Embed Size (px)
Citation preview

5/28/2016
1
Practical Issues in Serrated Colorectal Polyps
Wendy L Frankel, MDChair of Pathology
Director of GI/Liver Pathology Fellowship
� Serrated polyps-definitions
� Differential and mimics� Serrated pathway to
microsatellite unstable (MSI) colorectal carcinoma
Outline
A. Traditional serrated adenoma (TSA)
B. Hyperplastic polyp (HP)
C. Sessile serrated adenoma/polyp (SSA/P)
D. SSA/P with dysplasia
E. Tubulovillous adenoma (TVA)
A. B. C. D. E.
53%
2%
20%
4%
22%
What is Your Diagnosis? Colorectal Polyps
� Adenomas and hyperplastic polyps used to be easy
� Adenomas precursors to cancer; genetic alterations in tumor suppressor genes (APC, p53) and oncogenes (KRAS)
� Hyperplastic polyps not
� Or are they??
5/28/2016
2
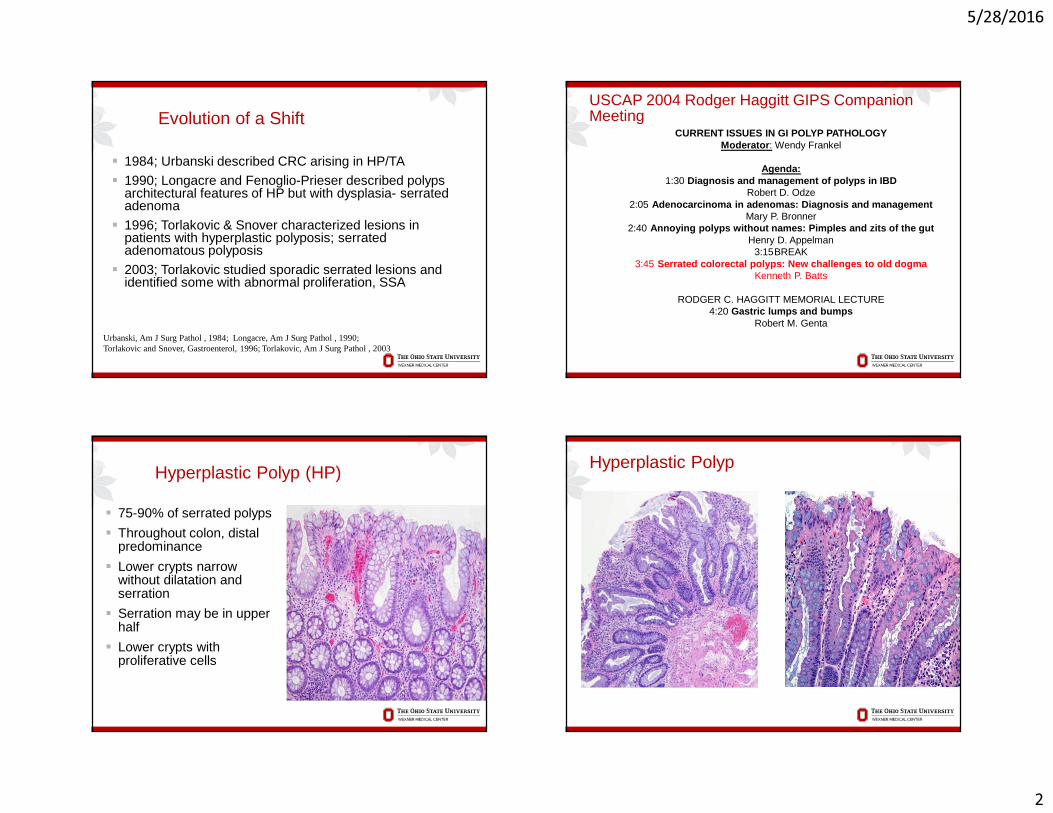
Evolution of a Shift
� 1984; Urbanski described CRC arising in HP/TA
� 1990; Longacre and Fenoglio-Prieser described polyps architectural features of HP but with dysplasia- serrated adenoma
� 1996; Torlakovic & Snover characterized lesions in patients with hyperplastic polyposis; serrated adenomatous polyposis
� 2003; Torlakovic studied sporadic serrated lesions and identified some with abnormal proliferation, SSA
