Embed Size (px)
Citation preview

In Practice ● JA N U A R Y 200632
VASCULAR STUDIES
Ultrasonography is gaining favour as a quick and non-invasive diagnostic tool in cases of suspected portosys-temic shunts (PSSs), but vascular ultrasound imaging isdifficult. Scintigraphy is a good screening technique forall types of PSS and provides information about shuntingfraction, but requires specialist equipment and kennelling,and is usually only performed at referral centres. Portalvenography, although invasive, therefore remains the prin-cipal imaging technique for definitively diagnosing allforms of shunt, allowing both the location and morpholo-gy of a shunt to be identified (Lamb and Daniel 2002).
If a PSS is strongly suspected, ultrasonography (ifavailable) should be performed first (using chemicalrestraint, if needed) to:■ Rule out obvious multiple acquired shunting vessels;■ Identify single shunts;■ Evaluate the portal vasculature; ■ Detect the presence of urolithiasis.
If surgery is to be performed to treat a single shunt,portal venography is recommended to rule out theunlikely chance of a double shunt and to obtain moremorphological information about the anomalous vessel.
TECHNIQUEPlain radiographs should always be obtained to evaluatethe radiographic exposure, detect the presence of urateurolithiasis (although calculi will only be radiopaque ifammonium biurate crystals are combined with struvite)and assess the size of the liver and kidneys; a small liverand large kidneys are sometimes seen in dogs with congen-ital PSSs, but not in cats. If there is no concurrent ascites,survey radiographs can also potentially show the irregular
CO
MP
AN
ION
A
NIM
AL
P
RA
CT
ICE
THIS final article in the series on contrast radiography describes how to conduct vascular and articularstudies, dacryocystorhinography, sinography and lymphangiography. In each case, only those techniques routinely performed in practice are discussed. Procedures that are difficult to perform and interpret, require specialist equipment, or have largely been superseded by advanced imagingtechniques such as ultrasonography, computed tomography and magnetic resonance imaging – all of which are now quite widely available – will not be considered.
Practical contrast radiography
5. Other techniques FRANCISCO LLABRES DIAZ
Despite the advent of advanced imagingtechniques, contrastradiography still providesvaluable information abouta variety of pathologies
In Practice (2006)28, 32-40
margins of a cirrhotic liver, which can lead to hepatic por-tal hypertension and multiple acquired extrahepatic shunts.
It is important to take plain radiographs with the samex-ray machine that is to be used for portal venography,using, if possible, a similar focus–film distance and the
Francisco LlabresDiaz graduated fromthe University ofZaragoza, Spain, in1996. After a briefperiod in practice inSpain, he moved tothe Animal HealthTrust, Newmarket. In 2005, he joinedDavies VeterinarySpecialists inHertfordshire. He holds the RCVScertificate anddiploma in veterinaryradiology, theEuropean diploma inveterinary diagnosticimaging, and is anRCVS recognisedspecialist in veterinarydiagnostic imaging.He is the currentchairman of theBritish and IrishDivision of theEuropean Associationof VeterinaryDiagnostic Imaging.
Portosystemic shunts
PSSs are classified as:■ Congenital/acquired;■ Single/multiple;■ Intrahepatic/extrahepatic.
Congenital PSSs are single (occasionally double)and usually intrahepatic in larger breeds of dog,but extrahepatic in small breeds of dog. Malteseterriers, Irish wolfhounds, Yorkshire terriers, andPersian and Himalayan crossbreeds are predisposedto the condition.
Acquired PSSs are usually multiple and affectolder patients that suffer from chronic portalhypertension, but may be seen in young patientssecondarily to congenital portal vein atresia or arte-rioportal fistulae. Two important points should beborne in mind: ■ Collateral shunting vessels are normal non-patent vessels in dogs and cats, and will open dueto the increased pressures in the portal system;■ Portal hypertension that develops as a sequela to a cardiac problem is the only type of portalhypertension (prehepatic, hepatic and posthepatic)where shunting will not develop, as the pressurerises equally in both the portal and systemic venoussystems.
