Embed Size (px)
Citation preview

Integration of Immunotherapy Across the Spectrum of Lung Cancer
Karen Kelly, MDProfessor of Medicine
Associate Director for Clinical ResearchJennifer Rene Harmon Tegley and Elizabeth Erica Harmon
Endowed Chair in Cancer Clinical ResearchUC Davis Comprehensive Cancer Center

Objectives
1.Review the current status of immunotherapy
2. Identify determinants of response
3.Discuss strategies to enhance efficacy

Patient achieved a PR but 4 months later a surveillance scan revealed liver metastases. His sister is a nurse and they want to know about immunotherapy.
Case PresentationDW is a 54-year-old white male with a T2aN3M0, Stage III-B squamous carcinoma of the left lung diagnosed in December 2013. The patient received concurrent chemoradiation therapy with weekly pacltaxel and carboplatin followed by two cycles of full dose paclitaxel + carboplatin.
PMH: Type II DM, HTN, COPD, sleep apneaSH: Former smoker quit in 2008; 30 pack yearsPE: Mildly obese WM; PS 0

I informed the patient that an immune checkpoint inhibitor (ICI) was not FDA approved. I evaluated him for an ICI clinical trial but he was ineligible due to lack of tissue and he was too anxious to wait for a biopsy to be performed and analyzed.
What would you recommend?1.Gemcitabine and carboplatin2.Docetaxel3.Docetaxel and ramicirumab4.Gemcitabine5.RFA to the two liver lesions
Case Presentation

The patient was treated with docetaxel for 4 cycles and progressed in the liver with multiple new lesions. He underwent a liver biopsy and was placed on a phase I trial of an PDL-1 inhibitor. He is s/p 2 cycles with a MR
Case Presentation

Basic Immunology The innate response is the rapidrecognition and eradication of invading pathogens (macrophages, monocytes, eosinophils, NK cells) and soluble mediators (activation of the complement cascade and acute phase reactants)
Activation of the innate response triggers the expression of costimulatory molecules and cytokines that allows for the specific adaptive response by cellular (T and B cells) andhumoral elements.
Activation requires antigenic fragments be presented by MHC to antigen specific receptors on cytotoxic (CD8) T cells
Ploegh HL Cancer Immunol Res 1:5-10; 2013; Ploegh HL Science 280 248-253, 1998

History of Immunotherapy in Lung Cancer
1970 1980 1990 2000 2010
CALGBLS-SCLC
Chemo XRT ± BCG
MAGRITStage 1B-III
Adj MAGE-A3 vs. Placebo
SWOG LS-SCLC
Maintenanceα Interferon
vs. OBS
LCSG 771Stage I NSCLC
Adj BCGvs. Placebo
STARTStage III NSCLCAdj Tecemotide
vs. Placebo
START2Stage III NSCLCAdj Tecemotide
vs. Placebo
SILVALS-SCLC
Maint Bec2/BGGvs. Observation
Randomized Phase III Trials
1970 1980 1990 2000 2010

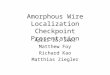
Cancer Immunity Cycle
Chen DS, et al. Immunity. 39:1-10, 2013.

T Cell Targets For ImmunoregulatoryAntibody Therapy
Mellman I et al. Nature: 480: 480-9, 2011

Immune Checkpoint Inhibitors
T cell death
Sznol M et al Clin Can Res 19:1021-1034, 2013

†at clinically relevant doses
IgG1 wtCuretech Anti-PD-1
ADCC intact Potential to deplete activated T
cells and TILs and diminish activity
Blocks PD-1/PD-L2 interaction in lungs
Potential for autoimmune pneumonitis
IgG4 hinge mutantBMS Anti-PD-1Merck Anti-PD-1
40% reduced ADCC† Potential to deplete activated T
cells and TILs and diminish activity
Blocks PD-1/PD-L2 interaction in lungs
Potential for autoimmune pneumonitis
IgG1 EngineeredGenentech Anti-PD-L1
MedI-4736
No ADCC† Decreased potential to deplete
activated T cells and TILs
Leaves PD-1/PD-L2 interaction intact in lungs
Decreased potential for autoimmune pneumonitis
Blocks PD-L1/B7.1 interaction Potential for enhanced priming
Examples:
Courtesy of Dr. Herbst
Comparison of Therapeutic Antibodies Blocking PD-1/PDL-1 Interaction

