Embed Size (px)
Citation preview

Practical Controversies in MS
Lucas McCarthy, MD, MSc
Neurologist, Director MS Center

© 2016 Virginia Mason Medical Center
Practical Controversies
How to approach common questions in the gray-zone of evidence-based practice?

© 2016 Virginia Mason Medical Center
The Evidence Free Zone

© 2016 Virginia Mason Medical Center
Practical Controversies in MS
• Misdiagnosis of MS
• Vitamin D testing / supplementation
• Use of complimentary / experimental treatments
• Treatment of Progressive MS

© 2016 Virginia Mason Medical Center
Poll Everywhere – Audience Participation
Open cell phone or laptop to following link to participate in live questions
https://pollev.com/MSsummit

Misdiagnosis of Multiple Sclerosis

© 2016 Virginia Mason Medical Center
Misdiagnosis of MS
Updated 2017 McDonald MS Diagnostic Criteria
Easier to diagnosis = Easier to misdiagnose?

© 2016 Virginia Mason Medical Center
MS Diagnosis – 2017 Updated Criteria
Lesions: ≥ 2 characteristic lesions (>3mm) in ≥ 2 different locations
Symptoms: objective clinical evidence of at least 1 lesion
Relapse: ≥ 1 characteristic clinical attack
Changes over Time: ≥2 CSF Oligoclonal bands or
>1 attack over time or
new lesions over time (including enhancing and non-enhancing)
*No other reasonable diagnosis

© 2016 Virginia Mason Medical Center
MS Diagnosis – Evolving Diagnostic Criteria
MS Diagnostic Criteria Comments
1965 - Schumacher Criteria 2 attacks of neurologic symptoms > 24 hours in duration,
separated by at least one month. No MRI yet
1983 - Poser Criteria Added cerebrospinal fluid (CSF) markers and Evoked
Potentials to diagnostic criteria. No MRI yet
2001 - McDonald Criteria Added MRI (commonly use since early 1990’s)
Classifications: "MS", "possible MS", or "not MS“
2005 –McDonald Criteria updated Added more MRI considerations; attention to enhancing
lesions and primary progressive MS (PPMS)
2010 – McDonald Criteria updated Added - Asymptomatic contrast enhancing lesion and non-
enhancing lesion = DIT
Earlier diagnosis possible
2017 - McDonald Criteria updated Added - +CSF and non-enhancing lesions = DIT; Enhancing
lesions do not have to be asymptomatic (except optic neuritis)
Even earlier diagnosis possible

© 2016 Virginia Mason Medical Center
MS Diagnosis – 2017 Updated Criteria
Using 2017 Criteria compared with 2010 MS Criteria:
23-27% more patients diagnosed with MS at first attack
Previously needed to wait until MRI change or second attack
Can make MS diagnosis easier now with 1st Attack and 1st MRI
Earlier Diagnosis, Earlier Treatment, Lower Future Disability
ECTRIMS 2018. Abstracts 139-142, presented October 11, 2018.

© 2016 Virginia Mason Medical Center
Exclude Others: Diseases that Mimic MSMultiple Sclerosis Differential Diagnosis
Autoimmune Infectious Genetic Other
Neurologic:
- Multiple Sclerosis
- Neuromyelitis Optica
- Autoimmune Encephalitis
- ADEM
- Susac’s Syndrome
- Hashimoto’s Encephalitis
- CLIPPERS
- CRION
Systemic:
- SLE (Lupus)
- APS
- Sjogren’s
- Sarcoidosis
- Behcet disease
- Celiac disease
- Paraneoplastic
HIV
Lyme
Syphilis
PML
Tuberculosis
Neuro-cysticercosis
Coccidiomycosis
Cryptococcus
Brucellosis
SSPE
HHV6
Whipple’s Disease
CADASIL
MELAS
Neurofibromatosis
Porphyria
Friedrich’s Ataxia
SCA
Adult Onset Leukodystrophy:
- Adreno-Leukodystrophy
- Metachromatic
- Alexander’s Disease
- Krabbe’s Disease
Neoplasm (Glioma, Lymphoma)
Vitamin B12 or Copper deficiency
Thiamine (B1) Deficiency
Vascular Malformations
Medication Effects (TNF-alpha)
Migraine Headache
ALS / Motor Neuron Disease
Compressive Myelopathy
Vascular:
- Stroke
- Amyloid Angiopathy
- Granulomatous Vasculitis
- Primary CNS Angiitis
- Moya-Moya Disease
Infiltrative:
- Langerhan’s Cell Histiocytosis
- Lymphomatoid Granulomatosis
- Erdheim-Chester Disease
- HLH

