Embed Size (px)
Citation preview

Continuous Temperature Monitoring Socks for Home Use in Patients with Diabetes and Charcot FootAlexander M Reyzelman1, DPM; Kristopher Koelewyn2, DPM; Maryam Murphy3, BS; Xuening Shen4, MS; E Yu4, BS; Raji Pillai5, PhD; Jie Fu4, BS; Henk Jan Scholten3, LLM; Ran Ma3, BSFrom 1California School of Podiatric Medicine, Samuel Merritt University, San Francisco, CA, United States, 2Northport VA Medical Center, Northport, CA, United States, 3Siren Care Inc, San Francisco, CA, United States, 4Siren Care (Shanghai) Information Technology Co Ltd, Shanghai, China, 5Medical Affairs Consulting Inc, Menlo Park, CA, United States
P5.05
ABSTRACTAim: Charcot neuroarthropathy (CN) is a progressive disease that is a severe and costlycomplication in persons with diabetic peripheral neuropathy (DPN). CN can result inhospitalization, ulceration, deformity, loss of mobility, infection, and amputation. For personswith DPN, diagnosis and monitoring of CN can be difficult. This is often due to failure torecognize the signs of the disease, or misdiagnosis due to comorbidities. Continuous temperaturemonitoring is a promising technology to assist with the early diagnosis, and monitoring of CN. Inthis report we introduce sensor-embedded socks designed for home use and daily wear, whichperform continuous temperature monitoring of the plantar surface of the foot. The aim of thisStudy[1] was to assess the accuracy of the socks, obtain user feedback on how comfortable sockswere for home use, and examine whether observed temperatures correlated with clinicalobservations for persons with CN.Methods: Temperature accuracy of the sensors was assessed prior to incorporation in the socksas well as in the completed sock design. A total of 35 patients with diabetic peripheralneuropathy (DPN), a subset of which had CN were enrolled at a single site pilot study.. Patientswith CN were provided with socks, and instructed to wear the socks continuously for 6 hoursafter which the socks could be removed, and returned to the clinic.Results: The temperatures measured by the standalone sensors were within 0.2℃ of thereference standard. For patients with CN, cases are presented that show how temperaturedifferences observed between the feet were consistent with clinical observations.Conclusions: We report the first use of wireless continuous temperature monitoring for dailywear and home use in patients with DPN and CN. The wearers found the socks to be no differentfrom standard socks. The temperature studies conducted show that the sensors used in the socksare reliable and accurate at detecting temperature, and the findings matched clinical observations.The socks serve as promising tool for the early diagnosis and monitoring of CN in patients withDPN.
BACKGROUNDAn estimated 30.3 million people in the United States (9.4% of the U.S. population) have been diagnosed with diabetes, according to the Centers for Disease Control and Prevention [2].Complications of diabetes, foot ulcers, and prognosisDiabetes damages blood vessels and nerves, particularly in the feet, and can lead to severe infections that are difficult to treat. About 25% of people with diabetes will experience a foot ulcer (DFU) in their lifetime [3, 4, 5]. When circulation is so poor that a foot ulcer fails to heal or when treatment fails to stop the spread of an infection, sepsis can result. In such cases, amputation is often necessary. Diabetes is the leading cause of lower limb amputations; DFUs precede approximately 84% of non-traumatic major amputations among people with diabetes [6, 7, 8]. The rates of recurrence of foot ulcers are very high, being greater than 40% after 1 year, and 60% within 3 years [3,9].Charcot foot, also called Charcot arthropathy, is one of the most debilitating outcomes of diabetes [10]. The condition causes increased blood flow to the foot and increased bone resorption. Immediately keeping all weight off (or off-loading) of incipient Charcot foot appears to minimize fractures and incapacitating deformities. However, there is a potential for delayed diagnosis and therapeutic intervention as plain X-rays may not show fractures at the early stages [11].
Skin temperature assessment in persons with diabetes is a valuable tool for assessing inflammation in diabetic feet, as well as its resolution [12, 13]. Home temperature monitoring has been shown to be an effective approach as an early warning system, to provide patients objective feedback so they can modify their activity and protect their foot before ulcers develop, and such monitoring is included in the International Working Group on Diabetic Foot clinical practice guidelines [14,15].
