Embed Size (px)
Citation preview

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
1 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Pre-Implantation trial of Histopathology In renal Allografts
Does the introduction of a national pre-implantation
biopsy histopathology service increase numbers, and improve outcomes, of kidney transplants performed in the UK: an open, stepped-wedge cluster, randomised
trial.
Version: 2.0
Date: 16/09/2019
CTU Ref: [16/88] ISRCTN: [11708741] REC: [17/EE/0481]

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
2 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Protocol Development Group:
Name Affiliation Authors’ Contributions
Gavin Pettigrew Cambridge University Hospitals NHS Foundation Trust
GP and DS conceived of the study. GP, DN, DS, and RC initiated the study design and CW, AD, AM and EL helped with implementation. GP is the primary grant holder. KH provided statistical expertise in clinical trial design and LP is conducting the primary statistical analysis. SR has key ongoing input into operational aspects (training, biopsy collection and transport, incident reporting). All authors contributed to refinement of the study protocol and approved the final version.
Claire Williment NHS Blood and Transplant
Alison Deary NHS Blood and Transplant
Ana Mora NHS Blood and Transplant
Emma Laing NHS Blood and Transplant
Karla Hemming University of Birmingham
Desley Neil University Hospitals Birmingham NHS Foundation trust
Dominic Summers
NHS Blood and Transplant
Roberto Cacciola Barts Health NHS Trust
Laura Pankhurst NHS Blood and Transplant
John Ayorinde Cambridge University Hospitals NHS Foundation Trust
Sandrine Rendel University of Oxford, Medical Sciences Division
e-Approved by:
Name Role Confirmed Date
Gavin Pettigrew Chief Investigator
General Information
This document was constructed using the National Health Service Blood and Transplant Clinical Trials Unit (NHSBT CTU) Protocol Template FRM4468 Version 1.0, which is based on the MRC CTU Protocol template Version 4.0 and the SPIRIT guidelines 2013. It describes the PITHIA trial, co-ordinated by the NHSBT CTU and provides information about procedures for entering participants into it. The protocol should not be used as an aide-memoire or guide for the treatment of other patients. Every care has been taken in drafting this protocol, but corrections or amendments may be necessary. These will be circulated to the registered investigators in the trial, but sites entering participants for the first time are advised to contact the Trial Manager to confirm they have the most up to date version.
Compliance
The trial will be conducted in compliance with the approved protocol, the Declaration of Helsinki [2013] the Principles of Good Clinical Practice (GCP), the UK Data Protection Act, the National Health Service Research Governance Framework for Health and Social Care (RGF) and any other applicable national regulations.
Sponsor
Cambridge University Hospitals NHS Foundation Trust and the University of Cambridge are the primary trial sponsors and have delegated responsibility for the overall management of the PITHIA trial to the NHSBT CTU. Queries relating to the sponsorship of

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
3 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
the trial should be addressed to the Research and Development Manager, c/o R&D Office Block S Level 4, Addenbrooke’s Hospital, Hills Road, Cambridge CB2 0QQ.
Funding
The trial will receive financial and non-financial support as follows: 1. National Institute for Health Research: Research for Patient Benefit (RfPB) Programme (PB-PG-1215-20033). NIHR will provide financial support for staff salaries, direct/indirect research costs as well as dissemination costs. In addition NIHR will provide access to their established research networks, research design services as well as other partners. 2. This trial has been funded primarily by award of the RfPB, but this does not cover excess treatment costs, most notably the cost of histopathology at the six national centres (Cambridge, Royal Free, Newcastle, Leeds, Birmingham and Edinburgh). Six digital pathology scanners are to be supplied for the duration of the trial, one for each designated centre. These scanners will be provided by Sysmex UK Ltd (Milton Keynes), with the cost to be met by Addenbrooke’s Charitable Trust and will include a service contract which will cover the duration of the trial.
Trial Registration
This trial is registered with the ISRCTN (study ID: ISRCTN11708741).
Trial Administration
Please direct all enquiries to the Trial Manager in the first instance. Clinical queries will be passed to the Chief Investigator via the Trial Manager.
CTU Details
NHSBT CTU Administration Office: 01223 588088
NHS Blood and Transplant Fax: 01223 5848136
Long Road Email: [email protected]
Cambridge
CB2 0PT
CTU Staff Details
Trial Manager Emma Laing Tel: 01223 588091
Email: [email protected]
Data Manager Renate Hodge Tel: 01223 588064
Email: [email protected]
Statistician Laura Pankhurst Tel: 0117 9757431
Email: [email protected]
Head of Operations Alison Deary Tel: 01223 588004
Email: [email protected]

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
4 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Chief Investigator
Mr Gavin Pettigrew Tel: 07841 004696
Dept of Level 9, Surgery Email: [email protected]
Hospital Addenbrooke’s
Address Line 1 Hills Rd, CB2 0QQ
Address Line 2
City Cambridge
County, Post Code CB2 0QQ
Country United Kingdom
Collaborators
Professor Karla Hemming Senior Lecturer at the Institute of Applied Health Research, University of Birmingham
Dr Desley Neil Consultant Histopathologist, University Hospital Birmingham
Dr Edward Wilson Senior Lecturer in Health Economics, Health Economics Group, University of East Anglia
Mrs Helen Thomas Head of Clinical Trial Statistics, NHSBT
Mr Dominic Summers NIHR Academic Clinical Fellow in Transplant Surgery
Mr Chris Callaghan Consultant Transplant Surgeon, and National Clinical Lead for Organ Utilisation
Professor John Forsythe Associate Medical Director, NHSBT
Mr Roberto Cacciola Consultant Transplant Surgeon
Professor Rutger Ploeg Consultant Transplant Surgeon, National Clinical Lead for Organ Retrieval,
Coordinating Principal Investigator of QUOD
(For full details of Trial Committees, please refer to Section 16)

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
5 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Study Synopsis
Scientific title of clinical study
Does the introduction of a national pre-implantation biopsy histopathology service increase numbers, and improve outcomes, of kidney transplants performed in the UK: a stepped-wedge cluster randomised trial
Public title of clinical study Does a 24 hour national digital histopathology service increase the number of kidney transplants in the UK?
Protocol Short Title/Acronym
Pre-implantation Trial of Histopathology in renal Allografts (PITHIA)
Protocol Version and Date
v2.0 16/09/2019
Primary Sponsor
Cambridge University Hospitals NHS Foundation Trust and the University of Cambridge
Funder
National Institute of Health Research – Research for Patient Benefit
Primary Clinical Trials Registry number
ISRCTN11708741
Date Study Registered 30/01/2018
Study design
Type of study ○ Interventional Study design ○ Randomised ○ Multi-centre stepped-wedge cluster ○ Unblinded Purpose: ○ Evaluation of a new service
Health Condition(s) or Problem(s) Studied
End stage renal disease Renal transplantation
Inclusion and exclusion criteria (kidneys for the histopathology service)
Inclusion Kidneys offered for transplantation from deceased donors
(DCD* and DBD**) aged ≥60 years Exclusion Kidneys offered as a component of a multi-organ
transplant *DCD: donation after circulatory death **DBD: donation after brain death
Setting
22 UK adult kidney transplant centres
Interventions to be compared
Active comparator: Full, free, 24/7 access to the National Histopathology service Comparator: Standard care
Study hypothesis
Provision of a national 24/7 pre-implantation biopsy service results, at reasonable cost, in transplantation of a greater proportion of kidneys offered from donors aged ≥60, and/or