Urbanski, Am J Surg Pathol , 1984; Longacre, Am J Surg Pathol , 1990; Torlakovic and Snover, Gastroenterol, 1996; Torlakovic, Am J Surg Pathol , 2003
CURRENT ISSUES IN GI POLYP PATHOLOGYModerator: Wendy Frankel
Agenda:1:30 Diagnosis and management of polyps in IBD
Robert D. Odze2:05 Adenocarcinoma in adenomas: Diagnosis and management
Mary P. Bronner2:40 Annoying polyps without names: Pimples and zits of the gut
Henry D. Appelman3:15BREAK
3:45 Serrated colorectal polyps: New challenges to old dogmaKenneth P. Batts
RODGER C. HAGGITT MEMORIAL LECTURE4:20 Gastric lumps and bumps
Robert M. Genta
USCAP 2004 Rodger Haggitt GIPS Companion Meeting
Hyperplastic Polyp (HP)
� 75-90% of serrated polyps
� Throughout colon, distal predominance
� Lower crypts narrow without dilatation and serration
� Serration may be in upper half
� Lower crypts with proliferative cells
Hyperplastic Polyp
5/28/2016
3
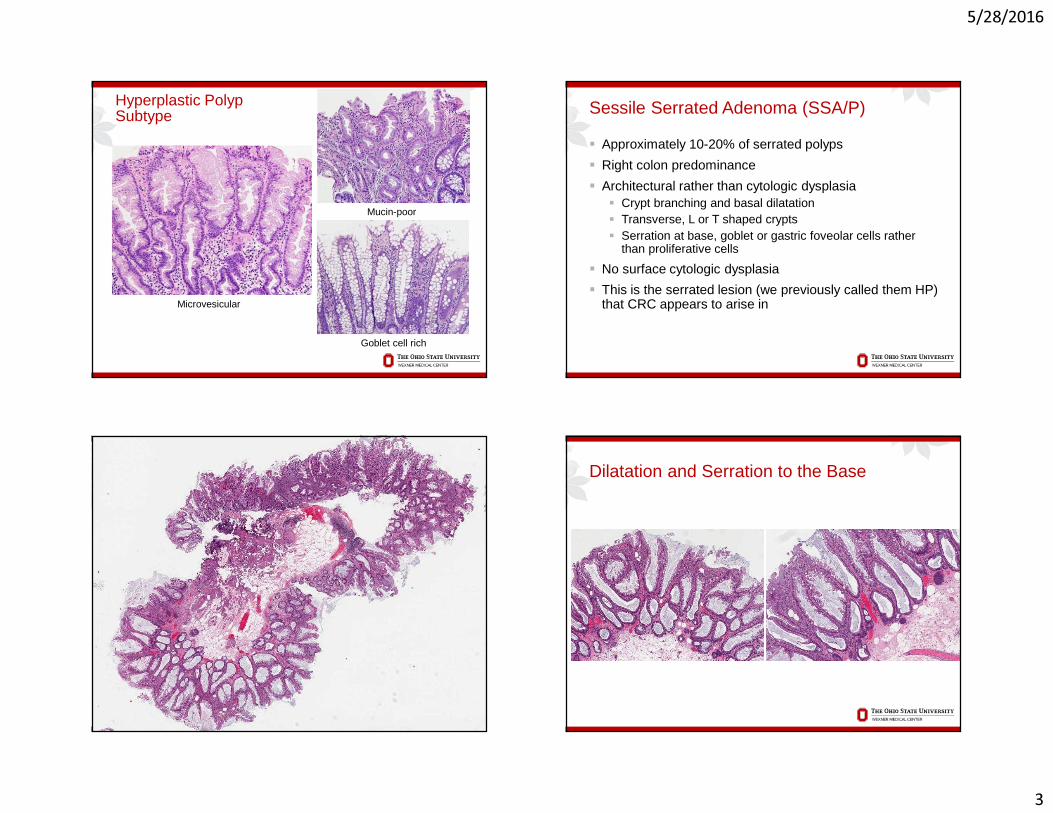
Hyperplastic PolypSubtype
Microvesicular
Mucin-poor
Goblet cell rich
Sessile Serrated Adenoma (SSA/P)
� Approximately 10-20% of serrated polyps
� Right colon predominance
� Architectural rather than cytologic dysplasia� Crypt branching and basal dilatation� Transverse, L or T shaped crypts� Serration at base, goblet or gastric foveolar cells rather
than proliferative cells
� No surface cytologic dysplasia