Currently available tools are designed to measure temperatures once a day or at long intervals, are for clinic use only, or include wired data transmission. Once-a-day measurements present a risk of giving false positives. Continuous monitoring allows the assessment of temperature over longer periods, taking into consideration varying levels of activity over time and thus have a greater potential to report consistent and clinically relevant temperature increases [16]. Continuous temperature-monitoring can reduce false positives and has the potential to further improve home care and early detection.
A pilot study was conducted to assess (i) how comfortable sensor-embedded socks were for daily use, and (ii) whether observed temperatures correlated with clinical observations. Illustrative cases are presented.
MATERIALS AND METHODSSensor-embedded socksThe socks are made of “smart textile”: textile with microsensors woven directly into the fabric (Siren Diabetic Socks, Neurofabric™, Siren Care, San Francisco, CA). These virtually invisible sensors are seamlessly integrated into the socks to monitor temperature changes on the bottom of the feet. The sensor-embedded socks are designed to be reusable and are machine washable and dryable.
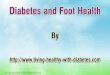
Figure 1 A. image of socks with tag (circled) containing battery, microcontroller unit and Bluetooth labeled and B. bottom of socks where sensors are located at hallux (sensor 1), metatarsal heads 1,3 and 5 (sensors 2-4), midfoot (sensor 5), and heel (sensor 6).
The sensors embedded in the socks are connected to a small tag on the sock, which encases a microcontroller unit, battery, and Bluetooth chip (Figure 1A). The 6 sensors take temperature measurements at 10-second intervals to track temperature increases at the bottom of the user's feet, at the hallux, metatarsals 1, 3 5, midfoot and heel (Figure 1B). The data are stored in the tag and sent via Bluetooth to the phone paired with each pair of socks.The smartphone app can be programmed to generate alerts when the user’s feet show temperature increases that that could be a warning sign of a potential ulcer. (Figure 2). In this study, the smartphone app displayed temperature readings to the user, but alerts were not generated.
Figure 2. Typical workflow for sensor-embedded socks
Assessment of accuracy of sensor-embedded socks sensors in detecting temperature, and User Experience.Please see Poster P15.01 for methods and results.
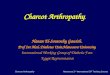
CASE STUDY 1Patient 30 (Study Group 2) is a 63-year-old male diagnosed with type 2 diabetes at 45 years of age. He has a history of ulcers and was diagnosed with Charcot arthropathy of the right foot at 57 years of age. Intake photographs (see Figure 2) and examination showed Charcot of the right foot with a collapsed midfoot.
Figure 2. Digital photograph of patient 30’s feet shows Charcot of the right foot
REFERENCES1. Reyzelman AM, Koelewyn K, Murphy M, Shen X, Yu E, Pillai R, Fu J, Scholten HJ, Ma R.
Continuous Temperature-Monitoring Socks for Home Use in Patients With Diabetes: Observational Study. J Med Internet Res. 2018 Dec 17;20(12):e12460.
2. Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2017. Atlanta, GA: Centers for Disease Control and Prevention, U.S. Dept of Health and Human Services; 2017.
3. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med 2017 Jun 15;376(24):2367-2375. PMID: 28614678
4. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA 2015 Jan 12;293(2):217-28. PMID: 15644549.
5. Armstrong DG, Lavery LA, Harkless LB, Van Houtum WH. J Am Podiatr Med Assoc. 1997 Jun;87(6):255-9. PMID: 9198345.
6. Lazzarini PA, Clark D, Derhy PH. What are the major causes of lower limb amputations in a major Australian teaching hospital? The Queensland Diabetic Foot Innovation Project, 2006 –2007. J Foot Ankle Res. 2011; 4(Suppl 1): O24. doi:10.1186/1757-1146-4-S1-O24
7. Barshes NR, Sigireddi M, Wrobel JS, Mahankali A, Robbins JM, Kougias P, Armstrong DG. The system of care for the diabetic foot: objectives, outcomes, and opportunities. Diabet Foot Ankle. 2013. PMID: 24130936.
8. Lazzarini PA, Pacella RE, Armstrong DG, van Netten JJ. Diabetes-related lower-extremity complications are a leading cause of the global burden of disability. Diabet Med. 2018 May 23. PMID: 29791033
9. Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. Lancet. 2005 Nov 12;366(9498):1719-24. PMID: 16291066
10. Lavery LA, Peters EJ, Armstrong DG. What are the most effective interventions in preventing diabetic foot ulcers? Int Wound J. 2008 Jun;5(3):425-33. PMID: 18593392.