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
6 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
improves kidney transplant function at one year post-transplant. Numbers of deceased donor kidney transplants performed annually in the UK are consequently significantly increased or improved in quality.
Primary outcome measures
1. Proportion of kidneys that are transplanted on first offer. 2. Estimated glomerular filtration rate (eGFR) measured at 10-15 months after transplant.
Secondary outcome measures
● ● Proportion of kidneys utilised ● Total number of kidney transplants performed, overall and
by centre ● Proportion of kidneys discarded after retrieval, out of all
retrieved kidneys ● Number and proportion of ‘single’ vs ‘dual’ kidney
transplants performed ● Absolute number of kidneys transplanted (per centre and
per time period) that were not accepted on first offer ● Biopsy utilisation and fidelity, defined as the proportion of
kidneys that are biopsied in concordance with the education plan, out of all kidney biopsies.
● Kidney Donor Profile Index (KDPI1) of transplants performed
● Cold ischaemia time (CIT) of transplanted kidneys ● 12-month recipient survival ● 12-month graft survival (censored for recipient death) ● Proportion of kidneys diagnosed with primary non-function ● Proportion of kidneys diagnosed with delayed graft function
(use of dialysis during the first postoperative week)
Subgroup Analysis ● ● DBD only ● DCD only ● Donors who are aged >70 years ● Centres with a historically low median UK Kidney Donor
Risk Index of transplanted DCD kidneys (low risk transplants compared to overall UK activity)
● Outcome for contralateral kidney from same donor when not subject to PITHIA biopsy
Duration of Study
Duration of cluster recruitment: All centres will be recruited prior to commencement of study
Duration of baseline monitoring: 4 months Duration of cluster intervention steps: 20 months (each
step is 4 months in duration) Duration of follow up: 12 months Overall: 36 months
Countries of recruitment United Kingdom
Target Sample Size
All adult UK transplant centres will be invited to participate in the study, except Cambridge. This is a total of 22 centres. Between 1st April 2014 and 31st March 2016, there were a total of 2306 first kidney offers for deceased (DBD and DCD) donors aged 60 years or over in the UK, excluding Cambridge. We estimate a similar number will be included in the analysis of the primary outcome measure.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
7 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Date of first enrolment October 2018
Recruitment Status Recruitment
Contact Details for Public Queries
Emma Laing NHS Blood and Transplant Long Road Cambridge CB2 0PT Tel:01223 588091 [email protected] / [email protected]
Contact Details for Scientific Queries
Gavin Pettigrew Level 9, Surgery Addenbrooke’s Hills Rd Cambridge CB2 0QQ
CTU Project Manager
Alison Deary Head of Operations, CTU NHS Blood and Transplant Long Road Cambridge CB2 0PT [email protected]
Lay Summary of Study There is a great shortage of kidneys for transplantation. All kidneys from deceased donors carry risk to the recipient (risk of not working, or of disease transmission), but donor age is strongly associated with poor function and early failure of the kidney transplant. This is important; because the majority of the pool of potential UK deceased donors are now over 60 years old. Thus, if we can improve our identification of kidneys from older donors that are better ‘quality’, we can maximise numbers of transplants performed without compromising transplant outcomes. The use of urgent kidney biopsy (analysis of a small portion under the microscope) to identify age-related damage has been reported to aid selection of those kidneys from older donors that are good enough ‘quality’ for transplantation. This approach has not been widely adopted in the UK, because the exact impact that the extra information provided by biopsy has on transplant numbers and on transplant outcomes is not clear, and its cost effectiveness remains unproven. Our study will evaluate whether providing an urgent 24-hour National Biopsy Service increases the number and function of kidneys transplanted from donors aged over 60 years. The study is a national trial: every four months a randomly-chosen group of UK kidney transplant centres will be offered access to the National Biopsy service (a ‘stepped-wedge randomised cluster trial’). By the end of the trial, all UK centres will have access, and we will then compare results for each centre from before and after the biopsy service was made available, as well as evaluating the cost of providing the service. We anticipate

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
8 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
that this comparison will show that biopsy availability increases the use of kidneys from elderly donors by about 11%, which equates to an additional 120 kidney transplants performed in the UK per year.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
9 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Figure 1(a): Individual participant schema
(Control)

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
10 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Figure 1(b): Individual participant schema
(Intervention)

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
11 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Figure 2: PITHIA Schema; stepped-wedge cluster randomised trial

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
12 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Contents
Contents
1. Background 16
1.1 Introduction ....................................................................................................................................... 16
1.2 Need for a trial .................................................................................................................................. 16
1.3 Explanation for choice of comparators ............................................................................................. 16
1.4 Description and justification of trial design ...................................................................................... 17
1.5 Potential benefits and risks of intervention ...................................................................................... 17
1.6 Specific objectives or hypotheses ..................................................................................................... 18
2. Study Setting 19
3. Selection of Sites 19
3.1 PI Qualifications and Agreements 19
3.2 Site Inclusion Criteria......................................................................................................................... 20
3.3 Site Exclusion Criteria ........................................................................................................................ 20
4. Inclusion and Exclusion Criteria ......................................................................................................... 20
4.1 Inclusion Criteria................................................................................................................................ 20
4.2 Exclusion Criteria ............................................................................................................................... 20
4.3 Co-Enrolment Guidelines .................................................................................................................. 20
5. Randomisation 20
5.1 Allocation – sequence generation ..................................................................................................... 20
5.2 Allocation – concealment mechanism .............................................................................................. 20
5.3 Allocation – implementation ............................................................................................................. 21
5.4 Blinding .............................................................................................................................................. 21
6. Intervention and Control Conditions 21
6.1 Introduction ....................................................................................................................................... 21
6.2 Interventions (See Figures 1a&1b) .................................................................................................... 21
6.2.1 Intervention Group 21
6.2.2 Control Group 22
6.2.3 Discontinuation of the Intervention 22
6.3 Adherence to intervention ................................................................................................................ 22
6.4 Concomitant Care .............................................................................................................................. 22
7. Study Outcomes 23
7.1 Primary Outcome Measure(s) ........................................................................................................... 23
7.2 Secondary Outcome Measures ......................................................................................................... 23

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
13 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
7.2.1 Safety Outcome Measures 23
7.3 Subgroup Analyses ............................................................................................................................ 23
8. Assessments and Follow-up 24
8.1 Trial Assessment Schedule ................................................................................................................ 24
8.2 Procedures for Assessing Efficacy of service ..................................................................................... 24
8.3 Procedures for Assessing Safety of service ....................................................................................... 24
8.4 Loss to Follow-Up .............................................................................................................................. 24
8.5 Trial Closure ....................................................................................................................................... 24
9. Safety Reporting 25
9.1 Definitions of Adverse Events ........................................................................................................... 25
9.2 Sponsor’s Responsibilities ................................................................................................................. 25
10. Quality Assurance and Control 25
10.1 Risk Assessment ................................................................................................................................ 25
10.2 Central Monitoring at CTU ................................................................................................................ 26
10.2.1 Direct access to patient records 26
10.2.2 Confidentiality 26
10.3 Auditing ............................................................................................................................................. 26
10.4 Histopathologist Concordance .......................................................................................................... 26
11. Statistical Considerations 27
11.1 Method of Generating Allocation Sequence ..................................................................................... 27
11.2 Outcome Measures ........................................................................................................................... 27
11.3 Sample size ........................................................................................................................................ 27
11.4 Interim Monitoring and Analyses ...................................................................................................... 30
11.5 Analysis Plan (Brief) ........................................................................................................................... 30
11.5.1 Analysis of primary and secondary outcomes 31
11.5.2 Other Analyses 32
11.5.3 Health Economic Analysis .......................................................................................................... 32
12. Ethical and Regulatory Issues 34
12.1 Compliance ........................................................................................................................................ 34
12.1.1 Site Compliance 34
12.1.2 Data Collection and retention 34
12.1.3 Access to Data 34
12.2 Ethical Conduct of the Study ............................................................................................................. 34
12.2.1 Ethical Considerations 34
12.2.2 Consent 34

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
14 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
12.3 Confidentiality ................................................................................................................................... 35
12.4 Other approvals ................................................................................................................................. 35
13. Indemnity 36
14. Finance 37
14.1 Funding .............................................................................................................................................. 37
14.2 Declaration of interests ..................................................................................................................... 37
15. Oversight and Trial Committees 38
15.1 Trial Management group (TMG) ....................................................................................................... 38
15.2 Trial Steering Committee .................................................................................................................. 38
15.3 Data Monitoring Committee ............................................................................................................. 38
15.4 Role of Study Sponsor ....................................................................................................................... 39
15.5 Role of Study Funder(s) ..................................................................................................................... 39
16. Publication 39
16.1 Dissemination .................................................................................................................................... 39
16.2 Authorship ......................................................................................................................................... 39
16.3 Approvals ........................................................................................................................................... 39
16.4 Identification ..................................................................................................................................... 40
16.5 Timing ................................................................................................................................................ 40
16.6 Acknowledgements ........................................................................................................................... 40
17. Protocol Amendments 40
18. Appendices 41
19. References 45

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
15 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Abbreviations and Glossary
AE Adverse event AR Adverse reaction CI Chief Investigator CIT Cold Ischaemic Time CRN Clinical Research Network COM Clinical Operations Manager CRF Case Report Form CTU NHSBT Clinical Trials Unit CUH DBD DCD DCF
Cambridge University Hospitals NHS Foundation Trust Donation after brain death Donation after circulatory death Data Clarification Form
DH Department of Health DM Data Manager DMC Data Monitoring Committee eGFR Estimated Glomerular Filtration Rate GCP Good Clinical Practice GP General Practitioner HE Health Economics HRA Health Research Authority HTA Human Tissue Authority ICC Intra-Cluster Correlation DMC Data Monitoring Committee ISRCTN International Standard Randomised Controlled Trial Number IRAS KDPI
Integrated Research Application System Kidney Donor Profile Index
MRC Medical Research Council NHS National Health Service NHSBT NHS Blood and Transplant NIHR National Institute for Health Research NORS National Organ Retrieval Service ODT Organ Donation and Transplantation PI Principal Investigator PITHIA Pre-Implantation Trial of Histopathology In renal Allografts
QC Quality Control QUOD Quality in Organ Donation programme (NHSBT) R&D Research and Development RCT Randomised Controlled Trial REC Research Ethics Committee RfPB Research for Patient Benefit (NIHR funding stream) RGF Research Governance Framework SNOD SOP
Specialist nurse for organ donation Standard operating procedure
SPK Simultaneous Pancreas Kidney [TBC] To be confirmed TMF Trial Master File TMG Trial Management Group TSC UKTR
Trial Steering Committee UK Transplant Registry