� This is the serrated lesion (we previously called them HP) that CRC appears to arise in
Dilatation and Serration to the Base
5/28/2016
4
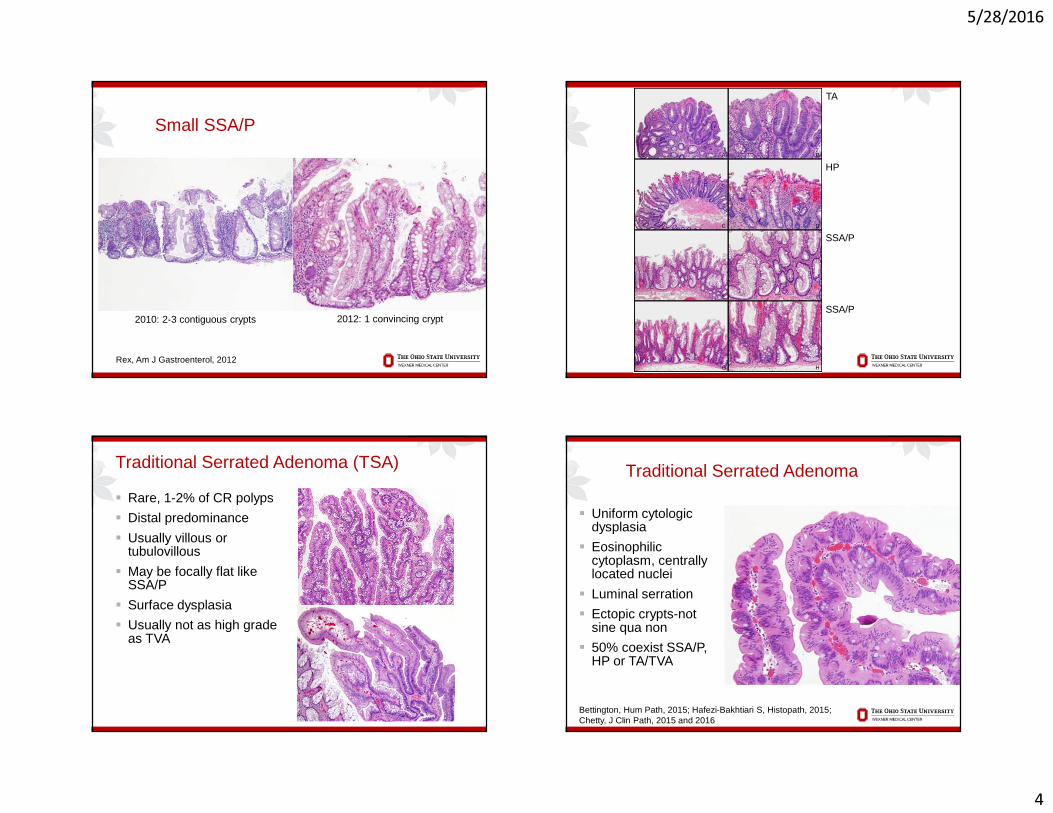
Small SSA/P
2012: 1 convincing crypt2010: 2-3 contiguous crypts
Rex, Am J Gastroenterol, 2012
TA
HP
SSA/P
SSA/P
Traditional Serrated Adenoma (TSA)
� Rare, 1-2% of CR polyps
� Distal predominance
� Usually villous or tubulovillous
� May be focally flat like SSA/P
� Surface dysplasia
� Usually not as high grade as TVA
Traditional Serrated Adenoma
� Uniform cytologicdysplasia
� Eosinophilic cytoplasm, centrally located nuclei
� Luminal serration
� Ectopic crypts-not sine qua non
� 50% coexist SSA/P, HP or TA/TVA
Bettington, Hum Path, 2015; Hafezi-Bakhtiari S, Histopath, 2015; Chetty, J Clin Path, 2015 and 2016
5/28/2016
5
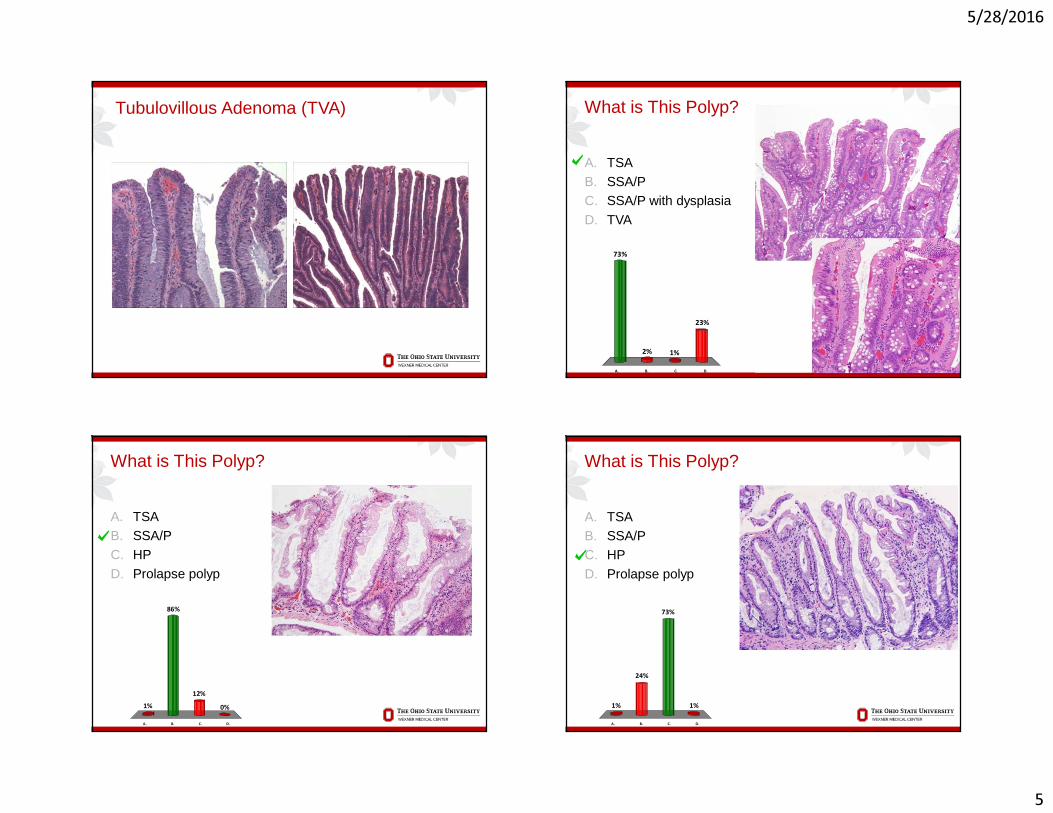
Tubulovillous Adenoma (TVA)
A. TSAB. SSA/PC. SSA/P with dysplasia
D. TVA
What is This Polyp?
A. B. C. D.
73%
23%
1%2%
A. TSAB. SSA/PC. HP
D. Prolapse polyp
What is This Polyp?
A. B. C. D.
1% 0%
12%
86%
A. TSAB. SSA/PC. HP
D. Prolapse polyp
What is This Polyp?
A. B. C. D.
1% 1%
73%
24%
5/28/2016
6
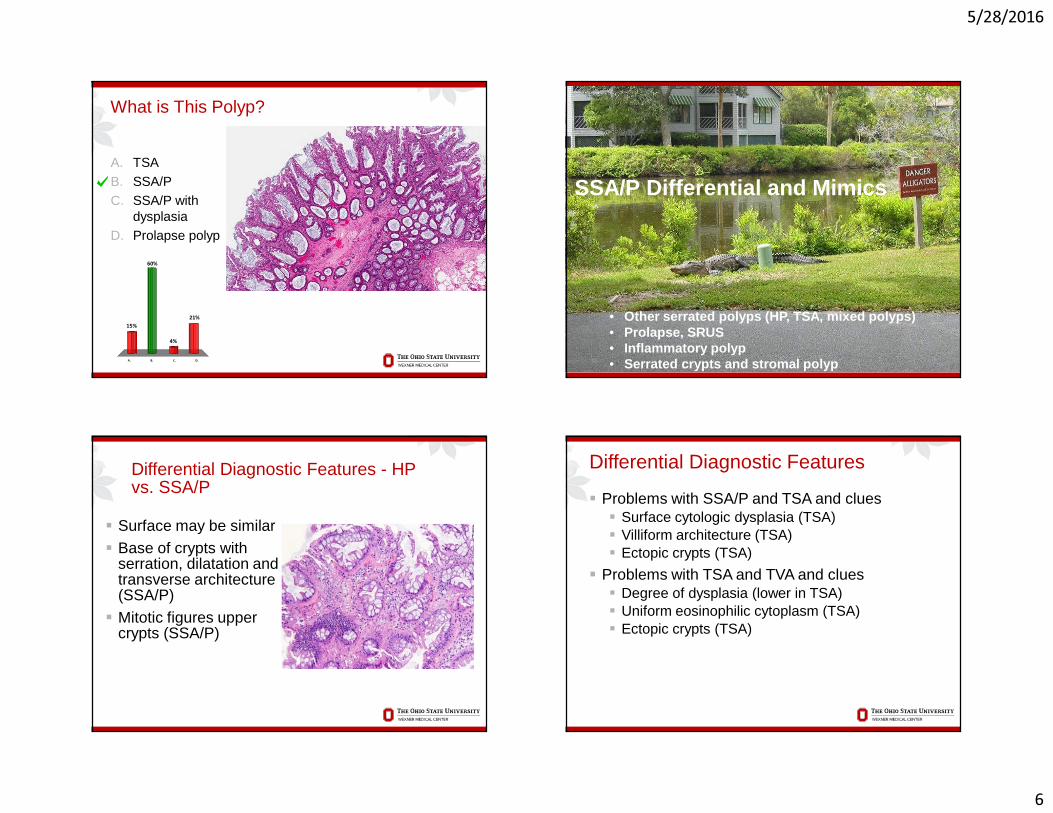
A. TSAB. SSA/PC. SSA/P with
dysplasiaD. Prolapse polyp
What is This Polyp?
