine era. JAMA 269(2): 2216.
doi:10.1001/jama.1993.03500020055031.PMID 8417239.
[92] Whitney CG; Farley, MM; Hadler, J; et al. et al. (May2003).
Decline in invasive pneumococcal disease af-ter the introduction of
protein-polysaccharide conjugatevaccine. N. Engl. J. Med. 348 (18):
173746.doi:10.1056/NEJMoa022823. PMID 12724479.
[93] World Pneumonia Day Ocial Website. World Pneu-monia Day
Ocial Website. Fiinex. Retrieved 13 August2011.
[94] Household Component Summary Data Tables.
[95] Household Component Summary Data Tables.
[96] One hospital charges $8,000 another, $38,000 -
TheWashington Post.
[97] Welte T, Torres A, Nathwani D (January 2012). Clin-ical and
economic burden of community-acquired pneu-monia among adults in
Europe. Thorax 67 (1): 719.doi:10.1136/thx.2009.129502. PMID
20729232.
Bibliography
John F. Murray (2010). Murray and Nadels text-book of
respiratory medicine (5th ed.). Philadelphia,PA: Saunders/Elsevier.
ISBN 1416047107.
-
13
Burke A. Cunha, ed. (2010). Pneumonia essentials(3rd ed.).
Sudbury, MA: Physicians Press. ISBN0763772208.
12 External links Pneumonia at DMOZ
-
14 13 TEXT AND IMAGE SOURCES, CONTRIBUTORS, AND LICENSES
13 Text and image sources, contributors, and licenses13.1
Text
Pneumonia Source:
http://en.wikipedia.org/wiki/Pneumonia?oldid=650001256
Contributors: Kpjas, Alex.tan, Josh Grosse, Karen John-son, Heron,
B4hand, Edward, D, Fred Bauder, Gabbe, Ixfd64, Paul Benjamin
Austin, Dori, Minesweeper, Mdebets, Ahoerstemeier,
Mac,CatherineMunro, Marumari, Julesd, Glenn, Tristanb, Oliver Crow,
Mxn, Smack, Etaoin, Richard Avery, Saument, Andrewman327,
Tp-bradbury, Ozuma, Saltine, Topbanana, Pollinator, Slawojarek,
Robbot, Fredrik, Chris 73, Gak, Donreed, Mayooranathan, Dmadeo,
Yosri,Hadal, GreatWhiteNortherner, Unfree, Giftlite, Thv, Ian
Maxwell, Nmg20, Haeleth, Nunh-huh, Peruvianllama, Everyking,
Capitalistroad-ster, Alison, Michael Devore, Davin (usurped),
Jfdwol, Silvermask, Stevietheman, SoWhy, Quadell, Antandrus,
Bcameron54, PDH,Khaosworks, DragonySixtyseven, Kevin B12, Bk0, Sam
Hocevar, JHCC, Joyous!, Ta bu shi da yu, Freakofnurture, Haruo,
JimJast, Dis-cospinster, Patricknoddy, Rich Farmbrough, FT2,
GeoEvan, Autiger, Paul August, Mehrenberg, Sgeo, Appleboy, RJHall,
Mr. Billion, Sfa-hey, Fenevad, DS1953, Aude, CDN99, Causa sui,
Keane4, Bobo192, Smalljim, Davidruben, Viriditas, Richi, Arcadian,
Valar, John Fader,Hagerman, Mareino, Knucmo2, Jumbuck, Schissel,
Danski14, Alansohn, Gary, Anthony Appleyard, Halsteadk, Andrewpmk,
Wouter-stomp, Riana, Lectonar, Axl, Ddlamb, Fritzpoll, Stillnotelf,
Lee S. Svoboda, Knowledge Seeker, Evil Monkey, RainbowOfLight,
GeneNygaard, Kazvorpal, Ceyockey, TigerShark, Nuggetboy, Mhearne,
Rikek, Tabletop, Yegorm, Dysepsion, SqueakBox, Graham87, Magis-ter
Mathematicae, Bunchofgrapes, Coneslayer, Rjwilmsi, Rogerd, Harro5,
Vegaswikian, Oblivious, Ligulem, Cww, Sferrier, Brighteror-ange,
The wub, Dolphonia, Bhadani, M A Mason, Ucucha, Fred Bradstadt,
Sango123, Avocado, FlaBot, Ian Pitchford, RobertG, AED,Nihiltres,