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
16 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
1. Background
1.1 Introduction
Kidney transplantation remains the best treatment option for most patients with end-stage renal disease2,3, but shortages in organs mean that patients in the UK wait around three years for a transplant4. Over half of the UK pool of potential deceased donors (people dying in critical care) are over 60 years old. Kidneys from donors aged over 60 have been shown to carry a significantly higher risk of failure than those from younger donors5. Consequently, only approximately 20-30% of kidneys from potential older donors are eventually transplanted - the remainder are discarded6.
1.2 Need for a trial
One approach to assessing which of these kidneys from older donors are safe to implant is to perform a biopsy of the kidney upon procurement at the donor operation. The biopsy is then assessed histologically and the severity of chronic background injury scored from 0 (no injury) to 12 (severely diseased). Remuzzi has shown that this score correlates with subsequent transplant outcome, and has proposed that depending on the score, the kidney can either be transplanted singly, discarded, or both kidneys from one donor transplanted into a single recipient7. One UK centre (Cambridge) has established a ‘pre-implantation biopsy service’ using the Remuzzi scoring system, but, with a modified interpretation of the result. Remuzzi’s original description advised clinicians to implant kidneys with scores of 1-3 out of 12 as single transplants and those with intermediate scores of 4-6 as duals. Kidneys with scores >6 were thought to be unsafe for implantation. The Cambridge experience demonstrated that kidneys with scores of 4 are safe to implant singly and those with scores of 5-6 transplanted as part of a dual transplant. Local results suggest that this approach enabled greater numbers of kidney transplants to be performed from older donors than would otherwise have been the case. Outcomes of these transplants are good, in that kidney graft survival is similar to that achieved for all UK deceased-kidney transplants - irrespective of donor age 8–10.
The Remuzzi approach has however, not become widely adopted. To avoid unnecessary delays in transplanting the kidney (which may adversely affect outcomes), the kidney biopsy must be processed as quickly as possible. This requires an urgent, out-of-hours renal histopathology service which may be costly for an individual centre. Concerns persist that the use of urgent histopathology may lead to discard of kidneys that would have otherwise provided satisfactory transplant function11. For this reason, relatively few transplant centres rely on urgent histopathology evaluation; consequently, its efficacy and cost effectiveness remain unknown.
1.3 Explanation for choice of comparators
The trial question is whether access to urgent histopathology results in an increase in the number of kidney transplants performed, whilst ensuring the outcomes of these transplants are acceptable. Because it was deemed unfair to limit the histopathology service to only some UK transplant centres (this would result in inequity of access for those patients whose centres did not receive the biopsy service), the trial has been designed according to a step wedge cluster randomised trial. This way, all UK renal transplant centres will benefit from access to the biopsy service at some point during the trial. This design will preserve equity of access to transplantation at the national level. The justification of trial design is discussed in further detail below12.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
17 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
1.4 Description and justification of trial design
This is an open, multicentre, stepped-wedge cluster randomised trial, with concurrent economic evaluation, which will assess the use of pre-implantation histopathology in kidney transplantation. It will compare the number of transplants performed, and the outcomes of these transplants, before and after the centre gains access to urgent histopathology assessment.
All UK adult kidney transplant centres, excluding Cambridge, (22) will participate over a 24 month period. Each transplant centre represents one cluster, and at 4-monthly intervals a new randomly selected group of clusters will be given access to the national histopathology service. Access enables clinicians to request pre-implantation biopsy analysis as a means of evaluating the suitability of a given kidney for transplantation.
Trial implementation of a national histopathology service is not straightforward. A simple comparison of UK transplant activity before and after the introduction of the service would be unable to distinguish the impact of histopathology availability from natural evolution of transplant practice. Similarly, a randomised trial in which individual kidneys are offered randomly with or without biopsy availability is not practical, because the availability of the biopsy information for only some kidneys is likely to 'contaminate' (i.e. change) implantation practice of kidneys offered without. Consequently, for the pool of elderly DCD and DBD kidney donors, introduction of such a trial is likely to lead to immediate reduction in acceptance of those kidneys offered without a biopsy; simply holding the trial would alter existing practices towards older kidney offers.
The stepped-wedge design has several advantages over a standard parallel cluster trial. Firstly, PPI feedback was strongly of the opinion that all centres receive access to the service at some stage, otherwise waiting list patients at centres with particularly long waiting times who never receive access to the service may remain disadvantaged. Secondly, the stepped-wedge approach allows us to stagger the intervention across the UK and allows the trial group the necessary time to provide a thorough education programme at each participating centre. This will involve a discussion of the indications for, and subsequent interpretation of, an urgent kidney biopsy12. Finally, because each cluster is large (small number of centres in the UK), a parallel design is less efficient compared to a stepped-wedge study, for all likely values of intra-cluster correlation.
The primary analysis will then focus on the proportion of kidneys which are transplanted on first offer from DBD and DCD donors aged ≥ 60 years. First offer acceptance is likely to be more resistant to ‘contamination’ effects; for example, when a centre with the biopsy service rejects a kidney, which is then offered to a second centre that does not yet have access to the biopsy service. On ethical grounds, the biopsy information will be made available to the second centre.
PITHIA is a registry-based randomised trial, in which follow-up data are routinely collected as part of the mandatory post-transplant UK Transplant Registry (UKTR), held by NHS Blood and Transplant. This has multiple advantages. Firstly, the trial can be performed without burdening patients with extra appointments, tests or added bureaucracy. Secondly, once the trial is established, transplant centres will have almost no extra work related to the trial. As a result, trial costs are minimised, making this a particularly cost effective approach13.
1.5 Potential benefits and risks of intervention
Increased numbers of kidney transplants and improved outcomes for those kidneys transplanted are the main potential benefits, as reflected in the primary outcome measures. The main risk of the intervention relates to the possibility of biopsy-related complications. Biopsy of transplanted kidneys carries a 1-2% risk of haemorrhage requiring blood transfusion. The incidence of biopsy related

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
18 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
complications following pre-implantation punch-biopsy of retrieved kidneys has not been formally reported, but the Cambridge Transplant Centre has been performing punch biopsy of implanted kidneys for ~18 months, without incident. Nevertheless, we predict the risk of biopsy-related haemorrhage will be about 1% in this study. This risk of haemorrhage will be factored by the responsible clinical team into the risk-benefit analysis of performing biopsy for the particular recipient of the offered kidney. It should be noted that, 85% of deceased-donor kidneys are already biopsied at retrieval for future experimentation (by the national QUOD bioresource, sponsored by NHSBT in close collaboration with all academic centres in the UK: http://www.quod.org.uk), and to date, there has been one reported graft loss due to biopsy related complications. Moreover, the choice of biopsy technique (punch biopsy) has been made following consultation with renal histopathologists and transplant surgeons; this technique is expected to further limit the risk of complications, as well as limit inter-observer differences in the quality of biopsy performed. There is also a risk that the biopsy service may lead to a reduction in the number of kidneys transplanted, because more kidneys are discarded following biopsy analysis. This, however, relates to a primary outcome of the trial, and is one of the main reasons for performing the trial. By the nature of the trial design, it will not be possible to ascertain diminished kidney usage until formal analysis of data after the trial is completed.
1.6 Specific objectives or hypotheses
This study will address how the introduction of a national histopathology service impacts upon UK kidney transplant practice, and will test the hypothesis: ‘Provision of a national 24/7 pre-implantation biopsy service results, at reasonable cost, in transplantation of a greater proportion of kidneys offered from deceased donors aged ≥ 60 years, and /or improves kidney transplant function at one year post-transplant. Numbers of deceased donor kidney transplants performed annually in the UK are consequently significantly increased or improved in quality.’ The study aims to: ● Introduce an efficient national histopathology service that uses electronic image transfer to
rationalise biopsy processing to a limited number of designated transplant centres. This will provide immediate access of the images to a team of specialist renal histopathologists located throughout the UK.
● Perform a randomised evaluation of this service, by staggering its introduction to UK renal transplant centres that do not currently have 24hr on call histopathology available (all but one centre). The evaluation will adhere to the principles of a stepped-wedge cluster randomised trial.
● Determine the cost-effectiveness of this service. ● Model an efficient randomised registry trial, which can be performed for relatively little cost
(because outcome data are already collected centrally), and which will provide a template for future transplant research.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
19 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
2. Study Setting This trial will be conducted in UK Adult Renal Transplant Centres (excluding Addenbrooke’s Hospital, Cambridge – although it is a pathology centre):
1. Belfast James McDaid
2. Birmingham Adnan Sharif (pathology centre)
3. Bristol Samuel Turner
4. Cardiff Laszlo Szabo
5. Coventry Debabrata Roy
6. Edinburgh John Terrace (pathology centre)
7. Glasgow Karen Stevenson
8. Guy’s Hospital Chris Callaghan
9. Hammersmith Hospital Frank Dor
10. Leeds Adam Barlow (pathology centre)
11. Leicester Atul Bagul
12. Liverpool Dan Ridgway
13. Manchester Zia Moinuddin
14. Newcastle Colin Wilson (pathology centre)
15. Nottingham Sam Dutta
16. Oxford Simon Knight
17. Plymouth Peter Rowe
18. Portsmouth Paul Gibbs
19. Royal Free Hospital Gareth Jones (pathology centre)
20. Royal London Rajesh Sivaprakasam
21. Sheffield Badri Shrestha
22. St George’s Hospital Abbas Ghazanfar
A centralised approach has been developed to provide the urgent histopathology service. This makes use of the infrastructure already provided by the National Organ Retrieval Service (NORS), which is needed for a pragmatic introduction of this service (as providing local urgent histopathology at each of the remaining 22 UK renal transplant centres would have prohibitive cost and staffing implications, particularly for smaller centres). Of the 10 abdominal NORS team bases, six (Royal Free, Birmingham, Leeds, Cambridge, Newcastle and Edinburgh) have been identified to provide 24-hour histopathology processing and biomedical scientist on-call cover. These centres provide good geographical coverage, therefore minimising delay due to biopsy travel.
3. Selection of Sites
3.1 PI Qualifications and Agreements
The investigator should be qualified by education, training and experience to assume responsibility for the proper conduct of the trial at their site and should provide evidence of such qualifications through an up to date curriculum vitae and/or other relevant documentation requested by the Sponsor, the REC, and/or the regulatory authorities.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
20 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
3.2 Site Inclusion Criteria
All UK adult kidney transplant centres (excluding Cambridge) have been invited to take part, and we have received letters of support from responsible authorities in each unit.
3.3 Site Exclusion Criteria
Only those sites which withdraw their consent to participate in the trial will be excluded.
4. Inclusion and Exclusion Criteria The inclusion and exclusion criteria for the urgent histopathology service are detailed below. A biopsy can be requested (at the time of offer) for organs which meet all the inclusion criteria and none of the exclusion criteria. The decision of whether to biopsy an eligible organ is that of the transplanting surgeon.
4.1 Inclusion Criteria
1. Kidneys offered for transplantation from deceased donors (DCD and DBD) aged ≥60 years.
4.2 Exclusion Criteria
1. All kidneys offered as a component of a multi-organ transplant.
4.3 Co-Enrolment Guidelines
This study does not constrain the behaviour of individual transplant centres in any way, nor does it prevent the use of organs in research, or quality assurance of any other project. For donors who have also consented to provide research samples for QUOD, it has been agreed that the PITHIA biopsy will have priority (only one biopsy is to be taken of a donor kidney).
5. Randomisation This trial will use a stepped wedge cluster randomised design. The unit of randomisation (cluster) will be the renal transplant centre. Each cluster will start off in the control condition and will be randomly allocated to the order with which they will switch to the intervention condition. There will be five switch dates, each of which will see four or five clusters transitioning in one step (Figure 2).
5.1 Allocation – sequence generation
We will use a restricted randomisation technique to randomly allocate the clusters to their cross-over date. To this end, we randomly select an allocation sequence (i.e. a cross-over order for the clusters) from a set of sequences constrained so that the sum of the total cluster sizes in the intervention status is similar to the total sum of the cluster sizes in the control status. We define ‘similar’ as a difference in the total sums (kidneys) exposed to intervention and control statuses being no different than expected middle 25th percentile range of differences.
5.2 Allocation – concealment mechanism
This allocation will be performed once all site approvals are in place (to be sure that all included sites will participate in the trial). The allocation will be held and implemented by the Independent

