Embed Size (px)
Citation preview

Population-basedNeuropathology:classification of disease
biomarkerdiscovery tool
Thomas J. Montine, MD, PhDAlvord Professor and ChairDepartment of PathologyUniversity of Washington
Disclosures: Consultant to: Eisai, Amgen, BMSNo off-label medicationsNo medical devices

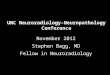
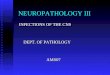
RiskGenetics
Previous life events Likelihood of initiation or progression
disease in the future.
Actual
Clinical Data degree & character of functional impairment
Normal Mild Impairment
Dementia or Parkinsonian
Laboratory Data disease type &
burdenNone + ++ +++
Chronic DiseaseModel
No Disease
Latency ProdromeFull
Expression
“Laboratory data” can be neuropath, lab med, and neuroimaging
“Clinical data” can be signs, symptoms, and neuropsych findings
Neuropathology of Dementia
Classification of Disease
Risk of disease vs. Actual diseaseExtent vs. Causes of functional impairment

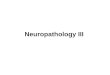
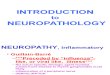
AD
ProteinopathyMito Stress
Glial activationEtc.
Aging, Genetics, Environment
PRODROME
VBI
LBD
DEMENTIALATENT DISEASE
Injury &Response to Injury
Repair &FunctionalCompensa-
tion
Chronic disease model of dementia
AD ≈45%
VBI ≈33%
LBD ≈10%
COGNITIVELY NORMAL
Neuropathology of Dementia
Classification of Disease

Dementia stageNeuropathology of Dementia
Classification of Disease

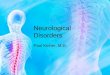
AD
ProteinopathyMito Stress
Glial activationEtc.
Aging, Genetics, Environment
PRODROME
VBI
LBD
DEMENTIALATENT DISEASE
Injury &Response to Injury
Repair &FunctionalCompensa-
tion
Chronic disease model of dementia
AD ≈45%
VBI ≈33%
LBD ≈10%
Neuropathology of Dementia
COGNITIVELY NORMAL

AD
ProteinopathyMito Stress
Glial activationEtc.
Aging, Genetics, Environment
PRODROME
VBI
LBD
DEMENTIALATENT DISEASE
Injury &Response to Injury
Repair &FunctionalCompensa-
tion
Chronic disease model of dementia
AD ≈45%
VBI ≈33%
LBD ≈10%
Neuropathology of Dementia
COGNITIVELY NORMAL
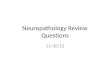
ACTHAASNun StudyOBAS

AD
ProteinopathyMito Stress
Glial activationEtc.
Aging, Genetics, Environment
PRODROME
VBI
LBD
DEMENTIALATENT DISEASE
Injury &Response to Injury
Repair &FunctionalCompensa-
tion
Summary
AD ≈45%
VBI ≈33%
LBD ≈10%
COGNITIVELY NORMAL
Neuropathology of Dementia
Classification of Disease
• 3 chronic diseases account for vast majority of dementia• Idiosyncratic convergence at all stages of impairment• Progressive aggregate disease vs. functional impairment• Apparent resilience and hightened vulnerability

2012 NIA-AA revised Guidelines for Neuropath EvaluationNeuropathology of Dementia
Classification of Disease


Isssue 1997 2012Clinical Dx of dementia
required for NP Dx of ADYes No
NP assessment based on Braak for NFTs & CERAD for Neuritic plaques
These plus Thal phase for Ab regional accumulation
NP assessment of commonly co-morbid diseases
Little guidance Explicit
Minimum regions to sample and stains to be used
Silent Explicit
Reporting and CPC Silent Guidelines
2012 NIA-AA revised Guidelines for Neuropath EvaluationNeuropathology of Dementia
Classification of Disease

LP within 3 wk of cognitive testing
Clinical Lab evidence for AD is rare in cognitively normal volunteers younger than 50 yr-old
≈ 20% of cognitively normal volunteers > 50 yr-old have laboratory evidence of AD• Have poorer cognitive function at baseline• Have much greater risk of converting to MCI
or AD in next 3 to 4 years
CSF tau and Ab42
Volunteers for lumbar puncture: OHSU, UCSD, & UW ADCSpectrum of Normal Cognition to Dementia
Neuropathology of Dementia
Biomarkers

Neuropathology of Dementia
Discovery Tool
Histelide• Molecular-specific regional quantification• IHC

Neuropathology of Dementia
Discovery Tool
Histelide• Molecular-specific regional quantification• IHC

Neuropathology of Dementia
Discovery Tool
Histelide• Molecular-specific regional quantification• IHC

Neuropathology of Dementia
Discovery Tool
Histelide• Molecular-specific regional quantification• IHC