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

In Practice ● JA N U A R Y 2006 33
Indications
Portal venography■ To confirm the presence of any macro-scopic blood shunting between the portaland systemic venous circulations■ To determine if the shunt is single ormultiple. Surgery is not indicated in cases ofmultiple acquired PSSs and their prognosisis poorer■ To help identify cases of two coexistingshunts (rare)■ To define a single shunting vessel asintra- or extrahepatic and to determine its general location if surgery is to be performed. Also, to subjectively assess thedegree of shunting and development of theintrahepatic portal vasculature■ To evaluate the degree of postsurgicalhepatic neovascularisation, by performing asecond study several weeks after surgery■ To confirm the presence of the portalvein (if anomalous development is suspect-ed) and to demonstrate its patency (if an intraluminal thrombus is present, forinstance)
Shoulder arthrography■ To evaluate the articular cartilage incases of suspected osteochondritis dissecansof the humeral head; also in cases wheredamage to and thinning of the articular car-tilage are suspected■ To detect radiolucent intra-articularlesions (eg, joint mice from detached flapsof articular cartilage or osteochondromas)as filling defects■ To assess the biceps tendon of origin
and its tendon sheath in cases of suspectedbicipital synovitis, and also in cases of osteo-chondritis dissecans, where radiolucent jointmice located in the bicipital tendon sheathcould ultimately cause tenosynovitis■ To investigate whether periarticular radi-opacities seen on plain radiographs are infact intra-articular■ To detect and evaluate the severity of ajoint capsule rupture
Dacryocystorhinography■ To assess cases of chronic epiphorawhere an obvious aetiology cannot befound by complete ophthalmological exam-ination, including fluorescein and Schirmertear tests and flushing of all the subdivi-sions of the lacrimal system with sterilesaline. Dacryocystorhinography can be espe-cially helpful in cases of nasolacrimal for-eign bodies and dacryocystitis■ To evaluate whether a known lesion isconnected to or has an effect on thelacrimal system (eg, cystic or soft tissuelesions in the nasal/maxillary area, peri-orbital swellings or periorbital fistulae)
Note that if a foreign body is suspected ofbeing the cause of the clinical signs seen, ret-rograde flushing can be attempted beforeradiography and after catheterising the dis-tal opening of the nasolacrimal duct into the nasal cavity. This ensures that the foreignmaterial is not pushed further distally intothe duct. An otoscope can be used to localisethe distal opening, but it is usually difficultto identify except in large breeds of dog
Sinography■ To evaluate the extent of a chronicdraining sinus or fistula and its possiblecommunications with organs or cavities.Knowledge of the length and orientation of the tract will help in planning the surgi-cal approach, especially if radiolucent for-eign material is the cause of the infectedsinus■ To assess the extent of wounds ofunknown depth. This is more commonlyused in equine practice and is not routinelyemployed in small animals
Lymphangiography■ To assess cases of lymphoedema (accumu-lation of fluid in the interstitial space sec-ondary to abnormal lymphatic drainage)when circulatory oedema (due to a problemwith the venous return) or other causes ofgeneralised oedema (eg, hypoproteinaemia,right-sided cardiac failure) have been ruledout. Primary lymphoedema is caused by aspecific problem with the lymphatic system,usually aplasia or dysplasia of the lymphaticvessels or lymph nodes, and is rare.Secondary lymphoedema is more common(see later). Vascular ultrasonography canalso be helpful for investigating venousabnormalities■ Mesenteric lymphangiography, in partic-ular, can be used to investigate cases of chylothorax where a problem with the thoracic duct is suspected. However, thistechnique is difficult and is not frequentlyperformed even at referral institutions
Water-soluble iodine-containing media Low osmolar non-ionic media*
Portal venography Yes A dose of 1 ml/kg at a concentration of at least 300 mgI/ml is required. The maximum volume per single injection is 90 ml. The maximum dose per study is 1000 to 1200 mgI/kg, although a maximum dose of 3200 mgI/kg has been suggested by Miller and others (2002)
Shoulder arthrography Yes Both ionic and non-ionic low osmolar contrast media will provide diagnostic arthrograms in the first few minutes after injection. However, non-ionic low osmolar contrast causes a milder inflammatory response and draws less fluid into the joint space due to its lower osmolarity. This allows evaluation of the areas of interest to be carried out over a longer period of time following injection because the contrast medium is less dilute
It is important to use a final concentration of 100 mgI/ml to avoid masking small lesions; the contrast should therefore be diluted, as necessary. A dose of 2 to 7 ml of contrast medium is usually needed to evaluate the scapulohumeral space; larger dogs require higher volumes, but injecting contrast under high pressures or using unrealistic amounts of contrast should be avoided, just in case there is a capsulardefect and the contrast leaks outside the joint
Larger volumes of contrast (0·4 ml/kg bodyweight at a concentration of 100 mgI/ml, if iohexol is used)are needed to assess the bicipital tendon sheath and all joint pouches
Dacryocystorhinography Yes A total dose of 0·5 to 1 ml at a concentration of 300 mgI/ml is routinely employed. A slight dose variation may be required, depending on patient size. A new contrast injection is usually needed for every radiograph in the study. The contrast medium viscosity will be preserved if the contrast is kept at room temperature before the injection. This helps contrast retention inside the duct and therefore radiographic interpretation
Sinography Yes A variable dose, depending on patient size and the depth of the draining tract, is used. Diluting thecontrast medium in sterile water to a concentration of 150 mgI/ml or using contrast medium of this concentration yields better results
Lymphangiography Yes A dose of 100 mgI/kg, diluted with 0·25 ml/kg of sterile saline, has been proposed for direct lymphangiography
*For example, iohexol (Omnipaque; GE Healthcare). Water-soluble low osmolar non-ionic media are preferable and safer to use than water-soluble high osmolar iodine-containing media, but are not essential
RECOMMENDED CONTRAST MEDIA FOR DIFFERENT TECHNIQUES
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

In Practice ● JA N U A R Y 200634
same film–screen (and grid, if any) combination. Thecontrast medium should be injected slowly and understerile conditions into a tributary vessel of the portal vein;a jejunal vein that is catheterised after celiotomy is considered the best method (Lamb and Daniel 2002),although other injection sites have been described (seelater). The radiograph should be obtained at the end of theinjection or during the last few seconds of the injection. Along sterile flexible polyethylene extension tube (Lectro-Spiral or Lectro-Cath; Vygon) prefilled with contrast isroutinely used.