11. Chantelau E. The perils of procrastination: effects of early vs. delayed detection and treatment of incipient Charcot fracture. Diabet Med. 2005 Dec;22(12):1707-12. PMID: 16401316.
12. Lavery LA, Higgins KR, Lanctot DR, Constantinides GP, Zamorano RG, Athanasiou KA, Armstrong DG, Agrawal CM. Preventing diabetic foot ulcer recurrence in high-risk patients: use of temperature monitoring as a self-assessment tool. Diabetes Care. 2007 Jan;30(1):14-20. PMID: 17192326.
13. van Netten JJ, Prijs M, van Baal JG, Liu C, van der Heijden F, Bus SA. Diagnostic values for skin temperature assessment to detect diabetes-related foot complications. Diabetes Technol Ther. 2014 Nov;16(11):714-21. PMID: 25098361.
14. Hazenberg CE, van Netten JJ, van Baal SG, Bus SA. Assessment of signs of foot infection in diabetes patients using photographic foot imaging and infrared thermography. Diabetes Technol Ther. 2014 Jun;16(6):370-7. PMID: 24690146
15. International Working Group on the Diabetic Foot. IWGDF Guidance on the prevention of foot ulcers in at-risk patients with diabetes. 2015.
16. Bus SA. Innovations in plantar pressure and foot temperature measurements in diabetes. Diabetes Metab Res Rev. 2016 Jan;32 Suppl 1:221-6. PMID: 26467347.
Figure 4. Digital photograph of patient 3’s feet shows Charcot of the right foot
Assessment of sensor-embedded socks worn by Patients with Diabetes.A single-site study was conducted under an IRB-approved protocol to evaluate the usability of the smart socks for patients with diabetic peripheral neuropathy (DPN). Informed consent was obtained from all patients.
Thirty-five (35) patients 18 years of age and older from a private clinical practice were enrolled into three (3) groups, based on patient reported medical history and/or medical documents. Group 1: subjects with DPN and no previous history of ulcers, n=11 Group 2: subjects with DPN and a previous history of ulcers, n=13 Group 3: subjects with DPN and a current pre-ulcer as determined by the investigator, n=11.
Group 1 Group 2 Group 3 Overall
Female | Male 5 | 6 4 | 9 1 | 10 10 | 25
Avg age 55 61 63 59
Avg age DM Dx (years)
46 43 44 44
Avg length DM (years)
9 18 19 15
DM1 | DM2 0 | 11 0 | 13 2 | 9 2 | 33
Subjects participated in two clinic visits. In the first visit, screening procedures were conducted which included the following: a general physical exam performed by a board-certified podiatrist, visual foot inspection, digital photographs of both feet, and medical history intake. Subjects were provided with the socks and were given an Android smartphone with the application needed for temperature monitoring. The socks were wirelessly connected with the smartphone via Bluetooth. The patients were instructed to wear the socks continuously for 6 hours after which the socks could be removed. The data was streamed via Bluetooth directly to the Android application installed on the phone provided to the patient during the screening/initiation visit. All data was stored in the sock tag and sent to the phone paired to the socks (via Bluetooth) assigned to the enrolled patient.
At the second or end-of-study visit to the clinic, 7 days + 2 days from the screening/initiation visit, the socks were returned to the investigator and the patient was examined for potential adverse reactions. An exit questionnaire was completed to obtain usability information from the patient on the comfortability of sock, ease of Android application use, and practicality of integrating this specific system into the patient’s everyday life. Upon exit from the trial, data was exported from the Android phone to a secure laptop for analysis. All data collected was de-identified and only subject numbers were used for the duration of the trial.
Table 1.Distribution of patients included in the study by age, sex and years with diabetes.
RESULTSThree Case Studies of Patients with Charcot Foot are presented below.
CASE STUDY 3Patient 26 (Study Group 2) is a 40-year-old female diagnosed with type 2 diabetes at 29 years of age. She has a history of ulcers and was diagnosed with Charcot arthropathy of the right foot at 37 years of age, and underwent surgery for Charcot deformity a few months earlier, and left foot 2nd digit amputation 4 years earlier. Intake photographs (see Figure 6) and examination showed Charcot of the right foot with a right plantar midfoot ulcer that was recently healed .