A. B. C. D.
15%21%
4%
60%
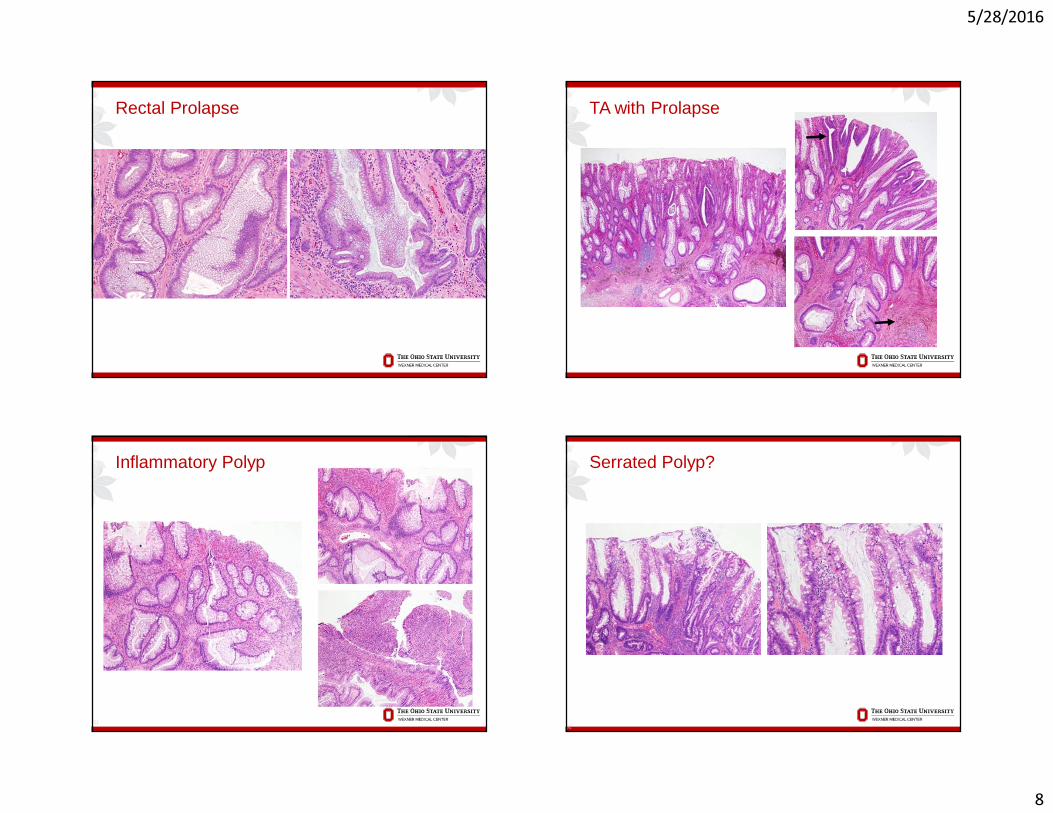
• Other serrated polyps (HP, TSA, mixed polyps)• Prolapse, SRUS• Inflammatory polyp• Serrated crypts and stromal polyp
SSA/P Differential and Mimics
Differential Diagnostic Features - HP vs. SSA/P
� Surface may be similar� Base of crypts with
serration, dilatation and transverse architecture (SSA/P)
� Mitotic figures upper crypts (SSA/P)
Differential Diagnostic Features
� Problems with SSA/P and TSA and clues� Surface cytologic dysplasia (TSA) � Villiform architecture (TSA)� Ectopic crypts (TSA)
� Problems with TSA and TVA and clues� Degree of dysplasia (lower in TSA)� Uniform eosinophilic cytoplasm (TSA)� Ectopic crypts (TSA)
5/28/2016
7
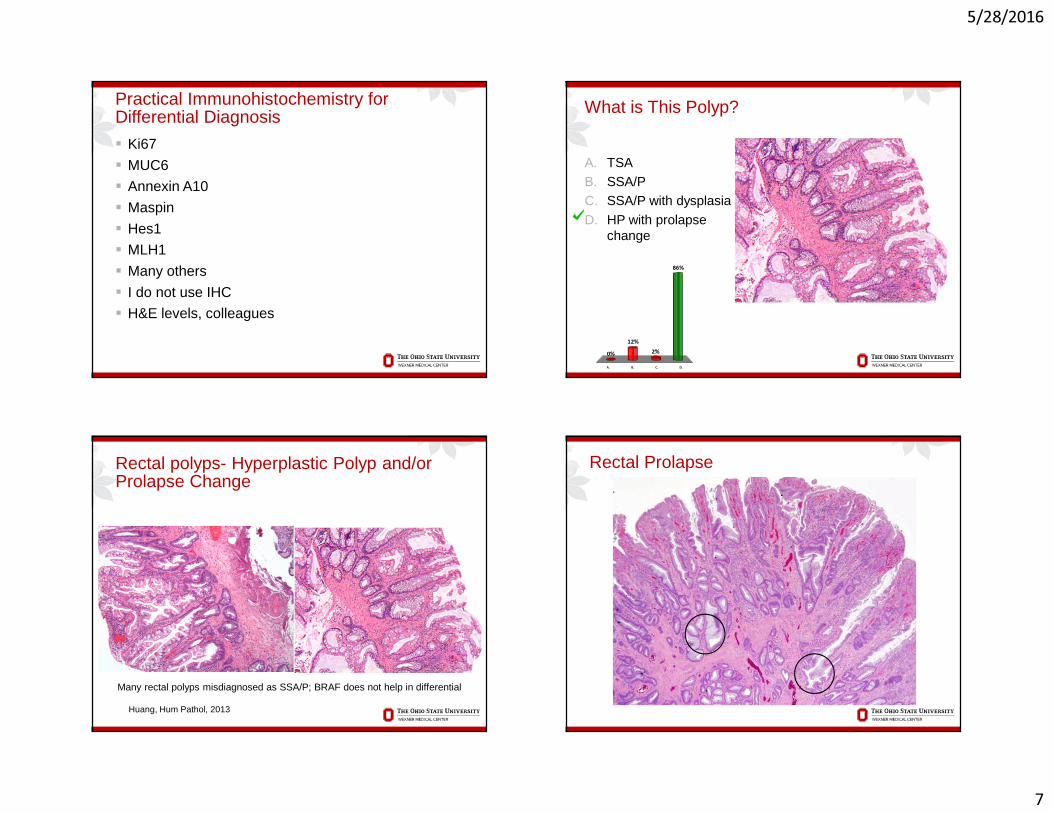
Practical Immunohistochemistry for Differential Diagnosis
� Ki67
� MUC6
� Annexin A10
� Maspin
� Hes1
� MLH1
� Many others
� I do not use IHC
� H&E levels, colleagues
A. TSAB. SSA/PC. SSA/P with dysplasia
D. HP with prolapse change
What is This Polyp?