© 2016 Virginia Mason Medical Center
Haselink. Top Mag Reson Imaging. 2006

© 2016 Virginia Mason Medical Center
Haselink. Top Mag Reson Imaging. 2006

© 2016 Virginia Mason Medical Center
MS Mis-diagnosis
Caution on Overdiagnosis for the sake of naming
“My radiologist said it could be MS”
“My symptoms fit perfectly with MS”
”I just want an answer…”

© 2016 Virginia Mason Medical Center
Alternative Diagnosis in an MS Specialty Clinic
754 consecutive patients referred to an MS Center in the Netherlands:
67 % - MS or Probable MS (52% Definite, 15% Probable MS)
23 % - No Certain Diagnosis
7.7 % - Other Neurologic Disease
• 2.2 % Ischemic Cerebrovascular Disease
• 0.5 % Vasculitis
• 0.4 % Multi-System Atrophy
1.3% - Other Demyelinating Disease
Nielsen et al. Ann Neurol 2005

© 2016 Virginia Mason Medical Center
MS Misdiagnosis
18% Misdiagnosed with MS on second opinion
Previously diagnosed MS patients did not fit criteria for MS when seen for second opinion at an MS specialty center (UCLA / Cedars-Sinai)
Other Diagnosis:
1. Migraine headache (most common)
2. Radiologically Isolated Syndrome (RIS)
3. Cervical spinal stenosis
4. Peripheral Neuropathy
5. Optic NeuropathyKaisey et al. ECTRIMS 2018 MS Conference

© 2016 Virginia Mason Medical Center
Experimental Diagnostic Testing
Iquity RNA testing
Machine Learning Discrimination
Analysis of serum RNA

© 2016 Virginia Mason Medical Center
Experimental Diagnostic Testing
Iquity RNA testing
RNA expression levels of 30 genes in blood
199 subjects with MS,
203 subjects with other neurologic disorders,
114 healthy control subjects
Used to train machine learning algorithms.
Journal of Clinical Bioinformatics 2013

© 2016 Virginia Mason Medical Center
Experimental Diagnostic Testing
Iquity RNA testing

Vitamin D and Multiple Sclerosis

© 2016 Virginia Mason Medical Center
Vitamin D and MS
Cohort Evidence
Low Vitamin D serum levels associates with increased prevalence of MS, MRI lesions and relapses in RRMS
“Correlation does not equal Causation”
Just because something is associated, does not make it causal.
Low Vitamin D levels also correlate with risk for:
• Colon cancer, Breast cancer, Prostate cancer, Type 1+2 Diabetes;
Cardiovascular Disease; Dementia; Osteoperosis; Depression; Schizophrenia; Rheumatoid Arthritis

© 2016 Virginia Mason Medical Center
Vitamin D
Ascherio A, Munger KL, Simon KC. “Vitamin D and Multiple Sclerosis”. Lancet Neurol. 2010

© 2016 Virginia Mason Medical Center
Vitamin D
Ascherio A, Munger KL, Simon KC. “Vitamin D and Multiple Sclerosis”. Lancet Neurol. 2010
(25 – 60 ng/mL)

© 2016 Virginia Mason Medical Center
Low Vit D associated with New MRI Lesions
Each 10 ng/mL higher vitamin D level was associated ~32% reduced risk of a subsequent contrast-enhancing lesion (IRR=0.68, 95% CI [0.54, 0.86], p=0.001)

© 2016 Virginia Mason Medical Center
Vitamin D and MS
Vitamin D has anti-inflammatory actions in vitro1
- enhanced Th2 and decreased Th1 cytokine production
- dendritic cell effects
- enhanced macrophage phagocytosis
In experimental autoimmune encephalitis (EAE)2
• pre-induction treatment prevents disease development
• Post-induction treatment ameliorates disease activity
Genetic association of SNPs with Vitamin D and MS
1Smolders et al. Neuroimmunol 2008 2Vieth R. Am J Clin Nutr 1999

© 2016 Virginia Mason Medical Center
Institute of Medicine (IOM) Recommendations
"a considerable overestimation of the levels of vitamin D deficiency" exists in North America