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
21 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Trial Statistician and will be revealed to the sites and trial team approximately three months before the date of transition of that site, to allow time to organise the education day at each site.
5.3 Allocation – implementation
To implement this, we will perform 10,000 simulations, of possible allocation sequences (or the exhaustive list of possible allocation sequences if this is fewer than 10,000). Using this and data extracted from the UKTR on the number of first kidney offers from deceased donors aged ≥60 between 1 April 2015 and 31 March 2017, we will determine for each sequence the difference in number of kidneys that would have been exposed to intervention and control. We will then select at random an allocation sequence from those falling within the middle 25th percentile range of differences.
5.4 Blinding
It is not possible to blind sites to their participation in the trial and therefore the trial will have an open design with no blinding to the intervention, once their date of transition from control to intervention has been revealed to them (3 months prior to the transition). This confers the additional benefit of enabling a structured and planned education programme to be delivered to each centre prior to their access to the biopsy service. Members of the trial team will also be blinded to when each cluster will be transitioning to the intervention and this will only be revealed to them 3 months prior to each site transitioning. After this point the trial team will be unblinded to the intervention.
6. Intervention and Control Conditions
6.1 Introduction
This is a stepped-wedge cluster randomised trial. All clusters will serve as their own control in the period prior to their exposure to the intervention. Once their centre has crossed over, the implanting surgeon will be able to request a pre-implantation biopsy on any kidney from a deceased donor. All biopsies will then be analysed and reported by a trained renal histopathologist (sited locally or remotely).
6.2 Interventions (See Figures 1a&1b)
6.2.1 Intervention Group
Access to national histopathology service: Transplant centres can request a kidney biopsy at the time of offering via NHSBT Hub Operations. Requesting a biopsy is not mandatory – the transplant centres can use the service at their discretion. A size 4 mm punch biopsy will be performed at the retrieval operation by the attending NORS team and will be placed in formalin whole. The PITHIA biopsy will be recorded on the HTA-A form, to ensure traceability is maintained. This trial will make use of the existing infrastructure of NHSBT's QUOD programme which provides the training, tracking and tracing qualifications required by HTA and NHSBT. The transplanting surgeon is responsible for closure of the biopsy site. The biopsy will be transported to the most appropriate histopathology centre. The most appropriate histopathology centre will be determined on a case by case basis by NHSBT Hub Operations. Appendix 2 outlines the schematic to support decision making. Once the biopsy arrives at the processing centre, the on-call biomedical scientist will prepare the specimen prior to scanning and uploading for review by the histopathologist who is also on-call. We have established a national

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
22 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
consortium of 15 consultant renal histopathologists who will score, remotely, the severity of baseline injury, and relay their assessment to the relevant transplant clinicians. Consent for the transplant will be obtained from the potential recipient following a discussion of the potential risks and benefits of the individual kidney on offer, in line with current standard practice and national guidelines. The biopsy result, if available, will help inform these discussions.
6.2.2 Control Group
Usual care: Therefore, no access national histopathology service. Centres are free to act as they otherwise would outside of the trial, and their activity will be monitored. Deceased donor kidney offering is coordinated centrally by NHSBT Hub Operations. The offering sequence is points-based system determined by a combination of recipient waiting time, recipient age, HLA match, age match and geographical factors. Background information about the donor and potential transplant is included at the time of the offer. Further information is available at ‘https://www.odt.nhs.uk/transplantation/tools-policies-and-guidance/policies-and-guidance/#kidney’.
6.2.3 Discontinuation of the Intervention
Transplant centres can use the service at their discretion, hence will be able discontinue using the intervention at any time.
6.3 Adherence to intervention
Introduction of the histopathology service to a centre will be preceded by a dedicated education package provided by a team of surgeons, renal nephrologists and renal histopathologists. This will detail the best available evidence to help guide how the biopsy analysis informs the decision to implant a deceased donor kidney. We are committed to providing this education package, which will consist of visits to each centre by a team of surgeons, renal nephrologists and renal histopathologists. They will meet with both transplant clinicians as well as local patient groups, to discuss how the histopathology service should be used, and how this may help in selection of kidneys for implantation. Transplant centres are not obliged to follow our guidelines for biopsy use; they, along with their patients, retain the final say over whether a kidney should be transplanted or not. However, the use of biopsies will be evaluated as part of a secondary trial analysis. The focus of this evaluation will be on how the service is used (which kidneys are biopsied and which are not) and how the information is acted on (which kidneys are transplanted and which are not). A further educational meeting will be held in the second month following access of each centre to the intervention (biopsy service). An analysis of that centre’s response to offers from all deceased donors over 60 and utilisation of the biopsy service for the first month will be presented and discussed. The eventual outcome (transplanted / discarded) for the offered kidney, and the contralateral kidney from the same donor, will be presented – this data is already routinely provided to each transplant centre by NHSBT, with centres encouraged to hold routine meetings to review utilisation practice. The PITHIA review meeting will be incorporated into the centre’s standard ‘utilisation’ meeting, where possible. The biopsy service will be evaluated on an intention to treat basis. We accept that in rare cases a biopsy may be requested but not performed, or processed and reported. This reflects the practical reality of any service.
6.4 Concomitant Care
There are no restrictions placed on how transplant centres manage their patients during the trial.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
23 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
7. Study Outcomes All outcome data will be obtained from the UKTR, held by NHSBT.
7.1 Primary Outcome Measure(s)
1. Proportion of kidneys that are transplanted on first offer. 2. Estimated glomerular filtration rate (eGFR) measured at 10-15 months after transplant14.
7.2 Secondary Outcome Measures
● Proportion of kidneys utilised ● Total number of kidney transplants performed, overall and by centre ● Proportion of kidneys discarded after retrieval, out of all retrieved kidneys ● Number and proportion of ‘single’ vs ‘dual’ kidney transplants performed ● Absolute number of kidneys transplanted (per centre and per time period) that were not
accepted on first offer ● Biopsy utilisation and fidelity, defined as the proportion of kidneys that are biopsied in
concordance with the education plan, out of all kidney biopsies. ● Kidney Donor Profile Index (KDPI)1 of transplants performed ● Cold ischaemia time (CIT), defined as the total time between perfusion of the donor kidneys
with cold preservation fluid during retrieval, and reperfusion with recipient blood at implantation.
● 12-month patient survival ● 12-month graft survival (censored for patient death) ● Proportion of kidneys diagnosed with primary non-function ● Proportion of kidneys diagnosed with delayed graft function (defined as the use of dialysis
during the first postoperative week)
7.2.1 Safety Outcome Measures
● Biopsy-related complication rate
7.3 Subgroup Analyses
● DBD donors only ● DCD donors only ● Donors who are aged >70 years ● Centres with a historically low median UK Kidney Donor Risk Index of transplanted DCD
kidneys (low risk transplants compared to overall UK activity) ● Outcome for contralateral kidney from same donor when not subject to PITHIA biopsy

