Embed Size (px)
Citation preview

Journal of Surgical Oncology 23:263-268 (1983)
Postoperative Radiation Therapy for Muscle- Invading Bladder Carcinoma
GENE KOPELSON, MD, AND JOHN A. HEANEY, MD
From the Departments of Therapeutic Radiology and Urology, Tufts University School of Medicine and Tufts-New England Medical Center, Boston
~~ ~
From 1974- 1980, 15 patients with pTz-4 bladder carcinoma received adjuvant postoperative radiation therapy (XRT) . The extent of initial surgery varied (six radical cystectomy, 5 partial cystectomy, four “total” transurethral resection). The planned XRT was 4,000-5,040 rads in 5-6 weeks to the pelvis (achieved in 14/15 patients) followed by a bladder boost in noncystectomized patients (achieved in W9). Survival at two years and five years was 54% (7/13 patients) and 27% (3/11 patients), respec- tively. Local-regional disease control (minimum two-year follow-up) was achieved in 7/11 (63%). Of seven patients alive at least two years later, small bowel complications (chronic diarrhea, obstruction) occurred in two; these latter patients each had had radical cystectomy. Adjuvant postoperative XRT may be useful in the multimodality management of patients with bladder carcinoma, especially those identified as high risk after pathologic staging and initial surgery. The poor regional control rate and relatively high incidence of complications seen in this and previous studies suggest that improved radiation technique is needed, both to ensure adequate coverage of the volume at risk and to minimize complications. Representative portals are shown to illustrate these features.
KEY WORDS: bladder neoplasms, radiotherapy
INTRODUCTION Major controversy continues in the uro-oncologic lit-
erature as to the value of preoperative radiation therapy for invasive bladder carcinoma. Although preoperative irradiation has several theoretical advantages over post- operative irradiation, the latter has improved regional disease control rates in other pelvic cancers such as rectum and rectosigmoid [1,2], uterus [3], and cervix
There is scant literature on the role of postoperative radiation therapy for high-risk bladder cancer patients, and the present review was undertaken to assess the results of such management in terms of disease control and complications.
MATERIALS AND METHODS From 1974-1980, 15 patients with muscle-invading
bladder carcinoma received adjuvant postoperative radia- tion therapy. Excluded were patients with gross disease left behind at the time of surgery or those without patho-
0 1983 Alan R. Liss, h e .
[41.
logic proof of muscle invasion. There were 11 men and four women, their age at diagnosis ranging from 50-83 years with a median of 68. Thirteen had transitional cell carcinoma and two had squamous cell carcinoma; all tumors were poorly differentiated except for one ( P T ~ ~ ) which was moderately well-differentiated. The extent of preirradiation surgery and pathologic stage appear in Table 1.
Transurethral resection removed all gross tumor in four patients; although some authors would include these patients in a “primary radiation” series, we elected to define them “adjuvant postoperative” as described by Miller [5]. Extraperitoneal partial cystectomy was done in five patients and was associated with negative margins in each; one of these patients had a lymph node dissection with negative (0/11) nodes, and another had a normal
Accepted for publication December 6, 1982. Address reprint requests to G . Kopelson, MD, Dept. Radiation On- cology, Salem Hospital, 81 Highland Avenue, Salem, MA 01970.

264 Kopelson and Heaney
TABLE I. Extent of Surgery and Pathologic Stage
Transurethral Partial Radical resection cystectomy cystectomy
Pathologic T2 2 0 1 T-stage" T3a 1 2 0
TBh 1 3 2 T4a 0 0 3 T4 b 0 0 0
"All patients had No and N, status except one patient, who had p T3hNI disease (see text).
lymphangiogram. Radical cystectomy and ileal conduit was done in six patients; additional lymph node sampling or dissection was performed in five and urethrectomy in two. Four of these patients had pNo status while 1 patient (with a pT3b tumor) had a single external iliac nodal metastasis (N,).
