Embed Size (px)
Citation preview

CASE REPORT Open Access
Post esophagectomy diaphragmatichernia: a case report of a rare causeof acute respiratory distressValérie Lamontagne1, Valérie Lafrenière-Bessi1, Arthur Vieira2, Éric Charbonneau1, Paula A. Ugalde2
and Frédéric Jacques1*
Abstract
Background: Diaphragmatic hernia is frequent among the elderly and is usually associated with mild chronicdigestive and respiratory symptoms.
Case presentation: An elderly post-esophagectomy male patient, in the early postoperative period of cardiacsurgery, presented with acute respiratory distress. An emergent surgery was performed to reduce a giantdiaphragmatic herniation.
Conclusions: An acute transhiatal herniation can cause serious respiratory impairment; surgical repair should beconsidered in select patients of cardiac surgery.
Keywords: Diaphragmatic hernia, Respiratory distress, Post-esophagectomy, Cardiac surgery
BackgroundDiaphragmatic hernia is a benign condition thatmanifests with chronic dyspnea and intermittentgastrointestinal symptoms, such as epigastric pain,postprandial fullness and nausea [1, 2]. Acute respira-tory distress associated with a giant diaphragmaticherniation of abdominal contents is unusual in theearly postoperative period of cardiac surgery. Atypicalsymptoms, detailed clinical management and the sur-gical hernia repair in an elderly post-esophagectomymale patient are described.
Case presentationA 74-year-old male, who had undergone 3 stent coronaryimplantation procedures in the previous 6 months, pre-sented to the hospital with progressive dyspnea and recur-rent chest pain. The patient’s medical history was notedfor esophageal cancer treatment that consisted of a radicalesophagectomy, gastric pull-up followed by chemotherapyand radiotherapy. Esophageal cancer recurrence was ruled
out. A transthoracic echocardiography revealed severeaortic regurgitation, moderate mitral regurgitation and aleft ventricular ejection fraction of 44%.The patient underwent a dual valve replacement pro-
cedure with a bioprothesis aortic valve (23 mm MagnaEase, Edwards Lifesciences, CA, USA) and mechanicalmitral valve (25 mm ON-X, CryoLife, GA, USA). Thepatient required 7 days of inotropes and intensive unitcare. On postoperative (PO) day 8, a right-sided chy-lothorax was diagnosed, and treated with simple drain-age and low-fat medium chain triglycerides diet. On POday 18, the patient evolved with acute respiratory deteri-oration and hypoxemia. Chest auscultation revealedperistaltic sounds on the left side. Chest x-ray revealedright pleural effusion and abdominal contents within theleft chest cavity (Fig. 1a). Despite pleural effusion drainage,the patient had only slightly improved the respiratory sta-tus (Fig. 1b). A chest computerized tomography confirmedthe presence of a large portion of the transverse and de-scending colon in the left hemithorax with no radiologicalsign of intestinal necrosis (Fig. 2). The diaphragmatic her-nia measured 15 cm and filled the whole transverse di-mension of the left chest on the anterior-posterior view. Atransthoracic echocardiogram ruled out acute cardiac
* Correspondence: [email protected] of Cardiac Surgery, Multidisciplinary Department of Cardiology,Institut universitaire de cardiologie et de pneumologie de Québec, UniversitéLaval, QC, CanadaFull list of author information is available at the end of the article
© The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Lamontagne et al. Journal of Cardiothoracic Surgery (2018) 13:114 https://doi.org/10.1186/s13019-018-0802-x

complications. Clinical deterioration was evidenced by in-creased oxygen requirements to 5 L/min, tachypnea,tachycardia and confusion.
Urgent diaphragmatic hernia repair was indicated andperformed by laparoscopy. The patient was placed in adorsal position with hyperextension of the upper third ofhis abdomen. Laparoscopic surgery was performedthrough two 12 mm trocars on the left and right para-umbilical region and three 5 mm trocars were used inthe subcostal region, one on the right side and two onthe left. The 10 mm 30G camera was inserted throughthe left paraumbilical incision. A large quantity of peri-toneal adherences was taken down with harmonic syn-ergy blades (Ethicon, OH, USA) under direct vision. Alarge diaphragmatic hernia was identified with a largeportion of the transverse colon and omentum within theleft chest cavity. Once the majority of the colon was re-duced the dissection of the hernial sac from the rightand from the left hiatal pillars toward the mediastinumand the apex of the left chest. Pealing the sac off wasmandatory for a complete reduction and repair of thehernia. As expected, the apical portion was the most la-borious however with proper exposure the dissectionwas safely performed. The colon stayed passively in theabdominal cavity. The repair of the hiatal hernia wasperformed by approximating the left and right pillarswith non-absorbable stiches. A Biodesign Hiatal HerniaGraft (Cook Medical, IN, USA) was placed surroundingthe hiatus. A prolene mesh (Ethicon, OH, USA) wasused to close the anterior space. Both grafts were fixedwith tacker fixation device (Medtronic, MN, USA). Thefinal result was satisfactory.The patient had postoperative ischemic colitis and
interstitial alveolar left lower lobe infiltrate. This wasmanaged with a conservative treatment based on antibi-otics and parenteral nutrition. A Pleur-X chronically in-dwelling catheter system (Becton Dickinson, NJ, USA)was installed in the patient before discharge, 3 monthsafter surgery. One year after discharge, the patient wasreadmitted with increased dyspnea. A right sided chy-lothorax, secondary to Pleur-X infection, was diagnosed.The drainage system was changed, antibiotic treatmentwas given for 2 weeks and the patient is now doing well.
Discussion and conclusionsThough the incidence of post-esophagectomy hiatal her-nia is increasing, the occurrence of acute giant hiatalhernia complicated with acute respiratory distress is rare[3, 4]. Asymptomatic patients with post-esophagectomyhernias are usually observed [5]. In cases of respiratorysymptoms, related to aspiration with gastroesophagealreflux disease or shortness of breath caused by mechan-ical pressure induced by intrathoracic herniation, surgi-cal treatment is indicated [6, 7].In this case, an urgent surgical repair was needed to
treat respiratory distress caused by an acute hiatal herniain the early postoperative period of cardiac surgery. The
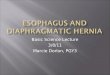
Fig. 1 Anterior to posterior chest roentgenogram showing: (a)recurrent right chylothorax combined with the left intrathoracicherniated colon (upright sitting position); (b) right pigtail catheterinsertion and chylothorax drainage (upright sitting position); (c)resolution of both the chylothorax and the herniated colon(supine position)
Lamontagne et al. Journal of Cardiothoracic Surgery (2018) 13:114 Page 2 of 3

