Embed Size (px)
Citation preview

Research ArticlePractice Patterns and Barriers for Intravenous Thrombolysis:A Survey of Neurologists in Saudi Arabia
Mohammed H. Alanazy ,1 Rima B. Barakeh,1 Alanood Asiri,1 Maha F. Edrees,1
Ahmad R. Abuzinadah,2 Bandar N. Aljafen,1 and TaimMuayqil1
1Department of Internal Medicine, King Saud University Medical City and College of Medicine,King Saud University, Riyadh, Saudi Arabia2Department of Internal Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence should be addressed to Mohammed H. Alanazy; [email protected]
Received 8 November 2017; Revised 3 January 2018; Accepted 18 January 2018; Published 13 February 2018
Academic Editor: Jeff Bronstein
Copyright © 2018 MohammedH. Alanazy et al.This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Only a small fraction of patients with acute ischemic stroke receive intravenous thrombolysis (IVT). We sought to assess barriersand practice patterns in using IVT for acute ischemic stroke among neurologists in Saudi Arabia. An electronic survey was sentto all neurologists registered with the Saudi Commission for Health Specialties. A total of 148 (77.5%) neurologists responded.The most common reported barriers for IVT administration were delayed presentation to hospitals (82.4%) and unclear time ofsymptom onset (50.0%). Only 9.9% of neurologists reported strict adherence to the American Heart Association/American StrokeAssociation guidelines for IVT administration. The most frequently waived criteria were “minor stroke with National Institutes ofHealth Stroke Scale [NIHSS]< 5” (49.4%) and “seizure at onset” (45.7%). For the extended 3–4.5-hourwindow, 18.5%of neurologistsreported strict adherence to the four exclusion criteria. The most frequently waived criteria were “age older than 80 years” (53.1%)and “history of both diabetes and prior stroke” (42.0%). In conclusion,most neurologists do not adhere to the IVT exclusion criteria.However, little consensus exists regarding which criteria do not interfere with IVT administration. Barriers to IVT administrationwere identified and require immediate action by healthcare authorities in Saudi Arabia.
1. Introduction
Stroke is the second leading all-cause mortality and is a lead-ing cause of disability worldwide [1]. In 2010, the estimatednumber of patients that experienced their first stroke was16.9 million worldwide [2]. The estimated number of stroke-related deaths was 5.9 million, 71% of which occurred inlow- andmiddle-income countries, where effective treatmentmay not be affordable [2]. In Saudi Arabia (SA), there are nonationwide studies on stroke incidence and prevalence, andthe current literature is based on limited, older regional stud-ies. In 1998, Al-Rajeh et al. reported an incidence rate of 29.8per 100,000 per year for stroke in patients living in the easternregion of SA [3]. The prevalence of stroke was estimated tobe 186 per 100,000 [4]. Incidence and prevalence rates ofstroke in SA are relatively lower than those in western coun-tries, which can be attributed to the predominantly young
population in SA [5–7]. The American Heart Association/American Stroke Association (AHA/ASA) has developedinternationally accepted guidelines for the management ofacute stroke [8, 9]. However, barriers to implementation andcompliance with these recommendations in SA have notbeen thoroughly explored. Such information may help futureguideline developers to address potential regional specificlimitations and take into consideration the differences inpractice patterns, which may reflect cultural norms.
Intravenous thrombolysis (IVT) with recombinant tis-sue-type plasminogen activator (tPA) is considered the stan-dard of care therapy for eligible patients with acute ischemicstroke if administered within 4.5 hours from symptom onset[8, 10].When administered within this time window, IVT hasbeen proven to improve functional outcomes. Although theIVT administration rate has markedly increased, it remainswidely underused, as it is only administered to a small
HindawiNeurology Research InternationalVolume 2018, Article ID 1695014, 8 pageshttps://doi.org/10.1155/2018/1695014

2 Neurology Research International
proportion of stroke patients (3.4–5.2%) [11]. This underusewas attributed to several reasons, including late hospitalarrival, unknown time of symptom onset, and stringenteligibility criteria [12–14].The criteria for IVT administrationwere drawn from the pivotal study by the National Instituteof Neurological Disorders and Stroke (NINDS) that led toFDA approval for IVT within 3 hours from stroke onset [15].However, most of the exclusion criteria were not evidence-based andwere instead derived based on expert opinion at thetime of the original study. Subsequent nonrandomized stud-ies reported desirable outcomes in patients who received IVToutside of the established guidelines [16–19].This, along withincreasing experience with IVT administration and advancesin neuroimaging, led to the questioning of the necessity ofsome of these exclusion criteria [14, 20, 21]. Recently, thesecriteria were modified by the FDA and AHA/ASA to allowfor IVT treatment in patients that meet some of the exclusioncriteria [9, 22]. However, some neurologists prefer individ-ualized clinical judgment when evaluating patients with arelative contraindication, whereas others may strictly followthe guidelines and deny IVT.
This study sought to determine the extent to which actualpractice patterns for IVT follow AHA/ASA guidelines and toassess the barriers to the use of IVT for acute ischemic strokeamong neurologists in SA.