Postoperative irradiation was begun 1-3 months post- operatively for 12/15 patients; one patient began treat- ment at 27 days postoperatively, and two began more than three months later. Pelvic treatment was delivered via %o (five patients) or a Brown-Boveri 45-MeV Be- tatron (ten patients). Anterior-posterior parallel-opposed fields were used in 14 patients; one had a four-field "box" technique. Planned pelvic irradiation of 4,000- 5,040 rads in 180-200-rad fractions was administered to 14/15 patients. In one patient treatment was stopped at 1,980 rads due to acute gastrointestinal side effects (see below),
For the six patients irradiated after radical surgery, shaped (ie, corner blocks) fields were used in three. Review of descriptions of the treatment setups revealed that in two, the scar was boosted anteriorly with bolus and/or an electron field. The ileal loop stoma was care- fully blocked from the anterior field in two patients also.
For the remaining nine noncystectomized patients, similar pelvic fields were used initially. A small field was then used (usually via rotational techniques) to boost the bladder in 819 patients to the following doses: 5,000- 5,550 rads, two patients; 5,500-6,OOO rads, three pa- tients; 3 6,000 rads, four patients. In one patient, low- dose preoperative irradiation (500 rads x 1) was given immediately prior to partial cystectomy .
It should be noted that this group of patients represents a small minority of the irradiated bladder cancer patients seen over this time period. It is a heterogeneous popula- tion mainly comprising cases originating outside this medical center who were referred here for postoperative irradiation.
No patient received adjuvant chemotherapy.
RESULTS Survival at two years and five years was 54% (7/13
patients) and 27% (3/11 patients), respectively. Adv-
TABLE 11. Absolute Survival Rates
2-year 5-year
PT2 1/3 013 pT-stage PT3 417 215
PT4 2/3 1 / 3 Total 7113 (54%) 3/11 (27%)
TABLE 111. Failure Patterns (Minimum 2-Year Follow-up)+
Sites of failure No. of oatients
Local-regional only 2 Distant only 2 Both 2 Neither 5 Unknown 2
'Total local-regional disease control rate in patients with known sites of failure 7/11 (63%).
TABLE IV. Complication Rate (Minimum Two-Year Follow-up)
Pelvic dose (rads) Extent of surgery 4,OO0-5,040
Transurcthral resection Partial cystcctomy Radical cvstectoniv
- 014 213
anced pathologic (pT) stage did not preclude prolonged survival (Table 11). Of the six patients who had radical cystectomy, four are alive and well more than 12 months later (one at 74 months); one died of a myocardial infarc- tion with coexistent distant metastases at 37 months, and the other patient died of regional and distant disease at 43 months. The other long-term survivors had partial cystectomy with pelvic irradiation and bladder boost.
Local-regional disease control was achieved for seven of 11 control patients (63%) in whom sites of failure are known (Table 111).
Two patients developed complications (chronic diar- rhea, one patient; nonfatal small bowel obstructions re- quiring multiple surgical procedures, one patient). The complications occurred after moderate dose pelvic irra- diation (4,OOO-5,040 rads) and radical surgery (Table IV) .