Chanting Fox, RexNL, Gurch, Stevenfruitsmaak, BradBeattie, Chobot,
Rewster, Gwernol, YurikBot, Koveras, Rob T Fire-y, Cabiria, Pburka,
WAvegetarian, Bergsten, Eleassar, Big Brother 1984, Herbertxu,
NawlinWiki, Wiki alf, Bachrach44, Jaxl, Duran,Irishguy, Albedo,
Nephron, Andersonblog, The Filmaker, Wolbo, Voidxor, Tony1,
Digitylgoddess, Dissolve, Nescio, Cstaa, WAS 4.250,Encephalon,
JCipriani, Closedmouth, Nemu, Sariberi, Badgettrg, JLaTondre,
Spliy, Jacqui M, Ben D., RG2, John Broughton, Andrew73,Quadpus,
SpLoT, SmackBot, Teenwriter, FloNight, Hydrogen Iodide, Pgk,
InvictaHOG, Hswapnil, Delldot, Eskimbot, HalfShadow, Xaos-ux,
DaveThomas, Gilliam, ERcheck, Master Jay, RDBrown, W8IMP,
Thumperward, DanF, MalafayaBot, SchftyThree, Moshe Con-stantine
Hassan Al-Silverburg, Baa, VenomSnake, Darth Panda, A. B., Scray,
Yidisheryid, Pooresd, TheKMan, Wotiuwoetuwte3525,32GN3B, R0xorz,
Fact Checker, Reppppp, Zvar, Krich, Jared, SnappingTurtle, ShaunES,
G716, Chandra rippett, Drphilharmonic, Sala-murai, Mattopaedia,
Kukini, SashatoBot, Lambiam, OhioFred, Kuru, Jidanni, Ninjagecko,
Sir Nicholas de Mimsy-Porpington, NongBot,Rawmustard, Larrymcp,
Waggers, SandyGeorgia, Avant Guard, Dl2000, Hu12, Vlad788, Alan.ca,
Iridescent, StephenBuxton, Igoldste,Marysunshine, Tawkerbot2,
Ouishoebean, Chitoboy, Jmockbee, Ghaly, Fvasconcellos, SkyWalker,
Tifego, JForget, CmdrObot, Eggman64,Ale jrb, Mattbr, KyraVixen,
Trails, GHe, THF, CuriousEric, Edenane, Williamallenmd, Moreschi,
Schaber, Cydebot, Psybrdelic, JFree-man, Myscrnnm, DumbBOT,
Robbieisfun, MrLenS, IComputerSaysNo, Kozuch, Leendert,
Krylonblue83, Casliber, FrancoGG, Mattisse,Epbr123, Wikid77,
Flynnj, Notjake13, Loudsox, Headbomb, Dayn, Laportechicago,
Escarbot, Navdar, Eleuther, Dantheman531, Tha-dius856, PicklePower,
Cyclonenim, AntiVandalBot, Majorly, Cwray, Just Chilling, Jayron32,
Msnomer, LibLord, Alphachimpbot, LordRichard, Richiez,
Canadian-Bacon, Res2216restar, JAnDbot, Husond, Instinct, Seddon,
Albany NY, Verbivorous, Thebaldbandit, Ben-nybp, Bongwarrior,
VoABot II, Kuyabribri, Lucyin, Jjoshua33, JHB, WhatamIdoing, MiPe,
Adrian J. Hunter, Allstarecho, DerHexer,Khalid Mahmood,
Supahfreekeh, Yobol, MartinBot, BetBot, Nicolauswb, Poeloq,
Moabalan, Foraminifera, AlexiusHoratius, Nono64,Fconaway,
J.delanoy, Leon math, Numbo3, Maneater**, AlanWolfe, L337
kybldmstr, FrummerThanThou, Mr Rookles, Maestozo, MikaelHggstrm,
Nsoltani, (jarbarf), Belovedfreak, NewEnglandYankee, Deimel,
Gaussgauss, Balaam42, Shoessss, Sunderland06, Timtam85,Treisijs,
Zomguberdude, Billborder, Vinsfan368, Izno, CardinalDan,
Idioma-bot, Lights, X!, Deor, Thedjatclubrock, Je G.,
Mocirne,MenasimBot, Hehkuviini, Rasillon, Philip Trueman, TXiKiBoT,
GimmeBot, Paine, A369852, Medicaldoctor129, Qwertyu123,
Gwinva,Sherrygravely, Melsaran, Gilvala, Madhero88, Ninjatacoshell,
Enigmaman, Xianlulaura, Cnilep, Brianga, Jesse1996, Doc James,
Alle-borgoBot, Heliocybe, RedRabbit1983, EmxBot, SieBot,
Winchelsea, Gerakibot, Da Joe, Dawn Bard, Caltas, ConfuciusOrnis,
BService,Micknaor, Exert, Sohelpme, Nopetro, Yerpo, ChrTh,
