Embed Size (px)
Citation preview
www.elsevier.com/locate/ygyno
Gynecologic Oncology
Predictors of vaginal relapse in stage I endometrial canceri
Andrea Mariania, Sean C. Dowdya, Gary L. Keeneyb, Michael G. Haddockc,
Timothy G. Lesnickd, Karl C. Podratza,*
aSection of Gynecologic Surgery, Mayo Clinic, 200 First Street SW, Rochester, MN 55905, USAbDivision of Anatomic Pathology, Mayo Clinic, Rochester, MN 55905, USAcDivision of Radiation Oncology, Mayo Clinic, Rochester, MN 55905, USA
dDivision of Biostatistics, Mayo Clinic, Rochester, MN 55905, USA
Received 5 November 2004
Available online 13 May 2005
Abstract
Objective. To identify factors predictive of vaginal relapse in stage I endometrial cancer, thereby potentially facilitating the selection of
patients who may benefit from vaginal brachytherapy.
Methods. The study population included 632 patients with stage I endometrial cancer managed with hysterectomy at our institution
between 1984 and 1996. Median follow-up was 73 months; 122 patients (19%) received adjuvant radiotherapy.
Results. Overall, 2.9% of the stage I cohort developed vaginal relapse at 5 years. Vaginal relapse was observed in 1.7% of patients
who received radiotherapy and in 3.0% of those whose treatment did not include radiotherapy (P = 0.36). Cox regression analysis
(including radiotherapy) identified only grade 3 differentiation (hazard ratio = 3.83, P = 0.007) as an independent predictor of vaginal
relapse. Patients with a low-grade tumor had a 5-year vaginal relapse rate of 2%, compared with 7% for those with a grade 3 tumor. When
only patients who did not receive adjuvant radiotherapy were considered, both grade 3 tumor and lymphovascular invasion were
significant predictors of vaginal relapse (P < 0.05). When neither variable was present, 2% of patients experienced vaginal relapse at 5
years, compared with 11% when either 1 was present (P < 0.001). Depth of myometrial invasion was not a significant predictor of vaginal
recurrence.
Conclusion. Histologic grade 3 tumor and lymphovascular invasion were the cogent predictors of vaginal relapse in our population. The
cost and morbidity of vaginal brachytherapy should be balanced against the potential risk of vaginal relapse in this group of patients.
D 2005 Elsevier Inc. All rights reserved.
Keywords: Endometrial cancer; Vaginal relapse; Lymphovascular invasion
Introduction
Endometrial cancer is the most common malignancy of
the female reproductive tract in the United States and is
exceeded annually in overall frequency only by cancers of
the breast, colon, and lung. It has been estimated that
0090-8258/$ - see front matter D 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.ygyno.2005.03.008
Abbreviations: FIGO, Federation of International Gynecology and
Obstetrics; LVI, lymphovascular invasion.i Presented at the 34th Annual Meeting of the Society of Gynecologic
Oncologists (SGO),NewOrleans, Louisiana, January 31 to February 4, 2003.
* Corresponding author.
E-mail address: [email protected] (K.C. Podratz).
during calendar year 2005, 40,880 new cases of endome-
trial cancer will be diagnosed and 7310 deaths will occur
[1].
Vaginal relapse is a relatively common pattern of
treatment failure for patients with endometrial cancer
[2] and can be effectively prevented by the adminis-
tration of vaginal brachytherapy [3]. Although more than
60% of isolated vaginal relapses occurring in patients
with stage I disease are treated successfully at the time
of recurrence [4,5], treatment-associated morbidity is
significant.
Traditional predictors of vaginal relapse have included
the presence of deep myometrial invasion and poor tumor
97 (2005) 820 – 827

A. Mariani et al. / Gynecologic Oncology 97 (2005) 820–827 821
differentiation [3]. Recently, lymphovascular invasion (LVI)
has been identified as a predictor of vaginal relapse in
patients with highly differentiated stage I endometrial cancer
with minimal myometrial invasion [6]. The identification of
patients at risk for vaginal relapse is especially important in
stage I endometrial cancer, for which locoregional therapy
(i.e., surgery and vaginal brachytherapy) may possibly be
the only treatment needed to achieve complete cure of the
disease [7]. Assessing the natural history of occult local
extension may suggest ways to successfully decrease
recurrence rates with locoregional therapy.
The objective of the present analysis was to identify
factors predictive of vaginal relapse in stage I endometrial
cancer, thereby potentially facilitating the selection of
patients who may benefit from vaginal brachytherapy.
Patients and methods
From 1984 to 1996, 1109 patients with endometrial
cancer were managed surgically at Mayo Clinic (Rochester,
Minnesota). Based on data from the medical records, 632
patients with epithelial endometrial cancer met the follow-
ing inclusion criteria: (1) treatment included hysterectomy
and removal of existing adnexal structures, (2) the disease
was stage I, and (3) no other malignancy was diagnosed
within 5 years before or after the diagnosis of endometrial
cancer (except for carcinoma in situ or skin cancer other
than melanoma).
Staging was defined according to the International
Federation of Gynecology and Obstetrics (FIGO) surgical
staging system [8]. For patients who received treatment
before 1988, stage was determined retrospectively on the
basis of the surgical and pathologic assessments. Histologic
classification was according to the World Health Organ-
ization classification [9]. Architectural grading was based on
the degree of glandular differentiation in accordance with
the FIGO guidelines [8]. LVI was considered present when
tumor cells were within or attached to the wall of a
capillary-like space. Tumor diameter was assessed as
previously reported [10].