2. Methods
We evaluated a previously published survey (with permis-sion from the corresponding author) [23] and modified itto include the absolute and relative IVT contraindicationsaccording to theAHA/ASA 2015 scientific statement and 2015FDA package insert. For content validity and readability, weasked four general neurologists and one stroke neurologist toindependently review the provisional version of the survey,and their inputs were incorporated into the final version(Online SupplementaryMaterial (available here)).The surveywas designed (using https://surveymonkey.com) and dis-tributed via email and private massages during the monthsof June and July of 2017. We included all board-certifiedneurologists who are registered with the Saudi Commissionfor Health Specialties (SCHS), including attending neurol-ogists (consultants including stroke neurologists and non-stroke neurologists), stroke fellows, neurology registrars, andsenior registrars. Regulations for the classification of board-certified physicians are available at https://www.scfhs.org.sa.Neurology residents were excluded. To ensure maximumsurvey distribution, we asked a neurologist in each hospital toforward the electronic survey to other neurologists workingin the same hospital. Reminder surveys were sent to nonre-sponders at the end of June andmiddle of July 2017.This studywas approved by the institutional review board of King SaudUniversity.
3. Statistical Analysis
Data were analyzed using SPSS statistics software version 21.Categorical data are reported as numbers and percentages.To assess whether the use of IVT in postresidency practice
was dependent on IVT administration during residency, wedichotomized the responses of frequency of IVT administra-tion to “never prescribed IVT” and “prescribed IVT as a neu-rologist.” Chi-square test was employed to assess whether thefrequency of IVT administration as a neurologist was influ-enced by the experience of IVT administration during resi-dency. Two-tailed 𝑃 < 0.05 was considered significant.
4. Results
Of the 191 neurologists from 14 cities in the country, 148(77.5%) participated and 104 (70.2%) returned a completelyanswered survey. Neurologists practicing in 11 of the 14 citieshave administered IVT (Online Supplementary Table 1).Because of the incomplete surveys, response ratewas differentfor each item. The majority of respondents (𝑛 = 99/124,79.8%) were working in tertiary governmental hospitals,15/124 (12.1%) were working in secondary hospitals, and10/124 (8.1%) were working in private hospitals. Of the res-pondents, 86/126 (68.3%) were attending neurologists, 4/126(3.2%) were stroke fellows, 19/126 (15.1%) were senior regis-trars, and 17/126 (13.5%) were registrars. More than half ofthe respondents (𝑛 = 71/125, 56.8%) were from Riyadh, and24 (19.2%) were from Jeddah, the largest two cities in SA.Thedistribution of participating neurologists per city is shown inOnline Supplementary Table 1.
IVT was prescribed by a significantly larger number ofneurologists (𝑛 = 88/97, 90.7%) who had the experience ofadministering it during residency than by those who did nothave that experience (𝑛 = 19/39, 48.7%), 𝑃 < 0.001.
The frequency of IVT administration is shown in Table 1.Only 81 (60%) of neurologists prescribed IVT in the 12months preceding the survey, and those were included in theanalysis of “IVT practice patterns.” Sixty-seven of 81 (82.7%)surveys were completely answered. Criteria that would notprevent IVT administration by neurologists are shown inTable 2. Only 8/81 (9.9%) neurologists reported to adhere tothe guidelines. The most frequently waived exclusion criteriawere “minor stroke with National Institutes of Health StrokeScale (NIHSS) score < 5” (𝑛 = 40/81, 49.4%), “seizure atonset” (𝑛 = 37/81, 45.7%), “ischemic stroke within 3 months”(𝑛 = 25/81, 30.9%), “rapidly improving stroke symptoms”(𝑛 = 24/81, 29.6%), and “pregnancy” (𝑛 = 24/81, 29.6%). Allother criteria were waived by less than 25% of participatingneurologists.
Regarding the extended 3–4.5-hour IVT window, 15/81(18.5%) neurologists chose to adhere to all the four exclusioncriteria (age > 80 years, history of diabetes and prior stroke,warfarin use regardless of International Normalized Ratio[INR] value, or NIHSS > 25). Of participating neurologists,43/81 (53.1%) waived “age > 80 years,” 34/81 (42.0%) waived“history of diabetes and prior stroke,” 20/81 (24.7%) waived“NIHSS> 25,” and 17/81 (21.0%)waived “warfarin use regard-less of INR value.”
Only a small percent of neurologists waived the criterionof receiving a novel oral anticoagulant (NOAC) in the last48 hours (Table 2). The majority of neurologists (𝑛 = 54/81,66.7%) reported they would not administer IVT to a patienttaking dabigatran if the time of last dose was unknown,

Neurology Research International 3
Table 1: Frequency of intravenous tissue plasminogen activator (IV-tPA) administration.
Answers to the question “How many times have you prescribed/recommended IV-tPAfor patients with acute ischemic stroke (in your postresidency practice)?”
Number ofresponses (%),total𝑁 = 136
I have never prescribed IV-tPA 29 (21.3)I have prescribed IV-tPA in the past but it was more than 2 years ago 13 (9.6)I have prescribed IV-tPA once in the past two years 13 (9.6)I have prescribed IV-tPA 1–3 times in the past year 36 (26.5)I have prescribed IV-tPA 4–6 times in the past year 15 (11.0)I have prescribed IV-tPA 7–10 times in the past year 10 (7.4)I have prescribed IV-tPA >10 times in the past year 20 (14.7)
Table 2: Number and percentage of neurologists who would administer intravenous tissue plasminogen activator (IV-tPA) in the presenceof each exclusion criterion.