A. B. C. D.
0%
86%
2%12%
Rectal polyps- Hyperplastic Polyp and/or Prolapse Change
Huang, Hum Pathol, 2013
Many rectal polyps misdiagnosed as SSA/P; BRAF does not help in differential
Rectal Prolapse
5/28/2016
8
Rectal Prolapse TA with Prolapse
Inflammatory Polyp
31
Serrated Polyp?
32
5/28/2016
9
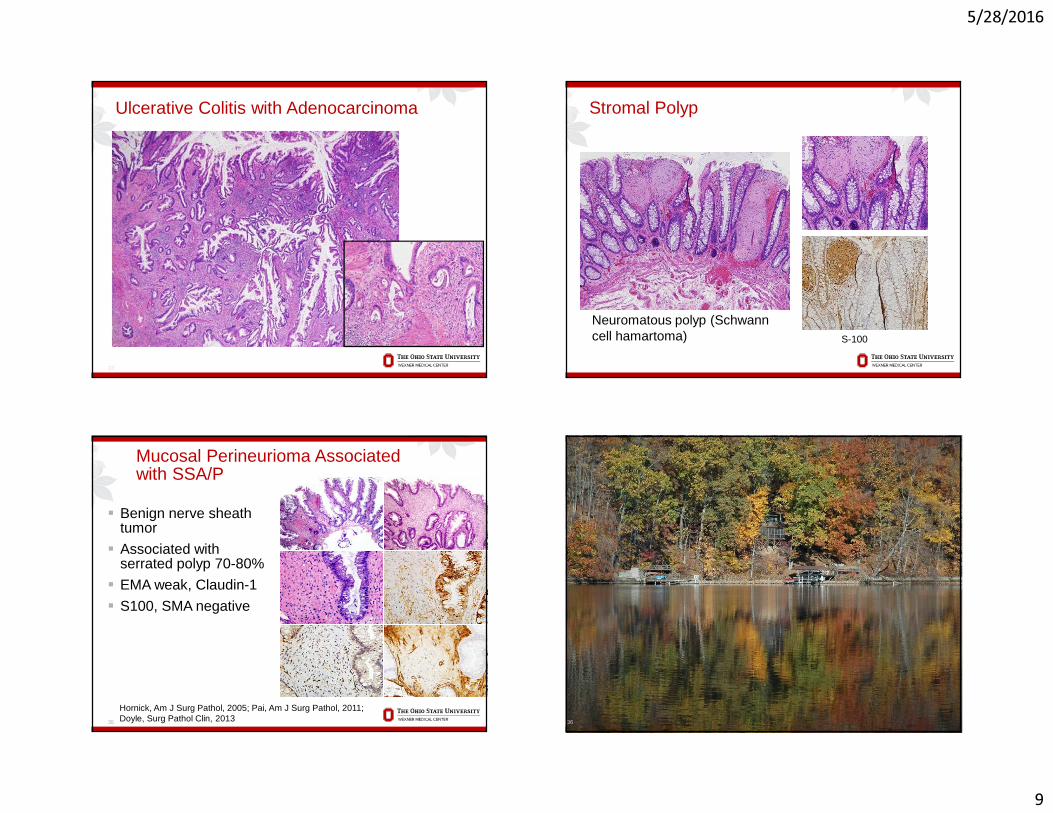
Ulcerative Colitis with Adenocarcinoma
33
Stromal Polyp
S-100
Neuromatous polyp (Schwann cell hamartoma)
Mucosal Perineurioma Associated with SSA/P
� Benign nerve sheath tumor
� Associated with serrated polyp 70-80%
� EMA weak, Claudin-1
� S100, SMA negative
35
Hornick, Am J Surg Pathol, 2005; Pai, Am J Surg Pathol, 2011; Doyle, Surg Pathol Clin, 2013 36
5/28/2016
10
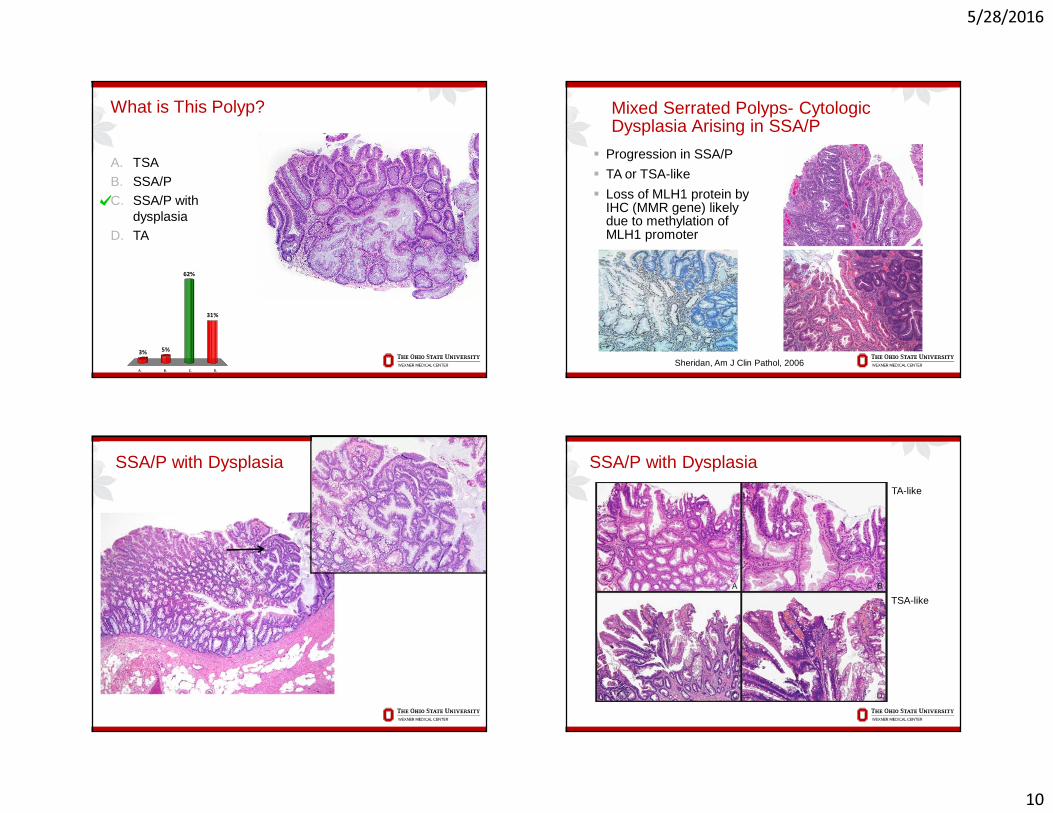
A. TSAB. SSA/PC. SSA/P with
dysplasiaD. TA
What is This Polyp?