Portal venograms obtained in left lateral recumbencywere found to be superior to those obtained in right later-al recumbency in a recent study, although no significantstatistical difference was found between radiographstaken in left lateral recumbency and dorsal recumbency(Scrivani and others 2001). A second injection with thepatient in dorsal recumbency will help to define whethera PSS is left or right sided.
INTERPRETATIONAs always, a systematic approach to the interpretation of the radiographs obtained is essential. In normal ani-mals, the injection of contrast medium into the portalsystem will highlight the portal vein and the tree-likepattern of intrahepatic portal vessels. The followingpoints should therefore be checked on every portalvenogram:■ The presence and patency of the prehepatic portalvein, together with a subjective assessment of the degreeof development of the intrahepatic portal system;■ Whether an abnormal portosystemic communicationexists and, if so, whether it is single or multiple;■ If a single portosystemic communication is identified,whether it is intra- or extrahepatic. An intrahepatic PSSis most likely if the caudal-most loop of the shunt or thelocation where it diverges from the original vessel is cra-nial to T13. However, respiratory motion can change thelocation of the shunt by 0·5 to 0·75 times the length of avertebra and, in any case, it is very difficult to determinethe most caudal point of a shunt in a radiograph of asmall-breed dog, puppy or cat! If a single PSS is suspect-ed from the patient’s signalment, pre-radiographic ultra-sound examination is indicated to help establish whetherit is intra- or extrahepatic;■ In patients where portal venography is repeated afterpartial ligation of a single shunt, it is important to evalu-ate the presence and degree of hepatic neovascularisa-tion. Some shunting usually remains unless a progressivecompressive device has been used, in which case long-term flow through the shunt should be down to a mini-mum or should have completely stopped four to fivemonths after surgery.
Contraindications to portalvenography
Portal venography is contraindicated in:■ Animals where, based on signalment, history andclinical signs, there is a strong clinical suspicion thatportal hypertension has caused multiple acquiredPSSs. In such cases, abdominal ultrasound examina-tion, focusing especially on the liver, portal vein andperiportal structures, together with ultrasound-guid-ed liver biopsy if a hepatic problem is suspected,constitute a more practical and rational approach.Ultrasonography can also be used to identify multi-ple shunting vessels, and investigate cases where a(rare) hepatic arterioportal fistula is suspected as thecause of portal hypertension (congenital in puppies,or acquired – for instance, secondary to neoplasia –in older patients). Where contrast studies arerequired, selective angiography of the coeliac arteryis the technique of choice■ Cases where severe cholestasis or liver failureneed to be ruled out as possible causes of raisedserum bile acids. Again, abdominal ultrasoundexamination constitutes a more practical approachto the investigation of these problems■ Cases where any other concurrent clinical prob-lem increases the risk of the patient having toundergo an exploratory laparotomy. Animals withsevere shunt-induced clinical signs should be sta-bilised first
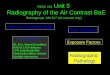
Home-made device used in theatre for portal venography, which, if positioned beforesurgery begins and covered with sterile drapes, allows multiple radiographs to be takenwithout having to move the patient and without affecting sterility. It can be made from any semi-rigid cardboard box wide enough to accept an x-ray cassette (in this case, an empty radiographic film box)
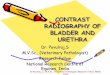
Single extrahepatic PSS in a six-month-old Border collie. In patients with single PSSs, thecontrast medium will flow from the portal tributary or portal vein via the shunting vessel tothe systemic vein (usually the caudal vena cava, but hepatic, azygos, internal thoracic, renalor perineal veins could also shunt blood) and on to the right side of the heart. In cases ofmultiple acquired PSSs, the shunting blood usually enters the renal or gonadal veins, thevenous sinuses in the vertebral canal or the caudal vena cava itself. In the example shown,the shunting vessel leaves the portal vein caudal to T13 (arrow), to reach the caudal vena cava, indicating that it is an extrahepatic shunt. This was confirmed at surgery
When conducting thetype of studies dis-cussed in this article,staff must wear protec-tive clothing, which,together with a mobilelead screen (if avail-able) and the use ofan extension tube pre-filled with contrast,will decrease exposureto scattered radiation.