Criteria for the question “Which of the potential IV-tPA exclusion criteria (based on 2015 AHA/ASAscientific statement or tPA package insert) WOULD NOT necessarily prevent you from administeringIV-tPA to a patient with a perceived disabling stroke (provided other inclusion/exclusion criteria are met)?”∗Multiple answers allowed
Number ofresponses (%),total𝑁 = 81
None. I do not “bend” any of the guideline exclusion criteria 8 (9.9)Minor stroke (NIHSS < 5) 40 (49.4)Rapidly improving stroke symptoms 24 (29.6)Ischemic stroke within 3 months 25 (30.9)Significant head trauma within 3 months 9 (11.1)Seizure at onset 37 (45.7)Intracranial or intraspinal surgery in the prior 3 months 11 (13.6)Blood pressure > 185/110mmHg despite appropriate treatment efforts to control it 11 (13.6)Current use of anticoagulant with INR > 1.7 or PT > 15 10 (12.4)Receiving heparin within 48 hours with aPTT value > 40 (abnormal) 6 (7.4)Receiving direct thrombin inhibitor or factor Xa inhibitor within 48 hours with normal coagulation profile(PT, PTT, INR, platelet count, clotting time, thrombin time, factor Xa activity assays) 12 (14.8)
Receiving direct thrombin inhibitor or factor Xa inhibitor within 48 hours with unknown coagulation profile(PT, PTT, INR, platelet count, clotting time, thrombin time, factor Xa activity assays) 6 (7.4)
Receiving direct thrombin inhibitor or factor Xa inhibitor within 48 hours with abnormal coagulation profile(PT, PTT, INR, platelet count, clotting time, thrombin time, factor Xa activity assays) 6 (7.4)
Received therapeutic LMWH within 24 hours 4 (4.9)Major surgery within 14 days 15 (18.5)Major extracranial trauma within 14 days 12 (14.8)Active internal bleeding 9 (11.1)Previous ICH 15 (18.5)Symptoms suggestive of subarachnoid hemorrhage (SAH) 6 (7.4)Intracranial unruptured unsecured aneurysm 11 (13.6)Intracranial remotely ruptured, secured aneurysm 13 (16.1)Platelet count < 100,000 10 (12.4)CT showing hypodensity > 1/3 of the cerebral hemisphere 12 (14.8)ST elevated MI in previous 3 months 11 (13.6)NSTEMI in previous 3 months 17 (21.0)Gastrointestinal hemorrhage in previous 21 days 13 (16.1)Genitourinary hemorrhage in previous 21 days 11 (13.6)Glucose < 50mg/dl (deficits persist after glucose correction) 12 (14.8)Known brain tumor 6 (7.4)Intracranial AVM (arteriovenous malformation) 9 (11.1)Arterial puncture at a noncompressible site within 7 days 11 (13.6)Pregnancy 24 (29.6)

4 Neurology Research International
Table 3: Number and percentage of neurologists who would administer IVT based on an INR value or NIHSS score.
Answers to the questions “In patients receiving warfarin, up to whatINR do you feel comfortable administering IV-tPA?”
Number of responses(%)
≤1.4 15 (22.4)≤1.5 11 (16.4)≤1.6 10 (14.9)≤1.7 29 (43.3)≤1.8 1 (1.5)≤1.9 1 (1.5)≥2.0 0Total number 67Answers to the question “Is there an NIHSS below which you usuallydo not offer IV-tPA?”
Number of responses(%)
1 3 (3.7)2 2 (2.5)3 8 (9.9)4 14 (17.3)5 5 (6.2)6 1 (1.2)Perceived disability of the deficit 35 (43.2)Other (please specify) 1 (1.2)Total number 81Answers to the question “Is there an NIHSS above which you do notoffer IV-tPA?”
Number of responses(%)
>25 26 (37.7)>30 9 (13.0)>35 1 (1.5)>40 1 (1.5)I do not restrict fibrinolysis based on an upper NIHSS score. 32 (46.4)Total number 69
regardless of normal coagulation; 9/81 (11.1%) reported theywould administer IVT if renal function is normal, and 6/81(7.4%) reported they would administer IVT even in thesetting ofmild renal impairment. In patientswith acute strokewhile taking warfarin, 29/67 (43.3%) of neurologists reportedthey would use IVT with an INR of ≤1.7, and the remainderchose different INR values as shown in Table 3.
The majority of neurologists (𝑛 = 53/69, 76.8%) reportedthey would not wait for a pregnancy test result beforeadministering IVT to awomanof childbearing age presentingwith acute ischemic stroke; the remainder (𝑛 = 16/69, 23.2%)reported they would wait for pregnancy test results.
Less than half of the neurologists (𝑛 = 35/81, 43.2%) donot deny IVT based on a lower NIHSS score, but rather theirdecision making is based on the perceived disability of thedeficit. Approximately half of the neurologists (𝑛 = 32/69,46.4%) do not restrict IVT based on an upper NIHSS score,Table 3.