All hematoxylin–eosin-stained slides of the tumor were
reviewed retrospectively by one of us (G.L.K.) to confirm
the original diagnosis of adenocarcinoma and to determine
FIGO grade, histologic subtype, and LVI.
All surgical procedures were the responsibility of a
gynecologic oncologist. Hysterectomy was generally per-
formed via the abdominal route. During the 13-year period,
several of the surgeons routinely used a modified radical
(type II) hysterectomy for the treatment of endometrial
cancer. The decision to perform a simple hysterectomy or a
wide extrafascial (with unroofing of the ureters) hysterec-
tomy usually depended on the personal preference of the
gynecologic surgeon rather than on histologic or clinical
variables. Several patients underwent vaginal hysterectomy,
followed by laparotomy for surgical staging (when indi-
cated), after the diagnosis of endometrial cancer was made
by means of frozen-section analysis. Selected patients with a
preoperative diagnosis of suspected cervical invasion under-
went radical (type III) hysterectomies. Lymphadenectomy
usually was performed only in patients considered by the
surgeon to be at risk for lymph node metastasis, according
to the histologic grade of the tumor and depth of myometrial
invasion as determined by an intraoperative analysis of
frozen tissue sections.
Postoperative adjuvant radiotherapy consisted of external
beam pelvic radiation or vaginal brachytherapy or both. The
decision to deliver adjuvant radiotherapy depended pre-
dominantly on the assessment by gynecologic oncologists
and radiation oncologists of the risks of local or regional (or
both) recurrence after pathologic evaluation of the surgical
specimen. This decision usually was dictated by the
presence of grade 3 differentiation, nonendometrioid histo-
logic subtype, or deep myometrial invasion, or a combina-
tion of these pathologic features.
If sufficient follow-up information about survival and
recurrence was not available in the clinical records, death
certificates were obtained and letters were sent or telephone
calls were made to patients and family physicians to obtain
the information.
‘‘Vaginal relapse’’ was defined as disease relapse on or
within the vaginal walls or cuff, generally detected by
physical examination or vaginal cytology and confirmed
histologically. Usually, at the time of recurrence, imaging
studies of the chest and/or abdomen and/or pelvis were
obtained to identify possible concomitant pelvic or distant
sites of recurrence. For the purpose of the present analysis,
we considered only the first site (or concomitant sites) of
detected primary recurrence.
For statistical purposes, endometrioid tumors, endome-
trioid tumors with squamous differentiation, and adenosqu-
amous tumors were considered together. Grades 1 and 2
tumors were combined and compared with grade 3 tumors.
The cutoff for tumor diameter was chosen as 2 cm on the
basis of our previous experience [10].
Statistical analysis was performed with the Fisher exact
test and v2 analysis to test for relations between pairs of
categorical variables. The Kaplan–Meier method and log-
rank test were used for time-to-event analyses, with
recurrence as the end point. Differences were considered
statistically significant at P < 0.05. SAS System 8.2
statistical software and JMP statistical program (version
4.0.4, SAS Institute, Inc., Cary, North Carolina) were used
for the analysis.
Results
Descriptive statistics
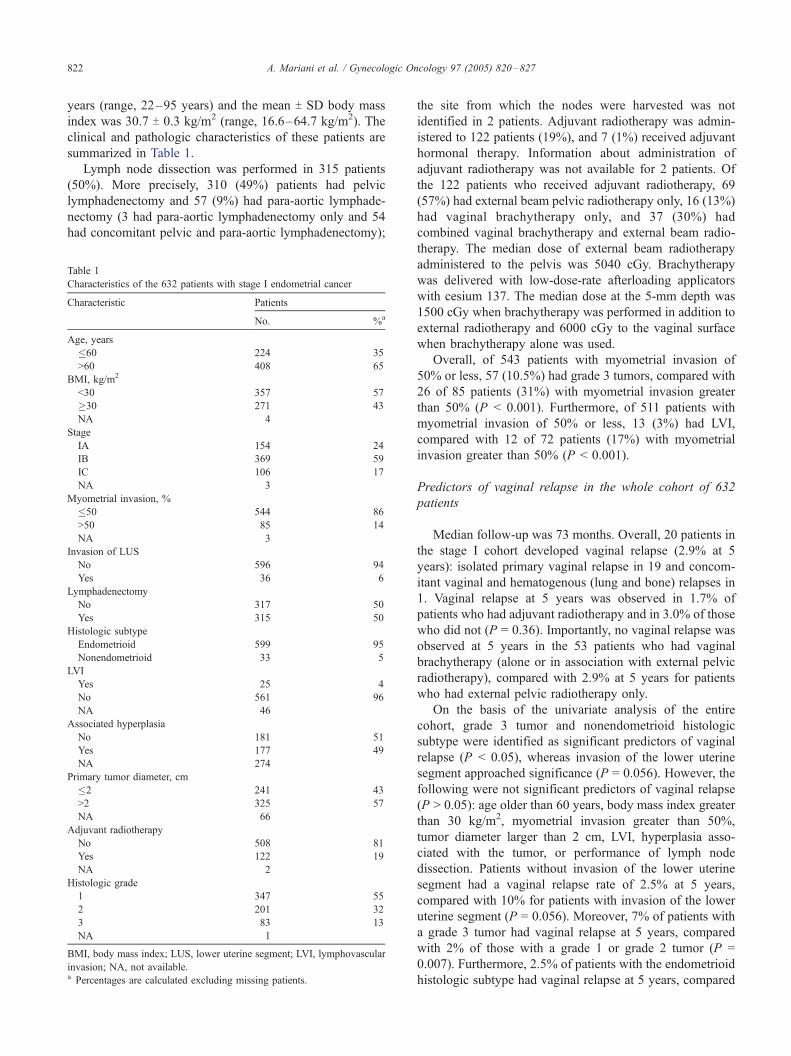
For the population of 632 patients with stage I
endometrial cancer, the mean age T SD was 64.5 T 11.0
A. Mariani et al. / Gynecologic Oncology 97 (2005) 820–827822
years (range, 22–95 years) and the mean T SD body mass
index was 30.7 T 0.3 kg/m2 (range, 16.6–64.7 kg/m2). The
clinical and pathologic characteristics of these patients are
summarized in Table 1.
