Embed Size (px)
Citation preview

Preface
The European Guidelines for Quality Assurance in Breast CancerScreening and Diagnosis of the European Commission (Perry et al.2004) pertain basically to mammography, and very little to adjunc-tive methods. But the early detection of breast cancer can be effec-tive only when the three pillars—clinical investigation, mammogra-phy, ultrasound—are united within a structured, quality-assuredprogram. The German S3 guidelines (Albert et al. 2003, 2008;Kreienberg et al. 2008) come closest to meeting this requirement.The European and American guidelines are very similar to eachother but are basically limited to mammography. Professor Klaus-Dieter Schultz and his team were instrumental in introducing theS3 guidelines, which were revised in 2008 to become the qualitystandard throughout Germany. The German and English editions ofthis atlas were therefore dedicated to Professor Schultz, whose sud-den death left a gaping hole in the German Senology Society. I creditProfessor Schultz with many valuable ideas that set my professionalhorizon during my years of working with him in the Society.
Rigorous efforts at early detection (secondary prevention) aswell as adjuvant surgical and medical treatments (tertiary preven-tion of recurrence and metastasis) have significantly improved thesurvival rates and mortality rates for breast cancer throughout theworld during the past 25 years. These factors do not account for thedeclining aggressiveness of malignant tumors that has been docu-mented in recent decades.
Primary prevention, or the prevention of gradual malignant tu-mor development in response to tumor-stimulating biological orsynthetic agents, is not yet a reality. This atlas is concerned withsecondary cancer prevention.
The illustrations in this book do not include mammograms thatdisplay obvious tumors with associated palpable nodules. There arevery good textbooks and atlases of mammography that present im-ages of this kind (for example, Barth and Prechtel 1991; Tabar et al.2000; Fischer and Baum 2005). A great many of the mammogramsin this book show only minimal changes or no abnormalities at all,which makes the ultrasound findings all the more impressive bycomparison. This is typical of the cases that are seen outside ofscreening programs. I have focused mainly on difficult cases illus-trating the diagnostic hurdles and forensic pitfalls that are encoun-tered in breast diagnosis. I hope that even experienced colleagueswill find this book a valuable teaching aid.
I could not illustrate everything that would be important in rou-tine situations—the scope of modern breast diagnosis is too exten-sive. But the book is intended to show how important it is to knowall the diagnostic possibilities in the breast, not onlymammography.
Because such high standards are placed on the technical qualityof mammograms throughout the world, our radiologic technologist,Elfi Steinhilber, contributed a special section dealing with mammo-graphic positioning and quality assurance. Using the PGMI system,physicians and their assistants who perform mammography canrate the technical quality of their mammograms as “perfect,”“good,” “moderate,” or “inadequate.” This section pertains to both
conventional and digital mammography and should be requiredreading for every breast diagnostician.
My computer expert, Oliver Wild, authored the section on digitalfull-field mammography. He explains the advantages of this technol-ogy for screening and modern diagnostic testing and for making adetailed comparison of current and previous mammograms—pri-mary digital images as well as images that have been secondarilyscanned into the computer.
A section written by my practice partner, Dr. Johannes Herr-
mann, gives readers the opportunity to interpret subtle mammo-graphic changes (in mammgraphic case presentation and training ininterpretation). These images simulate a screening situation. Someof the mammograms show only minimal changes or appear normaldespite the presence of a breast tumor. This section illustrates thelimitations of mammograms and shows that mammography aloneis (outside of screening) no longer the gold standard and can yieldoptimum results only in concert with other modalities. Typicalscreening cases are also illustrated.
Recall the publications of Nakama et al. (1991), Gordon andGoldenberg (1995), Teboul and Halliwell (1995), Kolb et al. (2002),and Leconte et al. 2003 to understand the possibilities of ultrasound,and the 2006 study by Dr. Wendie Berg of Johns Hopkins University(Berg et al. 2008), in which mammography plus breast ultrasounddetected almost one-third more cancers than mammography alone.So what are we waiting for?
It should be added that ultrasound may yield false-positives thatprompt unnecessary interventions, but this does not alter the factthat ultrasound reduces interval cancers and improves the pros-pects for a cure. Mammography generates a significantly higherrate of false-positive findings (30%), which cause serious distressfor the affected women. The addition of ultrasound eliminates ap-proximately 50% of recalls, fully compensating for the 5% rate offalse-positive sonographic findings. Fine-needle aspiration (FNA) isparticularly useful for identifying false-positive ultrasound findingsat low cost and very quickly (Berg et al. 1962; Zajicek 1974; Schön-dorf 1977; Lindholm 1999; Orell 1999; Frohwein 2002).
The section on screening and tumor progression underscores thistheme by showing how tumors that were missed on previous mam-mograms can be detected retrospectively on the basis of relativelysubtle findings. Every breast diagnostician has missed a tumor ordelayed its diagnosis at one time or another. This should not be a fre-quent occurrence, however. We practitioners cannot treat the con-cept of interval cancer as an abstraction; sometimes we must ex-plain in a court of law why we missed a tumor that may haveharmed our patient.
Other sections in this book deal with breast cancer in youngwomen and during pregnancy. Diseases of the male breast are alsoaddressed.
We examine the pitfalls of pre- and postoperative diagnosis andthe possibilities and limitations of breast diagnosis in the postoper-ative care setting. Performed by nonscreening radiologists and
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
VII