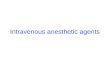
When analyzing neurologists’ responses to barriers ofIVT administration, we included responses from all neurol-ogists whether or not they prescribed IVT in the past 12months. The majority (𝑛 = 89/108, 82.4%) of neurologists
chose “late presentation to emergency room (ER),” 54/108(50.0%) chose “unclear time of onset,” and 36/108 (33.3%)chose “delayed referral from ER to neurologist,” Figure 1.Eleven neurologists marked “other” and provided descriptivebarriers, which we classified under the following themes: (1)lack of resources including tPA, intensive care unit (ICU) bed,stroke team, trained nurses, imaging, and neuroradiologists;(2) problems with logistics including delay in triage, lack ofstroke code and treatment protocol, lack of centralized strokecare, and delay in insurance approval for private hospitals;and (3) problems with consent including lack of an IVTconsent and a decline or delay in signing consent by patientsor their family members.
5. Discussion
Our study showed that there is, in general, underuse of IVT inSaudi Arabia. Similar to previous reports [12, 13], themajorityof neurologists we surveyed agreed that the most commonbarriers interfering with IVT are late presentation to ER andunclear time of onset (82.4% and 50.0%, respectively). Theseresults indicate lack of public awareness and are consistent

Neurology Research International 5
Late
pre
sent
atio
n to
ER
Unc
lear
tim
e of o
nset
Dela
yed
refe
rral
from
ER
to n
euro
logi
st
Patie
nt o
r fam
ily d
eclin
ing
IV-tP
A
Abse
nce o
f IV-
tPA
or d
elay
in IV
-tPA
prep
arat
ion
Dela
y in
obt
aini
ng b
rain
CT
Impa
ired
coag
ulat
ion,
due
to d
iseas
e,dr
ugs,
etc.
Failu
re to
cont
rol h
igh
bloo
d pr
essu
re
Oth
er
0
10
20
30
40
50
60
70
80
90
Perc
enta
ge o
f res
pons
es (%
)
Figure 1: Barriers that interfere with IVT administration to patientswith acute stroke as selected by neurologists (𝑛 = 108).
with previous studies [24, 25]; thus, an initiative by thenational health authorities in SA to raise public awarenessof acute stroke symptoms and the time-dependent nature oftreatment is warranted. Approximately one-third of neurol-ogists we surveyed reported that in-hospital delays resultedin long door-to-needle time, emphasizing an urgent need toinitiate stroke codes within emergency treatment facilitiesand to ensure that emergency physicians and triage nurses aretrained to promptly recognize and manage potential strokepatients.
One barrier that may influence the rate of IVT use is thelack of residency training in acute stroke management. Ourstudy showed that a higher percentage of neurologists withthe experience of administering IVT during their residencysubsequently prescribed IVT in their postresidency practice,as compared to those who did not have IVT experienceduring their residency (90.7% versus 48.7%). Although thisdifference in IVT use can be attributed to several factors suchas infrastructural resources and logistics, our results suggestthat the impact of residency training in acute stroke manage-ment plays a major role. It is not surprising that 39 (28.7%)neurologists in our cohort did not prescribe IVT during theirresidency since it is likely that several of them completed resi-dency training prior to the availability of IVT for acute stroke[24]. The SCHS has taken several steps to improve neurologyresidency training over the past few years. Nonetheless, it isimperative to ensure that all neurology-board trainees receivesufficient training within a stroke unit to improve theirdecision-making skills and increase confidencewhen treatingpatients with acute stroke. There is a large unmet need ofstroke care in SA. Although IVT was administered by the
participating neurologists in 11 of the 14 cities, only 3 hospitalsin the country, all located in Riyadh, have a dedicated stroketeam and stroke unit, and few hospitals in Riyadh andJeddah have a stroke code mostly carried out by nonstrokeneurologists (personal communication, Dr. F. Al-Senani,Saudi Stroke Association). Only two centers in the countryhave a stroke fellowship registered with the SCHS with a totalof 4 fellows. In addition, there are limited stroke neurologistsin the country and, therefore, in most tertiary hospitals,IVT is administered by nonstroke neurologists. With recentadvances in endovascular therapy [26, 27], it is essential toestablish, in every province, comprehensive stroke centerscapable of providing stroke care to patients transferredfrom other hospitals. Considering the limited number ofneurologists and more specifically stroke neurologists inSA, the use of telestroke networks will facilitate timelyIVT administration, especially in rural areas with limitedresources, in which the IVT bolus dose is given in the ER,and the remaining dose infused while the patient is beingtransferred to a tertiary hospital (drip-and-ship) [28].
