Embed Size (px)
Citation preview

Upper GI Histopathology Update
Dr David CundellST4 Histopathology, BRI

Acknowledgement
Dr Newton Wong, Consultant Histopathologist at BRI and regional network lead for Upper GI Histopathology.

Outline• Specimens & request forms

Outline• Specimens & request forms
• Staging

Outline• Specimens & request forms
• Staging
• Molecular biology / personalised medicine

Outline• Specimens & request forms
• Staging
• Molecular biology / personalised medicine
• Carter report – future of path services

•Specimens
– Please resist any temptation to open surgical specimens. Slicing through tumours can compromise accurate staging assessment
– Pathologist should be left to open them after inking any non-peritonealised CRM

• Clinical information for the request form useful at the time of cut up
–Previous investigation findings
–Operation undertaken, not just the name of the organ removed
–Any margin that may be at particular risk
–Significant co-existant pathology – does patient have another malignancy?
–Treatment – has patient been given chemo/radiotherapy? Including the use of any monoclonal antibody therapy

•Staging
– Anatomical definitions in oesophageal anatomy
– Junctional neoplasms
– TNM 7 update for oesophagus and stomach cancer

• Cervical Oesophagus:
– From the lower border of the cricoid cartilage to the thoracic inlet, about 18 cm from the incisors.

•Intrathoracic (including abdominal oesophagus):
– Upper thoracic portion: From the thoracic inlet to the level of the tracheal bifurcation (18-24 cm).
– Mid-thoracic portion: From the tracheal bifurcation midway to the gastroesophageal (GE) junction (24-32 cm).
– Lower thoracic portion: From midway between the tracheal bifurcation and the gastroesophageal junction to the GE junction, including the abdominal esophagus between 32-40 cm.

Classification of Gastroesophageal Junction
Adenocarcinoma, Siewert I-III
•Type I: tumour of distal oesophagus, infiltrates the oesophagogastric junction from above
•Type II: true carcinoma of the cardia arising immediately at the oesophagogastric junction
•Type III: subcardial gastric carcinoma that infiltrates the oesophagogastric junction and distal oesophagus from below.
Siewart JR et al. “Adenocarcinoma of the Esophagogastric Junction: Results of Surgical Therapy Based on Anatomical/Topographic Classification in 1,002 Consecutive Patients.” Ann Surg. 2000 September; 232(3): 353–361.

TNM 6 to 7
• Tumours of gastric cardia / OGJ to be harmonised with distal oesophagus as bulky tumours at diagnosis that straddled the junction introduced different stage groupings depending on designation
• Simplify T categories across the tubular GIT to aid conceptualisation
• Gastric carcinoma may have LN metastases when still confined to lamina propria due to abundant lymphatics in gastric mucosa (cf. colorectal)
ReferenceWashington, K. 7th Edition of the AJCC Cancer Staging Manual: Stomach. Ann Surg Oncol (2010) 17:3077-3079

TNM 7
Oesophagus

TNM 7 changes
Tumors arising at the OGJ, or in the cardia of the stomach within 5 cm of the OGJ and cross the OGJ, are staged using the TNM system for oesophageal rather than stomach cancer.

TNM 7 changes
Tumors arising at the OGJ, or in the cardia of the stomach within 5 cm of the OGJ and cross the OGJ, are staged using the TNM system for oesophageal rather than stomach cancer.
All other cancers with a midpoint in the stomach lying more than 5 cm distal to the OGJ, or those within 5 cm of the OGJ but not extending into the OGJ or esophagus, are staged using the stomach TNM

TNM 7 Oesophageal
Cancer
Depth of invasion pT Stage
In situ, intraepithelial, noninvasive; high grade dysplasia
Tis
Invasive tumor confined to mucosa (LP, MM)
T1a
Invades submucosa T1b
Muscularis propria invaded T2
Adventitia and/or soft tissue invaded
T3
At serosal surface T4a
Invades adjacent organ T4b

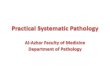
Layers of the oesophageal wall

TNM 7 Oesophagus - validated through retrospective re-staging
Reid TD, Sanyaolu LN, Chan D, Williams GT, Lewis WG. Relative prognostic value of TNM7 vs TNM6 in staging oesophageal cancer. Br J Cancer 2011 Sep 6;105(6):842-6. Department of Surgery, South East Wales Cancer Network, University Hospital of Wales, Cardiff, UK. (n=200)
Zhonghua Zhong Liu Za Zhi. 2012 Jun;34(6):461-4. Preliminary experience of clinical applications of the 7th UICC-AJCC TNM staging system of esophageal carcinoma. Lu et al. Source Department of Thoracic Surgical Oncology, Cancer Hospital (Institute), Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing 100021, China. (n=1397)
Both studies drew the conclusion that TNM7 provides superior prognostic information.