Figure 6. Digital photograph of patient 3’s feet shows Charcot of the right foot
CONCLUSIONSIn this pilot study of 35 patients temperature data were collected for 24 hours in the patients shown here. These patients were not enrolled specifically because they had Charcot, though this condition was marked on their intake form. Upon review of their data, even in this time, a pattern in Charcot patients that were similar to each other and distinct from the non-Charcot patients was observed. The pattern is a diffuse temperature elevation across the whole foot that approaches the 2.2℃/4℉ threshold, but does not necessarily exceed it. Basically the whole foot becomes warmer, but not always above the threshold.
This was an unexpected result of the study and merits further research. A study over a longer period of time (12 months) with a specific subset of Charcot patients is under way to see if active and inactive Charcot foot shows different temperature patterns when compared with non-Charcot diabetic foot.
Charcot is a dangerous complication of diabetes that can be difficult to diagnose for people living with diabetes and neuropathy. This is often due to failure to recognize the signs of the disease, or misdiagnosis due to co-morbidities including gout and osteomyelitis. During the acute stage of Charcot Foot, there may be difficulty of diagnosis due to confusion with infection, gout, or rheumatoid arthritis. But, early diagnosis and treatment of CN is key for improved outcomes. Continuous temperature monitoring may be a useful tool for early identification of the active or acute stage of Charcot.
Discussion: Similar to the other case studies, a diffuse temperature elevation across the foot is observed which approaches but not necessarily exceeds the 2.2℃/4℉ threshold. The increase temperature difference during the day and the decrease toward the end of the day could potentially be linked to increased and decreased levels of activity during those parts of the day.
Patient 3 wore the sensor-embedded socks for 12 hours, during which period the right foot was consistently warmer than the left foot (Fig 7). The delta increases during the day, potentially caused by increased activity. The right hallux, and MTP-1 were elevated more than 2.2℃/4℉. A change in delta is seen when the patient took off their shoes, and was only wearing a left shoe for a while.
Figure 7. Each line on the graph shows a moving average of the temperature difference (i.e. Left foot temperature – Right foot temperature) for metatarsal heads 1, 3 and 5 (light blue, dark blue, orange respectively) heel (gray), arch (yellow), and hallux (green). The lines span the period the socks were worn, with time shown on the x-axis. The dotted red lines shows the 2.2℃temperature threshold for the left (upper line) and right foot (lower line).
Patient 30 wore the sensor-embedded socks for 8 hours, during which period the right foot was consistently warmer than the left foot. The temperature on the right hallux, MTP-1, MTP-3, MTP-5, and arch was elevated more than 2.2℃/4℉, upto 8℃. (Fig 3).
Figure 3. Each line on the graph shows a moving average of the temperature difference (i.e. Left foot temperature – Right foot temperature) for metatarsal heads 1, 3 and 5 (light blue, dark blue, orange respectively) heel (gray), arch (yellow), and hallux (green). The lines span the period the socks were worn, with time shown on the x-axis. The dashed and dotted red line shows the 2.2℃temperature threshold for the left and right foot respectively.
CASE STUDY 2Patient 3 (Study Group 2) is a 69-year-old male diagnosed with type 2 diabetes at 47 years of age. He has no history of ulcers and was diagnosed with Charcot arthropathy of the right foot at 57 years of age. Intake photographs (see Figure 6) and examination showed Charcot of the right foot with a collapsed midfoot, and no pre-ulcerative lesion.
Patient 3 wore the sensor-embedded socks for 5 hours, during which period the temperature on the entire right foot was elevated, and the right MTP-1 was elevated more than 2.2℃/4℉, upto6oF. (Fig 5).
Figure 5. Each line on the graph shows a moving average of the temperature difference (i.e. Left foot temperature – Right foot temperature) for metatarsal heads 1, 3 and 5 (light blue, dark blue, orange respectively) heel (gray), arch (yellow), and hallux (green).The lines span the period the socks were worn, with time shown on the x-axis. The dotted red lines shows the 2.2℃temperature threshold for the left (upper line) and right foot (lower line).
Discussion: In this patient, a diffuse temperature elevation across the whole front of the right foot is observed. Basically the whole right foot is warmer than the let foot. The increase and decrease in elevation could potentially be linked with increased and decreased activity.
Discussion: Similar to case study 1, a diffuse temperature elevation is seen across the whole of the foot with Charcot. The right foot is warmer than the left, but the elevation does not necessarily cross the 2.2℃/4℉ threshold.