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

In Practice ● JA N U A R Y 2006 35
Potential pitfalls■ Leakage of contrast medium or a considerable delaybetween the end of the injection and exposure usuallyresults in not enough contrast being present in the vessels.■ If contrast medium is injected into the splenic vein or parenchyma, a PSS arising caudal to these sites (eg, from the cranial or caudal mesenteric vein) will notbe identified. Moreover, the opacified splenic parenchy-ma could potentially be superimposed on the shuntingvessel.■ It is important to be aware of ‘hepatic microvasculardysplasia’, a disease affecting both dogs and cats, wheremicroscopic PSSs occur but no macroscopic shunt is visible on portal venography, despite the clinical signsbeing similar to those associated with a macroscopiccommunication. Compatible histopathological changesin liver biopsies together with the lack of identificationof a macroscopic shunt during surgery and portal venog-raphy or scintigraphy are needed before this diagnosis isreached (Christiansen and others 2000).
ARTICULAR STUDIES
In cases where bicipital tenosynovitis or injury to thebiceps tendon is suspected following clinical examina-tion, ultrasonography can be used to assess the bicepstendon of origin (noting any areas of mineralisation,oedema or tears) and the surrounding tendon sheath(checking for distension) before a more invasive arthro-gram is performed. The two techniques are complemen-tary, but the major advantages of ultrasound examinationare that it is less invasive and can be performed withoutthe need for chemical restraint in a cooperative patient.
TECHNIQUESurvey radiographs should always be obtained to evalu-ate the radiographic exposure and to detect any abnor-malities revealed by plain radiography, such as:■ Flattening of the humeral head, mineralised cartilageflaps, mineralised joint mice (pieces of fragmented carti-lage that are usually resorbed but may continue to grow andbecome mineralised), or subchondral bone defects with or
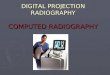
Portal venography in a domestic shorthaired cat before (left) and three months after (right) partial ligation of a singleintrahepatic PSS. Red arrow, portal vein; yellow arrow, PSS; blue arrow, immediate opacification of the caudal vena cava after injection of the contrast medium (note the intrahepatic portal vasculature is not highlighted by contrast)
New bone formation in the intertubercular groove. Apart from routine mediolateral and caudocranial views of the shoulder (A and B), the cranioproximal-craniodistal oblique view (C) can be useful to show mineralisation of the biceps tendon, the presence of mineralised joint mice or changes in theintertubercular groove, which are characteristic for bicipital tenosynovitis
(A) (B) (C)
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

In Practice ● JA N U A R Y 200636
without an increase in peripheral subchondral radiopacityin cases of osteochondritis dissecans (OCD). Joint mice canbe seen in the scapulohumeral space, the bicipital tendonsheath, and in the caudal or medial pouches (best viewedon the caudocranial projection) of the shoulder joint;■ New bone formation at the level of the intertuberculargroove or supraglenoid tuberosity, or dystrophic miner-alisation of the biceps tendon of origin in cases of bicipi-tal tenosynovitis;■ Joint effusion or a vacuum phenomenon in somecases of OCD;■ Secondary or unrelated osteoarthritic changes;■ Other lesions such as a primary tumour of the proxi-mal humerus, osteomyelitis, septic arthritis, fractures,luxations or mineralised osteochondromas.
Always compare radiographs of the affected jointwith those of the contralateral joint taken under the sameconditions. These provide a good baseline for compari-son if they are normal, but can also help to identify casesof bilateral OCD, which are not uncommon, even if clin-ical signs appear to be only unilateral. It is important tocorrelate radiological findings with clinical signs and theresults of the physical examination to establish the realsignificance of the radiographic changes.
General anaesthesia and aseptic preparation of theinjection site are mandatory. When investigating articu-lar injuries, fluid analysis is important to detect inflam-matory or degenerative changes and also to rule outother possible causes of lameness and pain. A sample ofsynovial fluid should therefore be obtained from the areaof interest before administering any contrast agent (seebox below). After making sure that no air remains in theneedle, slowly inject warmed contrast medium. The useof a short flexible extension tube can sometimes help toavoid movement of the needle tip in the joint space.Once the full dose of contrast has been injected, manipu-late the joint to spread the contrast medium evenlythroughout all the different areas.