Safety, Activity, and Immune Correlates of Anti–PD-1 Antibody in Cancer
Topalian SL, Hodi FS, Brahmer JR, Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD, Sosman JA, Atkins MB, Leming PD, Spigel DR, Antonia SJ, Horn L, Drake CG, Pardoll DM, Chen L, Sharfman WH, Anders RA, Taube JM, McMiller TL, Xu H, Korman AJ, Jure-Kunkel M, Agrawal S, McDonald D, Kollia GD, Gupta A, Wigginton JM, Sznol M.
Tumor Type (dose, mg/kg)
No. Pts OR (CR/PR)No. Pts (%)
SD 24 wkNo. Pts (%)
PFS (mos,median)
NSCLC(1-10)
129 22 (17) 13 (10) 2.3
MEL(0.1-10)
107 33 (31) 7 (7) 3.7
RCC(1 or 10)
34 10 (29) 9 (27) 7.3

Anti-tumor activity consistent across the drug class
Immune Checkpoint Inhibitors
Agent N RRN (%)
NSCLC
Nivolumab1 129 22 (17)
MK-34752,3 33129
7 (21)25 (19)
MPDL3280A4 53 12 (23)
BMS 9365595 49 5 (10)
MEDI-47366 6 3/6 (50)
1Brahmer et. al. WCLC, 2013, 2Garon et. al. WCLC 2013, 3Ghandi et. al. AACR 2014, 4Horn et. al. WCLC 2013, 5Brahmer et. al. NEJM 2012, 6 Khleif et. al. WCLC 2013

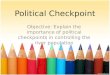
Characteristics of Responses in NSCLC Patients Treated With Nivolumab
Time to and duration of response while on treatment
Time to responseOngoing response
Response duration followinglatest reported dose of therapy
Time (week)0 16 32 48 64 80 96 112 128 144 160
Squamous
Non-squamous
• Response occur within 8-12 weeks (black dot)
• Responses occur in nonsquamous and squamous histology
• Responses can last after agent has been discontinued (red bar)
Brahmer J et al. J Thorac Oncol 2013; 8(2s), abstr MO18.03, S365

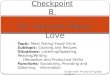
OS by Nivolumab Dose in NSCLC Patients
Censored
0 6 12 18 24 3027211593 33 36 42 48 5439 45 51 57
2-year OS Rate 45% (9 patients at risk)
1-year OS Rate 56% (17 patients at risk)
0
10
20
30
40
50
60
70
80
90
100
OS
(%)
Months Since Treatment Initiation
Group Median OS, mo (95% CI)
1 mg/kg 9.2 (5.3, 11.1)
3 mg/kg 14.9 (7.3, –)
10 mg/kg 9.2 (5.2, 12.4)
ORR was 3%, 24.3% and 20.3%, respectively for nivolumab 1, 3, and 10 mg/kg doses, respectively
Rizvi et al. LALC Meeting 2014

Mechanism of Action
CD8+ T cells Activation of cytotoxic T cells Increased γ interferonHerbst RS et al. Nature 515: 563-7, 2014

Phase II Trial: Immune Checkpoint Inhibitor
Ramalingam S et al. CMSTO, 2014

Phase II Trial: Immune Checkpoint Inhibitor
Ramalingam S et al. CMSTO, 2014

Phase II Trial: Immune Checkpoint Inhibitor
Ramalingam S et al. CMSTO, 2014

Phase II Trial: Immune Checkpoint Inhibitor
Ramalingam S et al. CMSTO, 2014

Phase II Trial: Immune Checkpoint Inhibitor
Ramalingam S et al. CMSTO, 2014
*Based on July 2014 DBL; Symbols represent censored observations