DISCUSSION It is recognized that either radical surgery with or
without preoperative irradiation or radical irradiation with salvage cystectomy are used to manage the majority of muscle-invading bladder cancers. Although the addition of postoperative irradiation to radical surgery has re- sulted in improvements in regional control rates of rec- tosigmoid, uterine, and other pelvic cancers, there is little information concerning this combination in bladder

TA
BL
E V
. Reo
orte
d E
xwri
ence
With
Pos
tow
rativ
e Ir
radi
atio
n fo
r B
ladd
er C
arci
nom
a
Irra
diat
ion
dose
(rad
s)
Surv
ival
rate
-
Initi
al
Ref
eren
ce
surg
ery
Preo
p
Cum
min
gs et
al [
101
Segm
enta
l
Dre
tler e
t al 1
121
Rad
ical
-
Mill
er 1
51
Var
ious
-
rese
ctio
n
cyst
ecto
my
Moh
iudd
in
Var
ious
50
0
Mul
ler e
t al [
6,7]
V
ario
us
-
Skin
ner e
t al [
6,7]
R
adic
al
1,60
0
Kop
elso
n an
d V
ario
us
500
in
et a
l [9
]
cyst
ecom
y
Post
op
3-Y
ear
5-ye
ar
5 ,00
0 -
9/31
(2
9%)
Uns
peci
fied
-
1/3
(33%
)
1012
4 (4
0%)
-
6,00
0
4.50
0 a
5,00
0-6,
000
45/1
34 (
34%
) 30
1112
(26
%)
-
-
3 ,OO
o
4,00
0-5,
040
7/13
'(54%
) 3/
11
(27%
) H
eane
v (m
esen
t)
one
case
+
boos
t
Reg
iona
l C
ompl
icat
ion
dise
ase
rate
co
ntro
l rat
e C
omm
ents
-
-
(25 %
) (6
7%)
14/9
2 (1
5%)
47/4
8 (9
8%)
-
-
9/20
(45
%)
-
2/7
(29%
) 7/
11 (
63%
)
Var
ious
pT-
stag
es; d
ata
is fo
r gra
de 1
11-IV
tum
ors
pN-p
ositi
ve p
atie
nts
Surv
ival
dat
a fo
r B,-
D,
patie
nts;
com
plic
atio
n an
d di
seas
e co
ntro
l rat
es
are
for
all p
atie
nts
irrad
iate
d po
stop
erat
ivel
y (i
e, o
f al
l pT
stag
es)
Var
ious
pT-
stag
es
"Hi g
rade
B, 6
5%; B
2 67
%; C
57%
. All
are
4-ye
ar s
urvi
val r
ates
. 'T
wo-
year
sur
viva
l (se
e te
xt).
W
a
P
t
q

266 Kopelson and Heaney
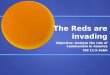
Fig. 1 . A 60-year-old man with pT4aNo grade 111 transitional cell carcinoma S/P radical cystectomy-urethrectomy with lymph node sampling. The tumor invaded the distal ureter and seminal vesicles in addition to the prostate. The whole pelvis received 4,500 rads in 26 fractions via these shaped AP-PA portals on the Betatron; the stoma was blocked anteriorly (A). At 2 years 10 months after completion of
irradiation, pelvic recurrence occurred, causing bilateral hydrone- phrosis necessitating percutaneous nephrostomy . Computerized tom- ogram (B) revealed recurrent tumor mass (small arrowheads) in relation to stoma (large arrowhead), which had been previously blocked during AP-PA fields.

cancer. Our experience along with that of others suggests that selected patients may benefit from adjuvant postop- erative irradiation and enjoy local control and long-term survival despite high stage (pT) local disease-Table V summarizes available data [5-121.
While the present series is preliminary and based upon few patients, it is the only report in which each of the following are known: (1) all patients had pT24 diseases, (2) the extent of surgery is specified, (3) irradiation dose and technique is stated, and (4) local-regional control, survival, and complication rates are given.
Although the data from this very small series of pa- tients cannot prove the efficacy of postoperative irradia- tion, they, along with those from previous series shown in Table V, do demonstrate that postoperative irradiation can be followed by long-term survival in high-risk pa- tients. While radical cystectomy with or without preop- erative irradiation is still considered the mainstay of therapy for most patients with muscle-invading bladder carcinoma, it is clear that some of these patients also can be cured by the combination of local excision (transure- thral resection or partial cystectomy) and postoperative radiotherapy.
Primary bladder carcinoma directly invades the pros- tate in 12-20% [13,14], the urethra in 4-8% [15,16], and the seminal vesicles in 15% [13] of patients with pT2-4 bladder carcinoma. Although such pT4, disease has been classically associated with a poor prognosis [ 14,15,17], occasional cures following postoperative irradiation, as documented by this report and other series [ 141, support its use in this setting. Patients with muscle-invading blad- der carcinoma who do not have urethrectomy with cys- tectomy may be suitable candidates for postoperative irradiation as up to 10% may otherwise die of local recurrence in the region of the retained urethra [ 181.