Oxymoron83, Antonio Lopez, Lightmouse, Miguel.mateo, Lumentec,
OKBot, Mael-gwnbot, MadmanBot, Twigat, Realm of Shadows, Lynnsamal,
Dabomb87, Nn123645, JL-Bot, Tattery, The sunder king,
Ricklaman,De728631, ClueBot, The Thing That Should Not Be, Marko
sk, Pairadox, Paul Abrahams, Mild Bill Hiccup, Lamasrock,
Caboose420,Zlm73, Osm agha, DrFO.Jr.Tn, Blanchardb, Shannon bohle,
Madbeal, Alexbot, CrazyChemGuy, ToNToNi, Rybee824, Keledin, Sun
Cre-ator, Tyler, Ravenna1961, NuclearWarfare, Cenarium, Peter.C,
Medos2, Razorame, Brianb824, Netanel h, Thingg, Korefauigy,
Aitias,Fatrobbie, UrsaLinguaBWD, SDY, Saguanau101, Saguanau5,
Thompsontough, DumZiBoT, BendersGame, Londonsista, Monkey3035,Tony
K10, Infoporn, Fruv, Hard working team, Dwight Burdette, Jkuo3,
TamePhysician, Addbot, Emotology, Done3557, Matt641, DOIbot,
Wickey-nl, DougsTech, Older and ... well older, Shokod, D.c.camero,
Shayla007, Debresser, Numbo3-bot, 55, Szalax, Walki-etalkiee, Ben
Ben, Luckas-bot, Yobot, Berkay0652, Uchiha611, MarcoAurelio, THEN
WHO WAS PHONE?, Nallimbot, KamikazeBot,EnTerr, ChildSurvival,
Ebalter, Teneil00, Magog the Ogre, AnomieBOT, Piano non troppo,
Aditya, Joker1189, Citation bot, Eumolpo,Lungsunit, LilHelpa,
Xqbot, Cureden, Capricorn42, Pneumoniaman123, Hammersbach,
Mario123456, Jaxyl, J04n, GrouchoBot, Kevdave,Soabenke, Ank85,
Maria Sieglinda von Nudeldorf, RibotBOT, Thehelpfulbot, Spongefrog,
FrescoBot, LucienBOT, Preventpneumo, Ci-tation bot 1, AstaBOTh15,
Boulaur, Jonesey95, Sultanofhyd, Thesevenseas, VenomousConcept,
Jandalhandler, 9014user, HCUP US,Da5id1, Jchapple88, TheBearPaw,
RjwilmsiBot, Whywhenwhohow, EmausBot, WikitanvirBot, Hreid11,
Observer6, , Cpant23,Drankush, GoingBatty, Uploadvirus, Ceeforcat,
Manum56, Lji1942, Jesanj, Kgsbot, CPnieuws, FeatherPluma,
Mahmoudalrawi, Will Be-back Auto, Mallexikon, Jamesdpalmer,
Nijilravipp, Vldscore, EnglishTea4me, Robthepiper, Jcgoble3,
Rezabot, JordanSeymore, , Helpful Pixie Bot, Dalit Llama, Lowercase
sigmabot, MKar, Mrjohncummings, Sahara4u, PhnomPencil, Cypella,
Neuroschizl,Je.rrt, FormerNukeSubmariner, Fallingmasonry,
RudolfRed, BattyBot, TylerDurden8823, 00AgentBond93, Dexbot, Ildiko
Santana, Mo-gism, Palma Marton Chatonnet, Randykitty, EtymAesthete,
Anrnusna, AH999, Captain Cornwall, Monkbot, Formerly 98,
TeaLover1996,Maplestrip and Anonymous: 651
13.2 Images
File:CT_scan_of_the_chest,_demonstrating_right-sided_pneumonia.jpg
Source: http://upload.wikimedia.org/wikipedia/commons/
7/7a/CT_scan_of_the_chest%2C_demonstrating_right-sided_pneumonia.jpg
License: CC BY-SA 3.0 Contributors: Own work Originalartist: James
Heilman, MD
File:Crackles_pneumoniaO.ogg Source:
http://upload.wikimedia.org/wikipedia/commons/c/c7/Crackles_pneumoniaO.ogg
License:CC BY-SA 3.0 Contributors: Own work Original artist: James
Heilman, MD
File:Gnome-mime-sound-openclipart.svg Source:
http://upload.wikimedia.org/wikipedia/commons/8/87/
-
13.3 Content license 15
Gnome-mime-sound-openclipart.svg License: Public domain
Contributors: Own work. Based on
File:Gnome-mime-audio-openclipart.svg, which is public domain.