CheckMate -017, A Phase 3 Study of Opdivo (Nivolumab) Compared to Docetaxel in Patients with Second-Line Squamous Cell Non-small Cell Lung Cancer (BMS press release, January 2015)
Docetaxel75 mg/m2 q 3 wks
Previously TxSquamous Cell
HistologyN=272
Nivolumab3 mg/kg q 3 wks
RANDOMIZATION
Nivolumab Docetaxel
Nivolumab

ALK Gene FusionROSI Gene Fusion
Squamous Cell
Crizotinib
Wild typeEGFR
Mutation +
Platinum with Pemetrexed Or
Platinum with Taxane
+ Bevacizumab*
Platinum Doublet***
ALK+
ErlotinibAfatinib
+ Bevacizumab
Treatment as per wild type
algorithmNivolumab
ErlotinibPemetrexed
First linetreatment
Maintenance(responders only)
Non-Squamous Cell
Second/Third Line treatment
Docetaxel**Pemetrexed** Erlotinib**
*Bevacizumab is not recommended in patients with untreated brain metastases, clinically significant hemoptysis or tumor cavitation **Treatment agent based on prior treatments, side effects profile, patient preference***Common platinum partners include Paclitaxel, Docetaxel, Abraxane, Gemcitabine, Vinorelbine
Docetaxel + Ramucirumab
Standard of Care Treatment Algorithm for Patients with Advanced NSCLC with PS 0-2
Erlotinib

Second line Phase III Trials
Trial Agent PD-L1 StatusCheckmate 057
Nivolumab vs. docetaxel (non-squamous)
Not required
Keynote 010 Pembrolizumab vs. docetaxel PD-L1 positiveOAK MPDL3280A vs. docetaxel PD L1 positiveLUNG-MAP MEDI4736 vs docetaxel Not required

KEYNOTE-001: Randomized Dose Comparison
Objectives• Evaluate safety, tolerability, and clinical activity of pembrolizumab • Evaluate correlation between clinical activity of pembrolizumab and PD-L1 expression
Mandatory Biopsy Within 60 Days of First Dose
Pembro 10 mg/kg Q3W
Pembro 10 mg/kg Q2W
Progressive Disease
Progressive Disease
R*1:1
• Treatment-naïve, stage IV NSCLC• ECOG PS 0-1• EGFR negative• No ALK rearrangement• PD-L1 positive (≥1% staining)• No systemic steroid• No autoimmune disease• No or stable brain mets
Balmanoukian SA, et al. Abstract #2
*First 11 patients were randomized to 2 mg/kg or 10 mg/kg Q3W
First Line Immunotherapy in Advanced NSCLC

Antitumor Activity by Pembrolizumab Dose
Pembro Dose
RECIST v1.1, Central Review irRC, Investigator Review
n
ORR DCR
n
ORR DCRn (%)
[95% CI]n (%)
[95% CI]n (%)
[95% CI]n (%)
[95% CI]
2 mg/kg Q3W 6 2 (33%)
[4%-78%]3 (50%)
[12%-88%] 6 4 (67%) [22%-96%]
5 (83%) [36%-100%]
10 mg/kg Q3W 20 4 (20%)
[6%-44%]14 (70%)
[46%-88%] 22 10 (46%) [24%-68%]
18 (82%) [60%-95%]
10 mg/kg Q2W 16 5 (31%)
[11%-59%]10 (63%)
[35%-85%] 17 7 (41%) [18%-67%]
12 (71%) [44%-90%]
Total 42 11 (26%) [14%-42%]
27 (64%) [48%–78%] 45 21 (47%)
[32%-62%]35 (78%) [63%-89%]
Interim Median PFS: • 27.0 weeks (95% CI, 13.6-45.0) by RECIST v1.1 per central review • 37.0 weeks (95% CI, 27.0-NR) by irRC per investigator review

Maximum Percent Change from Baseline in Tumor Size in Evaluable Patients (N=35)
10 mg/kg Q3W10 mg/kg Q2W2 mg/kg Q3W
* Still on treatment
** * * * * * * * * * * * * * *
* * * * *
(Central Review, RECIST v1.1)
Rizvi NA et al. J Clin Oncol. 32(5s) Abstract 8007, 2014