Poor survival has been described for patients with pelvic node metastases which have been documented either lymph-angiographically (cN +) or pathologically (pN+) [19-211. However, few patients die of recurrent pelvic cancer, the majority developing bone and lung metastases which were probably present at the time of primary therapy-thus nodal involvement signifies that tumor resides in distant sites [21]. However, local ther- apy can lead to long survival. At Massachusetts General Hospital from 1955- 1967, 35 patients were pN + at rad- ical cystectomy [12]. Of 32 not given postoperative irra- diation, five (15%) survived five years, while one of three given irradiation had similar survival. At New York Hospital, 10 of 103 (9.5%) patients who were pN+ survived five years-some of these were irradiated [22]. Other series show survival of pN+ patients to vary between 5% and 36% [6,21,23,29]. In our series, the single pN+ patient had a T3b tumor and is alive and well seven months after 5,040 rads delivered to the pelvis in 180-rad fractions.
Postoperative Bladder Carcinoma Irradiation 267
Most pN+ patients have T3 or T4 tumors [12,19-21, 291, and thus postoperative pelvic irradiation may be expected to increase regional control and perhaps sur- vival rates also. As nodal disease may be a signal of diffuse micrometastatic disease, adjuvant chemotherapy should be considered in this patient population [24].
Pooled data from four series reveals that of 236 various stage patients who had five-year follow-up after partial cystectomy or segmental resection but without postoper- ative irradiation [ 10,ll , 25,261, only seven (3 %) devel- oped a wound recurrence, although others report an incidence of 25% [24]. Coverage of the entire scar can be difficult; and because scar recurrences postirradiation have been noted after doses in excess of 5,000 rads [27], the scars of these patients might be treated postopera- tively with 5,500 rads.
Complication rates after postoperative irradiation vary with the extent of disease, types of surgery, and irradia- tion dose and field size (Table V). The high rate of small bowel complications after radical surgery and irradiation (2/3, Table IV) supports the suggestion that the combi- nation of these modalities increases the complication rate compared to either modality alone [5-7,281.
When irradiation follows intraperitoneal surgery, it ap- pears to increase the risk of small bowel complications over that following extraperitoneal surgery. Small bowel may become fixed in the pelvis after transperitoneal sur- gery and, in order to spare more normal tissue, four shaped fields could be used to treat the pelvis rather than typical unshaped anterior-posterior fields used for most of the patients in the present series. Although sparing of the stoma is recommended, such a block, when only anterior-posterior fields ?re used, can led to an infield recurrence (Fig. 1). By the use of four fields, however, the stoma site can be spared without sacrifice of dose to the volume at risk.
CONCLUSION This report, though based on only a few patients,
suggests that occasional long-term survival can be achieved for patients with pT24 bladder carcinoma who re- ceive postoperative irradiation. By the use of careful ra- diation therapy portal planning, complications can theo- retically be kept at a reasonably low level. Further study of adjuvant postoperative irradiation is justified for high- risk patients with muscle-invading bladder cancer in those institutions not advocating adjuvant preoperative irradia- tion.
ACKNOWLEDGMENTS The authors would like to thank Mindy, Charles, and
Barry Kopelson for their help in preparation of this pa- per.

268 Kopelson and Heaney
1.
2.
3 .
4.
5. 6.
7.
8.
9.
10,
11.
12.
13.