Neutral mediolateral and caudocranial radiographs,with slightly higher exposure settings than plain radio-graphs, usually +5 to +10 kV, according to the size ofthe patient, should be obtained without delay. If a lesionis seen or suspected in the region of the intertuberculargroove, or bicipital tendon or its sheath, a cranioproxi-mal-craniodistal oblique view should also be taken.
Positional radiography can be useful, although theappearance of the different structures is not standard,which can make assessment difficult:■ A mediolateral flexed or extended radiograph concen-trates the contrast medium in the region of the caudalpouch or the bicipital tendon sheath, respectively, allow-ing their complete assessment. The bicipital tendon oforigin, however, will be narrower on the flexed mediolat-eral projection but wider on the extended one, and sothese views should only be used when checking for fill-ing defects or to evaluate distension of the bicipital ten-don sheath, as they can be misleading if they are used toevaluate the diameter of the tendon itself;
■ Rotational views can be useful for evaluating the car-tilage and subchondral bone of the medial aspect of thehumeral head in those cases where an OCD lesion is sus-pected, but was not seen on the neutral and rotated plainmediolateral radiographs.
INTERPRETATIONOnce the quality of the arthrogram has been evaluated,the joint space, including the different joint pouches, thebiceps tendon and its sheath, the articular cartilage, thesubchondral bone and the underlying humeral epiphysismust be systematically assessed.
Arthrographic findings associated with OCD include: ■ The presence of a focal area of thick articular carti-lage over a subchondral bone defect; ■ An irregularity in the outline of the articular cartilage; ■ The presence of a cartilage flap, highlighted by a thinline of contrast between the flap and the subchondralbone defect; ■ The presence of joint mice, seen as filling defects;
Osteochondromas can appear as intra-articular fillingdefects although no accompanying subchondral bonelesions are seen.
Typical radiographic changes seen in cases of bicipitaltenosynovitis are poor relative distension and irregularityof the bicipital tendon sheath (due to synovial prolifera-tion and adhesions) together with an irregular appearanceof the biceps tendon itself associated with fibrosis andscarring. In some cases of focal tendon tearing, poor out-lining of the tendon can be seen in the area of the lesion.
It is important to remember that an arthrogram is notindicated if septic arthritis is suspected, unless the infec-tion is secondary to trauma and a puncture wound orjoint capsule rupture need to be confirmed/ruled outbefore surgery.
Potential pitfalls■ Spillage of contrast over the skin or cassette shouldbe avoided.■ Poor contrast filling of the joint space and all thestructures being evaluated may result from either insuffi-cient contrast volume or extracapsular extravasation.This leads to poor distension of the joint pouches andbicipital tendon sheath and poor delineation of the artic-ular cartilage surface, making assessment difficult. Inaddition, all the articular structures should be distendedto a similar degree; some cases of bicipital tenosynovitisshow poor distension of the bicipital tendon sheath whencompared with the degree of filling of the caudal jointpouch, due to the presence of scarring tissue and adhe-sions between the tendon and the sheath. Poor fillingcould easily mimic this appearance.■ Excessive contrast can obscure small lesions andcause extracapsular extravasation, which can render thestudy non-diagnostic if large volumes of contrast leavethe joint capsule.■ If the contrast medium is too opaque (ie, not diluted),small lesions can be missed.■ Arthrography can be an insensitive technique fordetecting small or mild lesions, both in cases of OCDand bicipital tenosynovitis. If the problem is thought tobe shoulder-related from the clinical signs, signalmentand history, arthroscopy can be more useful; however, itshould be noted that the particular area of the bicipitaltendon is not accessible to the arthroscope and, in suchcases, ultrasonography should be used.
Collecting a synovial fluid sample from the shoulder joint
With the patient in lateral recumbency, insert a 20 to 22 gauge, 3·75 cm spinalneedle with stylet 1 cm distal to the acromion and direct it medially, and slightlycaudally and distally. Stop advancing the needle as soon as synovial fluid is seenin the hub of the needle or once synovial fluid can be aspirated.
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

In Practice ● JA N U A R Y 2006 37
DACRYOCYSTORHINOGRAPHY
General anaesthesia (rather than sedation) is recommend-ed when conducting dacryocystorhinography. Again,plain radiographs should be obtained to evaluate position-ing and exposure, and to identify areas of lysis, new boneformation, radiopaque foreign bodies or cysts that couldexplain the clinical signs seen. Lysis in the area of thenasolacrimal duct does not automatically imply the pres-ence of a neoplastic process, as lysis can also be detectedin chronic cases of dacryocystitis.
TECHNIQUECatheterise the upper lacrimal punctum of the side of thepatient away from the x-ray cassette. This is the best siteas it is continuous with the nasolacrimal duct in almost astraight line. Flexible catheters (Portex irrigating cannula;Sims Portex) with the tip cut off are helpful and easy touse. Inject contrast medium while applying pressure to thelower punctum to prevent contrast spillage. It is difficultto avoid some contrast reflux outside the system; coveringthe area around the medial canthus of the eye with a swabwill help to avoid artefacts by soaking up spilled contrast,after which the soaked swab should be removed.