gynecologists, these follow-up examinations require special exper-tise in the differenzial diagnosis of mammographic, sonographic,and MRI findings.
Breast implants are included because of the growing numbers ofwomen who present with these devices after breast-conservingtherapy. These cases cannot be adequately evaluated by single-view mammography, and we must obtain a second view or even athird view in selected cases. Familiarity with different types of im-plant is essential in order to be able to make an accurate differenzialdiagnosis.
We take a critical look at imaging modalities that either are usedas a matter of course or are withheld from patients due to their highcost. These include magnetic resonance imaging (MRI), positronemission tomography (PET), and PET/CT. Why should MRI be usedonly in patients with lobular carcinoma to define tumor extent andevaluate the healthy breast, merely because MRI has been identifiedas the best evidence-based modality for lobular cancer detection?MRI should be available for the preoperative analysis of all malig-nant tumors, especially in younger women, if it will advance treat-ment planning. Most doctors would not think twice about evaluat-ing the knee joint or a little finger with MRI. Why, then, is there areluctance to apply this modality to breast cancer, with its manytherapeutic challenges and potenzial for recurrence?
We touch on the importance of dedicated, certified breast centersas an effective approach to early cancer detection and treatment.These breast centers have been an important factor in the world-wide decline of breast cancer mortality. Centers are springing upeverywhere in the world, which is a positive development (Kreien-berg et al. 2008).
It is unacceptable for a woman to be referred to a hospital forcancer treatment simply because the referring physician is a friendof the department head. The international care standard for breastcancer treatment is met only at a specialized care center where alldiagnostic and therapeutic information is coordinated, archived,and reviewed at multidisciplinary case conferences—a place whereall therapeutic options are available and can be practiced in an opti-mal way. Digital patient databases are essential in this setting, al-though security and confidentially issues have kept them from be-ing established on a broad, interdisciplinary scale.
The axilla is a region of profound importance. Untold misery hasresulted from aggressive, often unnecessary, axillary lymph nodedissections (with or without irradiation) in breast cancer patients.The worldwide introduction of the sentinel node biopsy has sparedmany women the sufferings of arm edema, axillary foreign-bodysensation, and radiating pains. My former colleagues Dr. Brigitte
Koellner and Dr. Petra Zimmer have dealt with this topic for years.They introduced the sentinel node biopsy at Esslingen Hospital10 years ago and worked with the gynecology chief Professor Dr.Thorsten Kuehn and his team to optimize the procedure. I extendspecial thanks to Dr. Koellner for writing the section on the sentinellymph node procedure.
Acknowledgments
An atlas of this kind is always a team effort. Many have helped me inbringing the book to completion, including those whoworked in thebackground. I am particularly indebted to my secretary, CorneliaWahl, who typed the manuscript and made revisions from her
home while caring for her child. I also express sincere thanks to myassistants Hatice Kara and Derya Celik, Heide Scherbaum, Milka Leo-vac, and Tuğçe Yiğit. They painstakingly collected the publishedmammograms and sonograms, scanned them into the computer,and looked up numerous case histories.
I am grateful to my colleagues Professor Dr. Thorsten Kuehn, chiefof gynecologyat EsslingenHospital, and ProfessorDr. StefanKraemer,who succeeded me as head of the radiology department at Esslin-gen Hospital, for providing me with valuable suggestions and illus-trative materials. I thank Dr. Hans-Helmut Dahm and his partner Dr.Joern Straeter for providing some of the cytology illustrations and alarge portion of the histologic illustrations that were included inthis book. I supplemented these illustrations with material fromthe collections of the leading German breast pathologists of recentdecades, Professor Roland Baessler (Fulda, Germany) and ProfessorKlaus Prechtel (Starnberg, Germany), with whom I worked for yearsand still maintain friendly ties. They provided me with illustrationsfor this atlas, and their contribution is gratefully acknowledged.
I also thank the former director of St. Joseph Hospital in Haan,Dr. Heinz Uedelhoven, who left me a large portion of his valuablemammogram and sonogram collection for use in scientific publica-tions. I have put several of these images to excellent use in the atlas.
I express special thanks to the radiologist Dr. Volker Frohwein ofLandstuhl, Germany, now retired. As a radiologist and cytologist (anextremely rare combination!), he was an enthusiastic, life-long col-lector of cytologic specimens from the breast. He published his ex-perience with breast cytology in the paper Frühdiagnostik des Mam-makarzinoms (2002). Dr. Volker Frohwein supplied most of thecytologic specimens pictured in this atlas.
One could hardly expect that images collected over a period ofdecades would consistently satisfy todayʼs quality standards. Forthis reason, I have replaced earlier images of poorer quality, andthe materials from Dr. Frohwein were valuable in this regard. MRimages of marginal quality have been replaced wherever possibleby similar images acquired with a 1.5-tesla scanner and the latestcoil technology. Dr. Stefan Kraemer helped me with this task.
I appreciate the help of my two former doctoral candidatesCoscina Weining and Oskar Weining-Klemm, who analyzed my casefiles from the past 10 years to identify the most economical andeffective early detection strategies as part of their doctoral disserta-tion. I am pleased to note that they found only a 1.5% incidence ofinterval cancers.
My daughter, Andrea Barth, not only edited this book time andagain, making stylistic revisions and offering excellent organization-al suggestions, but also helped me with the statistical materials. Shehas thus made a valuable contribution to the concept of the book.My son, Dr. Stephan Barth (St. Johann, Austria), did extensive litera-ture research that was necessary to ensure that the contents of theatlas were up to date. He also revised the chapter on breast cancer inmales.
I thank the staff at Thieme Publishers, especially Gabriele Kuhn-Giovannini, and Elisabeth Kurz for their work in producing the Eng-lish edition. I extend special thanks to the translators of the book,Terry Telger and Julie Foster, and to the copy editor Len Cegielka forhis excellent work.
Finally I would like to thank all the retired department heads atEsslingen Hospital for decades of friendly cooperation and wishthem all the best.
Volker Barth, MD
Preface
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
VIII

A
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
a B b C c D d E e F f G g H h I i J j
Question on Fig. 4.25
Which statement is correct?
(a) Benign calcifications were removed with clear margins.
(b) Malignant calcifications were removed with clear margins.
(c) Benign calcifications were not removed with clear margins.
(d) Malignant calcifications were not removed with clear margins.
→ Answer on p. 347
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
Fig. 4.26 A 62-year-old woman with an 18-month history of recurrent galactorrhea from a single duct in one breast. She had no other clinicalabnormalities and no family history of breast cancer (similar to the case in Fig. 5.114a, p. 245).
a Ultrasound scan of shows a 1.2 × 0.8 × 0.8 cm nodule withsmooth margins and a well-circumscribed central hypoecho-ic cyst. The surrounding tissue is rich in stroma and appearsnormal.
Fig. 4.25 Borderline area between DH, ADH, and carcinoma. (continued)
c Specimen radiograph with three localizing wires and the main calcifi-cation cluster.
d Histologic section of the calcifications. The sections were evaluatedby three pathologists.
4 Macroanatomy, Histology, Radiography, and Ultrasound52