A. B. C. D.
3%
31%
62%
5%
Mixed Serrated Polyps- CytologicDysplasia Arising in SSA/P
� Progression in SSA/P
� TA or TSA-like
� Loss of MLH1 protein by IHC (MMR gene) likely due to methylation of MLH1 promoter
Sheridan, Am J Clin Pathol, 2006
SSA/P with Dysplasia SSA/P with Dysplasia
TA-like
TSA-like
5/28/2016
11
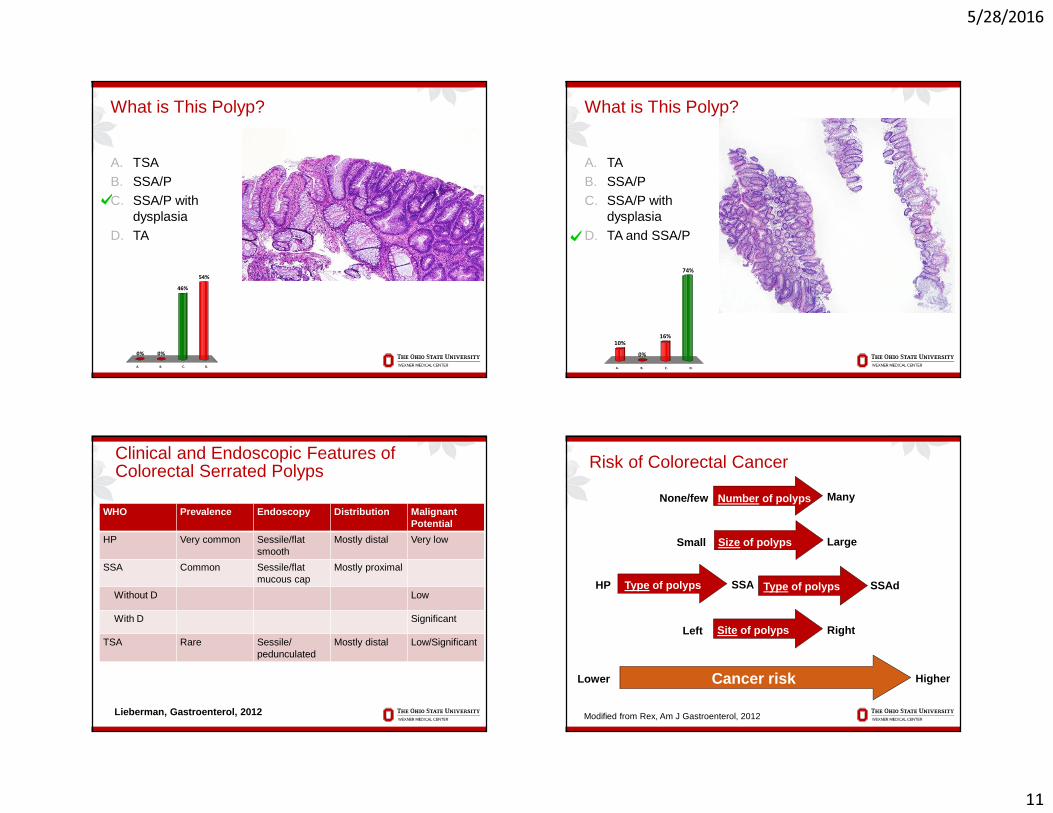
A. TSAB. SSA/PC. SSA/P with
dysplasiaD. TA
What is This Polyp?
A. B. C. D.
0%
54%
46%
0%
A. TAB. SSA/PC. SSA/P with
dysplasiaD. TA and SSA/P
What is This Polyp?