Slightly raise the caudal aspect of the head beforeinjection to prevent caudal displacement of the contrastmedium within the nasal cavity. Severe contrast contam-ination of the area around the nasoturbinates can renderthe examination non-diagnostic.
A retrograde contrast injection is recommended ifforeign material is suspected to be present in the duct,even if some of it has already been dislodged by a previ-ous retrograde saline flush.
It is best to leave the catheter in place and obtain theradiographs just after injection. If a stricture along theduct is suspected, it may be necessary to take a secondradiograph during the last second of a new injection toshow the area of the stricture under pressure. The use ofa short contrast-prefilled extension tube, together with alead screen, will decrease operator exposure to scatteredradiation.
A lateral radiograph of the skull is usually preferable,but a dorsoventral intraoral radiograph of the nasal cavi-ties and surrounding bones will avoid superimposition ofthe two sides of the patient. If an intraoral cassette is notavailable, an oblique radiograph (rostroventral caudo-dorsal oblique view of the rostral skull) can be obtained,although the nasal cavities always appear shortened onthis projection.
INTERPRETATIONWhen interpreting radiographs, it is important to recog-nise the normal features of a dacryocystorhinogram. Inevery study, the size (diameter), position and radiopacityof the highlighted duct must be evaluated. In addition,the presence of contrast medium in abnormal areas,which could indicate fistula formation, for example,should be noted. As with other contrast techniques, consistency of findings is vital, and at least two radio-graphs showing the same finding are needed before anydefinitive diagnosis is reached. In those cases where the abnormal findings are in or around the proximal thirdof the nasolacrimal duct, it may be better to repeat a lat-erolateral radiograph rather than obtain an orthogonalradiograph, as the superimposition of the maxillary bone and teeth may hinder the radiographic interpretation of
These images show dacryocystorhinography performed in a retrograde fashion in a one-year-old labrador retriever presented with a swelling on the medial canthus of the eye. The aim of the contrast study was to assess whether the round cystic lesion seen rostral to the orbit on the plain radiograph (above) was connected to the nasolacrimal system. (below) Dacryocystorhinogram showing the distal portion of the nasolacrimal duct. Theproximal portion is not clear and some contrast leakage has occurred in the region of the globe, but the study confirms patency of the nasolacrimal system and that it is notcommunicating with the cystic lesion. In normal dacryocystorhinograms, a thin undulatingradiopaque line is seen progressing rostrally from the fossa in the lacrimal bone to therostral opening of the duct, usually 2 cm caudal to the nares. A slight variation in internaldiameter is acceptable, particularly a mild narrowing of the proximal third of the duct, asthis portion is within the osseous lacrimal canal that runs through the lacrimal and maxillarybones. Some dogs can also have a cul-de-sac rostral to the nasal opening or a normal secondopening into the nasal cavity dorsal to the root of the upper canine tooth. If the majority of contrast leaves the duct through this opening, it is possible that the rostral-most aspectof the duct will not be seen. The dorsal canaliculus and the tiny lacrimal sac are usuallyimpossible to differentiate from the nasolacrimal duct unless some contrast also highlightsthe ventral canaliculus, as both canaliculi will merge at the level of the sac
this portion of the duct on the dorsoventral intraoralview. ■ Consistent narrowing or discontinuity of the naso-lacrimal duct suggests an obstruction, which could besecondary to intraluminal causes (eg, foreign body orcells/debris in cases of relatively acute dacryocystitis),changes to the duct’s wall (eg, in cases of more chronicdacryocystitis with scarring), or extraluminal causes (eg, fractures of the surrounding bone, tumours, cysts or abscesses).
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

In Practice ● JA N U A R Y 200638
It is always difficult to establish whether a cystic dilation of the duct is the cause or the result of dacryo-cystitis, as cystic dilations of the duct, together withchanges in the shape of the duct and lysis of the sur-rounding bone, may be present in very chronic cases. Ifthe concurrent epiphora and mucopurulent discharge ischronic, it is likely that the cystic area is secondary.Correlation between the findings of the contrast tech-nique and the history and results of the ophthalmologicalexamination are fundamental to reaching the correctdiagnosis.■ Any periorbital, maxillary or nasal mass lesion canaffect the position of the nasolacrimal duct. A dacryo-cystorhinogram is not really used to diagnose thesepathologies per se; rather, it is helpful for evaluating thepossible relationship between the mass lesion and theocular signs.■ The radiopacity of the contrast medium may bealtered by radiolucent intraluminal material (either mix-ing with the contrast or appearing as a filling defect),which may not have been evident on plain radiographs.Commonly, only the caudal margin of foreign material is highlighted by contrast medium. A complete fillingdefect will only be seen if the contrast bypasses the foreign material.