Time to and Durability of Response
• 11 of 11 (100%) responses are ongoing– Median duration of response not reached
(median follow-up, 36 weeks)• 7 of 11 (64%) responders remain on treatment
– Median duration of treatment: 27.1 weeks (range, 15.0+ – 48.3+)
• 19 of 21 (90%) responses are ongoing– Median duration of response not reached
(median follow-up, 36 weeks)• 18 of 21 (86%) responders remain on treatment– Median duration of treatment: 27.1 weeks (range, 6.1 – 57.1+)
RECIST v1.1 Central Review
0 10 20 30 40 50Time, weeks
Indi
vidu
al P
atie
nts
Trea
ted
With
Pem
bro
irRC Investigator Review
0 10 20 30 40 50 60Time, weeks
Indi
vidu
al P
atie
nts
Trea
ted
With
Pem
bro
Pembro 2 mg/kg Q3WPembro 10 mg/kg Q3WPembro 10 mg/kg Q2W
Partial ResponseProgressionOn Treatment
Rizvi NA et al. J Clin Oncol. 32(5s) Abstract 8007, 2014

First Line Immunotherapy in Advanced NSCLC
Pembrolizumab NivolumabNumber of Patients 45 20ORR 26% 30%SD 38% 35%PFS (median) 27 weeks 36 weeks
Gettinger SN et al. ASCO 2014 #8024

CA209-012 (CheckMate 012) Study Design:
Nivolumab 10 mg/kg IV Q3W until disease progression or unacceptable toxicity
Primary objective: safety and tolerabilitySecondary objectives: ORR and PFS rate at 24 weeks
Exploratory objective: OS
Squamous Non-squamous Any histology
Nivolumab 5 mg/kg IV Q3W until disease progression or
unacceptable toxicity
Nivolumab 10 mg/kg IV Q3W + Gem 1250 mg/m2
+ Cis 75 mg/m2
(four 21-day cycles)
Nivolumab 10 mg/kg IV Q3W + Pem 500 mg/m2 + Cis 75 mg/m2
(four 21-day cycles)
Nivolumab 10 mg/kg IV Q3W + Pac 200 mg/m2
+ Carb AUC 6(four 21-day cycles)
Nivolumab 5 mg/kg IV Q3W + Pac 200 mg/m2
+ Carb AUC 6(four 21-day cycles)
Chemotherapy-naïve patients with stage IIIB or IV NSCLC
Antonia SJ et al. CMSTO Abstract #3, 2014
First Line Immunotherapy + Chemotherapy in Advanced NSCLC

Efficacy Endpoints
Nivolumab 10 mg/kg Nivolumab 5 mg/kg
Gem/Cis (n = 12)
Pem/Cis (n = 15)
Pac/Carb (n = 15)
Pac/Carb(n = 14)
ORR, % 33 47 47 43
SD, % 58 47 27 43
18-month OS rate, % 33 60 40 86
Median OS, weeks 51 83 65 NR
NR = not reached

Overall Survival by Treatment Arm
Time Since First Dose (Weeks)
OS
(%)
0
20
40
60
80
100
B/L 12 24 36 48 60 72 84 96 108 120 132
Regimen mOS (wks)
Nivolumab 10 mg/kg + Gem/Cis 51
Nivolumab 10 mg/kg + Pem/Cis 83
Nivolumab 10 mg/kg + Pac/Carb 65
Nivolumab 5 mg/kg + Pac/Carb NR
x

Ongoing Phase III TrialsTrial Line of
TherapyAgent PD-L1 Status
CheckMate 026 First Nivolumab vs. investigator choice
chemotherapy
PD-L1 positive
Keynote 042/42 First Pembrolizumab vs. investigator choice
chemotherapy
PD-L1 positive
ARCTIC Third Line MEDI4736 vs. Chemotherapy
Not required
PACIFIC Locally Advanced
Following concurrent chemo-RT vs. placebo
Not required
Phase III Trials in Development: 1) Maintenance therapy in advanced NSCLC2) Adjuvant therapy