TNM 7
Stomach

TNM 7: Tumour changes, stomach
Tis Intraepithelial tumor without invasion of the lamina propria (including high grade dysplasia)
T1a Tumor invades lamina propria or muscularis mucosae
T1b Tumor invades submucosa
T2 Tumor invades the muscularis propria (NB. previously pT2a was MP invasion & pT2b subserosal invasion)
T3 Tumor penetrates the subserosa (NB. Previously pT3 included serosal invasion)
T4a Tumor invades serosa
T4b Tumor invades adjacent stuctures

TNM 7: Tumour changes, stomach
Incidence of nodal metastasis is a good predictor of prognosis justifying new subclassification of pT1
(NB. Previously pT1 encompassed invasion of LP, MM & SM)
Tis Intraepithelial tumor without invasion of the lamina propria (including high grade dysplasia)
T1a Tumor invades lamina propria or muscularis mucosae
T1b Tumor invades submucosa
T2 Tumor invades the muscularis propria (NB. previously pT2a was MP invasion & pT2b subserosal invasion)
T3 Tumor penetrates the subserosa (NB. Previously pT3 included serosal invasion)
T4a Tumor invades serosa
T4b Tumor invades adjacent stuctures

TNM 7: Tumour changes, stomach
Tis Intraepithelial tumor without invasion of the lamina propria (including high grade dysplasia)
T1a Tumor invades lamina propria or muscularis mucosae
T1b Tumor invades submucosa
T2 Tumor invades the muscularis propria (NB. previously pT2a was MP invasion & pT2b subserosal invasion)
T3 Tumor penetrates the subserosa (NB. Previously pT3 included serosal invasion)
T4a Tumor invades serosa
T4b Tumor invades adjacent stucturesA. Marchet et al. Validation of the new AJCC TNM staging system for gastric cancer in a large cohort of patients (n=2,155): focus on the T category European Journal of Surgical Oncology 2011. (T2/3 cases n=686). Retrospective review of 686 patients previously classified as having T2 tumors, using new TNM staging > T2 and T3 disease were 270 (39.4%) and 416 (60.6%), respectively. After a median follow-up of 55 months, the 5-year overall survival rates were 67.3% and 52.3% for patients with T2 and T3 tumors, respectively (P<0.001). Prognostic difference significant

TNM 7: Node changes, stomach
Nx Regional LN cannot be assessed
N0 No regional LN mets
N1 Mets in 1-2 regional LN (pN1 previously 1-6)
N2 Mets in 3-6 regional LN (pN2 previously 7-15)
N3a Mets in 7-15 regional LN (pN3 previously > 15)
N3b Mets in ≥ 16 regional LN

TNM7: Metastasis changes, stomach
Mx - deleted
Clinical M staging until biopsy proven metastasis
M0 = No distant mets
M1 = Distant mets:• Positive peritoneal cytology• Non regional or distant LN• Peritoneal surfaces• Other organs
Therefore only pM1 exists, used following tissue diagnosis of distant metastasis or positiveperitoneal cytology

Outline
• Molecular pathology / personalised medicine
– Her-2 analysis in gastric cancers
– Mutational analysis in GISTs
– NICE: K-RAS analysis re: cetuximab for liver metastases

Molecular pathology – All carried out locally
•HER-2 testing for gastric adenocarcinomas
•Mutational analysis for gastrointestinal stromal tumours (GISTs)
•K-Ras analysis– As cetuximab can be prescribed for some patients with
wild type K-Ras liver metastases from colorectal adenocarcinoma.