1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
tTsSrRqQpPoOnNmMlLkK
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
b Bilateral oblique mammograms (magnified views). (ACR 2, BIRADS?, PGMI).
Question 1 on Fig. 4.26
Where is the tumor located in the mammogram? (Give coordinates.)
Question 2 on Fig. 4.26
How would you interpret the lesion based on clinical, cytological, sonographic,
and mammographic findings?
(a) Fibroadenoma
(b) Medullary carcinoma
(c) Intacystic or intraductal papilloma
→ Answers on p. 347
Fig. 4.26 Recurrent galactorrhea. (continued)
c Bilateral craniocaudal mammograms (PGMI).
d Cytology: fine-needle aspiration (FNA) yieldselongated cells with a narrow cytoplasmic rimthat are arranged in a “school of fish” pattern.
e Histologic section shows intraductal proliferation with cells similar tothose in d.
Preinvasive Lesions 53

Noncalcifying ductal carcinoma is not detectable at ultrasound,even with a high-resolution probe (11–13MHz), until it reaches atleast 5mm in diameter. This is still significantly earlier than it canbe detected on mammograms. Vignal et al. (2002) conducted a his-topathologic study to determine why ultrasound is superior tomammography in detecting some carcinomas. They found thatwith certain early carcinomas, hyaluronic acid is stored within thetumor tissue and its surroundings. While this process is visible so-nographically, appearing as a hypoechoic focal mass, it is mammo-graphically occult. Only when fibrotic structures containing actin(desmoid reactions) or microcalcifications form do they becomevisible on mammograms. However, these structures were presentin only 13 of the 22 carcinomas that were investigated in the study.
When the tumor is in close contract with a TDLU or main duct(see p. 23), ultrasound displays an ill-defined area that may or maynot have a hyperechoic rim. The lesion increases in size until itcrosses into neighboring septa and undergoes asymmetric spread(see Fig. 5.64 d, p. 162). This opacity may be round or elliptical, or itmay have a triangular shape with the apex pointing toward the nip-ple (segmental tumor involvement).
Noncalcifying ductal carcinoma appears on gadolinium-en-hanced T1-weighted MR subtraction images as an ill-defined areaof contrast uptake (detectable when 1 cm or larger). The degree ofenhancement depends on the degree of tumor differentiation. Poor-ly differentiated (G3) tumors show intense enhancement, inter-mediate-grade (G2) tumors show moderate enhancement, andwell-differentiated (G1) tumors show little or no enhancement.This method is not entirely reliable, therefore (see Figs. 4.27 k,p. 349 and Figs. 4.29 e,k, p. 56 f) and correlates with tumor vascular-ity.
The first clinical manifestation of ductal carcinoma is nipple re-traction (see Fig. 4.37b, c). Ten percent of cases present with abloody or brownish watery discharge, which means that the tumorcan be visualized by ductography (see Fig. 4.27 l, m, p. 349).
The morphologic, clinical, radiographic, sonographic, and MRimaging features of early noncalcifying ductal carcinoma are listedbelow:l Morphologic features: tumor proliferation within the ducts.l Radiographic features: increased duct density, reticular opaci-
ties, asymmetries, frequent absence of radiographic signs.
l Clinical features: no palpable mass, nonspecific doughy firmnessof the glandular tissue, nipple retraction, discharge (bloody orwatery).
l Sonographic features: ductectasia with intraductal proliferation.l MRI features: predominantly ductal gadolinium enhancement.
It is not unusual to find intraductal carcinomas in proximity to acyst, or a cyst may develop next to the intraductal tumor when thetumor mass obstructs the draining duct (Fig. 4.15). In extremelyrare cases carcinomas develop in the wall of duct cysts, creating theappearance of a cystic carcinoma (see Fig. 5.138, p. 274).
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
Fig. 4.36 Ultrasound displays noncalcifying ductal carcinoma as ascalloped, hypoechoic nodule measuring 1.8 × 1.2 cm. Faint acousticshadows are visible at the edges of the lesion. Adjacent glandular tissueis rich in connective tissue (interlobular stroma).
Fig. 4.37 A 59-year-old woman who presented with a nonspecificmass at the 12-o’clock position in the upper quadrant of the leftbreast.Therewasnoskinornipple retractionandnodischarge. The lesionwas identified histologically as noncalcifying invasive ductal carcinoma.
a Mammography showing left oblique view: inhomogeneous linearopacities a great distance from the nipple (thus no nipple retraction).
b Histologic section of the areola (a different patient) shows a retroar-eolar noncalcifying tumor infiltrating the milk ducts, with nipple retrac-tion as a first clinical sign of malignancy. c Clinical aspect of tumor-in-duced nipple retraction.
4 Macroanatomy, Histology, Radiography, and Ultrasound66

Ductal Spread with Calcifications
See Fig. 4.34d, p. 65.The pathologist finds calcifications or hydroxyapatite in approx-
imately two-thirds of all ductal carcinomas (Barth et al. 1977), whilethe radiologists finds them in only one-third of cases. This relates tothe resolution limits of radiographs and to particle size. The parti-cles are smaller and more numerous in calcifying ductal carcinomathan in other infiltrating malignancies (Hassler 1969). They are
pleomorphic in the comedo type, flocculent in the papillary type,and punctate in the cribriform type. They present a variety of clustershapes within the lobes and lobules including triangular (Fig. 4.38)and dovetail configurations. Lanyi refers to these configurationsagain and again in his numerous publications (Lanyi 1986, 2003; La-nyi et al. 1994). The calcifications occur not only in the lumina of theducts and lobules but also—with benign lesions—in the interlobularstroma (Barth 1979a). The particles vary in size and present bizarre
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
Fig. 4.38 Comedocarcinoma.
a Clinical appear-ance of the breastshows a tumor bulg-ing beneath the skin(arrows) and a milkywhite nipple dis-charge (milk of cal-cium).
b Mediolateral mammogram shows massive coarse calcifications withpleomorphic particles. The Cooper ligaments of the nipple also show cal-cifications (tumor involves the entire lobe and has spread into surround-ing tissues).
c Cut surface of thetumor shows ectaticgrayish-white ducts,some ruptured, withyellow comedoneplugs that can bepopped like acneblackheads andsqueezed from thecut surface (hencethe name “come-done”).
Invasive Carcinoma 67