REFERENCES
Hoskins B, Gunderson L, Dosoretz D, Galdabini J: Adjuvant postoperative radiotherapy in carcinoma of the rectum and rec- tosigmoid (Abstr). Int J Radiat Oncol Biol Phys 6 : 1379, 1980. Withers HR, Romsdahl MM. Saxton JP: Postoperative radio- therapy for cancer of the rectum and rectosigmoid (Abstr). Int J Radiat Oncol Biol Phys 6: 1380, 1980. Goodman R, Hellman S: The role of postoperative irradiation in carcinoma of the endometrium. Gynecol Oncol 2:354-361, 1974. Guttman R: Significance of postoperative irradiation in carci- noma of the cervix: A ten year study. Am J Roentgenol 108: 102- 108, 1970. Miller L: Bladder cancer. Cancer 39:973-980, 1977. Skinner DG, Kaufman JJ, Tift JP: Experience with high dose, short course, preoperative radiation therapy and immediate sin- gle stage cystectomy in management of bladder cancer: A pre- liminary report. Trans Am Assoc Genitourin Surg 70: 113-118, 1979. Skinner DG, Crawford ED, Kaufman JJ: Complications of rad- ical cystectomy for carcinoma of the bladder. J Urol 123:640- 643, 1980. Miiller RP, Schertel L, Frohler H; Zur klinik und strahlenther- apie der harnblasemnalignome. Strahlentherapie 156:223-227, 1980.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
Mohiuddin M, Kramer S, et al: Combined pre- and postoperatic 25, adjuvent radiotherapy for bladder career-an update (Abstr.) Int J Radiat Oncol Biol Phys 8(s-1): 123, 1982. Cummings KB, Mason JT, Correa RJ, Gibbons RP: Segmental resection in the management of bladder carcinoma. J Urol
Utz DC, Schmitz SE, Fugelso PD, Farrow GM: A clinicopath- ologic evaluation of partial cystectomy for carcinoma of the urinary bladder. Cancer 32: 1075-1081, 1973. Dretler SP, Ragsdale ED, Leadbetter WF: The value of pelvic lymphadenectomy in the surgical treatment of bladder cancer. J Urol 109:414-416, 1973. 29. Melicow MM: Tumors of the bladder: A multifaceted problem. J Urol I12:467-478, 1974.
26.
119~56-58, 1978. 27.
28.
Schellhdmmer PF, Bean MA, Whitmore WF Jr: Prostate in- volvement by transitional cell carcinoma: Pathogenesis, patterns and prognosis. J Urol 118:399-403, 1977. Schellhammer PF, Whitmore WF Jr: Transitional cell carcinoma of the urethra in men having cystectomy for bladder cancer. J Urol 115:56-60, 1976. Cordonnier JJ, Spjut HJ: Urethral occurrence of bladder carci- noma following cystectomy. J Urol 87:398-400, 1962. Whitmore WF Jr, Marshall WF: Radical total cystectomy for cancer of the bladder. J Urol 87:853-860, 1962. Wallace DM: Cited by Laskowksi TZ, Scott R Jr, Hudgins PT: Combined therapy: Radiation and surgery-Treatment of blad- der cancer. J Urol99:733-740. Rodger A, Wild SR, Duncan W: Bipedal lymphography in the management of bladder cancer. Clin Radio1 3 1 :555-558, 1980. Turner AG, Hendry WF, MacDonald JS, Wallace DM: The value of lymphography in the management of bladder cancer. Br J Urol48:579-586, 1976. Smith JA Jr, Whitmore WF Jr: Regional lymph node metastases from bladder cancer. J Urol 126591-593, 1981. LaPlante M, Brice M: The upper limits of hopeful application of radical cystectomy for vesical carcinoma: Does nodal metas- tasis always indicate incurability? J Urol 109:261-264, 1973. Whitmore WF: Integrated irradiation and cystectomy for blad- der cancer. Brit J Urol 52: 1-9, 1980. Skinner DG: Current perspectives in the management of high- grade inyasive bladder cancer. Cancer 45: 1866-1874, 1980. Brannan W, Ochsner MG, Fuselier HA, Landry GR: Partial cystectomy in the treatment of transitional cell carcinoma of the bladder. J Urol 119:213-214, 1978. Peress JA, Waterhouse K, Cole AT: Complications of partial cystectomy in patients with high grade bladder carcinoma. J Urol 118:761-762, 1977. Shipley WU: Postoperative irradiation. Presentation for the American Society of Clinical Oncology, 1981 meeting. Sullivan JW, Grabstald H, Whitmore WF Jr: Complications of ureteroileal conduit with radical cystectomy: Review of 336 cases. J Urol 124:797-801, 1980. Skinner DG: Management of invasive bladder cancer: A reticu- lous pelvic node dissection can make a difference. J Urol 128:34- 38, 1982.