Embed Size (px)
Citation preview

Brain Injury, May 2009; 23(5): 445–449
Post-traumatic mutism in children
XI JIAN, WANG JUNYU, & LIU JINFANG
Department of Neurosurgery, Xiangya Hospital, Central South University, Changsha, Hunan Province, PR China
(Received 7 May 2008; accepted 18 February 2009)
AbstractObjective: To explore the pathological mechanism of post-traumatic mutism (PTM) in children.Methods: A retrospective study of 16 children who suffered from severe head injury and developed PTM.Results: Post-traumatic coma lasted from 2–72 days, average 15.5 days; while post-traumatic mutism lasted from 2–56 days,average 11.94 days. The correlation between duration of coma and mutism was significant (p< 0.001). SPECT found thatmultiple persistent ischaemic brain regions occurred in all patients; the mean number of regions was 5.6. The patients weresub-divided into three groups based on the number of ischaemic regions: group 1, � 4; group 2, 5� 6; group 3, � 7. Theduration of mutism did not differ significantly between groups 1 and 2, but the difference between group 3 and the othertwo groups combined was significant (p< 0.05).Conclusion: Most PTM occurred in patients with diffuse brain injury. The duration of mutism was related to the number ofischaemic brain regions and the duration of post-traumatic coma.
Keywords: Children, brain injury, mutism, SPECT, brain region, ischaemia
Introduction
Post-traumatic mutism (PTM) occurs rarely and ischaracterized by the short-term dysfunction of verbalexpressing ability after trauma without a significantdecrease in comprehension. Levin et al. [1] reportedthat the incidence of PTM was 3% in patients withsevere brain trauma and was slightly higher inchildren than adults, which the incidence of PTMin children has no issued statistical results yet. Twoprevious publications also showed that PTM wasrare in adult patients with severe brain trauma [2, 3].
PTM is not caused by damage to Broca’s speechcentre. It can be differentiated from psychogenicmutism, akinetic mutism, post-traumatic aphasiaand cerebellar mutism by a period of total absence ofvocal emission associated with a gradual recovery ofverbal comprehension and communication skills,preserved oropraxies and vocalizations related topain and emotions [4]. However, there are still
considerable arguments about the mechanism ofonset of PTM. Dayer et al. [4] summarized theimaging information from six children who sufferedfrom PTM and suggested that none had an occupy-ing effect after intracranial injury. In contrast, someother case reports suggested that PTM resulted fromdiffuse cerebral trauma [5–8].
Such studies only involved in imaging data lackinginformation about focal cerebral metabolism orblood flow, which might underlie the discrepanciesbetween the studies. The imaging data alone, whichis restricted by resolution and other factors, isinsufficient to reflect the general post-trauma con-dition. SPECT can provide information about focalcerebral blood flow, which should help to completelyanalyse the functions of injured brain and explorethe mechanism of onset of PTM.
This study reports a retrospective study of 16children hospitalized with PTM (Table I) fromApril 1999 to October 2006. The clinical
Correspondence: Wang Junyu, Department of Neurosurgery, Xiangya Hospital, Central South University, Changsha 410008, Hunan Province, PR China.E-mail: [email protected]
ISSN 0269–9052 print/ISSN 1362–301X online � 2009 Informa Healthcare Ltd.DOI: 10.1080/02699050902838157
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Nor
th T
exas
on
11/2
1/14
For
pers
onal
use
onl
y.

manifestation, Glasgow Coma score (GCS) atadmission, coma duration, the manifestation onCT, MRI and SPECT, the duration of PTM afterthe end of coma (spontaneous eye opening) and thedegree of recovery were analysed.
Patients and methods
General data
Sixteen patients (12 boys and four girls) with anaverage age of 7.34 years and a GCS of 7.37 atadmission were studied: two cases with acutesubdural haematoma combined with contusion andlaceration of the brain, two cases with intracerebralhaematoma, 12 cases with severe Diffuse AxonalInjury (DAI) and two cases with pre-operativeplatycoriasis.
Patient management
Two patients received craniotomy, one of which alsounderwent single decompressive craniectomy. Allpatients were treated in the ICU. Early tracheotomywas performed in patients with airway obstruction orSaO2 below 95%. All patients received multiplelumbar punctures until the CSF became clear. Allcases also received vasodilators and neurotrophicmedication as routine. Hyperbaric oxygenationwithout corticosteroids was given to patients in astable condition. Families tried to communicate withthe children in various ways, including speech andsign language, during PTM. The patients were askedto make finger movements. The older patients wereasked to read newspapers and books silently and tomake corresponding lip movements.