Lymph node dissection was performed in 315 patients
(50%). More precisely, 310 (49%) patients had pelvic
lymphadenectomy and 57 (9%) had para-aortic lymphade-
nectomy (3 had para-aortic lymphadenectomy only and 54
had concomitant pelvic and para-aortic lymphadenectomy);
Table 1
Characteristics of the 632 patients with stage I endometrial cancer
Characteristic Patients
No. %a
Age, years
�60 224 35
>60 408 65
BMI, kg/m2
<30 357 57
�30 271 43
NA 4
Stage
IA 154 24
IB 369 59
IC 106 17
NA 3
Myometrial invasion, %
�50 544 86
>50 85 14
NA 3
Invasion of LUS
No 596 94
Yes 36 6
Lymphadenectomy
No 317 50
Yes 315 50
Histologic subtype
Endometrioid 599 95
Nonendometrioid 33 5
LVI
Yes 25 4
No 561 96
NA 46
Associated hyperplasia
No 181 51
Yes 177 49
NA 274
Primary tumor diameter, cm
�2 241 43
>2 325 57
NA 66
Adjuvant radiotherapy
No 508 81
Yes 122 19
NA 2
Histologic grade
1 347 55
2 201 32
3 83 13
NA 1
BMI, body mass index; LUS, lower uterine segment; LVI, lymphovascular
invasion; NA, not available.a Percentages are calculated excluding missing patients.
the site from which the nodes were harvested was not
identified in 2 patients. Adjuvant radiotherapy was admin-
istered to 122 patients (19%), and 7 (1%) received adjuvant
hormonal therapy. Information about administration of
adjuvant radiotherapy was not available for 2 patients. Of
the 122 patients who received adjuvant radiotherapy, 69
(57%) had external beam pelvic radiotherapy only, 16 (13%)
had vaginal brachytherapy only, and 37 (30%) had
combined vaginal brachytherapy and external beam radio-
therapy. The median dose of external beam radiotherapy
administered to the pelvis was 5040 cGy. Brachytherapy
was delivered with low-dose-rate afterloading applicators
with cesium 137. The median dose at the 5-mm depth was
1500 cGy when brachytherapy was performed in addition to
external radiotherapy and 6000 cGy to the vaginal surface
when brachytherapy alone was used.
Overall, of 543 patients with myometrial invasion of
50% or less, 57 (10.5%) had grade 3 tumors, compared with
26 of 85 patients (31%) with myometrial invasion greater
than 50% (P < 0.001). Furthermore, of 511 patients with
myometrial invasion of 50% or less, 13 (3%) had LVI,
compared with 12 of 72 patients (17%) with myometrial
invasion greater than 50% (P < 0.001).
Predictors of vaginal relapse in the whole cohort of 632
patients
Median follow-up was 73 months. Overall, 20 patients in
the stage I cohort developed vaginal relapse (2.9% at 5
years): isolated primary vaginal relapse in 19 and concom-
itant vaginal and hematogenous (lung and bone) relapses in
1. Vaginal relapse at 5 years was observed in 1.7% of
patients who had adjuvant radiotherapy and in 3.0% of those
who did not (P = 0.36). Importantly, no vaginal relapse was
observed at 5 years in the 53 patients who had vaginal
brachytherapy (alone or in association with external pelvic
radiotherapy), compared with 2.9% at 5 years for patients
who had external pelvic radiotherapy only.
On the basis of the univariate analysis of the entire
cohort, grade 3 tumor and nonendometrioid histologic
subtype were identified as significant predictors of vaginal
relapse (P < 0.05), whereas invasion of the lower uterine
segment approached significance (P = 0.056). However, the
following were not significant predictors of vaginal relapse
(P > 0.05): age older than 60 years, body mass index greater
than 30 kg/m2, myometrial invasion greater than 50%,
tumor diameter larger than 2 cm, LVI, hyperplasia asso-
ciated with the tumor, or performance of lymph node
dissection. Patients without invasion of the lower uterine
segment had a vaginal relapse rate of 2.5% at 5 years,
compared with 10% for patients with invasion of the lower
uterine segment (P = 0.056). Moreover, 7% of patients with
a grade 3 tumor had vaginal relapse at 5 years, compared
with 2% of those with a grade 1 or grade 2 tumor (P =
0.007). Furthermore, 2.5% of patients with the endometrioid
histologic subtype had vaginal relapse at 5 years, compared

Fig. 1. Adjuvant radiotherapy for stage I endometrioid endometrial cancer.