should be performed by the same physician whenever possible. Di-agnostically relevant regions of the breast should be scanned andx-rayed in the same session and evaluated by the same eye. It is in-efficient for a gynecologist to perform ultrasound while a radiolog-ist takes the x-rays at a different time and location.
The indications for breast ultrasound are as follows:l Investigation of palpable abnormalitiesl Investigation of clinically occult mammographic findings (focal
densities with smooth or ill-defined margins, circumscribedasymmetries)
l Radiographic breast density of ACR 2–4l Previous silicone implantation, reconstruction, or augmentationl Regular screening examinations in high-risk patients age 25
years or older, supported by mammography and magnetic reso-nance imaging
l Imaging guidance of diagnostic and therapeutic interventionalprocedures in the breast
l Questions relating to hormone replacement therapy in meno-pausal women
The physicianwho performs mammography—whether a radiologistor gynecologist—should have the option of performing both mam-mography and ultrasound and to order any necessary intervention-al procedures without delay.
Examination Technique
Generally the examiner should scan both breasts while applyingcarefully controlled transducer pressure. The examination shouldinclude both axillae, and the infraclavicular fossae should be scan-ned in follow-up examinations to rule out malignancy in the clavic-ular recess (see Fig. 5.61, p. 157 and Fig. 5.54a, p. 146), and theother recess (see Fig. 4.24k, p. 347).
The patient is usually positioned supine with the arms claspedbehind the head. A semilateral or wedge-supported position maybe helpful for evaluating the outer quadrants, especially in patientswith large breasts.
With an oblique supine position, the breast is optimally flat-tened against the chest wall and even peripheral nodules will notslip out of the scanning plane beneath the transducer. The patientshould not be examined in a standing or sitting posture unless shehas noticed something peculiar in a certain position that is not re-producible in the supine position.
Contact pressure during the examination should be sufficient toprovide clear differentiation of intramammary structures (fat, con-nective tissue, glandular parenchyma), but pressure should not beso high as to induce any pain. During scanning, the transducershould always be held perpendicular to the breast parenchyma asoblique scanning will cause artifacts.
The field of view should maximally occupy the width of themonitor screen. The pectoral fascia should form the lower (far)boundary of the scan and should be clearly defined. If the pectoralfascia cannot be clearly identified, the breast should be scanned ata lower frequency to allow deeper sound penetration.
Uniform focusing should be achieved between the skin and pec-toral fascia, preferably through the use of multiple focal zones.
Scanning should be performed in overlapping planes to ensurecomplete coverage of the breast. Attention is given to the shape of
thebreast parenchyma. It is best to use a radial scanning pattern, tak-ing as a reference point the retroareolar region and the terminal ductlobular units of a particular mammary lobe. This is particularly im-portant in the investigation of physiologic changes. The transduceris positioned radially for the analysis of individual lobes. From thatposition the transducer is angled and rotated to locate the principalduct of interest, which provides a landmark for anatomic orientation(Fig. 5.60). The breast is scanned primarily in horizontal and verticalplanes, however, for the detection or exclusion of suspicious lesions.
The scan planes should be reproducible both in the documenta-tion of abnormalities (scan plane centered over the tumor) and inthe visualization of focal lesions. Reproducibility is aided by thebody markers that are available in every system.
TipThe documentation of an abnormal finding should at least covera representative parenchymal region in each breast and shouldinclude the nipple region. The abnormality should be visualizedand measured in two planes. The axillary region should also bedocumented if it has been scanned.
The documentation of a focal lesion should include the followingdata on lesion location:l Affected side (right/left)l Clock-face position of the lesion relative to the nipplel Distance from the center of the nipple to the closest lesion mar-
gin (in mm or cm)l Lesion depth = distance from the skin to the closest lesion mar-
gin (in mm or cm)l Size of the lesion in three dimensions measured in twomutually
perpendicular scan planes
The major tumor axis should also be indicated. In addition to purelymetric data, the lesion shouldbe characterized in termsof its echoge-nicity (e.g., a hypoechoic or hyperechoic corewith an echogenic rim).
The following features are used to describe the sonographic mor-
phology of a lesion:l Echogenicity relative to surrounding tissues: anechoic, hypo-
echoic, isoechoic, or hyperechoicl Shape: round, oval, complex, patchyl Margins: smooth, lobulated, irregular, ill-definedl Internal echo pattern: homogeneous, inhomogeneous, hetero-
geneousl Sound transmission: shadowing, indifferent, enhancementl Surroundings: satellite or second lesions, contralateral lesionsl Axillary lymph nodes: fatty, indifferent, suspicious, enlarged
The breast ultrasound report should include the following data andinformation:l Patient identityl Date of examinationl Essential information on the current and prior history (previous
findings!)l Indication for breast ultrasoundl Visual and palpable findingsl Sonographic findingsl Relationship to mammogram or magnetic resonance image (if
available)
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
5 Early Detection and Appropriate Treatment154

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
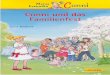
Fig. 5.60 Anatomy of the mammary lobes and scanning technique during breast ultrasound (from Teboul and Halliwell 1995).
a b
5
2
7
6
4
3
8
1
1
1
c d
2
3
1Lobules
Duct
3
6
4
3
78
8
9
Scanned duct
Lobules
a Diagrammatic representation of a mammary lobe in the retroareolar re-gion (1). The lobules near the nipple (6) tend to be shorter and thickerthan the peripheral lobules (4). Some lobules (7) run perpendicular tothe main duct (3) (see also Fig. 2.1a) and overlap the anterior edge ofthe lobe, creating a cobblestone appearance (see Fig. 5.70 d). Others(8) extend into the Cooper ligaments and pass with them into the cuta-neous fascia (9).b Anatomy of the terminal duct lobular unit: nipple and retroareolar re-gion (1), lactiferous sinus (2), lactiferous duct (3), and the most com-mon types of lobule (4–7): short, thick lobule close to the nipple (4), lo-bule with microcystic degeneration (5), atrophic lobule (6), cysticenlargement of a lobule (7), and multiple lobules with branched connec-tions (8). Lobules usually exhibit a cloverleaf shape in the periphery.
The terminal duct lobular unit of Wellings (1972) is a complex formedby the ductolobular and tubular units and containing acini and terminalducts. The terminal duct lobular units (TDLUs) are the basic milk-produc-ing units of the breast.
Most carcinomas originate in the TDLU and are basically ductolobularcarcinomas (see also Figs. 4.12, 4.13, p. 31). During maturation of thebreast, the lobules sprout from the surface of the main ducts and extendtoward the skin, emphasizing the importance of maintaining firm trans-ducer contact during ultrasound scanning.
c Axial (radial) scan along a milk duct. Scanning in this plane most clearlydefines the lobules in relation to their surroundings. Ideally, each individ-ual lobe should be analyzed separately, but in practice this is necessaryonly if an atypical lesion is found.
The most important sonographic criterion for lobular stimulation is lo-bar prominence. Radial scanning of the lobes (1) provides the best over-view of ductolobular structures and most clearly depicts their pathologyand physiology. Some lobules may extend a distance from the main ductand project into the skin or angle back toward the duct.
Transducer position should be tailored to individual anatomy. Theprobe can be angled from its radial placement along the duct (2) tocompensate for the variable position of the TDLUs. Normally the ductscan be traced to the periphery of the lobe by radial advancement of theprobe.d Transverse scans are directed at right angles to the main duct, provid-ing cross-sectional views of the duct and afferent ductules. The lobulesthat connect with the terminal duct may occasionally form a stellate ar-rangement. Sometimes these anatomic patterns are definable, but onlywith a 13–18MHz probe.
Ultrasound 155