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
24 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
8. Assessments and Follow-up
8.1 Trial Assessment Schedule
Trial participants will not undergo any additional assessment for the trial, over and above those which they would typically receive as part of their usual care. Therefore, no trial assessment schedule is required.
8.2 Procedures for Assessing Efficacy of service
The trial will use data that is routinely collected on the national UKTR, held by NHS Blood and Transplant. The national registry has a mandatory collection system that produces comprehensive information on organ donors, organs, transplants and recipients. Some follow up data (particularly eGFR) is known to be only 90% complete – individual renal centres will be given assistance from the NHSBT CTU to ensure as complete return as possible.
8.3 Procedures for Assessing Safety of service
Incident reports submitted to NHSBT which relate to biopsy complications will be monitored by the NHSBT CTU, and periodically assessed by the Data Monitoring Committee in order to evaluate safety. Cold ischaemia time will also be monitored by the DMC. For full detail, refer to Section 9 – Safety Reporting.
8.4 Loss to Follow-Up
We anticipate that loss to follow up will be an uncommon event. Transplant recipients within the first year usually represent a highly motivated, engaged patient group who are followed up extremely closely outside of the trial environment. Data needed for this trial is mandated for collection by NHSBT and collected independently of the trial. Any data required for this trial which are noted to be missing will be highlighted and chased up by the CTU and ODT Hub Information Services at NHSBT.
8.5 Trial Closure
The trial will end 12 months after the final cluster have had access to the histopathology service for four months (36 months after the beginning of the trial). This allows 12-month eGFR to be recorded for all kidneys which are eligible for inclusion in the analysis. The trial has no planned early-stopping criteria. The TSC have the power to stop the trial on safety grounds.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
25 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
9. Safety Reporting Organ biopsies are a routine part of clinical practice, and today, a large proportion of retrieval hospitals participate in the national QUOD programme (http://www.quod.org.uk/index.html) which requires samples to be taken from organs. According to HTA regulations, QUOD reports monthly on general incidents without consequences for patients as well as on serious adverse events with
consequences for patients related to the kidney biopsies obtained. Current update reveals 9/3128
and 5/3128 incidents (2014-2017), respectively. This is below the 5% complication rate of percutaneous ‘Tru-Cut’ biopsies of transplanted kidneys reported in the literature. But the Cambridge experience with punch biopsy suggests that the rate is considerably less than that reported for native kidney biopsy, and this is consistent with published literature15. Reports are periodically sent to the HTA, Senior Management Teams and Advisory Groups within NHSBT. It is a statutory condition of a licence for procurement or transplantation activity to rapidly report to NHSBT (acting on behalf of the HTA), relevant and necessary information concerning adverse events which may influence the quality and safety of organs as a result of testing (which includes biopsy testing). For PITHIA, centres will therefore follow their usual procedures for highlighting concerns – by completing an NHSBT incident submission form https://safe.nhsbt.nhs.uk/IncidentSubmission/Pages/IncidentSubmissionForm.aspx. These reports will be reviewed periodically by the Data Monitoring Committee (DMC). Untoward incidents related to the process of organ retrieval and transplantation is routinely collected by NHSBT. Further detail may be found here: http://www.odt.nhs.uk/odt/governance-and-quality/incident-reporting/.
9.1 Definitions of Adverse Events
In this trial, the adverse events of interest are any biopsy-related complications (e.g. haemorrhage, nephrectomy, blood transfusion) in the donated kidney. As described above, these will be reported routinely to NHSBT. All kidneys which have been biopsied as part of PITHIA will be flagged and notified to the NHSBT CTU trial team.
9.2 Sponsor’s Responsibilities
● The CTU (on behalf of the Sponsor) will forward all adverse events to the Chief Investigator
(or a medically qualified delegate) for review. ● As biopsy-related complications are the main safety outcomes of interest, the Trial Manager
will maintain a log of all adverse events, which will be presented to the Trial Management Group (TMG) at their monthly meetings. All serious / biopsy-related reports must also be sent to all members of the DMC in real-time.
● The DMC will meet at approximately 6-monthly intervals. A line listing of all reported events will be presented at those meetings.
● A copy of each DMC report will be provided to the Sponsor. ● Any event that requires reporting to the Human Tissues Authority (HTA) will be reported via
NHSBT normal avenues, as per standard practice.
10. Quality Assurance and Control
10.1 Risk Assessment
A risk assessment has been conducted which acknowledges the potential risks to the trial. This section provides an overview of the Quality Assurance (QA) and Quality Control (QC) measures

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
26 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
that will be put in place to ensure the trial is performed and data generated and recorded in accordance with the principles of ICH GCP.
10.2 Central Monitoring at CTU
The CTU will work with the ODT Hub Information Services at NHSBT to ensure that any missing data required for the trial outcome measures are as complete as possible.
10.2.1 Direct access to patient records
The only data which will need to be accessed is that pertaining to the UKTR, held by NHSBT which patients consent for on receiving an organ transplant. Approval for use of this data for the trial has been approved by NHSBT.
10.2.2 Confidentiality
The data will be handled in accordance with the principles of the UK Data Protection Act.
10.3 Auditing
In addition to potential audits by the local R&D department, NHSBT CTU reserves the right to conduct site audits, either as part of its ongoing audit programme, or in response to adverse observations during monitoring of the trial data.
10.4 Histopathologist Concordance
The Consultant Histopathologists participating in the trial will undergo formal training in using the Remuzzi scoring system as follows:
An initial ‘calibration’ session, using visual aids and discussion to align boundaries for scoring.
Histopathologists will be asked to score 30 cases online. This will be compared to the ‘true’ scores decided by a central team of lead histopathologists. A weighted Kappa statistic will be calculated and used to help decide if a histopathologist requires further training.
An additional session may be required to discuss difficult cases and for further education. This may lead us to require a further 20 cases be marked prior to the trial beginning. We expect this process will allow the identification of outlier pathologists who require further training to achieve concordant marking, or who need not be included in the initial on-call rota.
Secondary review of the biopsies analysed during the trial is planned to ensure reliability and reproducibility: After the first year, a set of 100 cases will be identified and subjected to a secondary blind review by a central team of lead histopathologists. These cases will be selected to ensure that all reporting histologists are represented proportionally. Further education or rota management can be planned following this exercise, which is aimed at achieving the highest possible consistency in reporting.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
27 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
11. Statistical Considerations
11.1 Method of Generating Allocation Sequence
See Section 5
11.2 Outcome Measures
See Section 6
11.3 Sample size
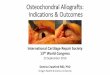
We plan to enrol a minimum of 20 UK kidney transplant centres (clusters), but have received positive responses from 22 centres. Power calculations are nevertheless based on just 20 clusters to allow for subsequent nonparticipation (albeit unlikely because biopsy availability will be provided as a free, ‘no-strings-attached’ service). The intervention will be implemented across 5 steps; each step is four months in duration, with 4 or 5 clusters being randomly chosen to cross at each step. There are no planned ‘roll-out’ periods within the study, because, upon randomisation, the system is made immediately available to that centre. The study will run for 24 months (4 months baseline monitoring at the start of the trial and then 5 steps all with a duration of 4 months), with an additional 12 months follow up. It has been shown that stepped wedge trial designs are minimally affected by varying cluster size16 hence we have not allowed for variation in cluster size in this power calculation. We will, however, use a restricted randomisation method to insure against a large imbalance in cluster size across the steps (see section 5- Randomisation for further details). Estimates for the sample size calculations were obtained from the UKTR, held by NHSBT. We followed the methodology proposed by Hooper et al. (2016)17 and Hooper and Bourke (2015)18 and this was implemented using SAS (version 9.4, Cary, NC) and an RShiny app (https://clusterrcts.shinyapps.io/rshinyapp/). We have checked sensitivity to these power calculations across a range of intra-cluster correlations (ICCs) and baseline proportions. As we have two primary outcomes a Bonferroni correction was applied and hence a 2.5% significance level will be used. Both primary outcomes will test a superiority hypothesis. 11.3.1 First Primary Outcome The first primary outcome is the proportion of kidneys that are transplanted on first offer. In the UK, if one centre declines the offer of a deceased kidney, that kidney is then offered to another centre. However, this first primary outcome will only analyse transplantation rates of the first offer for each kidney. Otherwise, a centre that has yet to receive urgent biopsy availability may be offered a kidney that has been declined by another centre, but only after biopsy has been performed. In such a case, it would be inappropriate to not inform the second centre of the biopsy results. In terms of utilisation, dual kidney transplants (transplanting both kidneys into one recipient) are not as effective as performing two single transplants (transplanting the kidneys singularly into two recipients); however both of these situations are better than discarding the kidneys. To account for this in this first primary outcome, if the first offers for a pair of kidneys results in a dual kidney transplant, then only one of the kidneys will be counted as being transplanted and the other will be counted as not transplanted. It is arbitrary whether the left or right kidney is counted as being transplanted because this is not accounted for in the analysis. Data was extracted on first kidney offers from potential deceased (DBD and DCD) donors aged 60 years and over, in the UK between 1 April 2014 and 31 March 2016. Offers of Simultaneous Pancreas Kidney (SPK), multi organ, fast track and any offers to Cambridge were excluded. The