Another barrier for the underuse of IVT is the presenceof one or more exclusion criteria. This study revealed thatonly a small percentage of neurologists (9.9%) strictly adhereto the IVT exclusion criteria (based on AHA/ASA guide-lines or tPA package insert). The most commonly waivedexclusion criterion was minor stroke (NIHSS < 5) (49.4%). Inaddition, 43.2% of neurologists reported they would not usea lower NIHSS score to withhold IVT, rather they base theirdecision on the perceived severity of the deficit. Conceivably,withholding IVT in patients with minor stroke (based onNIHSS) may lead to missed opportunity to treat the poten-tially disabling stroke symptoms with a low NIHSS (isolatedaphasia, neglect, hemianopia, and gait disturbance), andsymptoms not fully captured by the NIHSS, such as symp-toms of posterior circulation and the right hemisphere. Previ-ous studies report that one-third of patients denied IVT dueto minor stroke or rapidly improving stroke symptoms hadpoor outcomes [29, 30]. The AHA/ASA guidelines recom-mend that patients with mild but disabling stroke within 3hours from onset should receive IVT, as the clinical benefithas been proven [9]. Likewise, IVT should not be delayedin patients with moderate to severe stroke who demonstrateearly incomplete clinical improvement to monitor further improvement. Such a delay leads to exceeding the 3-hour treat-ment window, especially since initial spontaneous improve-ment can be followed by worsening [29–31]. Approximately,one-half of neurologists in our study report they would notrestrict IVT based on a higher NIHSS score. Although strokeseverity is a predictor of high hemorrhage risk [32, 33],the benefit of IVT in improving functional outcomes, inotherwise eligible patients, has been proven [9]. Therefore,IVT is recommended for patients with severe acute strokesymptoms who present within 3 hours from symptom onset[9].
Seizure at stroke onset was waived by 45.7% of the neu-rologists we surveyed. Seizure at stroke onset was considereda relative contraindication in the AHA/ASA 2013 guide-lines [8]. Additionally, according to their recent scientificstatement, IVT was considered a reasonable treatment for

6 Neurology Research International
acute stroke patients with seizure at onset, if the deficit wasattributed to stroke [9]. However, seizure at stroke onset wasremoved from updated FDA guidelines [22].
Pregnancy is associated with an increased risk of devel-oping acute ischemic stroke [34]. In our study, 29.6% of neu-rologists waived pregnancy from the exclusion criteria, and76.8% report they would administer IVT to women of child-bearing age presenting with acute stroke without waitingfor a pregnancy test result. The FDA labeled tPA as a pre-gnancy category C [22], and pregnancy is listed as a relativecontraindication in the AHA/ASA guidelines [9]. The largemolecular size of tPA (7200 kDa) prevents it fromcrossing theplacenta [35], and it is likely not teratogenic in doses used foracute stroke [9]. Since the risk of intrauterine and systemicbleeding remains a concern due to the lack of controlledstudies, IVT can be used in pregnancy if the anticipatedbenefit of treating a moderate to severe stroke outweighs therisk of uterine bleeding [9].
Eleven (13.6%) neurologists in our cohort report theywould administer IVT even if blood pressure (BP) is>185/110mmHg. Elevated BP is associatedwith increased riskof symptomatic intracranial hemorrhage (sICH) [36]. TheAHA/ASA statement requires that BP is lowered and stabi-lized below 185/110mmHg before administering IVT, and BPmust be maintained <180/105mmHg for at least 24 hoursfollowing tPA infusion [9]. Both hyper- and hypoglycemiararely present with a focal neurological deficit mimickingacute stroke. In our cohort, 14.8% of neurologists reportthey would administer IVT even with a glucose level of<50mg/dl. It is recommended to treat high (>400mg/dL)and low (<50mg/dL) glucose levels first, and to administerIVT to otherwise eligible patients if the deficit persists despiteoptimizing glucose level [9].
In our study, a small percentage of neurologists reportthey would administer IVT to patients with acute stroke andan abnormal coagulation profile, or if they had received ananticoagulant within 48 hours.The thresholds of coagulationvalues at which the risk of bleeding outweighs the benefitof IVT have not been precisely determined. Considering thelack of robust data supporting the safety and efficacy of IVTin the presence of abnormal coagulation values (platelets <100000/mm3, INR > 1.7, aPTT > 40 seconds, or PT > 15 sec-onds), administration of IVT is not recommended [9]. How-ever, it is rare to have such abnormal coagulation valuesin stroke patients that are not previously suspected. There-fore, these laboratory results are not necessary before IVTadministration, unless bleeding abnormalities, such as theconcurrent use of oral anticoagulants, are suspected [9].In our sample, only 2 neurologists (3%) report they arewilling to use IVT even with an INR > 1.7 (1.8 and 1.9).Data from stroke registries suggest that IVT administrationin patients on warfarin with an INR ≤ 1.7 is safe [37–39].Oral anticoagulants are listed on the FDA warning labelwithout a specific INR value indicated [22]. The AHA/ASAguidelines do not recommend IVT for patients on warfarinwith an INR > 1.7 and/or a PT > 15 seconds, patients whoreceived a therapeutic dose of LMWH in the last 24 hours,or patients taking a direct thrombin inhibitor or a factor Xainhibitor, unless coagulation tests (e.g., aPTT, INR, platelet
count, ecarin clotting time, thrombin time, or appropriatedirect factor Xa activity assays) are normal, or more than 48hours have passed since the last dose (assuming normal renalfunction) [9].