The histogram shows the percentage of patients who had adjuvant
radiotherapy according to substage (stage IA–IB vs. IC), presence of
lymphovascular invasion (LVI), and histologic grade (G1–2 vs. G3). The
administration of adjuvant radiotherapy to patients with stage IA or IB
disease was directed by the presence of a grade 3 (G3) tumor. Note that only
patients with endometrioid tumor were considered. For 3 patients, no
information was available on the depth of myometrial invasion or histologic
grade. For 2 patients, no information was available about the administration
A. Mariani et al. / Gynecologic Oncology 97 (2005) 820–827 823
with 9% of patients with nonendometrioid histologic
subtype (P = 0.03). However, Cox regression analysis
(including adjuvant radiotherapy) identified only grade 3
differentiation (P = 0.007; hazard ratio [HR] = 3.83; 95%
confidence interval [CI], 1.435–10.22) as an independent
predictor of vaginal relapse. When performance of lymph
node dissection was added to the Cox regression analysis,
grade 3 differentiation was still the only independent
predictor of vaginal recurrence.
As expected, patients with high-risk features, such as
deep myometrial invasion, nonendometrioid histologic
subtype, LVI, no hyperplasia associated with the tumor,
primary tumor diameter larger than 2 cm, or grade 3
differentiation, were significantly more likely to receive
adjuvant radiotherapy (Table 2, Fig. 1).
Predictors of vaginal relapse in patients who did not receive
adjuvant radiotherapy
If only the 508 patients who did not receive adjuvant
radiotherapy are considered, both grade 3 differentiation and
Table 2
Percentage of patients receiving radiotherapy according to clinicopatho-
logic risk factor
Characteristic Radiotherapy,a % of patients P
Age, years 0.25
�60 17
>60 21
BMI, kg/m2 0.48
<30 20
�30 18
Stage <0.001
IA 2
IB 14
IC 66
Myometrial invasion, % <0.001
�50 12
>50 69
Invasion of LUS 0.1
No 19
Yes 31
Histologic subtype 0.02
Endometrioid 18
Nonendometrioid 36
LVI 0.01
Yes 40
No 17
Associated hyperplasia <0.001
No 27
Yes 10
Primary tumor diameter, cm <0.001
�2 5
>2 29
Histologic grade <0.001
1 7
2 31
3 44
BMI, body mass index; LUS, lower uterine segment; LVI, lymphovascular
invasion.a Information about adjuvant radiotherapy was not available for 2 patients.
of adjuvant radiotherapy.
LVI were significant predictors of vaginal relapse (P <
0.05), and nonendometrioid histologic subtype approached
significance (P = 0.08). However, the following were not
significant predictors of vaginal relapse (P > 0.05): age
older than 60 years, body mass index greater than 30 kg/m2,
invasion of the lower uterine segment, myometrial invasion
greater than 50%, tumor diameter larger than 2 cm,
hyperplasia associated with the tumor, and performance of
lymph node dissection. Results are summarized in Table 3.
Specifically, 2% of patients with a grade 1 or grade 2 tumor
had vaginal relapse at 5 years, compared with 11% of those
with a grade 3 tumor (P < 0.001). Of note, there was no
significant difference in the 5-year rate of vaginal relapse
between patients with a grade 1 tumor (2.2% rate) and those
with a grade 2 tumor (1.5% rate). Moreover, 3% of patients
with the endometrioid histologic subtype had vaginal
relapse at 5 years, compared with 10% of those with a
nonendometrioid histologic subtype (P = 0.08). Further-
more, 7% of patients with LVI had vaginal relapse at 5
years, compared with 3% of those without LVI (P = 0.02)
(Table 3). Cox regression analysis identified only grade 3
differentiation (P = 0.004; HR = 5.45; 95% CI, 1.70–17.48)
and LVI (P = 0.01; HR = 6.94; 95% CI, 1.55–31.03) as
independent predictors of vaginal relapse. When neither of
these 2 variables was present, 2% of patients experienced
vaginal relapse at 5 years, compared with 11% when either
variable was present (P < 0.001). Of the 2 patients who did
not have adjuvant radiotherapy but in whom both variables
were present, 1 had vaginal relapse 63 months after
diagnosis and the other 1 was alive with no evidence of
disease after 91 months of follow-up (Table 4). Again, when
performance of lymph node dissection was added to the Cox
regression model, grade 3 differentiation and LVI retained

Table 3
Percentage of vaginal recurrences at 5 years according to clinicopathologic
risk factor in the 508 patients who did not receive adjuvant radiotherapy
Characteristic Vaginal recurrence at 5 years, % P
Age, years 0.90
�60 3
>60 3
BMI, kg/m2 0.39
<30 4
�30 2
Myometrial invasion, % 0.39
�50 3
>50 0
Invasion of LUS 0.19
No 3
Yes 10
Histologic subtype 0.08
Endometrioid 3
Nonendometrioid 10
LVI 0.02
Yes 7
No 3
Associated hyperplasia 0.96
No 2
Yes 3
Primary tumor diameter, cm 0.63
�2 4
>2 3
Histologic grade <0.001
1–2 2
3 11
Lymph node dissection 0.66
Yes 3
No 3
BMI, body mass index; LUS, lower uterine segment; LVI, lymphovascular
invasion.