Mutism recovery
All patients recovered emotional expression andunderstood the power of language after the end ofcoma. The duration of mutism until oral expressionwas recorded. At first patients uttered incoherentmonotonic words such as mom, pain, urine and soon, followed by coherent sentences 2–3 days later,but most speech was still slow and in some patientswas accompanied with dysarthria. Two-to-threeweeks later, oral expression returned to normal inmost children.
CT, MRI and SPECT
CT and SPECT were performed on all cases. Theencephalic ischaemic regions detected by SPECTwere divided into two sides and 10 sites includingfrontal lobe, temporal lobe, parietal lobe, occipitallobe, thalamus and basal ganglia. MRI was per-formed on 12 cases.
Tab
leI.
Gen
eral
info
rmat
ion
and
SP
EC
Tre
sult
sof
pat
ien
ts.
Du
rati
on
(day
s)Is
chem
icre
gion
dis
trib
uti
on
inS
PE
CT
Pat
ien
tn
o.
Age
(yea
rs)
Sex
Inju
rym
ech
anis
mC
om
aM
uti
smG
CS
on
adm
issi
on
fron
tal
tem
pora
lp
arie
tal
occ
ipit
alth
alam
us
Ou
tcom
e(G
OS
)
111
MF
allin
g3
28
Lef
tL
eft
Rig
ht
Good
reco
very
27
MT
raff
icac
cid
ent
22
8L
eft
Lef
tL
eft
Good
reco
very
313
MT
raff
icac
cid
ent
10
12
8R
igh
tR
igh
tB
ilat
eral
Lef
tB
ilat
eral
Good
reco
very
43.5
MT
raff
icac
cid
ent
24
13
5R
igh
tR
igh
tB
ilat
eral
Bilat
eral
Mod
erat
ed
isab
ilit
y5
13
FT
raff
icac
cid
ent
53
8B
ilat
eral
Rig
ht
Rig
ht
Rig
ht
Good
reco
very
62
MF
allin
g7
77
Lef
tL
eft
Lef
tL
eft
Lef
tG
ood
reco
very
77
MT
raff
icac
cid
ent
85
8R
igh
tR
igh
tR
igh
tB
ilat
eral
Mod
erat
ed
isab
ilit
y8
8M
Tra
ffic
acci
den
t9
88
Rig
ht
Rig
ht
Rig
ht
Rig
ht
Good
reco
very
94
FF
allin
g8
58
Lef
tL
eft
Lef
tL
eft
Mod
erat
ed
isab
ilit
y10
8M
Tra
ffic
acci
den
t26
18
6B
ilat
eral
Bilat
eral
Rig
ht
Rig
ht
Bilat
eral
Sev
ere
dis
abilit
y11
3M
Tra
ffic
acci
den
t72
56
4W
hole
bra
inh
ypop
erfu
sion
Sev
ere
dis
abilit
y12
5F
Tra
ffic
acci
den
t11
12
6L
eft
Lef
tL
eft
Bilat
eral
Mod
erat
ed
isab
ilit
y13
9M
Tra
ffic
acci
den
t5
38
Rig
ht
Lef
tL
eft
Lef
tR
igh
tG
ood
reco
very
14
14
MT
raff
icac
cid
ent
99
7B
ilat
eral
Rig
ht
Rig
ht
Lef
tR
igh
tG
ood
reco
very
15
4M
Tra
ffic
acci
den
t32
24
5R
igh
tB
ilat
eral
Rig
ht
Rig
ht
Bilat
eral
Sev
ere
dis
abilit
y16
6F
Tra
ffic
acci
den
t17
12
6R
igh
tR
igh
tB
ilat
eral
Rig
ht
Bilat
eral
Mod
erat
ed
isab
ilit
y
446 X. Jian et al.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Nor
th T
exas
on
11/2
1/14
For
pers
onal
use
onl
y.

Statistical analysis
The rank sum test and the correlative analysis wereprocessed by SPSS10.0 software.
Results
Mutism and coma
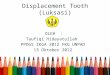
Coma lasted from 2–72 days (average 15.50 days)and PTM lasted from 2–56 days (average 11.94days) (Table I). The duration of mutism waspositively related to duration of coma (Figure 1).