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
28 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
percentage of first offers which were transplanted was 28.4%. The median number of first offers per cluster per month was 4.38. As the trial will be running for 24 months, it is anticipated that 2102 (=24 months *20 centres *4.38) kidneys will be offered during the trial across control and intervention periods. A mixed linear regression model was fitted to the extracted data, with a binary outcome (whether the offer resulted in a transplant), a fixed effect for date of offer (which converted each year into thirds i.e. six, four month time periods called period henceforth), a random effect for cluster and a random interaction between cluster and period. Restricted maximum likelihood was used for model estimation. From this model, the within period intra-cluster correlation and cluster autocorrelation were calculated as 0.03 and 0.92 respectively. Assuming an average cluster-period size of 18, to detect an 11% increase in the number of first offers transplanted the trial will have 85% power (assuming a significance level of 2.5%). An increase from 28% to 39% would represent a clinically important increase in the number of transplants. We have not allowed for attrition in this sample size calculation as there is unlikely to be any missing data. This is due to the robustness of the organ offering data collected by NHSBT – it is a mandatory requirement of the Human Tissue Act (2004) for NHSBT to collect data on the removal of organs from donors and to whom those organs are transplanted into. We checked the sensitivity of this calculation by looking at an increase, and separately a decrease, of 2% in the baseline proportion, and by varying the WP-ICC (lower WP-ICC set as 0 and upper WP-ICC set as 0.08) and the CAC (lower CAC set as 0.74 and upper CAC set as 1)). The trial has within the region of 80% power for all anticipated values of WP-ICC and CAC, and likely values of cluster-period sizes. The power curve, with the baseline proportion set as 28%, is shown in figure 3. Figure 3: Power curve for the first primary outcome, proportion of kidneys that are transplanted on first offer. The curves show the increase in power as the cluster size increases, for 20 clusters, 5 steps, 4 clusters crossing over at each step and the proportion under control and intervention of 28% and 39% respectively. The black curve shows the power for the base values of WP-ICC and CAC (0.03 and 0.92 respectively), and the remaining curves show for lower and upper levels of the WP-ICC (0 and 0.08 respectively) and CAC (0.74 and 1 respectively).

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
29 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
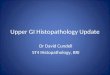
11.3.2 Second Primary Outcome The second primary outcome is the eGFR measured at one year after transplant. Data was extracted on all recipients who received a kidney only transplant from deceased donors (DBD and DCD) aged ≥60 years, in the UK between 1 April 2014 and 31 March 2016. Any recipient who received their transplant at Cambridge was excluded. The median number of transplant recipients per cluster per month was 2, hence providing an average cluster-period size of 8. As the trial will be running for 24 months, it is anticipated that 960 (=24 months*20 centres*2) kidney transplant recipient’s will be assessed for this eGFR outcome during the trial across control and intervention periods. eGFR was calculated using the MDRD formula using uncalibrated serum creatinine measurements14, hence if missing data was present for the recipients’ sex, age, ethnicity and serum creatinine at 12 months, then eGFR could not be calculated (19%). The mean eGFR was 41.91 with a standard deviation of 16.06. A mixed linear regression model was fitted to this data, with a continuous outcome (eGFR), a fixed effect for date of transplant (which was converted each year into thirds i.e. six, four month time periods), a random effect for cluster and a random interaction between cluster and period. Restricted maximum likelihood was used for model estimation. From this model, the within period intra-cluster correlation and cluster autocorrelation were calculated as 0.06 and 0.08 respectively. Assuming an average cluster-period size of 8 (which allows for dropout), this outcome will have 89% power to detect a mean difference of 6ml in eGFR (assuming a significance level of 2.5%). We checked the sensitivity of this calculation by looking at an increase, and separately a decrease, of 0.5 in the mean difference; and by varying the WP-ICC by +/-0.05 and CAC by +/- 0.016 (which equates to +/- 20% of the base CAC). The trial has within the region of 80% power for all anticipated values of WP-ICC and CAC, and likely values of cluster-period sizes. The power curve, with the mean difference set as 6, is shown in figure 4. As the CAC was particularly small, we separately explored the effects of a large CAC value (0.8) and found this had minimal impact.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
30 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
Figure 4: Power curve for the second primary outcome eGFR measured at 12 months after transplant. The curves show the increase in power as the cluster size increases, for 20 clusters, 5 steps, 4 clusters crossing over at each step and the mean difference of 6 and standard deviation of 16.06. The black curve shows the power for the base values of WP-ICC and CAC (0.06 and 0.08 respectively), and the remaining curves show for lower and upper levels of the WP-ICC (0.01 and 0.11 respectively) and CAC (0.06 and 0.10 respectively).
11.4 Interim Monitoring and Analyses
The Trial Manager will receive incident reports relating to biopsy complications that are fed back by individual centres to NHSBT. The Data Monitoring Committee (DMC) will review the biopsy complications data and have the power to recommend early closure to the Trial Steering Committee on the basis of harm. Formal rules to stop the trial on the grounds of futility or efficacy (for example by calculation of O’Brien Fleming boundaries)19, were deemed inappropriate for this trial due to the short duration and trial design. Similarly, it is not thought possible to assess biopsy related complications using formal statistical analysis. Instead, the DMC will be asked to review events, at intervals to be agreed with the committee, to allow them to make an informed judgement on these events. This proposal to not conduct a formal statistical test for harms is endorsed by the Spirit statement20.
11.5 Analysis Plan (Brief)
The analyses will be described in detail in a full statistical analysis plan. This section summarises the key issues.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
31 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
The baseline characteristics will be summarised by 1) exposure and non-exposure to the intervention (i.e. access to preimplantation biopsy service) and 2) by allocated sequence. These characteristics will include donor age, cause of death, co-morbidity, ethnicity, recipient age and recipient centre, and will be at individual level. All analyses will be performed on an intention to treat basis. This will include all eligible patients on whom values of a response variable have been obtained and will be analysed according to the treatment as specified in the randomisation list. The primary outcomes will be compared using two-sided tests and at a 2.5% significance level. Departures from randomisation at cluster level are defined as any cluster which does not switch to the intervention when stated in the randomisation list. A cluster is able to withdraw at any point during the trial. Per protocol analysis, which will exclude departures from randomisations and any cluster withdrawals, will also be completed for both primary outcomes of the trial.
11.5.1 Analysis of primary and secondary outcomes
All primary and secondary outcomes will adjust for period (since the intervention is sequentially rolled out) and cluster (as participants within the same centre are not independent). For the first primary outcome a logistic regression model, with random effects for cluster and cluster by period; and adjusting for period (fixed effect), will be used for the hypothesis test and to obtain the associated confidence interval. This will be supplemented with a risk difference obtained from a binomial model with identity link, random effects for centre and centre by period; and adjusting for period (fixed effect). The absolute numbers will be presented by trial arm. Mean eGFR values in each treatment group at one year will be compared using a normal regression model, adjusting for random cluster effect, random cluster by period interaction and a fixed effect for period. As eGFR at 12 months is only recorded for patients who are alive with a functioning graft at 12 months, the primary analysis will be complete case and there will be no imputation for missing values. The number of participants surviving to 12 months will be reported and of those the number who have a 12-month eGFR recorded. The adjusted mean and standard deviation eGFR at 12 months will be reported by treatment arm, alongside the adjusted treatment difference with 95% confidence interval and p-value. A sensitivity analysis, will repeat the analysis for the second primary outcome but with the following imputations: if a patient’s graft failed within 12 months, the eGFR at 12 months will be drawn from a normal distribution based on the mean value and standard deviation of patients on dialysis in the UK. If a patient died with a functioning graft within 12 months of transplant, the 12 month eGFR will drawn from a normal distribution based on the mean and standard deviation value at 12 months for all participants in the trial with a functioning transplant at one year and have a eGFR recorded. This method assumes that deaths with a functioning graft will occur at random given the observed data. Insufficient clinical data is collected at the 12-month time point to accurately impute any missing measurements and hence the imputation model does not include any other covariates. The methods used for the analysis of secondary outcomes in the form of proportions will be similar to that described for the first primary outcome. Similarly to the first primary outcome, in situations where a pair of kidneys are transplanted as a dual transplant into one recipient this will be counted as one transplant instead of two (in terms of utilisation; thus, not as effective as performing two single transplants, but better than discard).