Table 4
Vaginal recurrence rates according to risk factorsa in 508 patients with stage
I endometrial cancer who did not receive adjuvant radiotherapy
Risk factora No. of patientsb 5-Year failure rate, %
None 448 2
Either one 57 11
Both 2 -
a Histologic grade 3 or lymphovascular invasion or both.b Neither histologic grade nor information about lymphovascular invasion
was available for 1 patient.- Of the 2 patients, 1 had vaginal relapse 63 months after primary surgery.
A. Mariani et al. / Gynecologic Oncology 97 (2005) 820–827824
their status as the only independent predictors of vaginal
relapse.
Of note, 85% of patients who had myometrial invasion
>50% had lymph node dissection, compared with 41% of
those with myometrial invasion �50% (P < 0.001). Lymph
node dissection did not significantly influence the percent-
age of vaginal recurrences at 5 years in patients deemed at
high risk for vaginal relapse. In fact, if only patients with
grade 3 tumor are considered, 16% of those who did not
have lymph node dissection had vaginal recurrence at 5
years, compared with 6% in appropriately staged patients
(P = 0.24). Furthermore, if only patients with LVI are
considered, 0% of those who did not have lymph node
dissection had vaginal recurrence at 5 years, compared with
8% in appropriately staged patients (P = 0.53).
Vaginal relapses in patients with nonendometrioid tumors
Among the 33 patients with a nonendometrioid tumor, 12
(36%) received adjuvant radiotherapy (8 had external pelvic
radiotherapy only, 3 had external pelvic radiotherapy in
association with vaginal brachytherapy, and 1 had vaginal
brachytherapy only). The overall rate of vaginal relapse at 5
years was 9%. No discernible difference in the frequency of
vaginal relapse was observed between patients who received
adjuvant radiotherapy (8%) and those who did not (10%)
(P = 0.85). Vaginal relapse was not observed in the 4
patients who had vaginal brachytherapy.
Predictors of vaginal relapse in patients with endometrioid
tumor: stratified analysis according to stage, LVI, histologic
grade, and adjuvant radiotherapy
The 599 patients with an endometrioid tumor were
stratified on the basis of substage and the presence of LVI
and grade 3 differentiation. We observed that adjuvant
radiotherapy was generally administered to patients with
stage IC disease independently of LVI or grade. By
contrast, only a small number of patients with stage IA
or IB disease received radiotherapy. In patients with limited
myometrial invasion, the decision to administer adjuvant
radiotherapy was usually dictated by the presence of grade
3 differentiation (Fig. 1). Among patients with an
endometrioid tumor who did not receive adjuvant radiation,
most vaginal relapses were confined to the subgroup with
stage IA or IB disease and either LVI or grade 3
differentiation. For this group of patients, the rate of
vaginal relapse at 5 years was 12%, compared with 2.1%
for patients with stage IA or IB disease and neither LVI nor
grade 3 differentiation. Of interest, no vaginal relapse was
observed in the 34 patients with stage IC disease who did
not receive any adjuvant radiation (8 patients had grade 3
differentiation or LVI) (Fig. 2).
Discussion
In the present study, we analyzed factors predictive of
vaginal recurrence in endometrial cancer. The rate of vaginal
relapse in our series of patients with stage I disease who did
not have adjuvant radiotherapy was 3% at 5 years. This rate
is similar to that reported in the literature [11,12]. However,
because of the retrospective design of our study, the true
overall risk of vaginal recurrence in patients with stage I
disease may have been underestimated [13]. In fact, patients
with risk factors predictive of recurrence were more likely to
receive adjuvant radiotherapy, which would be expected to
lower the estimated risk of vaginal relapse (Table 2, Fig. 1).