Imaging data
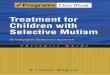
A CT scan was performed on all patients 1–2 daysafter trauma and the main imaging changes were:subarachnoid haemorrhage in 12 cases, acute sub-dural haematoma combined with cerebral contusionin two cases, linear fracture in six cases, intracerebralhaematoma in two cases and DAI in 12 cases. MRIobtained at 7–30 days after trauma in 12 childrenshowed no significant cerebellar lesions, with a smallencephalomalacia in the body of the corpus callosumin one child at 30 days post-trauma (Figure 2).
SPECT
All patients received a SPECT scan, showing morethan one ischaemic brain region in each case. Asshown in Table I, the distribution of ischaemicregions can be summarized as follows: all cases hadischaemic changes in one or both sides of the frontallobe (left side, five cases; right side, seven cases; bothsides, four cases) and the temporal lobe (left side, sixcases; right side, seven cases; both sides, three cases).Fifteen of 16 cases had ischaemic regions in thethalamencephalon (left side, three cases; right side,four cases; both sides, eight cases). Two cases had noischaemic changes in the parietal lobe. The leastinvolved region was the occipital lobe.
The patients were classified into three groupsaccording to the number of ischaemic encephalicregions detected by SPECT: group 1,� 4; group 2,5� 6; group 3, � 7. The rank sum test was used tocompare the number of ischaemic regions andduration of mutism among the three groups. Therewas no significant difference between groups 1 and 2( p> 0.10); groups 1 and 2 combined were signifi-cantly different from group 3 ( p<0.05). Theseresults suggested that the duration of mutism wasprolonged when the number of ischaemic regionsexceeded seven. Statistical analysis failed to find asignificant correlation between the number ofischaemic regions either in the left or right hemi-sphere and the duration of PTM ( p¼ 0.265).
Discussion
In this study, 12 cases (75%) were due to DAI, whileanother four patients with intracranial haematoma,which had an occupying effect, also displayedsignificant multiple ischaemic brain regions afteroperation. It seems that PTM is more commonlyseen in patients with diffuse brain injury, especiallyin DAI, than in those with simple focal brain injury.
Comparing with the patients with psychogenicmutism, cerebellar mutism or akinetic mutism,almost all patients with PTM have experiencedcoma after trauma. After a coma lasting from 2–72days (average 15.5 days), the patients included inthis study suffered from PTM lasting for 2–56 days(average 11.94 days). The further statistical analysisshowed that the duration of PTM was positivelycorrelated with the duration of coma. The correla-tion of PTM with coma duration could predict afavourable, complete and rapid recovery of speecheven after many weeks of total mutism and, there-fore, support the child, his family and the nursingstaff during this distressful situation, even benefit forthe family and patient’s management.
Imaging data (CT and MRI) may give somesuggestions for the mechanism of PTM in children.However, there are still considerable argumentsabout the anatomical orientation of children withPTM and related brain regions containing cerebel-lum, callosum, thalamencephalon, diencephalons,brainstem and periaqueductal grey [4–9]. In thisstudy, CT and MRI showed diffuse brain injury in14 out of 16 patients. A punctated haemorrhagicfocus also appeared unexpectedly in early CTimaging. CT at 6 hours post-trauma in 14 childrenshowed a punctated haemorrhagic focus in the rightfrontal and temporal lobe. Encephalomalacia in thecallosum or cerebral atrophy were found by CT orMRI in some cases in the middle or late post-
Figure 1. Correlation of coma and mutism duration (days).
PTM in children 447
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Nor
th T
exas
on
11/2
1/14
For
pers
onal
use
onl
y.

traumatic period. Unfortunately, none of the aboveimaging changes were linked with the anatomicallocation of PTM. Moreover, the information derivedfrom CT or MRI images was not adequate for theunderstanding of the whole status of injured brain.Thus, this report processed SPECT for the patientsto learn the regional cerebral blood flow. SPECT ofthese patients at the same stage of disease showedmuch more severe changes than CT and MRI andeach patient had ischaemia in multiple brain regions,involving almost all the regions mentioned above.The further statistical analysis indicated that theduration of mutism was prolonged when the numberof ischaemic regions exceeded seven. The SPECTanalysis is a benefit for the prediction of PTMduration. Moreover, it was considered that theimprovement of ischaemic status of injury brainwould make better for PTM recovery, which isunder further investigation in the laboratory.