© 2016 Virginia Mason Medical Center
High Dose Vitamin D Supplements in MS
Prior lower dose trials did not show significant benefits
Larger trials have been and are being done
Lets look at some – trend toward benefit, low risk for harm

© 2016 Virginia Mason Medical Center
High Dose Vitamin D Supplements
Seemingly safe at high doses (~10,000IU D3 daily) in RCTs
Burten, JM et al. A phase I/II dose-escalation trial of vitamin D3 and calcium in multiple sclerosis. Neurology 2010.
25 treated patients (49 total) spent 36+ weeks on doses of 10,000 IU/day D3 or greater. No significant side effects.
Sotirchos et al. Safety and immunologic effects of high vs low dose cholecalciferol in multiple sclerosis. Neurology 2016
20 treated patients (40 total) - 10,400IU vs. 800IU D3 in with RRMS x 6 months. No significant safety concerns. 1 Relapse in each group. Reductions in IL17 seen in treated group.

© 2016 Virginia Mason Medical Center
High Dose Vitamin D Supplements
Largest high dose Vitamin D trial to date:
SOLAR trial:
Smolders et al. “Efficacy of vitamin D3 as add-on therapy in patients with relapsing-remitting multiple sclerosis receiving subcutaneous interferon β-1a”. ECTRIMS 2016
229 MS patients
Taking Interferon β-1a sc alreadyAge 18 - 55
Vitamin D levels < 150nmol/ml (60ng/ml)
Randomized to 14,000IU D3 (VigantOL Oil) vs. placebo
48 Weeks duration*reported but unpublished
data

© 2016 Virginia Mason Medical Center
SOLAR Trial Results
Poor recruitment – reduced study duration from 96 to 48 week
*Primary Endpoint: % Disease Activity Free (NEDA)
No relapses, no EDSS progression, no new or enhancing lesions
Results Reported : https://clinicaltrials.gov/ct2/show/results/NCT01285401
Presented: Ectrims 2016
Endpoint
Vitamin D3
14,000
(n = 113)
Placebo
(n = 116)Difference P Value
*Disease
Activity Free (%)37.2 35.3 1.9% 0.912
Relapse Free (%) 78.8 75.0 3.8%
Annualized
Relapse Rate0.28 0.41 31.7% 0.165
New/Active MRI
Lesions (mean)1.09 1.49 32% 0.0005

© 2016 Virginia Mason Medical Center
Vitamin D Supplementation Trials
Camu et al. Cholecalciferol supplementation in relapsing multiple sclerosis patients treated with subcutaneous interferon beta-1a: a randomized, controlled trial. ECTRIMS 2016. Abstract P750
129 pts, randomized placebo controlled trial; 2 year duration
100,000IU D3 q2 weeks (7,143IU / day) + IFNB-1a
Results: No benefit for MS relapse (ARR 0.34 vs. 0.45, p = 0.38)
Subgroup analysis: per protocol, completers (90 out of 129):
- ARR reduction – RR 0.40, p = 0.011
- New T2 lesions – RR 0.23, p < 0.001
- New T1 lesions – RR 0.22, p = 0.001*reported but unpublished
data

© 2016 Virginia Mason Medical Center
Vitamin D Supplementation Trials
Koduah et al. Vitamin D supplementation in multiple sclerosis: primary efficacy endpoint and safety of a randomized, controlled, double-blind phase II trial (EVIDIMS). ECTRIMS 2018.
EVIDIMS trial - German multicenter RCT
Patients: 53 pts with CIS or MS on IFNB-1b
Intervention: equivalent to 10,200 IU vs. 200 IU D3 Daily x 18mo
Primary Outcome: New T2 lesions – no significant difference
*reported but unpublished
data

© 2016 Virginia Mason Medical Center
Evidence

© 2016 Virginia Mason Medical Center
Systematic Review – Vit D and MS
Jagannath VA et al. Vitamin D for the management of multiple sclerosis. Cochrane Database Syst Rev. 2018 Sep 24
12 RCTs including 933 subjects in years 2010 – 2017
464 in vitamin D group, 469 in comparison groups