The ultrasound report should consist of several parts:l A description of the parenchymal structure to determine assess-
abilityl Localizationl Biometry and sonographic morphology of focal lesionsl Associated findings
Finally, a BIRADS score is determined to express the overall level ofsuspicion for a given lesion (ACR BIRADS):l Category S1: negativel Category S2: benign finding (e.g., cyst)l Category S3: probably benign (follow-up in 6 months)l Category S4: suspicious abnormality (4A, low; 4B intermediate;
4C moderate suspicious)l Category S5: highly suspicious of malignancyl Category S6: histologically confirmed malignancy
Each category is associated with a recommended action that in-cludes follow-up intervals and the possible need for further diag-nostic or interventional measures.
Schematic Protocol of Ultrasound Examination
The traditional analysis of malignant structures in breast ultrasoundis based almost entirely on the geometry of the lesion while ignor-ing basic anatomic structures—the ductal and lobular parenchyma.
Teboul and Halliwell (1995) defined benign and malignant crite-ria for the terminal duct lobular unit (TDLU) that are not widelyknown or utilized. In this approach it is not enough to scan thebreast in horizontal and vertical planes to look for atypical lesions;it must also be scanned radially along the course of the duct anddocumented (Fig. 5.61c), especially for the investigation of tumorsor changes during the course of the menstrual cycle. Follow-up ex-aminations should be interpreted with reference to this baselinedocumentation so that the same segments can be comparatively an-alyzed. This is the only way to evaluate changes in the TDLUs overtime, and it facilitates the detection of new lesions. It also ensuresan overlapping examination of all breast segments, which is of fo-rensic importance (Fig. 5.61c).
This examination, then, includes evaluation of the lactiferousducts, mammary lobes, and lobules. There are many cases in whichthis analysis can give form and meaning to apparent architecturaldisarray in a breast sonogram. To make a sonographic analysis ofthis kind, examiners must have a thorough knowledge of the patho-anatomy of the breast so that they can localize changes to specificanatomic structures (ducts, connective tissue, Cooper ligaments,skin, muscular fascia, pectoral muscles). The diagnosis should be adescriptive one that is stated in relation to these anatomic struc-tures (see p. 23 ff).
Increasingly, breast ultrasound should come to rely more onmorphology as a basis for diagnostic analysis. The geometry andmargins of a lesion must be placed within an anatomic context.
Teboul and Halliwell (1995) draw the following conclusions:l A meticulous, duct-oriented sonographic analysis of the breast
parenchyma is essential for planning cancer treatment and de-tecting abnormal parenchymal responses to hormonal stimuli,for example.
l The key to this analysis lies in identifying the terminal duct lob-ular units (TDLUs) within the breast and determining their rela-tionship to pathologic changes.
l Duct-oriented ultrasound is the only sure way to establish ana-tomic orientation in the breast and define the relationship be-tween the breast parenchyma and the structures around it.
This kind of localization and identification can often, though not al-ways, be accomplished with a high-resolution transducer (11–18MHz). Structural analysis of the lobules and TDLUs in responseto hormone replacement therapy or contraceptive use, for example,has the potential to become an important and previously unutilizedapproach in modern diagnostic ultrasound.
It would be desirable for manufacturers to produce higher-fre-quency transducers as well as ultrasound systems in which the lastexamination could be automatically displayed on a separate screenfor reference, similarly to Fig. 5.61d. The examiner should alwayswork in the same direction, beginning in the axilla and ending at a6 oʼclock position with each breast (see Fig. 5.61c). He/she can thusbe sure that each breast quadrant is examined twice and that com-parable documents are available for future examinations. The exam-iner should always follow the same systematic sequence when per-forming breast ultrasound in order to obtain comparable results(see Fig. 5.61d).
Basic Structures of the Breast and their Variants on Ultrasound,with Mammographic Correlation
The basic structures of the breast can be analyzed reasonably wellwith high-resolution transducers. Fat and glandular tissue showcontrasting echogenicities. Fatty tissue is dark (hypoechoic), whilethe glandular tissue, consisting of lobular parenchyma and the in-tra- and interlobular stroma, appears bright (hyperechoic) (seeFig. 5.75e, f, p. 177). Within the breast parenchyma, the lobes aredifficult to distinguish from one another, although this can be doneindirectly by visualizing the major ducts. The lobules and TDLUsappear as small, dark (hypoechoic) round to oval structures thatare clearly distinguishable from the hyperechoic fibrous septa (seeFig. 5.65, p. 163). This requires that the TDLUs are in a proliferativestate and are not atrophic (see Chapter 4, p. 23).
The breast consists of up to 12 lobes, each based on a major ductthat runs a straight or tortuous course (especially in the retroareolarregion) from the nipple to the periphery of the breast. Only radialscanning can define all or part of the main duct, which appears as ahypoechoic channel. The TDLUs (lobules with acini and functionalintralobular stroma) are found in proximity to the ducts. The TDLUsare not very well developed before 18 years of age. If they are detect-able at all, they appear as focal hypoechoic areas during the secondhalf of the menstrual cycle or the premenstrual phase. Fat and con-nective tissue (interlobular fibrosis) predominate normally in theadolescent breast (see Figs. 5.63, p. 160). Exceptions are possible es-pecially some weeks before menarche (see Fig. 5.62 a–d, p. 159) andin cases of malignancy (see Fig. 5.64, p. 161).
More lobule-bearing areas can be found in the postpubescentbreast. Lobules may be seen in various areas up until the first preg-nancy, usually in the relatively long lateral superior lobes in the up-per outer quadrants. The lobules become larger and more denseshortly before and during menstruation. Afterward they regress un-til ovulation, then enlarge again during the second half of the cycle
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
5 Early Detection and Appropriate Treatment156