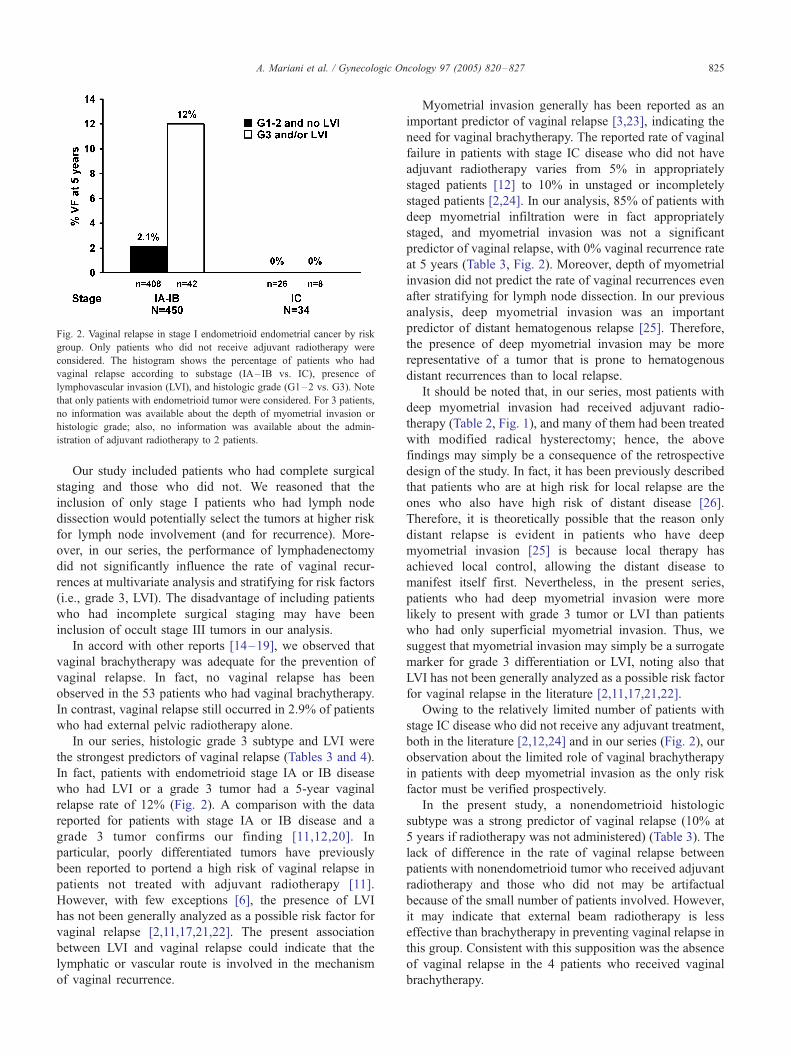
Fig. 2. Vaginal relapse in stage I endometrioid endometrial cancer by risk
group. Only patients who did not receive adjuvant radiotherapy were
considered. The histogram shows the percentage of patients who had
vaginal relapse according to substage (IA– IB vs. IC), presence of
lymphovascular invasion (LVI), and histologic grade (G1–2 vs. G3). Note
that only patients with endometrioid tumor were considered. For 3 patients,
no information was available about the depth of myometrial invasion or
histologic grade; also, no information was available about the admin-
istration of adjuvant radiotherapy to 2 patients.
A. Mariani et al. / Gynecologic Oncology 97 (2005) 820–827 825
Our study included patients who had complete surgical
staging and those who did not. We reasoned that the
inclusion of only stage I patients who had lymph node
dissection would potentially select the tumors at higher risk
for lymph node involvement (and for recurrence). More-
over, in our series, the performance of lymphadenectomy
did not significantly influence the rate of vaginal recur-
rences at multivariate analysis and stratifying for risk factors
(i.e., grade 3, LVI). The disadvantage of including patients
who had incomplete surgical staging may have been
inclusion of occult stage III tumors in our analysis.
In accord with other reports [14–19], we observed that
vaginal brachytherapy was adequate for the prevention of
vaginal relapse. In fact, no vaginal relapse has been
observed in the 53 patients who had vaginal brachytherapy.
In contrast, vaginal relapse still occurred in 2.9% of patients
who had external pelvic radiotherapy alone.
In our series, histologic grade 3 subtype and LVI were
the strongest predictors of vaginal relapse (Tables 3 and 4).
In fact, patients with endometrioid stage IA or IB disease
who had LVI or a grade 3 tumor had a 5-year vaginal
relapse rate of 12% (Fig. 2). A comparison with the data
reported for patients with stage IA or IB disease and a
grade 3 tumor confirms our finding [11,12,20]. In
particular, poorly differentiated tumors have previously
been reported to portend a high risk of vaginal relapse in
patients not treated with adjuvant radiotherapy [11].
However, with few exceptions [6], the presence of LVI
has not been generally analyzed as a possible risk factor for
vaginal relapse [2,11,17,21,22]. The present association
between LVI and vaginal relapse could indicate that the
lymphatic or vascular route is involved in the mechanism
of vaginal recurrence.
Myometrial invasion generally has been reported as an
important predictor of vaginal relapse [3,23], indicating the
need for vaginal brachytherapy. The reported rate of vaginal
failure in patients with stage IC disease who did not have
adjuvant radiotherapy varies from 5% in appropriately
staged patients [12] to 10% in unstaged or incompletely
staged patients [2,24]. In our analysis, 85% of patients with
deep myometrial infiltration were in fact appropriately
staged, and myometrial invasion was not a significant
predictor of vaginal relapse, with 0% vaginal recurrence rate
at 5 years (Table 3, Fig. 2). Moreover, depth of myometrial
invasion did not predict the rate of vaginal recurrences even
after stratifying for lymph node dissection. In our previous
analysis, deep myometrial invasion was an important
predictor of distant hematogenous relapse [25]. Therefore,
the presence of deep myometrial invasion may be more
representative of a tumor that is prone to hematogenous
distant recurrences than to local relapse.
It should be noted that, in our series, most patients with
deep myometrial invasion had received adjuvant radio-
therapy (Table 2, Fig. 1), and many of them had been treated
with modified radical hysterectomy; hence, the above
findings may simply be a consequence of the retrospective
design of the study. In fact, it has been previously described
that patients who are at high risk for local relapse are the
ones who also have high risk of distant disease [26].