Data from the Get With The Guidelines-Stroke registryindicate that none of the European Cooperative Acute StrokeStudy (ECASS) III exclusion criteria is associated with worseoutcome or higher risk of sICH in the 3–4.5-hour windowcompared with the 0–3-hour window [40]. In our study,18.5% of neurologists strictly adhered to the ECASS IIIexclusion criteria, whereas approximately 53% waived theage criteria, and 42% waived history of previous stroke anddiabetes. It has previously been argued that age alone shouldnot be a criterion to exclude elderly patients from IVT therapy[16, 40–43]. Although there was no difference in the rate ofsICH between younger and older age groups (≤80 and >80years of age), mortality rates were higher in the older agegroup [16, 40–43]. However, the mortality in patients >80years was highwhether or not tPAwas administered [43], andthis can likely be attributed to the natural history of strokeoutcome in this age group [42–44].Therefore, the AHA/ASArecommends IVT for stroke patients > 80 years of age andpresenting within the 3–4.5-hour treatment window [9]. Inaddition, IVT is recommended for patients with prior strokeand diabetes and for patients on warfarin with an INR < 1.7,whereas the benefit of IVT for patients with NIHSS > 25remains uncertain [9].
Our study has several limitations. We did not design oursurvey to assess endovascular therapy practice patterns or theuse of perfusion imaging to aid in ischemic penumbra assess-ment. Although we had a high response rate, data were miss-ing from 17.3% of the surveys analyzed for “IVT practice pat-tern,” therefore hindering the generalizability of our results.The use of a web-based survey may have introduced biaseswith more responses from participants having familiaritywith such surveys. Considering that tPA exclusion criteriahave various levels of recommendations, potential biases mayhave been introduced by using the phrase “bending the guide-line exclusion criteria.” However, we would expect, in thatcase, that the majority of participants would strictly adhereto the guidelines, while in fact only a small percentage choseto adhere to the exclusion criteria listed, reflecting theirknowledge of the various levels of recommendations. This issimilar to a previous study in which adherence to the guide-lines was reported by 18% of participants [23]. Additionally,we did not collect the neurological subspecialties of our par-ticipants, and thuswewere unable to compare responses fromstroke neurologists to responses fromnonstroke neurologists.However, we donot think thiswould have changed our resultsas stroke care is largely provided by nonstroke neurologists inSA. The majority of our participants were from Riyadhand Jeddah, which is likely a reflection of the number ofneurologists practicing in these two most populated cities ofSA [45].
In conclusion, only a small percentage of neurologistsreport that they strictly adhere to the IVT guidelines, whilethe majority waived one or more exclusion criteria. Therewas little consensus among neurologists regarding whichcriteria to adhere to. Our study suggests that the AHA/ASA

Neurology Research International 7
statement, which leaves room for clinical judgment in thepresence of some relative contraindications, is more practicaland well-perceived by practicing neurologists. The majorbarriers reported for IVT underuse in SA were delay inpresentation tomedical attention, unknown time of symptomonset, and in-hospital delay. These findings impose a largedemand on healthcare authorities to implement measures toraise public awareness of acute stroke symptoms and signs,improve patient accessibility, transfer to stroke centers, andimprove IVT administration rates for eligible stroke patients.
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this paper.
Supplementary Materials
Survey: the electronic survey distributed on neurologists.Supplementary Table 1: city-wise distribution of neurolo-gists who participated showing tPA administration per city.(Supplementary Materials)
References
[1] E. J. Benjamin,M. J. Blaha, S. E. Chiuve et al., “HeartDisease andStroke Statistics—2017 Update,” Circulation, vol. 135, pp. e146–e603, 2017.
[2] VL. Feigin, MH. Forouzanfar, R. Krishnamurthi et al., “Globaland regional burden of stroke during 1990-2010: findings fromthe Global Burden of Disease Study 2010,”The Lancet, vol. 383,pp. 245–254, 2014.
[3] S. Al-Rajeh, E. B. Larbi, and O. Bademosi, “Stroke register:experience from the eastern province of Saudi Arabia,” Cere-brovascular Disease, vol. 8, no. 2, pp. 86–89, 1998.
[4] S. Al Rajeh, O. Bademosi, H. Ismail et al., “A community surveyof neurological disorders in Saudi Arabia: the Thugbah study,”Neuroepidemiology, vol. 12, no. 3, pp. 164–178, 1993.
[5] S. Al Rajeh and A. Awada, “Stroke in Saudi Arabia,” Cerebrovas-cular Disease, vol. 13, no. 1, pp. 3–8, 2002.
[6] S. Al Rajeh, A. Awada, G. Niazi, and E. Larbi, “Stroke in aSaudi Arabian National Guard community: analysis of 500consecutive cases froma population-based hospital,” Stroke, vol.24, no. 11, pp. 1635–1639, 1993.
[7] N. Poungvarin, “Stroke in the developing world,” The Lancet,vol. 352, pp. S19–S22, 1998.
[8] E. C. Jauch, J. L. Saver, H. P. Adams et al., “Guidelines for theearly management of patients with acute ischemic stroke: aguideline for healthcare professionals from the American HeartAssociation/American Stroke Association,” Stroke, vol. 44, no.3, pp. 870–947, 2013.
[9] B. M. Demaerschalk, D. O. Kleindorfer, O. M. Adeoye et al.,“Scientific Rationale for the Inclusion and Exclusion Criteriafor Intravenous Alteplase in Acute Ischemic Stroke A Statementfor Healthcare Professionals from the American Heart Associ-ation/American Stroke Association,” Stroke, vol. 47, no. 2, pp.581–641, 2016.