A. B. C. D.
10%
74%
16%
0%
Clinical and Endoscopic Features of Colorectal Serrated Polyps
WHO Prevalence Endoscopy Distribution Malignant Potential
HP Very common Sessile/flatsmooth
Mostly distal Very low
SSA Common Sessile/flatmucous cap
Mostly proximal
Without D Low
With D Significant
TSA Rare Sessile/pedunculated
Mostly distal Low/Significant
Lieberman, Gastroenterol, 2012
Risk of Colorectal Cancer
Modified from Rex, Am J Gastroenterol, 2012
Number of polyps
Size of polyps
Type of polyps
Site of polyps
Cancer risk
None/few
Small
HP
Left
Lower
Many
Large
SSA
Right
Higher
Type of polypsType of polyps SSAd
5/28/2016
12
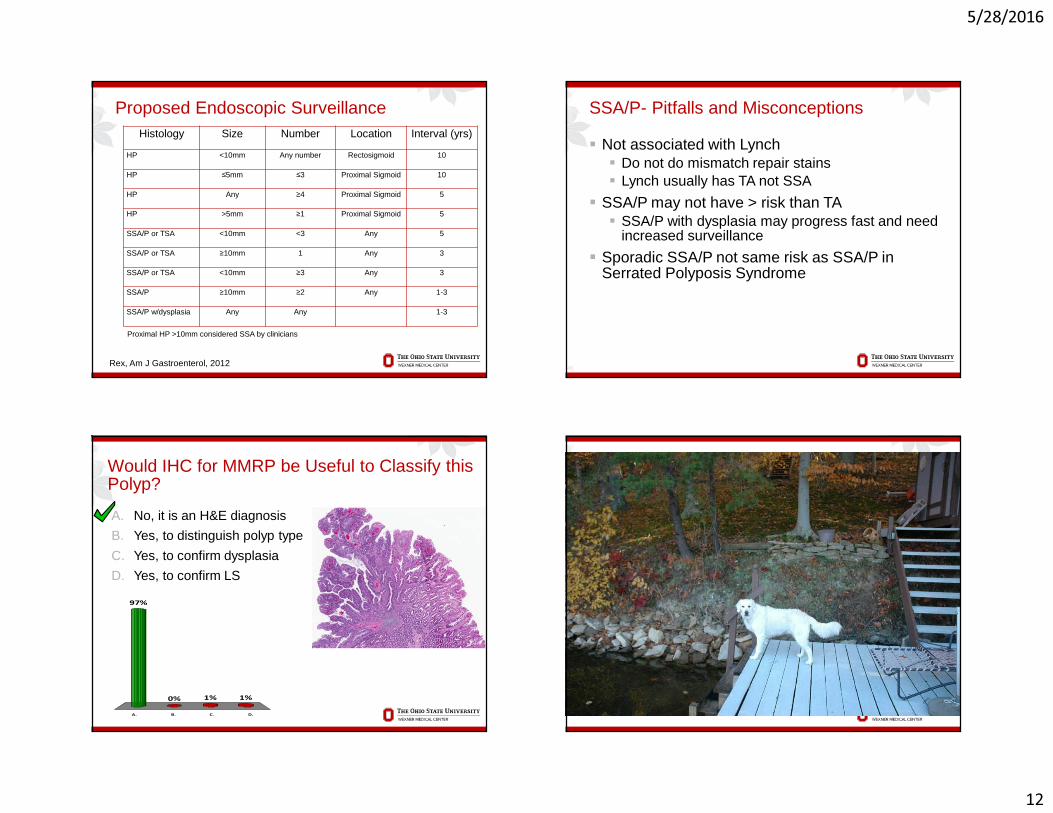
Histology Size Number Location Interval (yrs)
HP <10mm Any number Rectosigmoid 10
HP ≤5mm ≤3 Proximal Sigmoid 10
HP Any ≥4 Proximal Sigmoid 5
HP >5mm ≥1 Proximal Sigmoid 5
SSA/P or TSA <10mm <3 Any 5
SSA/P or TSA ≥10mm 1 Any 3
SSA/P or TSA <10mm ≥3 Any 3
SSA/P ≥10mm ≥2 Any 1-3
SSA/P w/dysplasia Any Any 1-3
Proposed Endoscopic Surveillance
Rex, Am J Gastroenterol, 2012
Proximal HP >10mm considered SSA by clinicians
SSA/P- Pitfalls and Misconceptions
� Not associated with Lynch� Do not do mismatch repair stains� Lynch usually has TA not SSA
� SSA/P may not have > risk than TA� SSA/P with dysplasia may progress fast and need
increased surveillance
� Sporadic SSA/P not same risk as SSA/P in Serrated Polyposis Syndrome
46
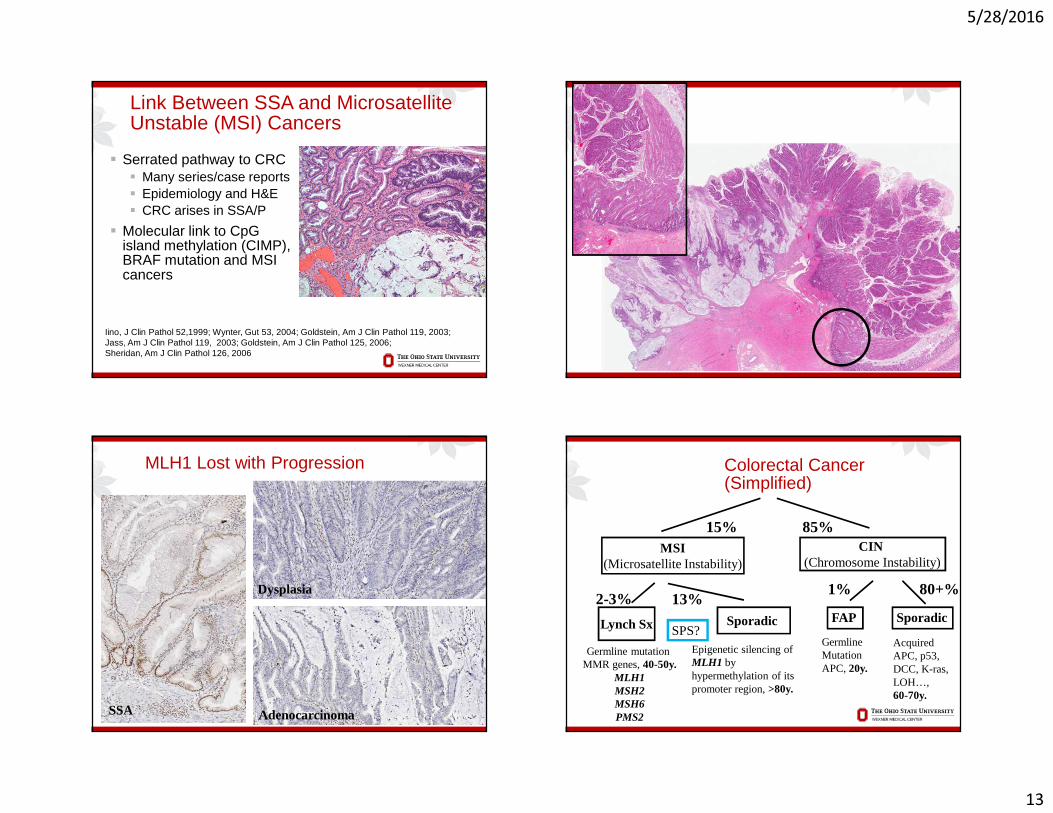
A. No, it is an H&E diagnosis
B. Yes, to distinguish polyp type
C. Yes, to confirm dysplasia
D. Yes, to confirm LS
A. B. C. D.
97%
1%1%0%
Would IHC for MMRP be Useful to Classify this Polyp?