Therefore, it is theoretically possible that the reason only
distant relapse is evident in patients who have deep
myometrial invasion [25] is because local therapy has
achieved local control, allowing the distant disease to
manifest itself first. Nevertheless, in the present series,
patients who had deep myometrial invasion were more
likely to present with grade 3 tumor or LVI than patients
who had only superficial myometrial invasion. Thus, we
suggest that myometrial invasion may simply be a surrogate
marker for grade 3 differentiation or LVI, noting also that
LVI has not been generally analyzed as a possible risk factor
for vaginal relapse in the literature [2,11,17,21,22].
Owing to the relatively limited number of patients with
stage IC disease who did not receive any adjuvant treatment,
both in the literature [2,12,24] and in our series (Fig. 2), our
observation about the limited role of vaginal brachytherapy
in patients with deep myometrial invasion as the only risk
factor must be verified prospectively.
In the present study, a nonendometrioid histologic
subtype was a strong predictor of vaginal relapse (10% at
5 years if radiotherapy was not administered) (Table 3). The
lack of difference in the rate of vaginal relapse between
patients with nonendometrioid tumor who received adjuvant
radiotherapy and those who did not may be artifactual
because of the small number of patients involved. However,
it may indicate that external beam radiotherapy is less
effective than brachytherapy in preventing vaginal relapse in
this group. Consistent with this supposition was the absence
of vaginal relapse in the 4 patients who received vaginal
brachytherapy.

A. Mariani et al. / Gynecologic Oncology 97 (2005) 820–827826
We previously reported predictors of hematogenous [25],
lymphatic [27], and peritoneal [28] relapse in endometrial
cancer. The present study, with the identification of
predictors of vaginal relapse, completes the analysis on
the different routes of metastasis in endometrial cancer. All
our findings may help in the decision to implement a target-
based plan of adjuvant therapy, based on the predicted
routes of tumor spread. In the presence of predictors of
hematogenous or peritoneal relapse, systemic therapy may
be efficacious [29]. Predictors of lymphatic relapse may
dictate the need for external adjuvant radiotherapy [30], and
predictors of vaginal relapse would suggest adjuvant vaginal
brachytherapy [14–19]. Hence, site-specific therapy would
be based on predictors of the four routes of relapse rather
than only on the stage of disease.
In conclusion, grade 3 differentiation and LVI were the
strongest predictors of vaginal relapse in our population.
The cost and morbidity of vaginal brachytherapy should be
balanced against the potential risk of vaginal relapse when
counseling patients who have stage I disease: a 2% risk of
vaginal relapse with low-grade lesions without LVI and 11%
with either grade 3 differentiation or LVI (or both).
Although the role of deep myometrial invasion in predicting
vaginal relapse appears to be a surrogate for grade 3 tumor
differentiation or LVI or both, verification awaits prospec-
tive analysis. Therefore, we currently recommend post-
operative vaginal brachytherapy only to patients with stage I
disease who have either one (or both) of the following 2
characteristics: grade 3 tumor differentiation or LVI.
Acknowledgments
Supported by the Mayo Cancer Center (P30CA15083)
and the Rochester Research Committee, Mayo Foundation.
References
[1] Jemal A, Murray T, Ward E, Samuels A, Tiwari RC, Ghafoor A, et al.
Cancer statistics, 2005. CA Cancer J Clin 2005;55:10–30.
[2] Creutzberg CL, et al. for the PORTEC Study Group. Surgery and
postoperative radiotherapy versus surgery alone for patients with
stage-1 endometrial carcinoma: multicentre randomised trial. Lancet
2000;355:1404–11.
[3] Elliott P, Green D, Coates A, Kreiger M, Russell P, Coppleson M,
et al. The efficacy of postoperative vaginal irradiation in preventing
vaginal recurrence in endometrial cancer. Int J Gynecol Cancer
1994;4:84–93.
[4] Tewari K, Cappuccini F, Brewster WR, DiSaia PJ, Berman ML,
Manetta A, et al. Interstitial brachytherapy for vaginal recurrences of
endometrial carcinoma. Gynecol Oncol 1999;74:416–22.
[5] Creutzberg CL, et al. for the PORTEC Study Group. Survival after
relapse in patients with endometrial cancer: results from a randomized
trial. Gynecol Oncol 2003;89:201–9.
[6] Alektiar KM, McKee A, Venkatraman E, McKee B, Zelefsky MJ,
Mychalczak BR, et al. Intravaginal high-dose-rate brachytherapy for
Stage IB (FIGO Grade 1, 2) endometrial cancer. Int J Radiat Oncol
Biol Phys 2002;53:707–13.
[7] Podratz KC, Mariani A, Webb MJ. Staging and therapeutic value of
lymphadenectomy in endometrial cancer. Gynecol Oncol 1998;70:
163–4.
[8] Creasman WT, Odicino F, Maisonneuve P, Beller U, Benedet JL,
Heintz AP, et al. Carcinoma of the corpus uteri. J Epidemiol Biostat
2001;6:47–86.
[9] Scully RE, Bonfiglio TA, Kurman RJ, Silverberg SG, Wilkenson EJ,
editors. Histological Typing of Female Genital Tract Tumours. 2nd ed.
Berlin’ Springer-Verlag; 1994. p. 13–8.
[10] Mariani A, Webb MJ, Keeney GL, Haddock MG, Calori G, Podratz
KC. Low-risk corpus cancer: is lymphadenectomy or radiotherapy
necessary? Am J Obstet Gynecol 2000;182:1506–19.