Original artist: User:Eubulides
File:Lower_respiratory_infections_world_map_-_DALY_-_WHO2004.svg
Source:
http://upload.wikimedia.org/wikipedia/commons/7/75/Lower_respiratory_infections_world_map_-_DALY_-_WHO2004.svg
License: CC BY-SA 2.5 Contributors:
Vector map from BlankMap-World6, compact.svg by Canuckguy et al.
Original artist: Lokal_Prol File:New_Pneumonia_cartoon.jpg Source:
http://upload.wikimedia.org/wikipedia/commons/f/fb/New_Pneumonia_cartoon.jpg
Li-
cense: Public domain Contributors: Transferred from
en.wikipedia; transferred to Commons by User:Quadell using
CommonsHelper.Original artist: Original uploader was InvictaHOG at
en.wikipedia
File:Padlock-silver.svg Source:
http://upload.wikimedia.org/wikipedia/commons/f/fc/Padlock-silver.svg
License: CC0
Contributors:http://openclipart.org/people/Anonymous/padlock_aj_ashton_01.svg
Original artist: This image le was created by AJ Ashton.
Uploadedfrom English WP by User:Eleassar. Converted by User:AzaToth
to a silver color.
File:Pleural_effusion.jpg Source:
http://upload.wikimedia.org/wikipedia/commons/e/e7/Pleural_effusion.jpg
License: Public domainContributors:
http://www.cdc.gov/ncidod/dvbid/dengue/slideset/spanish/set1/vi/slide08.htm
Original artist: User InvictaHOG on en.wikipedia
File:Streptococcus_pneumoniae.jpg Source:
http://upload.wikimedia.org/wikipedia/commons/2/20/Streptococcus_pneumoniae.jpg
License: Public domain Contributors: This media comes from the
Centers for Disease Control and Prevention's Public Health Image
Library(PHIL), with identication number #262. Original artist:
Photo Credit: CDC/Janice Carr Content Providers(s): CDC/Dr.
Richard Facklam
File:Symbol_support_vote.svg Source:
http://upload.wikimedia.org/wikipedia/en/9/94/Symbol_support_vote.svg
License: Public do-main Contributors: ? Original artist: ?
File:Symptoms_of_pneumonia.svg Source:
http://upload.wikimedia.org/wikipedia/commons/2/20/Symptoms_of_pneumonia.svg
Li-cense: Public domain Contributors: All used images are in public
domain. Original artist: Mikael Hggstrm.
File:WPA_Pneumonia_Poster.jpg Source:
http://upload.wikimedia.org/wikipedia/commons/7/77/WPA_Pneumonia_Poster.jpg
Li-cense: Public domain Contributors: Work Projects Administration
Poster Collection (Library of Congress).
http://memory.loc.gov/service/pnp/cph/3f00000/3f05000/3f05300/3f05391r.jpg
Original artist: WPA Federal Art Project
13.3 Content license Creative Commons Attribution-Share Alike
3.0
Signs and
symptomsCauseBacteriaVirusesFungiParasitesIdiopathic
MechanismsViralBacterial
DiagnosisPhysical
examImagingMicrobiologyClassificationDifferential diagnosis
PreventionVaccinationOther
ManagementBacterialViralAspiration
PrognosisClinical prediction rulesPleural effusion, empyema, and
abscessRespiratory and circulatory failure
EpidemiologyChildren
HistorySociety and cultureAwarenessCosts
ReferencesExternal linksText and image sources, contributors,
and licensesTextImagesContent license