[10] W. Hacke, M. Kaste, E. Bluhmki et al., “Thrombolysis with alte-plase 3 to 4.5 hours after acute ischemic stroke,” The NewEngland Journal ofMedicine, vol. 359, no. 13, pp. 1317–1329, 2008.
[11] O. Adeoye, R. Hornung, P. Khatri, and D. Kleindorfer, “Recom-binant tissue-type plasminogen activator use for ischemicstroke in the united states: A doubling of treatment rates overthe course of 5 years,” Stroke, vol. 42, no. 7, pp. 1952–1955, 2011.
[12] P. A. Barber, J. Zhang, A. M. Demchuk, M. D. Hill, and A. M.Buchan, “Why are stroke patients excluded from TPA therapy?An analysis of patient eligibility,” Neurology, vol. 56, no. 8, pp.1015–1020, 2001.
[13] Y. Z. Deng, M. J. Reeves, B. S. Jacobs et al., “IV tissue plasmino-gen activator use in acute stroke: Experience from a statewideregistry,” Neurology, vol. 66, no. 3, pp. 306–312, 2006.
[14] D. Tong, “Are all IV thrombolysis exclusion criteria necessary?:Being SMART about evidence-based medicine,”Neurology, vol.76, no. 21, pp. 1780-1781, 2011.
[15] National Institute of Neurological Disorders and Stroke rt-PAStroke Study Group, “Tissue plasminogen activator for acuteischemic stroke,”TheNew England Journal of Medicine, vol. 333,pp. 1581–1587, 1995.
[16] C. A. Cronin, N. Shah, T. Morovati, L. D. Hermann, and K. N.Sheth, “No increased risk of symptomatic intracerebral hemor-rhage after thrombolysis in patients with European CooperativeAcute Stroke Study (ECASS) exclusion criteria,” Stroke, vol. 43,no. 6, pp. 1684–1686, 2012.
[17] M. Rubiera, M. Ribo, E. Santamarina et al., “Is it time to reassessthe SITS-MOST criteria for thrombolysis?: A comparison of pa-tients with and without SITS-MOST exclusion criteria,” Stroke,vol. 40, no. 7, pp. 2568–2571, 2009.
[18] M. Guillan, A. Alonso-Canovas, J. Garcia-Caldentey et al., “Off-label intravenous thrombolysis in acute stroke,” European Jour-nal of Neurology, vol. 19, no. 3, pp. 390–394, 2012.
[19] A.Meretoja, J. Putaala, T. Tatlisumak et al., “Off-label thrombol-ysis is not associatedwith poor outcome in patients with stroke,”Stroke, vol. 41, no. 7, pp. 1450–1458, 2010.
[20] A. Aleu, P. Mellado, C. Lichy, M. Kohrmann, and P. D. Sche-llinger, “Hemorrhagic complications after off-label thromboly-sis for ischemic stroke,” Stroke, vol. 38, no. 2, pp. 417–422, 2007.
[21] J. De Keyser, Z. Gdovinova, M. Uyttenboogaart, P. C. Vroomen,and G. J. Luijckx, “Intravenous alteplase for stroke: Beyond theguidelines and in particular clinical situations,” Stroke, vol. 38,no. 9, pp. 2612–2618, 2007.
[22] “Activase (alteplase). Prescribing information,” 2017,https://www.gene.com/download/pdf/activase prescribing.pdf.
[23] F. De Los Rios, D. O. Kleindorfer, A. Guzik et al., “Intravenousfibrinolysis eligibility: A survey of stroke clinicians’ practicepatterns and review of the literature,” Journal of Stroke andCerebrovascular Diseases, vol. 23, no. 8, pp. 2130–2138, 2014.
[24] A. M. Al Khathaami, H. Algahtani, A. Alwabel, N. Alosherey, S.Kojan, and M. Aljumah, “The status of acute stroke care inSaudi Arabia: An urgent call for action!,” International Journalof Stroke, vol. 6, no. 1, pp. 75-76, 2011.
[25] A. Alaqeel, A. Alammari, N. Alsyefi, F. Al-Hussain, and Y.Mohammad, “Stroke awareness in the Saudi community livingin Riyadh: Prompt public health measures must be imple-mented,” Journal of Stroke and Cerebrovascular Diseases, vol. 23,no. 3, pp. 500–504, 2014.
[26] W. J. Powers, C. P. Derdeyn, J. Biller et al., “2015 AmericanHeart Association/American stroke association focused updateof the 2013 guidelines for the early management of patientswith acute ischemic stroke regarding endovascular treatment: aguideline for healthcare professionals from the American HeartAssociation/American stroke association,” Stroke, vol. 46, no.10, pp. 3020–3035, 2015.

8 Neurology Research International
[27] M. Goyal, B. K. Menon, W. H. van Zwam et al., “Endovascularthrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials,”The Lancet (London, England), vol. 387, no. 10029, pp. 1723–1731,2016.
[28] L. H. Schwamm, N. Chumbler, E. Brown et al., “Recommen-dations for the Implementation of Telehealth in Cardiovascularand Stroke Care: A Policy Statement from the American HeartAssociation,” Circulation, vol. 135, no. 7, pp. e24–e44, 2017.