© 2016 Virginia Mason Medical Center
Systematic Review – Vit D and MS
No Significant Differences:
Annualized Relapse Rate (ARR) - difference = -0.05 (-0.17 to 0.07)
from five trials; 417 participants
EDSS – mean difference = -0.25, (-0.61 to 0.10)
from five trials; 221 participants
MRI Gad enhancing lesions – difference = 0.02, (-0.45 to 0.48) two trials; 256 participants

© 2016 Virginia Mason Medical Center
Systematic Reviews – Vit D and MS
Jagannath VA et al. Cochrane Database Syst Rev. 2018 Sep 24
“evidence suggests no benefit of vitamin D for patient‐important outcomes
among people with MS”
McLaughlin et al. J Neurol. 2018
“No statistically significant difference was seen for any of the outcome
measures. There were non-significant trends in favour of vitamin D for all
outcome measures”
Zheng et al. Mult Scler Relat Disord. 2018 Jul
“Our findings suggest that vitamin D appeared to have no therapeutic effect
on EDSS score or ARR in the patients with MS.”

© 2016 Virginia Mason Medical Center
Vitamin D Supplementation – Risks
Meta-analysis
Serious Adverse Events – difference = 1%, (-3% to 4%)
Minor Adverse Effects – difference = 2%, (-2% to 6%)
Cost of Testing: Vit D-25(OH)- $96 (range $33 – $231)1
IOM Report 2011:
• >4000IU D3 daily supplement not recommended
• levels >50–60 ng/mL should be avoided
• “are associated with increases in all-cause mortality, greater risk of cancer at some sites like the pancreas, greater risk of cardiovascular events, and more falls and fractures among the elderly”
1Healthcarebluebook.com; Accessed 3/2019; 2NIH Office of Dietary Supplements
https://ods.od.nih.gov/factsheets/VitaminD-HealthProfessional/

© 2016 Virginia Mason Medical Center
Vitamin D Status
Institute of medicine Endocrine society
Vitamin D status
“Deficient” – ≤ 20 ng/mL (≤ 50 nmol/L)
“Insufficient” – 21–29 ng/mL (51–74 nmol/L)
“Sufficient” 20 ng/mL (50 nmol/L) ≥ 30 ng/mL (≥ 75 nmol/L)
“Ideal” – 40–60 ng/mL (100–150 nmol/L)
Considered “safe” – ≤ 100 ng/mL (≤ 250 nmol/L)
Daily vitamin D intake recommendations (upper limit recommendation)
Infants 400 IU/day 400–1000 IU/day
Children 600 IU/day (2500–3000 IU/day) 600–1000 IU/day (4000 IU/day)
Adults 600 IU/day (4000 IU/day),
800 IU/day for seniors
1500–2000 IU/day (10,000 IU/day)

© 2016 Virginia Mason Medical Center
Ongoing Clinical Trials
VIDAMS trial: Vitamin D to Ameliorate MS
Ellen Mowry, MD at Johns Hopkins; Recruiting 2012 – 2019
Patients: 172 pts with RRMS; age 18 – 50, EDSS ≤ 4
Intervention: 600 IU vs. 5,000 IU D3 + Glatiramer Acetate
Primary outcome: Relapses
Secondary outcomes: MRI lesions, EDSS, brain volume, OCT, LCVA

© 2016 Virginia Mason Medical Center
Options for MS Providers
Do not recommend supplements until more evidence
- pros: saves costs and unnecessary supplementation
- cons: risk ‘missing out’ on treatment if beneficial
’Blindly’ recommend supplements to all
e.g. 2,000IU D3 daily (200% RDA for adults)
- pros: saves costs of testing, possible benefits for multiple diseases
- cons: unnecessary for those not deficient?, cost of supplements
Test Vitamin D levels and Supplement if lower than ’goal’
- pros: avoids unnecessary supplementation
- cons: costs of labs (not covered) and supplements, unclear if beneficial, no goal levels established

Off Label Use of Experimental Complimentary MS Disease Modifying Therapy

© 2016 Virginia Mason Medical Center
Repairing / Preventing MS Damage?
Current MS Drugs prevent but do not likely help with repair
Many off-label medications and supplements have been studied
Some may recommend these therapies to their patients

© 2016 Virginia Mason Medical Center
Repairing / Preventing MS Damage?
Off label medications or SupplementsUnder Investigation for MS Repair / Slowing Degeneration:
• Biotin
• Clemastine
• Simvastatin
• Alpha Lipoic Acid
• Phenytoin
• Minocycline