Potential pitfalls■ Contrast medium in the periorbital area or on the x-ray cassette will obscure the area of interest. ■ Poor contrast filling of the nasolacrimal duct mayoccur due to contrast reflux. Ideally, contrast mediumshould be present in the nostrils by the time the radio-graph is taken. However, this may not be possible incases of chronic epiphora due to a non-patent duct or insome brachycephalic breeds, as the contrast medium canroutinely flow into the nasopharynx in these patients.
SINOGRAPHY
General anaesthesia is helpful when conducting sinogra-phy, and good preparation of the area of interest is essen-tial to avoid wet hair artefacts caused by dried exudatesor topical preparations around a wound. Plain radio-graphs should be obtained to assess exposure and also to identify radiopaque foreign bodies, areas of free gas,periosteal reactions or areas of soft tissue swelling. It isalso important to obtain samples for cytology, cultureand antibiotic sensitivity testing before injecting anycontrast medium.
TECHNIQUEInsert a sterile flexible catheter prefilled with contrastmedium (to avoid introducing air bubbles) through the skin defect. Use a sterile radiopaque marker before-hand to obtain a rough idea of the length and orientationof the tract. Although some authors recommend introducing a catheter as deeply as possible and theninjecting contrast medium as the catheter is pulled out, in an attempt to fill up the tract, it is easier to position the tip of a Foley catheter in the proximal portion of the tract and inject contrast until some pressure is felt in the hope that the tract is completelyfilled with contrast by that stage. The Foley cathetershould be kept in position once the balloon is inflated.Alternatively, if a Foley catheter is not available, a purse-string suture or atraumatic forceps can be placedaround the catheter. Excessive pressure must not beapplied when injecting the contrast medium, as thisincreases the risk of contrast leaking around the area of injection, thus rendering the radiographs non-diag-nostic; it also introduces contaminated contrast mediumand exudate through previously unaffected fascialplanes.
Cystic dilation of the nasolacrimalduct in a five-and-a-half-year-old Irish setter with chronic epiphora. The dog was diagnosed as havingchronic dacryocystitis with secondarynasolacrimal duct cystic formation. (A) Plain radiograph. (B and C) Lateralradiographs after two differentinjections of contrast medium,showing contrast accumulation within a focal lesion ventral to thenasolacrimal duct (arrows), which isconsistent with a cystic lesion. Thefact that the contrast medium remains in this area rules out leakage of contrast into the nasal cavity
(A) (B)
(C)
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

In Practice ● JA N U A R Y 2006 39
Two orthogonal views and possibly lesion-orientatedoblique views of the area are necessary to maximise the information about the tract. Multiple injections of contrast medium may be needed if the contrast medium rapidly flows out of the area of interest. A second exposure, just before the end of contrast injec-tion, can be useful to identify focal strictures or smallramifications of the tract. As discussed earlier, appropri-ate precautions should be taken to limit exposure to scattered radiation.
INTERPRETATIONConsistent findings on different views are fundamentalfor interpretation of the radiographs, especially as nonormal images are available for comparison. Woodensticks, for example, are meant to be relatively well-defined filling defects, but visualisation depends on having enough contrast medium completely surroundingthe foreign body. On the other hand, abnormal com-munications between hollow organs or body cavities can potentially be demonstrated very well by this technique.
Potential pitfalls■ Superimposition of spilled contrast medium aroundthe skin defect.■ The tract is only partially highlighted by the contrastmedium. This can be due to either incorrect dosage of contrast being administered (if, for example, the tract is longer than expected) or reflux of the contrastagent.■ The contrast medium stops at a stricture or fails tohighlight small ramifications of the tract.■ It can be extremely difficult to accurately interpret an irregularly shaped filling defect: small foreign bodies, exudate or blood clots all look very similar radiographically.
LYMPHANGIOGRAPHY
TECHNIQUEAs with the techniques discussed above, plain radio-graphs are important to assess exposure and also to help rule out obvious diagnoses that could be responsi-ble for the clinical signs: lymphoedema, for example,may occur secondarily to infection or a neoplasticprocess that compresses or invades lymphatics, or evenprevious trauma, surgery or radiotherapy affecting thelocal lymphatic system. To complicate matters further,due to the close functional relationship between the lymphatic and venous systems, the clinical signs seen in some cases of large caudal retroperitoneal masses or cranial mediastinal masses can actually be due to problems in both systems. Moreover, chronic problemsassociated with venous return will be complicated bylymph drainage failure. Therefore, it is always worthchecking for signs of these abnormalities on the plainradiographs.