until the next period (see Figs. 5.65–5.67, p. 163 ff). The TDLUs arevery prominent and easily visualized (often right after ovulation)in women with severe premenstrual complaints, although premen-strual syndrome may occur in the absence of lobular proliferation.The reason for this is unknown.
The lobules are most abundant during pregnancy and lactation,when the breast consists predominantly of milk-producing glandu-lar parenchyma while fat and connective tissue are displaced to themargins of the greatly enlarged TDLUs. The main ducts are dilated,and their fluctuating milk contents can be clearly visualized (seeFigs. 5.68–5.70, p. 168ff).
After lactation is completed, focal enlargement of the lobulespersists for a period of several months to years (see Fig. 5.69,p. 170). After that time the lobules gradually regress to a normalstate. Maturation of the breast is complete following the first preg-nancy (see p. 7).
Starting at about age 40 years and after menopause, the TDLUscontinuously regress from the periphery of the breast toward thenipple, again resulting in a predominance of fat and connective tis-sue. For unknown reasons, somewomen retain a substantial volumeof lobular tissue after age 40. As a result, approximately 30% of men-opausal women have relatively dense mammograms, also due inpart to an increase in connective tissue (see p. 98). Researchersshould investigate whether these breasts are responding to endoge-nous or exogenous hormonal stimulation and whether this may in-
crease the risk of breast cancer (especially lobular neoplasms). Thechanging radiodensity of the mammogram depends on the prolifer-ation of TDLUs and not on the interlobular stroma (see p. 23). In anycase it could be extremely useful for gynecologists to detect cyclicand atypical lobular proliferation in the breast in order to evaluatehormonal responses. Menopausal women with proliferating TDLUswho are on hormone replacement therapy could be prescribed a dif-ferent hormone (e.g., an estrogen-only product, especially after hys-terectomy) or might discontinue HRT if a different hormone is foundto have no effect on lobular regression. Women who do not showsignificant lobular proliferation at ultrasound presumably wouldnot have an increased breast cancer risk with HRT. Women who doshow TDLU proliferation in response to tamoxifen, for example,should be tested for paradoxical hyperestrogenemia, which may re-quire the discontinuation of tamoxifen.
These and other facts have not yet been scientifically investigat-ed but could become important in gynecologic consultations. Ultra-sound has yet to fulfill its potential. There are still unsuspected pos-sibilities in the assessment of patients on HRT, perhaps includingthe use of higher-resolution transducers or even probes that couldbe “tuned” to the hormone status of individual patients.
Figs. 5.71–5.83 (p. 172ff) illustrate numerous cases with mam-mography and ultrasound imaging which may be diagnosticallymisleading but which can be considered to be within the realm ofnormal, non-malignant variants.
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
Fig. 5.61 Protocol for breast ultrasound. The examiner should always follow the same routine when performing breast ultrasound in order toobtain comparable results. In particular, the scans should cover breast regions that are not depicted in mammograms–most notably the recesses(axillary, clavicular, sternal, abdominal, and lateral) (a). Sonographic coverage considerably therefore exceeds mammographic coverage (b). Startingfrom the right axilla, the scans should proceed to the lateral, upper, medial, and lower quadrants in an overlapping pattern, and the ducts associatedwith each quadrant should be documented at approximately the 9-, 12-, 3-, and 6-o’clock positions. The same procedure is followed in the left breast,providing mirror-image information on the breast parenchyma and ensuring that all quadrants are examined twice. This consistent routine has for-ensic importance as well (c). Previous sonograms should be available for follow-ups to facilitate the prompt detection of pathologic changes andphysiologic variations in the glandular tissue (d). This is effectively accomplished in the digital age by using worklists supplied by equipment manu-facturers.
�������
����� ����������������
������
�����
������
��������������
������
�������
�����������
a Diagramof therecessesandtheareacoveredbymammography(brownshading).Mammogramscannot fullycover theaxillary recess (R. ax.), clav-icular recess (R. c.), sternal recess (R. st.), abdominal recess (R. abd.),or lat-eral recess (R. lat.). Some changes, especially in the sternal recess, are notmammographically detectable in obese women (see Fig. 4.24e, p. 50,Fig. 4.24 j, k, p. 347).
����� ������������� ����������������
������������
������������
����� !������
�����"������
����� !������
�����"������
�����#�����������#������
!
�
$%
!
�
$%
�������
������
������
�������
����������
������
�������
�������
b Ultrasound coverage of the breast parenchyma. The yellow-shadedarea represents the area accessible to ultrasound scanning. The ducts(2,3,4,5) and axilla (1) are indicated in red. These duct-oriented scanplanes through the breast parenchyma permit an accurate assessmentof physiologic responses to hormonal stimuli, etc.
Diagnosis with Ultrasound 157

A
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
a B b C c D d E e F f G g H h I i J j
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
Fig. 5.102 Gel bleed/implant type/implant rupture (?) in a 66-year-old woman. Both breasts underwent silicone implantation years before forcosmetic reasons. MRI raised suspicion of a left-sided implant rupture due to gel bleed (a). The implants were removed and examined.
a Fat-suppressed inversion-recovery MR se-quences show deep wrinkling of the implantsurfaces with silicone oil outside the implants(e.g., c–D/21–22). A linguine sign is not pres-ent (upper two pairs of images coronal, lowertwo pairs transverse).
b Mammography of the right implant undercompression shows numerous lines andstreaks caused by implant seams and surfacewrinkles (compare with d). Left: The implantwas imaged from the front. Right: The implantwas imaged from the side.
5 Early Detection and Appropriate Treatment222