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
32 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
The total number of kidney transplants and the number of single vs dual transplants will be presented overall and by treatment arm. Mean KDPI and CIT will be presented by treatment arm and a normal linear regression model (adjusting for period, a random effect for cluster and random interaction for period and cluster) will be used to test for any difference in treatment. Survival times and rates will be estimated using the Kaplan-Meier method and compared using a multivariate frailty model to account for clustering between centres. This model will also be adjusted for period. Findings will be reported as hazard ratios with 95% confidence intervals. As a consequence of that having two primary end-point measures, several different ‘positive’ trial outcomes are possible:
i) That the proportion of kidney offers from donors over 60 years old that are transplanted increases AND that the one-year eGFR for these transplants is greater.
ii) That the proportion of kidneys offers that are transplanted increases, but that the one year eGFR is unchanged.
iii) That the proportion of kidney offers that are transplanted is unchanged, but that the one year eGFR of the transplanted kidneys is greater.
We would view all three outcomes as confirming a benefit for the use of pre-implantation biopsy analysis. Outcome (iii) above, while positive, would likely lead to a re-evaluation of acceptance patterns for deceased donor kidney offers in the different UK kidney transplant centres, because it would possibly suggest that there is scope to further increase transplant numbers safely.
11.5.2 Other Analyses
Biopsy related complications will be tabulated overall and by treatment arm. For each of the 4 subgroup analysis, the primary outcome will be replicated for each subgroup separately. Although access to the urgent pathology service is immediate and is preceded by formal education, it is still possible that the response (change in behaviour towards older donors) may be more gradual. To monitor for this effect, a sensitivity analysis will be conducted which will exclude the first four weeks following crossover to the intervention arm, and replicate the primary outcomes, to observe whether this significantly alters our conclusions. This will coincide with further review with each centre in the second month after crossover; this review will present and discuss that centre’s response to offers and biopsy utilisation for the first four weeks after gaining access to the Histopathology Service.
11.5.3 Health Economic Analysis
A within-trial and decision model-based economic evaluation will be conducted from the perspective of the NHS comparing the national histopathology service versus treatment as usual (no biopsy service). The within trial analysis will estimate the cost of the histopathology service including capital investment (e.g. scanners), training for centres, staffing and transportation costs per centre, and cost of patient NHS contacts (e.g. dialysis, transplant surgery, or secondary care contact). Cost data will be extracted from trial records and the UKTR, held by NHSBT. The outcome will be the number of patients with a functioning transplant per centre at 12 months. The analysis will therefore report the incremental cost per incremental functioning kidney at 12 months.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
33 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
The within-trial timeframe of 12 months is insufficient to fully capture the differences in costs and outcomes between the study arms. Therefore, a decision-model based economic evaluation will combine cost and outcomes evidence from the trial with other relevant evidence from the literature. Full details of the model will be described in the economics analysis plan. The analysis will be conducted separately from the main statistical analysis.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
34 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
12. Ethical and Regulatory Issues
12.1 Compliance
This trial complies with the Declaration of Helsinki [2013]. It will also be conducted in compliance with the approved protocol, the principles of Good Clinical Practice (GCP), the UK Data Protection Act, the requirements of the Human Tissues Act and the UK Policy Framework for Health and Social Care Research.
12.1.1 Site Compliance
The site will comply with the above regulations and guidelines. An agreement and/or HRA Statement of Activities as appropriate will be in place between the site and the Sponsor, setting out respective roles and responsibilities. The site will inform the CTU as soon as they are aware of a possible serious breach of compliance, so the CTU can report the breach if necessary, within 7 days as per the UK regulatory requirements. For the purposes of this regulation, a serious breach is one that is likely to affect to a significant degree: ● The safety or physical or mental integrity of the subjects in the trial, or ● The scientific value of the trial.
12.1.2 Data Collection and retention
Trial documentation should be kept securely, and held for 30 years after the end of the trial. During this period, all data should be accessible to the competent authorities and the Sponsor with suitable notice.
12.1.3 Access to Data
Custody of the final data set will reside with the Chief Investigator and NHSBT CTU (for audit purposes). Access to the final data set for additional analyses will be permitted under the agreement of the Trial Steering Committee, according to the publication policy in section 16.
12.2 Ethical Conduct of the Study
12.2.1 Ethical Considerations
Before initiation of the trial, the protocol will be submitted to a Research Ethics Committee for ethical approval. Any subsequent amendments will be submitted to, and approved by, the same Research Ethics Committee.
12.2.2 Consent
All patients who are added to the national transplant waiting list consent for the use of their anonymised, routinely-collected data to be used for audit and research (see attached example consent form) in advance. In addition, each patient will provide consent for the specific kidney transplant they are offered, after discussion with the implanting team about the risks of the proposed transplant and their risks of waiting for another kidney offer (see BTS/NHSBT consent guidelines http://www.bts.org.uk/Documents/Consent%20Guidance%201%20April%202013.PDF). Part of the assessment of risk will be the biopsy score, where it is available. Clearly, if the biopsy is thought to be required on clinical grounds then it is likely to be taken at the time of retrieval, prior to

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
35 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
consultation with the recipient. Because consent for data collection is already mandatory for entry into the UK transplant waiting list, and because the trial endpoint data are already returned to NHSBT, individual patient consent for the study is not required. The PITHIA trial information sheet will be provided to each of the participating transplant centres, for the patients listed on their kidney transplant waiting list (to be provided at review appointments, for example). We will remain in regular contact with both national and local kidney patient groups. We view the involvement of the local kidney patient groups (attached to each of the transplant centres) as an integral component of the education package offered to each centre prior to receipt of the biopsy service. The consent of the transplant centres to take part in the study is implicit, given their support for the trial application and participation. This is in accord with the Ottawa consensus statement 40 on the ethics of cluster randomised trials.
12.3 Confidentiality
All study-related data will be sent from participating centres to the UKTR securely in accordance with usual practice. The histopathology results (Remuzzi scoring) will be forwarded in a pseudo-anonymised fashion to NHSBT CTU with organ donation registry identifiers only so they may be included in the trial data set. NHSBT CTU will not store any records which contain names or other personal identifiers.
12.4 Other approvals
Confirmation of capacity and capability must be received from the R&D department of each participating site, following REC and HRA approvals.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
36 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
13. Indemnity The NHS indemnity scheme applies to this trial when it is being conducted in the UK. Section 4 of the non-commercial clinical trial agreement 2008 describes the indemnity arrangements as follows: As both Sponsor and site are NHS bodies, i.e. NHS bodies/NHS Foundation Trusts in England, Wales or Northern Ireland and are indemnified by the same Indemnity Scheme (being one of the NHS Litigation Authority clinical negligence or the Welsh Risk Pool or the Clinical Negligence Fund in Northern Ireland) and the Party incurring any loss can recover such loss under one of the Indemnity Schemes, then such Party shall rely on the cover provided by the Indemnity Scheme and not seek to recover the Loss from the other Party(ies). Where the other Party(ies) caused or contributed to the Loss, it undertakes to notify the relevant Indemnity Scheme(s) to take this into account in determining the future levies of all Parties in respect of the indemnity schemes. If:
● The Parties are members of the same Indemnity Scheme in England, Wales or Northern Ireland and the Party incurring the Loss is not indemnified for that Loss by its Indemnity Schemes; or
● All Parties are NHS bodies in Scotland; or ● The Parties are NHS bodies/Foundation Trusts established in different jurisdictions within
the United Kingdom; Then the Parties shall apportion such Loss between themselves according to their respective responsibility for such Loss. Should the Parties be unable to agree the apportionment the matter shall be resolved in accordance with clause 16.5. If one or more Parties are NHS Foundation Trusts and the Party incurring the Loss is not responsible for all or part of the Loss and is not indemnified in respect of the Loss by one of the Indemnity Schemes then the Party incurring the Loss shall be entitled to recover the Loss from the other Party (ies) pursuant to the provisions of this Agreement. The Chief Investigator is an employee of the University of Cambridge, who have provided the following indemnity cover:
The University Insurance Office has advised that insurance for negligent and non-negligent harm can be arranged if this study is approved by the NHS Ethics committee. Cover is provided under the University's Clinical Trials and/or Human Volunteer Studies policy, the insurers are Newline, the insurance policy reference is B0823Q31000177 and the Limit of Indemnity under the policy is £10m.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
37 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
14. Finance
14.1 Funding
Funding arrangements will be provided in the Trust agreement with the Sponsor. 1. National Institute for Health Research: Research for Patient Benefit (RfPB) Programme (PB-PG-1215-20033). NIHR will provide financial support for staff salaries, direct/indirect research costs as well as dissemination costs. In addition, NIHR will provide access to their established research networks, research design services as well as other partners. 2. This trial has been funded primarily by award of the RfPB, but this does not cover excess treatment costs, most notably the cost of histopathology at the six national centres (Cambridge, Royal Free, Newcastle, Leeds, Birmingham and Edinburgh). Six digital pathology scanners are to be supplied for the duration of the trial, one for each designated centre. These scanners will be provided by Sysmex, with the cost to be met by Addenbrooke’s Charitable Trust and will include a service contract which will cover the duration of the trial.
14.2 Declaration of interests
The authors have no competing interests, financial or otherwise, to declare.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
38 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
15. Oversight and Trial Committees There are a number of committees involved with the oversight of the trial. These committees are detailed below.
15.1 Trial Management group (TMG)
A Trial Management Group (TMG) comprising the Chief Investigator, other lead investigators and members of the CTU. The TMG will be responsible for the day to day running and management of the trial. It will aim to convene monthly, either face to face or by teleconference. Members include, but are not limited to:
o Gavin Pettigrew (Chair) – CI, University of Cambridge o Dominic Summers - Academic Clinical Fellow and Registrar in Transplant Surgery,
Cambridge o Desley Neil – Consultant Histopathologist, University Hospital Birmingham o Karla Hemming – Senior Lecturer / Statistician, University of Birmingham o Alison Deary – Head of Operations, NHSBT CTU o Ana Mora – Clinical Operations Manager, NHSBT CTU o Emma Laing – Trial Manager, NHSBT CTU o Liz Armstrong – Head of Transplant Development, NHSBT o Laura Pankhurst – Trial Statistician, NHSBT
o John Ayorinde - Clinical Research Fellow (Organ Retrieval and Transplantation)
15.2 Trial Steering Committee
The Trial Steering Committee (TSC) has membership from the TMG and independent members, including the Chair. The role of the TSC is to provide overall supervision for the trial, and provide advice through its’ independent chair. The ultimate decision on continuation of the trial lies with the TSC and it will aim to convene twice a year. Members:
o Estee Torok (Chair) o Fiona Loud o Jasvir Parmar o Gavin Pettigrew o Richard Hooper o Rupert Pearse o Stuart Powell (Patient Representative) o Keith Pennington (Patient Representative) o Sponsor Representative o Laura Pankhurst (Trial Statistician) o Emma Laing (Facilitator)
15.3 Data Monitoring Committee
A Data Monitoring Committee chaired by an Independent Expert and including a further Independent Expert and Statistician will be appointed and will convene to discuss safety data pertaining to the six months leading up to that meeting. The full role and responsibility of the DMC will be documented and established before the trial starts and will be in accordance with current guidance from the Health Research Authority. The group can provide advice to the chair of the TSC