common causes of respiratory distress, such as cardiactamponade, pleural effusion, fluid overload and pros-thesis thrombosis or dehiscence, were excluded. A chestX-ray followed by a computerized tomography scan con-firmed a herniated colon into the left chest cavity withcomplete lung atelectasis.Surgical treatment of diaphragmatic hernia is usually
performed after recurrent and dramatic symptoms [1, 8].Physicians should keep in mind that a large hiatal herniacan develop in post-esophagectomy patients and causeatypical symptoms such as chronic dyspnea, exercise in-tolerance and recurrent chest pain. Rapid respiratory de-compensation in patients with indolent diaphragmatichernia can occur with changes in the respiratory physi-ology, especially with acute changes in intrathoracicpressure. Risk assessment for surgical repair of giant hia-tal hernia prior to cardiac surgery must be considered.In the case reported herein, the patient recovered well,but emergent hiatal hernia repair remains high risk.Careful follow-up is also needed for the management ofpleural effusions in patients with a chronically indwellingcatheter system.
AbbreviationPO: postoperative
AcknowledgmentsNot applicable.
FundingNot applicable.
Availability of data and materialsNot applicable.
Authors’ contributionsVLB, FJ, RB, JB, PAU and SL have contributed to the conception and writingof the manuscript. All authors have approved the final manuscript.
Ethics approval and consent to participateInstitutional review board approval to publish was obtained.
Consent for publicationPatient consent was obtained.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in publishedmaps and institutional affiliations.
Author details1Service of Cardiac Surgery, Multidisciplinary Department of Cardiology,Institut universitaire de cardiologie et de pneumologie de Québec, UniversitéLaval, QC, Canada. 2Service of Thoracic Surgery, Multidisciplinary Departmentof Respirology, Institut universitaire de cardiologie et de pneumologie deQuébec, Université Laval, Quebec City, Canada.
Received: 24 May 2018 Accepted: 5 November 2018
References1. Bawahab M, Mitchell P, Church N, Debru E. Management of acute
paraesophageal hernia. Surg Endosc. 2009;23:255–9.2. Greub G, Liaudet L, Wiesel P, Bettschart V, Schaller MD. Respiratory
complications of gastroesophageal reflux associated with Paraesophagealhiatal hernia. J Clin Gastroenterol. 2003;37(2):129–31.
3. Brenkman FJH, Parry K, Noble F, et al. Hiatal hernia after Esophagectomy forcancer. Ann Thorac Surg. 2017;103:1055–62.
4. Mirdamadi SA, Arasteh M. Hiatal hernia: an unusual presentation of dyspnea.N Am J Med Sci. 2010;2(8):395–6.
5. Stylopoulos N, Gazelle SG, Rattner DW. Paraesophageal hernia: operation orobservation. Ann Surg. 2002;236:492–501.
6. Berkman N, Simon Z, Almog Y, Kramer MR. Acute gastric dilation causingrespiratory failure and “tension pneumothorax” in an elderly woman with adiaphragmatic hernia. Chest. 1993;104:317–8.
7. McDonnell MJ, Ahmed M, Das J, et al. Hiatal hernias are correlated withincreased severity of non-cystic fibrosis bronchiectasis. Respirology.2015;20:749–57.
8. Ito H, Kitami M, Ohgi S, et al. Large hiatus hernia compressing the heart andimpairing the respiratory function. J Cardiol. 2003;41:29–34.
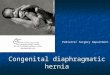
Fig. 2 Chest computed tomography depicting left lung atelectasia as a consequence of colic herniation in the chest: a coronal view); (b)Transverse view
Lamontagne et al. Journal of Cardiothoracic Surgery (2018) 13:114 Page 3 of 3