© 2016 Virginia Mason Medical Center
Updates – Biotin for progressive MS?
High dose Biotin (MD1003) for improvements in Progressive MS
First trial in France in 154 patients, progressive MS, 12 month trial
12.6% had improvements in disability at 1 year
MS Journal 9/2016

© 2016 Virginia Mason Medical Center
High dose Biotin (MD1003) for improvements in Progressive MS
In extension trial for 1 more year, all groups given Biotin
Initially given Placebo, patients given Biotin had improvements 11.9% disability improvement at 1 year extension
MS Journal 9/2016
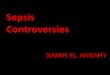
MD1003 (Biotin) Reduced MS Progression

© 2016 Virginia Mason Medical Center
MD1003 (Biotin) Reduced MS Progression
Tourbah et al. MS Journal 2016
Other Progressive MS Trials
Placebo group
MD1003 (Biotin) Group
Switched to MD1003 (Biotin)
Worse
Disability

© 2016 Virginia Mason Medical Center
Ongoing Phase III Trial - High Dose Biotin
100,000mcg Biotin (proprietary) TID vs. Placebo
Patients with primary or secondary progressive MS
Add on therapy to current stable Disease Modifying MS Medication
Typical dosing OTC – 5,000mcg Biotin Daily
Safety is good compared to placebo, can cause Blood Test Abnormalities (e.g. Thyroid studies, Troponin)

© 2016 Virginia Mason Medical Center
Clemastine Fumarate for MS Repair?
A repurposed non-prescription sedating anti-histamine
(similar to Benadryl in mechanism of action)
Clemastine studied for repair of Optic Nerve damage in MS

© 2016 Virginia Mason Medical Center
Clemastine Fumarate for MS Repair?
A repurposed non-prescription anti-histamine for MS?
Clemastine studied for remyelination of Optic Neuritis in MS
Small Pilot Trial – 50 patients (25 on drug, 25 on placebo)
Small significant improvement in VEP electrical response
(1.7ms speed improvement, average speed ~105ms)
Ongoing Larger trial - NCT02521311
ReCOVER Trial, 90 pts, Acute Optic Neuritis, Clemastine vs. Placebo
3 months of treatment, then monitoring for 9 monthsGreen et al. Lancet, 10/2017

© 2016 Virginia Mason Medical Center
Simvastatin for MS

© 2016 Virginia Mason Medical Center
Simvastatin for MS
MS STAT 1 Trial
N=140
18-65 yrs old
EDSS 4.0 – 6.5
no relapses or steroid use in 3 months
No DMT use in last 6 months

© 2016 Virginia Mason Medical Center
Simvastatin for MS
• Relative Brain Atrophy reduced by 43% vs. Placebo
• Absolute Brain Atrophy Rate reduced by 0.25%/year
• 0.28% in Simvastatin vs. 0.58% in Placebo per year, p = 0.003
Perspective:
FREEDOMS 2010 Fingolimod study
Brain Volume Changes 12-24mo:
0.37% in Fingolimod 0.5mg vs. 0.67% in Placebo, p = 0.002
MS STAT2 Trial – ongoing (NCT03387670)
1180 patients, 40 vs. 80mg vs. Placebo x 35 months; no DMT use

© 2016 Virginia Mason Medical Center
Alpha Lipoic Acid for MS
SPMS aged 40–70 years
Enrolled in a single center, (OHSU)
2-year, double-blind, randomized trial
1,200 mg LA daily vs placebo
Spain et al. Neurol Neuroimmunol Neuroinflamm 2017

© 2016 Virginia Mason Medical Center
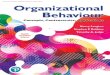
Alpha Lipoic Acid for MS
68% reduction in annualized percent change in brain volume (slowed decline)
Spain et al. Neurol Neuroimmunol Neuroinflamm 2017
Annualized Brain
Volume Loss
LA -0.21%
Placebo -0.65%
COMPARISONS:
MS STAT Trial
-0.28 % vs. -0.58%
FREEDOMS Trial
-0.37% vs. -0.67%

© 2016 Virginia Mason Medical Center
Use of Experimental Therapy
Ongoing placebo controlled clinical trials:
• Biotin
• Simvastatin
• Alpha Lipoic Acid
• Clemastine
Equipoise – uncertainty of differences, null hypothesis
Use of off-label therapies outside of clinical trials

Thank you