[29] E. E. Smith, A. R. Abdullah, I. Petkovska, E. Rosenthal, W. J.Koroshetz, and L. H. Schwamm, “Poor outcomes in patientswho do not receive intravenous tissue plasminogen activatorbecause of mild or improving ischemic stroke,” Stroke, vol. 36,no. 11, pp. 2497–2499, 2005.
[30] E. E. Smith, G. C. Fonarow, M. J. Reeves et al., “Outcomes inmild or rapidly improving stroke not treated with intravenousrecombinant tissue-type plasminogen activator: Findings fromget with the guidelines-stroke,” Stroke, vol. 42, no. 11, pp. 3110–3115, 2011.
[31] K. Nedeltchev, B. Schwegler, T.Haefeli et al., “Outcome of strokewith mild or rapidly improving symptoms,” Stroke, vol. 38, no.9, pp. 2531–2535, 2007.
[32] M. D’Amelio, V. Terruso, G. Famoso et al., “Early and late mor-tality of spontaneous hemorrhagic transformation of ischemicstroke,” Journal of Stroke and Cerebrovascular Diseases, vol. 23,no. 4, pp. 649–654, 2014.
[33] The NINDS t-PA Stroke Study Group, “Intracerebral hem-orrhage after intravenous t-PA therapy for ischemic stroke,”Stroke, vol. 28, no. 11, pp. 2109–2118, 1997.
[34] R. H. Swartz, M. L. Cayley, N. Foley et al., “The incidence ofpregnancy-related stroke: A systematic review and meta-analysis,” International Journal of Stroke, vol. 12, no. 7, pp. 687–697, 2017.
[35] A. Steinberg and T. P. Moreira, “Neuroendocrinal, neurode-velopmental, and embryotoxic effects of recombinant tissueplasminogen activator treatment for pregnant women withacute ischemic stroke,” Frontiers in Neuroscience, vol. 10, articleno. 51, 2016.
[36] B. K. Menon, J. L. Saver, S. Prabhakaran et al., “Risk score forintracranial hemorrhage in patients with acute ischemic stroketreated with intravenous tissue-type plasminogen activator,”Stroke, vol. 43, no. 9, pp. 2293–2299, 2012.
[37] Y. Xian, L. Liang, E. E. Smith et al., “Risks of intracranial hem-orrhage among patients with acute ischemic stroke receivingwarfarin and treated with intravenous tissue plasminogenactivator,” Journal of the American Medical Association, vol. 307,no. 24, pp. 2600–2608, 2012.
[38] M. D. I. Vergouwen, L. K. Casaubon, R. H. Swartz et al., “Sub-therapeutic warfarin is not associated with increased hemor-rhage rates in ischemic strokes treated with tissue plasminogenactivator,” Stroke, vol. 42, no. 4, pp. 1041–1045, 2011.
[39] M. V. Mazya, K. R. Lees, R. Markus et al., “Safety of intravenousthrombolysis for ischemic stroke in patients treated with war-farin,” Annals of Neurology, vol. 74, no. 2, pp. 266–274, 2013.
[40] C. A. Cronin, K. N. Sheth, X. Zhao et al., “Adherence to ThirdEuropean Cooperative Acute Stroke Study 3- to 4.5-hourexclusions and association with outcome: data from Get withthe Guidelines-Stroke,” Stroke, vol. 45, no. 9, pp. 2745–2749,2014.
[41] G. Boulouis, F. Dumont, C. Cordonnier, M. Bodenant, D. Leys,and H. Henon, “Intravenous thrombolysis for acute cerebral
ischaemia in old stroke patients ≥80 years of age,” Journal ofNeurology, vol. 259, no. 7, pp. 1461–1467, 2012.
[42] J. Garcıa-Caldentey, M. Alonso De Lecinana, P. Simal et al.,“Intravenous thrombolytic treatment in the oldest old,” StrokeResearch and Treatment, vol. 2012, Article ID 923676, 7 pages,2012.
[43] B. D. Bray, J. Campbell, A. Hoffman, P. J. Tyrrell, C. D. A.Wolfe, and A. G. Rudd, “Stroke thrombolysis in england: Anage stratified analysis of practice and outcome,” Age and Ageing,vol. 42, no. 2, pp. 240–245, 2013.
[44] G. A. Ford, N. Ahmed, E. Azevedo et al., “Intravenous alteplasefor stroke in those older than 80 years old,” Stroke, vol. 41, no.11, pp. 2568–2574, 2010.
[45] General Authority for Statistics, “Demography survey,” 2017,https://www.stats.gov.sa/sites/default/files/en-demographic-re-search-2016 4.pdf.

Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Disease Markers
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwww.hindawi.com Volume 2013
Hindawiwww.hindawi.com Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwww.hindawi.com Volume 2018
PPAR Research
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwww.hindawi.com Volume 2018
Journal of
ObesityJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwww.hindawi.com Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwww.hindawi.com Volume 2018
Diabetes ResearchJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Research and TreatmentAIDS
Hindawiwww.hindawi.com Volume 2018
Gastroenterology Research and Practice
Hindawiwww.hindawi.com Volume 2018
Parkinson’s Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwww.hindawi.com
Submit your manuscripts atwww.hindawi.com