1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
27
28
tTsSrRqQpPoOnNmMlLkK
Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
Fig. 5.102 Gel bleed/implant type/implant rupture. (continued)
c Appearance of the implants. Front views (above) show fibrous encapsu-lation of the left implant (reddish-white coating) while the right implantis clear. Portions of the outer shell are visible on the upper portion of theleft implant (N/26–27). Side views (below) show the outer shell “bakedonto” the left implant (reddish-yellow coating, N/21).
d Cut surface of the right implant (compare with c). Silicone has a uni-form greenish-yellow color and a relatively firm, nonfluid consistency.No cavity is present between the silicone and capsule.
e1, e2 View of the left implant. The pathologist cut a specimen from thereddish portion of the outer shell (fibrous encapsulation at Q–q/25).
e3 Histologic section from the outer shell (80× magnification) shows afirm, fiber-rich capsule with foreign body granulomas and silicone parti-cles (p.e. R–S/18, pink) (image courtesy of Hans-Helmut Dahm, Esslin-gen).
Question 1 on Fig. 5.102
What type of implants are these?
(a) Single-lumen implants
(b) Double-lumen implants
(c) Triple-lumen implants (gel/water/gel)
→ Answer on p. 378
Question 2 on Fig. 5.102
How would you interpret the MRI changes?
(a) Gel bleed
(b) Partial rupture of the outer implant shell
(c) Complete rupture of the whole implant
→ Answer on p. 378
" Fig. 5.102f–h
MRI: Breast Implants 223

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
IndexPage numbers in italics refer to figures.
A
accessory breasts 199acini 23, 25ACR see American College of Radiologyadenomaslactating see lactating adenomaspure 164
adenosis, breastmammography 113, 125, 355, 358sonography 163–164, 182–186see also sclerosing adenosis
ADH see atypical ductal hyperplasiaadolescent girlsbreast ultrasound 156, 159–160screening 109see also younger women
advanced breast cancer, locally 325–326,403, 403–404
agediagnosis of breast cancer 15, 15, 16precancerous lesions and 34–35radiation-induced cancer risk and 16, 16
alcohol consumption 9, 18, 33allergic reactions, radiolabeled colloid 311American College of Radiology (ACR)grades, breast density 8, 33, 98–99guidelines and standards 230, 231, 239
anaplastic carcinoma, diffuse 72, 73anatomy, breast 23, 24angiosarcoma see Kaposi sarcomaantiestrogen therapy 14, 34apocrine carcinoma 69screening pitfalls 140–141, 362, 362
arm edema 193, 197, 371prevention 307, 308
artifacts 133, 359, 359asymmetry, breast 46–47, 346athletic activities see sports activitiesatypical ductal hyperplasia (ADH)34–35, 36–37, 345, 345differential diagnosis 44–45, 51–52, 346fine-needle aspiration 237intracystic papilloma with 52–53, 347preoperative localization 301–303, 397treatment 46see also ductal carcinoma in situ
atypical lobular hyperplasia (ALH) 58axillamammography and ultrasound193–198, 194–200
physical examination 198
axillary lymph node dissection 21, 308after sentinel node biopsy312, 312–313, 398
alternative to 311morbidity 5, 307, 308, 308
axillary lymph node metastases 20, 21–22after refusal of chemotherapy278–279, 391
ductal carcinoma in situ 45follow-up examination for 335, 337, 407magnetic resonance imaging 202mammography 200, 372palpation 90sentinel lymph node biopsy 311ultrasound 195, 198, 199, 371, 371, 372
axillary lymph nodes 407, 408normal 195, 371sentinel biopsy see sentinel lymphnode biopsy
B
bilateral tumors 120–121, 356mammographic screening 139–140,362, 362
undetected 148–149, 365biopsy 3, 230–239complications 231, 234, 234–235cost comparisons 239, 251, 253, 254evaluation of different methods251–254, 254
magnetic resonance imaging (MRI)-guided 254–256, 255
open surgical 239, 256possibilities, limitations and risks256, 257–261, 383–384
during pregnancy 283procedure 231–235, 232–234stereotactic guidance see digitalstereotactic biopsy
ultrasound-guided 235–246see also core-needle biopsy; fine-needleaspiration biopsy; sentinel lymph nodebiopsy; vacuum biopsy
BIRADS classification 99, 156blood clot, intracystic 248, 382Bloom–Richardson grading system 74bone marrow biopsies 22bone scans, radionuclide 337, 340BRCA1 gene mutations 10, 14, 16–17BRCA2 gene mutations 10, 14, 16–17
breast awareness 15–16breast centers 4, 5–6quantitative criteria forwell-functioning 299
breast-conserving treatment 5ductal carcinoma in situ 46–51, 48–50,346, 346–347
lymphedema after 320, 400, 400–401breastfeeding 7, 33see also lactation
Breast Imaging Reporting and Data System(BIRADS) classification 99, 156
breast ultrasound 153–193
C
CAD see computer-aided detectioncalcifications 110after reduction mammoplasty321–322, 401
artifactual 133, 359, 359benign 137, 361, 361biopsy 69, 238, 249, 250, 256, 382BIRADS classification 99changes over time 41, 41, 42–43diagnostic difficulties 44, 44–45,46–47, 346
diagnostic tests 265, 385differential diagnosis 68–69ductal carcinoma in situ 37, 38–39,40, 40, 41–43
invasive carcinoma 62invasive ductal carcinoma 67, 67–69, 68lobular carcinoma in situ 39mixed tumors 72, 72preoperative localization 301–303, 397specimen radiography 305–307, 306
carcinoma in situ 34–35carcinoma of unknown primary(CUP syndrome) 202, 259, 384
carcinomatous lymphangitis 351male breast 296–297, 396
cardiovascular disease 11case presentations, mammographic110, 111–126
causes of breast cancer 7–19cerebral metastases 340, 405,409–410, 410
cheese cysts 283, 392, 392chemotherapy
427