For studies of the distal limb, a few millilitres of contrast medium can be injected directly into the soft tissues distal to the area of interest or even into a lymph node if there is one distal to the abnormal area. Several radiographs of the area should then beobtained at regular intervals, the timing of which will depend largely on the speed at which the contrastmedium is cleared away from the injection site by the lymphatic system. This indirect technique is easier toperform than direct methods, where a dye (eg, methyleneblue) is injected into the soft tissues distal to the abnormality after which a catheter is placed under sterile conditions into one of the lymphatic vessels highlighted by the dye. While the direct technique offersbetter and more specific results, it is a challenging andmore expensive procedure that is far less likely to be performed in practice.
(left and above) Use of sinography ina patient presented for investigationof a chronic draining sinus followinga pharyngeal stick injury severalmonths previously. Contrast mediuminjected at the open wound reachesthe oesophagus (yellow arrows), but also highlights the fragment of wood, seen as a filling defectventral to the space between C2 and C3 in a vertical orientation
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

In Practice ● JA N U A R Y 200640
INTERPRETATIONThe interpretation of lymphangiograms is difficult as many vessels and collaterals can be highlighted by the contrast, and it is almost impossible to obtain a normal study to compare radiographs with, unless thecontralateral limb is radiographed after injecting thesame amount of contrast medium. Again, the generalprinciples of interpretation should be applied. Suspectlesions must be seen on two different radiographs; addi-tional orthogonal and oblique views can also be helpful.Huge numbers of collaterals, or dilated and tortuouslymphatic vessels must be treated with suspicion; whilecollateral vessels may help to delay or partially controlthe lymphoedema, and veins can, under these circum-stances, drain part of the lymph, there is no direct rela-tionship between their presence and the severity of theclinical signs.
Lymph node aplasia and small, blind-ending lym-phatic vessels are highly suggestive of primary lympho-edema, especially in young animals.
ReferencesCHRISTIANSEN, J. S., HOTTINGER, H. A., ALLEN, L., PHILLIPS, L. & ARONSON, L. R. (2000) Hepaticmicrovascular dysplasia in dogs: a retrospectivestudy of 24 cases (1987-1995). Journal of theAmerican Animal Hospital Association 36, 385-389LAMB, C. R. & DANIEL, G. B. (2002) Diagnosticimaging of dogs with suspected portosystemicshunting. Compendium on Continuing Educationfor the Practicing Veterinarian 24, 626-635MILLER, M. W., FOSSUM, T. W. & BAHR, A. M.(2002) Transvenous retrograde portography for identification and characterization ofportosystemic shunts in dogs. Journal of theAmerican Veterinary Medical Association 221,1574, 1586-1590SCRIVANI, P. V., YEAGER, A. E., DYKES, N. L. & SCARLETT, J. M. (2001) Influence of patientpositioning on sensitivity of mesentericportography for detecting an anomalousportosystemic blood vessel in dogs: 34 cases (1997-2000). Journal of the American VeterinaryMedical Association 219, 1251-1253
Further readingDAVIDSON, E. B., GRIFFEY, S. M., VASSEUR, P. B. & SHIELDS, S. L. (2000) Histopathological,radiographic, and arthrographic comparison of thebiceps tendon in normal dogs and dogs with bicepstenosynovitis. Journal of the American AnimalHospital Association 36, 522-530KIRBERGER, R. M., WRIGLEY, R. H., BARR, F. &DENNIS, R. (2001) Handbook of Small AnimalRadiological Differential Diagnosis. Philadelphia,W. B. SaundersWALLACK, S. T. (Ed) (2003) The Handbook ofVeterinary Contrast Radiography. San Diego, San Diego Veterinary Imaging
AcknowledgementsThe author would like to thank the Diagnostic Imaging Unit of the Animal Health Trust for the use of the radiographs on pages 32 to 38, and Dr Nuria Corzo-Menendez and Dr Jerry Davies for the images used on page 39. Thanks also to Dr Janet Daly, from the Centre for Preventive Medicine of the Animal Health Trust, for her help with the composition of this article.
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

doi: 10.1136/inpract.28.1.32 2006 28: 32-40In Practice
Francisco Llabres Diaz techniquesPractical contrast radiography 5. Other
http://inpractice.bmj.com/content/28/1/32Updated information and services can be found at:
These include:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on September 8, 2014 - Published by inpractice.bmj.comDownloaded from

![Review Article Side Effects of Radiographic Contrast Media ...downloads.hindawi.com/journals/bmri/2014/741018.pdf · hyperthyroidism following nonionic contrast radiography [ , ]](https://img.pdfslide.net/doc/110x75/5f21775c829d2f17996fe70c/review-article-side-effects-of-radiographic-contrast-media-hyperthyroidism-following.jpg)