Human language function gradually develops inthe dominant hemisphere after birth. The languagecentre is less consummate in younger children. MRIand PET have shown that more than 10 brainregions are related to language function and that along time is required to build various languagenetworks, with numerous acquired language storesbeing located in the extensive brain region. Gaillaret al. [10] reported that children need to activatemore brain regions than adults to achieve the sameverbal fluency, which has the same condition in theright hemisphere in children, because of theirincomplete brain development. Thus, it is easy to
understand that in children more brain regions,including the right hemisphere, need to be involvedto complete a verbal fluency task. Three cases ofinjury mainly in the right hemisphere were observedin a sample of six children in imaging data collectedby Dayer et al. [4] Both the fMRI by Schlaggar et al.[11] and Wood et al. [12] and the cortex electricalstimulation during surgery by Stevenet et al. [13]revealed that maturation of the brain languageregion correlates significantly with age. The lefthemisphere damage was not as severe as the rightside in CT and MRI data shown in the results andthe correlation between the number of ischaemicregions in both hemispheres and the duration ofmutism was not significant ( p¼0.265). The dis-tribution of ischaemic brain regions in another studyon severe post-trauma coma adult patients revealedthat there was no significant PTM, which wasconsistent with this study [2]. The imaging data ofsix patients with PTM summarized by Dayer et al.[4] suggested that the involvement of mesencephalicstructures played a key role in the aetiology ofPTM. From these data, it is assumed that PTM inchildren may be related to their incomplete braindevelopment.
In summary, most PTM in children resulted fromdiffuse brain injury and ischaemic changes usuallyappeared in multiple brain regions. PTM durationwas correlated with coma duration. However, therelationship between PTM and damage to thelanguage centre in the dominant hemisphere wasnot significant. Although it appears that no lastingmemory or painful recollection of this situationoccurred in these patients, children with PTM mayexpress definite frustration at being unable to speak.One should be aware of this and look for alternativeways for the child to communicate in PTM duration,which will be of benefit for the future development ofthe child.
Declaration of interest: The authors report noconflicts of interest. The authors alone are respon-sible for the content and writing of the paper.
References
1. Levin HS, Madison CF, Bailey CB, Meyer CA,Eisenberg HM, Guinto FC. Mutism after closed head injury.Archives of Neurology 1983;40:601–606.
2. Wang J, Xi J, Jiang B. The research of persistent coma aftersevere head injury and brain ischemia. Chinese Journal ofNeurosurgical Disease Research 2005;4:34–36.
3. Wang J, Jiang B, Zhang M. Clinical characteristics andprognosis of 34 patients with cerebral diffuse axonal injury.Chinese Journal of Traumatology 2001;17:26–28.
Figure 2. MRI at 28 days after trauma in a 3.5-year-old child:Encephalomalacia in callosum (white arrow).
448 X. Jian et al.
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Nor
th T
exas
on
11/2
1/14
For
pers
onal
use
onl
y.

4. Dayer A, Roulet E, Maeder P. Post-traumatic mutism inchildren: Clinical characteristics pattern of recovery andclinicopathological correlations. European Journal ofPediatric Neurology 1998;2:109–116.
5. Koh S, Turkel SB, Baram TZ. Cerebellar mutism in children:Report of six cases and potential mechanisms. PediatricNeurology 1997;16:218–219.
6. Bramanti P, Sessa E, Salutari L. Posttraumatic mutism.Journal of Neurosurgical Science 1994;38:117–122.
7. Nakasu Y, Isozumi T, Nioka H, Handa J. Mechanism ofmutism following the transcallosal approach to the ventricle.Acta Neurochirgica (Wien) 1991;110:146–153.
8. Ferrara VL. Acute traumatic mutism. Surgical Neurology1985;23:573–574.
9. Grippo J, Vergel MF, Comar H. Mutism in children. Reviewsin Neurology 2001;32:244–246.
10. Gaillar WD, http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?db¼pubmed&cmd¼Search&term¼%22GaillardþWD%22%5BAuthor%5D Hertz-Pannier L, Mott SH.Functional anatomy of cognitive development: fMRI ofverbal fluency in children and adults. Neurology 2000;54:180–185.
11. Schlaggar BL, Brown TT, Lugar HM. Functional neuroa-natomical differences between adults and school-age childrenin the processing of single words. Science 2002;296:1408–1409.
12. Wood AG, Harvey AS, Wellard RM. Language cortexactivation in normal children. Neurology 2004;63:1035–1044.
13. Steven GO, Mitchel SB, Ettore L. Localization of languagefunction in children: Results of electrical stimulation map-ping. Journal of Neurosurgery 2003;98:465–470.
PTM in children 449
Bra
in I
nj D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Nor
th T
exas
on
11/2
1/14
For
pers
onal
use
onl
y.