[11] Straughn Jr JM, Huh WK, Kelly FJ, Leath III CA, Kleinberg
MJ, Hyde Jr J, et al. Conservative management of stage I endo-
metrial carcinoma after surgical staging. Gynecol Oncol 2002;84:
194–200.
[12] Straughn JM, Huh WK, Orr Jr JW , Kelly FJ, Roland PY, Gold MA,
et al. Stage IC adenocarcinoma of the endometrium: survival com-
parisons of surgically staged patients with and without adjuvant
radiation therapy. Gynecol Oncol 2003;89:295–300.
[13] Keys HM, et al. Gynecologic Oncology Group. A phase III trial of
surgery with or without adjunctive external pelvic radiation therapy in
intermediate risk endometrial adenocarcinoma: a Gynecologic Onco-
logy Group study. Gynecol Oncol 2004;92:744–51 [Erratum in:
Gynecol Oncol. 94 (2004) 241–2].
[14] MacLeod C, Fowler A, Duval P, D_Costa I, Dalrymple C, Elliott P,
et al. Adjuvant high-dose rate brachytherapy with or without external
beam radiotherapy post-hysterectomy for endometrial cancer. Int J
Gynecol Cancer 1999;9:247–55.
[15] Mohan DS, Samuels MA, Selim MA, Shalodi AD, Ellis RJ, Samuels
JR, et al. Long-term outcomes of therapeutic pelvic lymphadenectomy
for stage I endometrial adenocarcinoma. Gynecol Oncol
1998;70:165–71.
[16] Seago DP, Raman A, Lele S. Potential benefit of lymphadenectomy
for the treatment of node-negative locally advanced uterine cancers.
Gynecol Oncol 2001;83:282–5.
[17] Fanning J. Long-term survival of intermediate risk endometrial cancer
(stage IG3, IC, II) treated with full lymphadenectomy and brachyther-
apy without teletherapy. Gynecol Oncol 2001;82:371–4.
[18] Chadha M. Gynecologic brachytherapy—II: intravaginal brachyther-
apy for carcinoma of the endometrium. Semin Radiat Oncol
2002;12:53–61.
[19] Bliss P, Cowie VJ. Endometrial carcinoma: does the addition of
intracavitary vault caesium to external beam therapy postoperatively
result in improved control or increased morbidity? Clin Oncol (R Coll
Radiol) 1992;4:373–6.
[20] Orr Jr JW, Holimon JL, Orr PF. Stage I corpus cancer: is teletherapy
necessary? Am J Obstet Gynecol 1997;176:777–88.
[21] Larson DM, Broste SK, Krawisz BR. Surgery without radiotherapy for
primary treatment of endometrial cancer. Obstet Gynecol
1998;91:355–9.
[22] Ng TY, Perrin LC, Nicklin JL, Cheuk R, Crandon AJ. Local
recurrence in high-risk node-negative stage I endometrial carcinoma
treated with postoperative vaginal vault brachytherapy. Gynecol Oncol
2000;79:490–4.
[23] Morrow CP, Bundy BN, Kurman RJ, Creasman WT, Heller P,
Homesley HD, et al. Relationship between surgical-pathological risk
factors and outcome in clinical stage I and II carcinoma of the
endometrium: a Gynecologic Oncology Group study. Gynecol Oncol
1991;40:55–65.
[24] Hogberg T, et al. Southern Swedish Gynecologic Oncology Group. A
prospective population-based management program including primary
surgery and postoperative risk assessment by means of DNA ploidy
and histopathology: adjuvant radiotherapy is not necessary for the
majority of patients with FIGO stage I– II endometrial cancer. Int J
Gynecol Cancer 2004;14:437–50.
[25] Mariani A, Webb MJ, Keeney GL, Calori G, Podratz KC. Hema-

A. Mariani et al. / Gynecologic Oncology 97 (2005) 820–827 827
togenous dissemination in corpus cancer. Gynecol Oncol 2001;80:
233–8.
[26] Corn BW, Lanciano RM, D_agostino R, Kiggundu E, Dunton CJ,
Purser P, et al. The relationship of local and distant failure from endo-
metrial cancer: defining a clinical paradigm. Gynecol Oncol 1997;
66:411–6.
[27] Mariani A, Webb MJ, Keeney GL, Aletti G, Podratz KC. Predictors of
lymphatic relapse in endometrial cancer. Gynecol Oncol 2002;84:
437–42.
[28] Mariani A, Webb MJ, Keeney GL, Aletti G, Podratz KC.
Endometrial cancer: predictors of peritoneal relapse. Gynecol Oncol
2003;89:236–42.
[29] Mariani A, Dowdy SC, Keeney GL, Long HJ, Lesnick TG, Podratz
KC. High-risk endometrial cancer subgroups: candidates for target-
based adjuvant therapy. Gynecol Oncol 2004;95:120–6.
[30] Mariani A, Webb MJ, Keeney GL, Podratz KC. Efficacy of
adjuvant radiotherapy (RT) in preventing pelvic and paraaortic
failure in patients with endometrial cancer (ENDOCA) and
positive lymph nodes. Int J Gynecol Cancer 2003;13(Suppl 1):75
[abstract].