Pseudo-Progression
iRECIST
May occur in 7-10% of patients

Comparison: RECIST-irRC Criteria*
Complete Response (CR)
Disappearance of all extranodal target lesions. All pathological lymph nodes must have decreased to <10 mm in short axis
Disappearance of all lesions in two consecutive observations not less than 4 weeks apart
Partial Response (PR) At least a 30% decrease in the SLD of target lesions, taking as reference the baseline sum diameters
≥50% decrease in tumor burden compared with baseline in two observations at least 4 weeks apart
Stable Disease (SD) Neither sufficient shrinkage to qualify for PR nor sufficient increase to qualify for PD
50% decrease in tumor burden compared with baseline cannot be established nor 25% increase compared with nadir
Progressive Disease (PD)
SLD increased by at least 20% from the smallest value on study (including baseline, if that is the smallest)The SLD must also demonstrate an absolute increase of at least 5 mm (two lesions increasing from 2 mm to 3mm, for example, does not qualify)
At least 25% increase in tumor burden compared with nadir (at any single time point) in two consecutive observations at least 4 weeks apart
*Total Burden=SPD index lesions + SPD new, measurable lesions
RECIST irRCNew, measurable lesions (i.e. ≥5 x 5 mm)
Always represent PD Incorporated into tumor burden
New, nonmeasurable lesions (i.e. <5 x 5 mm)
Always represent PD Do not define progression (but preclude irCR)
Non-index lesions Changes contribute to defining BOR of CR, PR, SD, and PD
Contribute to defining irCR (complete disappearance required)
Wolchok J et al Clin Can Res 19:7412-7420, 2009

Treatment Related Adverse Events
System Immune Related Adverse EventsGastrointestinal Colitis (Diarrhea, perforation)Renal Acute Interstitial Nephritis (Increased serum
Creatinine)
Pulmonary Pneumonitis (dyspnea, cough)Dermatologic Dermatitis (Lichenoid/ spongiotic dermatitis,
rash), Vitaligo
Hepatic Hepatitis (elevated LFTs)Neurologic Central and Peripheral (Aseptic Meningitis,
Guillan-Barre Syndrome, Myasthenia Gravis
Endocrine Hypophysitis, thyroiditis, adrenal insufficiencyOcular Uveitis, Iritis
• Fatigue is the most common AE (24%)• Grade 3-4 AEs are uncommon (6-12.6%)

Identifying Predictor(s) of Response
Responses are higher in PD-L1+ tumors but seen in PD-L1- tumors
Nivolumab (anti-PD-1)
Pembrolizumab (anti-PD-1)
MEDI4736 (anti-PD-L1)
MPDL3280A (anti-PD-L1)
Solid
tumors Mel Mel Mel
NSCLC
NSCLC RCC
H/N MelNSC
LCNSC
LCNSC
LCNSC
LC
Bladder Mel
NSCLC
Solid
tumors
0
10
20
30
40
50
60
70
80
all patientsPD-L1+PD-L1-
Lipson, Taube, et al. Semin Oncol. In press.

Identifying Predictor(s) of Response
PD-L1 IHC Expression By Various Assays Tumor GNE DAKO 28-8 Merck CC23 5H1Melanoma 40% 45% 71% 42%
NSCLC 45-50% 49% 45% (25% if ≥50% Staining)
Renal 20% 24%
Bladder 21% 28%
Head And Neck 31% 46%
Glioblastoma 25% 100%
• No validated assay• Variable cut off levels for positivity
Challenges
PD-L1 positive (TC)PD-L1 positive (IC)PD-L1 negative

Identifying Predictor(s) of Response Immune Cell PD-L1 Expression
Patients treated with MDPL3280A
NSCLC
Herbst RS et al. Nature 515: 563-7, 2014