5/28/2016
13
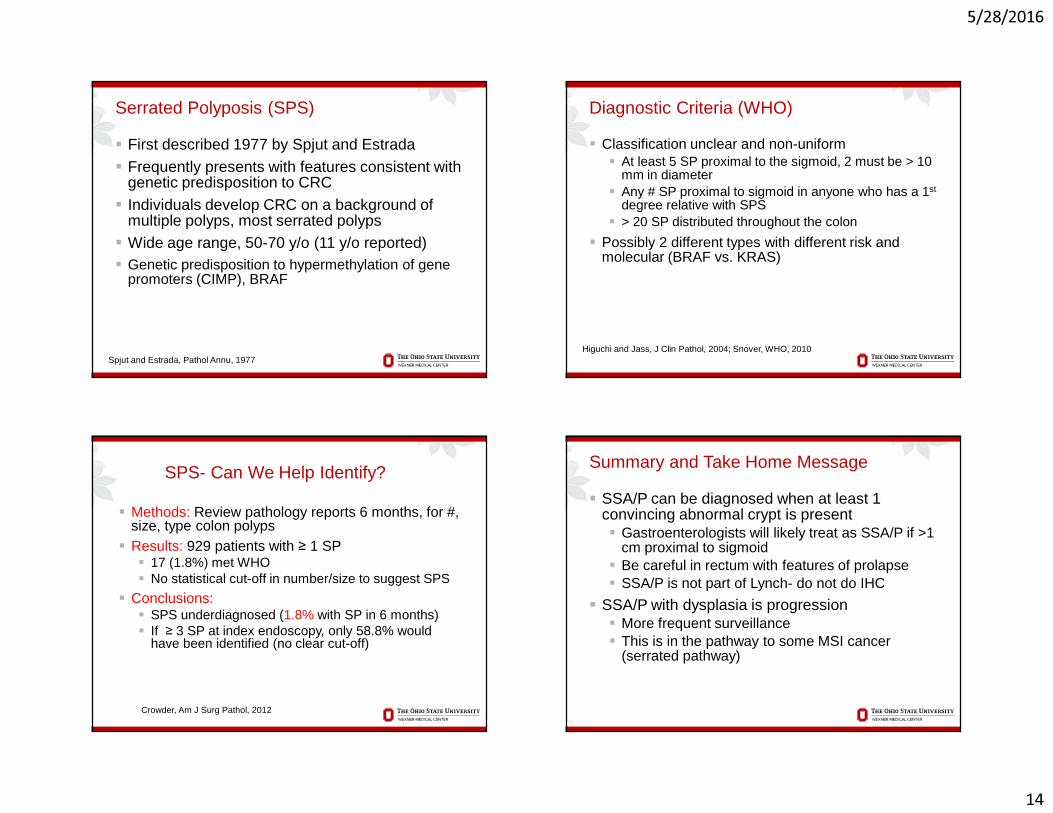
Link Between SSA and Microsatellite Unstable (MSI) Cancers
� Serrated pathway to CRC� Many series/case reports� Epidemiology and H&E� CRC arises in SSA/P
� Molecular link to CpGisland methylation (CIMP), BRAF mutation and MSI cancers
Iino, J Clin Pathol 52,1999; Wynter, Gut 53, 2004; Goldstein, Am J Clin Pathol 119, 2003;Jass, Am J Clin Pathol 119, 2003; Goldstein, Am J Clin Pathol 125, 2006; Sheridan, Am J Clin Pathol 126, 2006
MLH1 Lost with Progression
SSA
Dysplasia
Adenocarcinoma
13%1% 80+%
FAP Sporadic
MSI(Microsatellite Instability)
CIN(Chromosome Instability)
Lynch Sx Sporadic
Germline mutation MMR genes, 40-50y.
MLH1MSH2MSH6PMS2
15%
2-3%
Epigenetic silencing of MLH1 by hypermethylation of its promoter region, >80y.
85%
Colorectal Cancer(Simplified)
Acquired APC, p53, DCC, K-ras, LOH…,60-70y.
Germline Mutation APC, 20y.
SPS?
5/28/2016
14
Serrated Polyposis (SPS)
� First described 1977 by Spjut and Estrada� Frequently presents with features consistent with
genetic predisposition to CRC� Individuals develop CRC on a background of
multiple polyps, most serrated polyps� Wide age range, 50-70 y/o (11 y/o reported)� Genetic predisposition to hypermethylation of gene
promoters (CIMP), BRAF
Spjut and Estrada, Pathol Annu, 1977
Diagnostic Criteria (WHO)
� Classification unclear and non-uniform� At least 5 SP proximal to the sigmoid, 2 must be > 10
mm in diameter� Any # SP proximal to sigmoid in anyone who has a 1st
degree relative with SPS� > 20 SP distributed throughout the colon
� Possibly 2 different types with different risk and molecular (BRAF vs. KRAS)
Higuchi and Jass, J Clin Pathol, 2004; Snover, WHO, 2010
SPS- Can We Help Identify?
� Methods: Review pathology reports 6 months, for #, size, type colon polyps
� Results: 929 patients with ≥ 1 SP� 17 (1.8%) met WHO� No statistical cut-off in number/size to suggest SPS
� Conclusions:� SPS underdiagnosed (1.8% with SP in 6 months)� If ≥ 3 SP at index endoscopy, only 58.8% would
have been identified (no clear cut-off)
Crowder, Am J Surg Pathol, 2012
Summary and Take Home Message
� SSA/P can be diagnosed when at least 1 convincing abnormal crypt is present� Gastroenterologists will likely treat as SSA/P if >1
cm proximal to sigmoid� Be careful in rectum with features of prolapse� SSA/P is not part of Lynch- do not do IHC
� SSA/P with dysplasia is progression� More frequent surveillance� This is in the pathway to some MSI cancer
(serrated pathway)
56
5/28/2016
15
57 Thanks, Questions?






![UvA-DARE (Digital Academic Repository) Serrated polyps ... · Processed on: 12-12-2016 507009-L-bw-Ijspeert CHAPTER 3 }v }( }oÇ v serrated polyposis syndrome in colorectal v v]vP](https://img.pdfslide.net/doc/110x75/5fd5be972419e75f622d4651/uva-dare-digital-academic-repository-serrated-polyps-processed-on-12-12-2016.jpg)