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
39 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
and can recommend premature closure of the trial to the TSC. The group will be expected to convene twice a year but may be assembled more urgently if thought necessary by the TMG.
15.4 Role of Study Sponsor
The Cambridge University Hospitals NHS Trust and Cambridge University had no role in the design of this study, and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results.
15.5 Role of Study Funder(s)
The NIHR had no role in the design of this study, and will not have any role during its execution, analyses, interpretation of the data, or decision to submit results. The funder will be notified prior to any publication arising from this trial.
16. Publication
16.1 Dissemination
The particular trial methodology was chosen to specifically address the question of whether introduction of a national histopathology service increases the number of kidney transplants performed. By involving all renal transplant units, it is expected that the proposed trial will automatically be a major research focus for transplantation in the UK, with analysis of the outcomes keenly awaited. Moreover we believe that, by providing a definitive answer to what is undoubtedly a key question in transplantation, the proposed trial has the potential to change international transplant practice. We therefore expect to present our findings to allied transplant professionals as oral presentations at several key transplant meetings held annually in the UK, Europe and the US (British Transplantation Society, European Society of Organ Transplantation and the American Transplant Congress). We are committed to publishing the results in peer review within three years after commencement of the trial, and anticipate that this will be in a top-line journal compliant with Open Access. Both NHS Blood and Transplant and Cambridge University Hospitals NHS Foundation Trust have dedicated Public Relations and Communications Teams, and we plan their involvement, such that publication will coincide with local and national press release. Volunteers from each of the renal patient groups attached to the various UK transplant centres will be supported in disseminating the trial results to the waiting list population at each centre. Because of the implications in the use of kidneys from ‘marginal’ or ‘higher-risk’ donors, we believe that the trial results will impact upon how patients are consented for kidney transplantation. We anticipate that the local kidney patient groups will be fully involved in drafting new consent forms for each unit that specifically address the risks and benefits associated with expanded criteria donors.
16.2 Authorship
Substantive contributions to the design, conduct, interpretation, and reporting of a clinical trial are recognised through the granting of authorship on the final trial report.
16.3 Approvals
Study results will be embargoed and not disseminated until authorised by the CI and TSC. Final manuscripts and presentations will be approved by the CI, Funder (NIHR) and TSC prior to publication.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
40 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
16.4 Identification
A trial identifier should be included on all presentations and publications (e.g. the ISCRTN).
16.5 Timing
It must be made clear that no data may be made public before publication and never without agreement from the CI and the NIHR.
16.6 Acknowledgements
For the main report of this study submitted for publication, together with associated methodology and health economic papers or posters/presentations, we will use the International Committee of Medical Journal Editors definitions of Authorship and Contributorship http://www.icmje.org/ethical_1author.html) The members of the TSC and DMC should be listed with their affiliations in the Acknowledgements/Appendix of the main publication and the support of the NHSBT Clinical Trials Unit, and Funder acknowledged in all publications/presentations.
17. Protocol Amendments Any substantial modifications to the protocol which may impact on the conduct of the study, affect patient safety, including changes of study objectives, study design, study procedures, study outcomes or significant administrative aspects will require a formal amendment to the protocol. Such amendment will be agreed upon by the TMG and TSC and approved by the REC and HRA prior to implementation and notified to the relevant UK transplant centres in accordance with local regulations.
Revision History:
Version Author Date Reason for revision
2.0 Gavin Pettigrew 16/09/2019 Changes to biopsy size. Minor revisions to ‘Statistical Considerations’ section (11). Extension to time window for the eGFR endpoint (10-15 months after transplant). Other minor administrative changes.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
41 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
18. Appendices
APPENDIX 1 - Remuzzi scoring (modified for use in the PITHIA trial)

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
42 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
43 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
44 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
APPENDIX 2 Transporting biopsy samples in the PITHIA trial
Cohort
Deceased kidney donors (DBD and DCD) aged 60 and over who donated in the UK between 1 April 2016 and 31 March 2017. A kidney donor is defined as someone who had a kidney retrieved for the intention of transplantation.
During this time period there were 461 kidney donors and of these 436 (95%) had at least 1 abdominal organ transplanted.
There are 6 biopsy centres and these are Edinburgh, Newcastle, Leeds, Birmingham, Cambridge and Royal Free.
All percentages are calculated using the total number of kidney donors who had at least 1 abdominal organ transplanted.
An ‘involved biopsy centre’ is one where either a retrieval team is based at a centre where there is a biopsy centre, or an abdominal organ is being transplanted at a centre which is a biopsy centre.
Notes and Limitations
- These figures do not capture organs from donors which did travel to transplant centre but were rejected and not used.

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
45 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
19. References
1. Israni, A. K. et al. New National Allocation Policy for Deceased Donor Kidneys in the United States and Possible Effect on Patient Outcomes. J. Am. Soc. Nephrol. 25, 1842–1848 (2014).
2. Tonelli, M. et al. Systematic review: kidney transplantation compared with dialysis in clinically relevant outcomes. Am. J. Transplant 11, 2093–2109 (2011).
3. Wolfe, R. A. et al. Comparison of Mortality in All Patients on Dialysis, Patients on Dialysis Awaiting Transplantation, and Recipients of a First Cadaveric Transplant. N. Engl. J. Med. 341, 1725–1730 (1999).
4. NHSBT. Annual Report on Kidney Transplantation. (2014). https://nhsbtdbe.blob.core.windows.net/umbraco-assets corp/1321/organ_specific_report_kidney_2014.pdf
5. Summers, D. M. et al. Kidney donation after circulatory death (DCD): state of the art. Kidney Int 88, 241–249 (2015).
6. Callaghan, C. J. et al. The discard of deceased donor kidneys in the UK. Clin Transpl. 28, 345–353 (2014).
7. Remuzzi, G. et al. Early experience with dual kidney transplantation in adults using expanded donor criteria. Double Kidney Transplant Group (DKG). J Am Soc Nephrol 10, 2591–2598 (1999).
8. Mirshekar-Syahkal, B. et al. Local Expansion of Donation After Circulatory Death Kidney Transplant Activity Improves Waitlisted Outcomes and Addresses Inequities of Access to Transplantation. Am. J. Transplant 17, 390–400 (2017).
9. Kosmoliaptsis, V. et al. Baseline Donor Chronic Renal Injury Confers the Same Transplant Survival Disadvantage for DCD and DBD Kidneys. Am. J. Transplant. 15, 754–763 (2015).
10. Mallon, D. H. et al. Successful Transplantation of Kidneys From Elderly Circulatory Death Donors by Using Microscopic and Macroscopic Characteristics to Guide Single or Dual Implantation. Am. J. Transplant. 15, 2931–2939 (2015).
11. Liapis, H. et al. Banff Histopathological Consensus Criteria for Preimplantation Kidney Biopsies. Am. J. Transplant 17, 140–150 (2017).

FORM FRM4894/1 Effective:30/04/15
CTU Protocol
46 PITHIA Protocol v2.0 16/09/2019
Cross-Referenced in Primary Document: MPD980
12. Hemming, K., Girling, A., Martin, J. & Bond, S. J. Stepped wedge cluster randomized trials are efficient and provide a method of evaluation without which some interventions would not be evaluated. J. Clin. Epidemiol. 66, 1058–1059 (2013).
13. Lauer, M. S. & D’Agostino, R. B. The Randomized Registry Trial — The Next Disruptive Technology in Clinical Research? N. Engl. J. Med. 369, 1579–1581 (2013).
14. Levey, A, Greene, T, Kusek, J, and Beck, G. A simplified equation to predict glomerular filtration rate from serum creatinine. J Am Soc Nephrol. 2000; 11: A0828 ((abstr)).
15. Bago-Horvath, Z. et al. The cutting (w)edgecomparative evaluation of renal baseline biopsies obtained by two different methods. Nephrol. Dial. Transplant. 27, 3241–3248 (2012).
16. Martin, J. Advancing knowledge in stepped-wedge cluster randomised trials. Univ. Birmingham, Unpubl. Dr. thesis (2017).
17. Hooper, R., Teerenstra, S., de Hoop, E. & Eldridge, S. Sample size calculation for stepped wedge and other longitudinal cluster randomised trials. Stat. Med. 35, 4718–4728 (2016).
18. Hooper, R. & Bourke, L. Cluster randomised trials with repeated cross-sections: some alternatives to parallel group designs Cluster randomised trials with repeated cross sections: alternatives to parallel group designs. BMJ 350, (2015).
19. O’Brien, P. C. & Fleming, T. R. A multiple testing procedure for clinical trials. Biometrics 35, 549–56 (1979).
20. Chan, A.-W. et al. SPIRIT 2013 Statement: Defining Standard Protocol Items for Clinical Trials. Ann. Intern. Med. 158, 200 (2013).