Identifying Predictor(s) of Response Prevalence of PD-L1 IHC Expression?
Prognostic significance of PD-L1 Expression?
Author N Stage (TC)PD-L1 (IC)PD-L1 PrognosisD’Incecco2015 122 IV 55.3%
Herbst2015 184 IV 24% 26%
Velcheti2014
204 340
I-IVI-IV
25%36%
PD-L1 associated with better survival
Mu2011 109 I-IV 53% PD-L1 associated
with poor survivalKowanetz 2010
254 (adeno) 37 (adeno) 139 (squamous) 16 (squamous)
I-IIIa IIIb-IV
I-IIIa IIIb-IV
31%19%31%31%
49%27%54%38%
D’Incecco A et al. Br J Can 112: 95-102, 2015; Herbst RS et al. Nature 515: 563-7, 2014Velcheti V et al. Lab Invest 94: 107-16, 2014; Mu CY et al. Med Oncol 28: 682-8, 2011Kowanetz M et al. WCLC 2013 Abstract

Tumor-Infiltrating Lymphocytes (TIL cells)
The presence of TIL cells at diagnosis
correlates with improved clinical
outcomes
CD3/AE1AE3
Zhang L et al. NEJM 348:203-13, 2003Galon J et al. Science 313: 1960-4, 2006Azimi F et al. J Clin Oncol 30: 2678-83, 2012Adams S et al. J Clin Oncol 2014 [Epub ahead of print]
Ovarian
Colon
Melanoma
Breast
Identifying Predictor(s) of Response

Tumor-Infiltrating Lymphocytes (TIL cells)
Identifying Predictor(s) of Response
Schalper, KA et al. JNCI 107:epublished Feb 3, 2015
• 552 patients from two cohorts• TIL cells did not correlate with OS• CD8 expression is an independent favorable prognostic marker

Identifying Predictor(s) of Resistance
CD8 negative Minimal CD8 expression Tumor rim CD8 expression
No evidence of CD8 T cell activityHerbst RS et al. Nature 515: 563-7, 2014

Identifying Predictor(s) of ResponseMutational Burden
Rizvi NA et al. Science 348:124-8, 2015
11/431/10
n=17n=17
n=16n=18
Median PFSNR vs 3.4 moHR 0.19 (0.08-0.47)P = 0.0004RR 59% vs 12%
Median PFSNR vs 3.5 moHR 0.15 (0.06-0.39)P = 0.0001ORR 56% vs 17%
Median PFS14.5 mo vs 3.5 moHR 0.23 (0.09-0.58)P = 0.0002
• Median values used to determine high vs low• No mutations or copy number alterations in CD274 (PDL-1 gene)• Smoking history did not discriminate for responders• Molecular smoking signature correlated with mutational burden

Combined Immunomodulation
Chen DS, et al. Immunity. 2013;39:1-10.

Phase I Trial of Ipilumumab and Nivolumab in First Line NSCLC N=49
Antonia SJ, et al. J Clin Oncol 32:5s, 2014 (suppl; abstr 8023)
ORRs: 8/49 (16%); PFS: 14 -16 wks
Treatment related Grade 3 or 4 AE (49%); Discontinuation (35%)
Combined Immunomodulation

Top Questions about Immune Checkpoint Inhibitors
• Anti- PD1 vs. Anti-PDL1?• Ideal schedule/duration of therapy?• Will/should PDL1 status guide treatment?• Sequencing/Maintenance Therapy? • Optimal Combinations?• Mechanisms of Resistance?

• Immune checkpoint inhibitors represent a new class of agents that are showing great promise for the treatment of advanced NSCLC.
• Immune checkpoint inhibitors have a distinct toxicity profile and response assessment that must be taken into account in treating patients with these agents.
• Immune checkpoint inhibitors represent the first of several strategies targeting the immune system for therapeutic benefit.
Summary

I have your molecular profile, tumor PDL-1, Immune PDL-1
and CD8 expression levels and a variety of other tumor assay
results for us to discussand use to select your
treatment

• Mrs. LW is a 45 year old Asian never smoker with stage IV adenocarcinoma of the lung with multiple bilateral pulmonary nodules and bone metastases. Her tumor was EGFR/ALK/ROS-1 wild type and PDL-1 negative. What is her chance of responding to an immune checkpoint inhibitor?
1. 70% 2. 50% 3. 10% 4. 5%
Question

• What immune related adverse event occurs in >5% of patients receiving nivolumab?
1. Colitis 2. Pneumonitis 3. Hepatitis 4. Hypthyroidism 5. Uveitis
Question