HER2 (Human Epidermal Growth Factor Receptor 2, Neu, ErbB-2)
A protein encoded by ERBB2 gene on chromosome 17q12
NB. ‘HER’2 similar structure to human epidermal growth factor receptor. ‘Neu’ derived from a rodent glioblastoma neural tumor. ‘ErbB’-2 similarity to protein product of avian erythroblastosis oncogene B. Gene cloning showed that HER2, Neu, and ErbB-2 proteins are all encoded by the same gene.
Amplification of ERBB2 linked to pathogenesis & progression of certain aggressive types of breast cancer but also gastric cancer
References
Xie SD et al. HER 2/neu protein expression in gastric cancer is associated with poor survival. Mol Med Rep. 2009;2(6):943-6. Forty-one out of 218 (18.8%) gastric cancer specimens showed HER 2/neu-positive expression. In multivariate analysis, HER 2/neu expression was a significant independent prognostic predictor of gastric cancer (p<0.001), and was associated with poor survival in gastric cancer patients.
Park DI et. HER-2/neu amplification is an independent prognostic factor in gastric cancer. Dig Dis Sci 2006 Aug;51(8):1371-9. Epub 2006 Jul 26. Twenty-nine (15.9%) of 182 patients expressed the HER-2/neu protein by immunohistochemistry. Tumors with HER-2/neu amplification were associated with poor mean survival rates (922 vs 3243 days) and 5-year survival rates (21.4% vs 63.0%; P < 0.05).
2008 Gastrointestinal Cancers Symposium: overall HER2 expression (IHC 3+ and/or FISH +) of 22% in 2168 patients tested and confirmed a higher rate of HER2 positivity in GEJ tumors than in gastric cancer samples (34% vs 20%).

EGFRs have plasma membrane-bound receptor tyrosine kinases.
– extracellular ligand binding domain, transmembrane domain, intracellular domain > second messenger signalling
HER2 heterodimerisation > autophosphorylation of tyrosine residues within the cytoplasmic domain of the receptors
Initiates a variety of signalling pathways– promotes cell proliferation– opposes apoptosis
NICE guidance Nov 2010:Herceptin / Trastuzumab as part of combination chemotherapy for patients with metastatic gastric or junctional carcinomas that overexpress HER2
Analyse either:– The amount of HER2 protein that has been translated (IHC)– Examine the nucleus to see if there is amplification of the gene (ISH)
ReferenceBartlett et al. HER2 testing in the UK: recommendations for breast and gastric in-situ hybridisation methods J Clin Pathol
2011;64:649e653. doi:10.1136/jcp.2011.089847

GIST
Most (50-80%) GISTs arise because of a mutation in c-kit, a gene encoding a receptor for a growth factor called stem cell factor (CD117)
Mutation of gene > activation of the KIT receptor tyrosine kinase > downstream phosphorylation in the signal transduction pathway > increased cellular proliferation.
In a minority of cases, GISTs result from mutational activation of the closely related tyrosine kinase PDGF receptor a (PDGFRA).
Molecular analysis involves assessment of:KIT exons 9 and 11, 13 & 17PDGFRA exons 12 and 18
The tyrosine kinase inhibitor imatinib / Glivec represents a major breakthrough in the treatment of GISTs, which are generally resistant to cytotoxic chemotherapy.
Additional cytogenetics:
Low risk: noncomplex or even normal karyotypes, with deletion of chromosome 14 often being the only observable cytogenetic aberration.Moderate-risk: as for low risk plus deletions of chromosomes 1p, 9p, 11p, or 22qMalignant: above plus amplification of 8q and 17q
Fresh tissue best for analysis

KRAS‘Kirsten rat sarcoma’ protein encoded by KRAS gene. KRAS protein is a GTPase tethered to cell membranes. Involved in signal transduction pathways, acting as a molecular on/off switch.
A single amino acid substitution, and in particular a single nucleotide substitution, is responsible for an activating mutation. The transforming protein that results is implicated in various malignancies, including colorectal carcinoma
KRAS mutation is predictive of a very poor response to cetuximab therapy in colorectal cancer (40% cases), as the mAb targets the EGFR upstream of the mutant protein. NICE: Cetuximab in combination chemotherapy is recommended for the first-line treatment of metastatic colorectal cancer only when all of the following criteria are met:
The primary colorectal tumour has been resected or is potentially operable.
The metastatic disease is confined to the liver and is unresectable.
The patient is fit enough to undergo surgery to resect the primary colorectal tumour and/or to undergo liver surgery if the metastases become resectable after treatment
ReferenceLeivre,A et al. KRAS Mutation Status Is Predictive of Response to Cetuximab Therapy in Colorectal Cancer Cancer Res 2006;66: (8). April 15, 2006

Outline• Specimens & request forms
• Staging
• Molecular biology / personalised medicine
• Carter report – future of path services

Consequences of the Carter report ‘Modernisation of Pathology Services’ published in December 2008
• Recommendations on the centralisation of service provision into networks– Satellite centres provide frozen section / MDT cover– Logistical problems with specimen handling – eg. the opening of
specimens for adequate fixation to prevent autolysis– Histopath costs are staff heavy but grouped with blood sciences,
inappropriate as different pattern of work less automation
• Changes underway in this region– Southmead, UHB & Weston may merge at NBT
http://www.pathologists.org.uk/publications-page/Carter%20Report-The%20Report.pdf

Thank you