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
locally advanced breast cancer325–326, 403, 403–404
chemotherapymetastatic breast cancer340, 342–344, 409
refusal of 278–279, 391chest radiographs 337chronic lymphocytic leukemia 194, 371clavicular recess, tumor located in146–147, 365
CNB see core-needle biopsycollodion, liquid 251, 252comedocarcinoma 67, 67male breast 296
complications, treatment-related313–314, 314–328
compression bandaging, post-biopsy231, 233, 234, 238, 249
computed tomography (CT)guided biopsy 254–256guided localization 304–305, 398lymph node metastases 407, 407
computer-aided detection (CAD), in digitalmammography 40, 69, 100
computer regulation thermography 78core-needle biopsy (CNB) 3, 231calcifications 69complications 231, 234, 234–235cost saving potential 239digital stereotactic (ST-CNB) 104,104–105, 232–234, 249–250, 250, 382
follow-up 336, 409indications 230magnetic resonance imaging (MRI)-guided 254–256
possibilities, limitations and risks258–259, 383–384, 384
ultrasound-guided 237–238versus other biopsy methods251–254, 254
coronary heart disease 90cost comparisonsbiopsy methods 239, 251, 253, 254follow-up regimens 338
cribriform ductal carcinoma 67CT see computed tomographycylindrical cell lesions of breast 35cysts, breast 31, 63, 247–248, 382“cheese” 283, 392, 392ductal carcinomas near to 66ductography 245, 380–381fine-needle aspiration biopsy 236malignant transformation 274, 389, 389management 69papillomas within see intracysticpapillomas
cytology 3, 235
D
DCIS see ductal carcinoma in situdecorin 33density, mammographic breast 98–99ACR grades 8, 33, 98–99BIRADS classification 99cancer risk and 8, 33–34, 98factors influencing 8–9, 33–34, 192hormone replacement therapy and12, 33–34
screening pitfalls 145, 365Wolfe classification 98
dermal appendages 237detective quantum efficiency (DQE) 101diagnostic tests/proceduresoptions available 78–256possibilities and limitations261, 262–274
dietary factors 8, 9diffuse carcinomas 63, 65, 65, 72–74digital mammography 1–3, 4, 100–105computer-aided detection (CAD) in40, 69, 100
full-field online 2, 101model of a diagnostic service 101–104,102, 103
screening unit 130–132, 131, 132storage plate system 100–101
digital photography 90digital stereotactic biopsy 249–251,250, 382comparative evaluation 251–254, 254complications 234–235systems 104, 104–105, 105technique 231–235, 232–234
digital stereotactic localization300, 301–305
digital tomosynthesis 4, 109diuretics 293–294, 396double reading, mammograms 109–110ductal carcinoma (invasive) 31, 65–69, 74calcifying 65, 67, 67–69, 68clinical presentation 66with enlarged axillary lymph nodes200, 372
hormone replacement therapy and 13locally advanced, treatment regi-men 325–326, 403, 403–404
missed diagnoses 150–153, 366–370,366–370
noncalcifying 65, 65–66, 66postoperative problems 319, 400screeningpitfalls 137,139–140,142–143,361, 361, 362, 362, 363–364, 364
stroma-rich (scirrhous) 71training mammograms 111–112, 114,117, 119, 124–126, 355, 358, 358
treatment considerations 56–57, 350
younger women 161–162, 281–282,392, 392
ductal carcinoma in situ (DCIS) 34, 37–58cribriform 40, 40diagnosis 35–37, 38–39, 40–44, 345differential diagnosis 44–45, 51–52, 54,346, 347
follow-up 62local recurrences 46, 62magnetic resonance imaging 40, 43–44,207, 373
mammographic screening 139–140,362, 362
monomorphic 40multicentric 45multifocal 45natural history 40–43, 41, 42–43,345, 345
numbers of women affected 34, 35papillary 40pleomorphic, usually large-cell 40preoperative localization 301–303, 397prognosis 58specimen radiography 306training mammograms 123, 357, 357treatment considerations 40, 45–51,48–57, 346, 346–349, 347–349
Van Nuys grading system 58younger women 275, 275–278, 390–391
ductal growth pattern, predominantly65–69
ductal hyperplasia (DH) 35atypical see atypical ductal hyperplasiadifferential diagnosis 51–52fine-needle aspiration biopsy 237
ductal papillomas see papillomas, ductalductectasia 28–29circumscribed focal, with associatedinflammation 266, 385
ductography 246, 381, 381–382fibrocystic change 187, 188hormone-related 159, 174, 175, 179, 191with plasma cell mastitis 262, 384–385with retained secretions 263, 385
ductography 241–246, 243–247, 380–382ductal carcinoma 66, 349technique 241, 242, 380terminal duct lobular units 27, 29
E
edema see arm edema; lymphedemaElston–Ellis grading system 74, 75endocrine influences see hormone-inducedchanges
endogenous agents 9environmental carcinogens 9
Index428

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
errors, treatment-related 313–314,314–328
estrogen-only therapy 3, 11, 12estrogen–progestin therapy, combined3, 11–12, 13
estrogens 9, 31European Federation of NeurologicalSocieties (EFNS) 340
European Protocol for the Quality Controlof the Physical and Technical Aspectsof Mammographic Screening (EPQC)96, 97
EUSOBI 230, 231EUSOMA 230examination, physical see physicalexamination
exocrine influences 8–9extensive intraductal component (EIC)48, 48–50, 63, 75
F
familial breast cancer 14diagnostic investigations 275–276,390, 390
males 295, 394see also high-risk women
family history, positive 14fat allograft, breast augmentation 224fat content, breast 8fat necrosisafter reduction mammoplasty317–318, 400
diagnostic evaluation 79–80, 265,350, 385
distinction from local recurrence 338on follow-up 337positron emission tomography229–230, 380
ferritin, elevated 140–141fibroadenomadifferential diagnosis 44–45, 70, 346fine-needle aspiration biopsy 237mistaken diagnosis 361, 361sonographic appearance 160, 163–164training mammograms 122–123, 356,356–357, 357
vacuum biopsy removal 238, 239,240–241, 380
younger women 277–278, 391, 391fibrocystic changesbreast ultrasound 175–176, 187–190with cysts and papillomas 245, 380,380–381
fine-needle aspiration biopsy (FNA)3, 231complications 231, 234–235cost saving potential 239
digital stereotactic (ST-FNA)104, 105, 233, 249
false-negatives 236, 237false-positives 237indications 230, 231, 235limitations and risks 257, 260–261,383, 384
palpable nodules 91, 236, 237pregnant women 237, 283supra- and infraclavicular nodes 198ultrasound-guided 235–237, 236versus other biopsy methods251–254, 254
flat epithelial atypia (FEA) 35FNA see fine-needle aspiration biopsyfolliculitis 81, 350follow-upcarcinoma in situ 62invasive carcinoma 328–341, 329–336,405–409
frostbite 86, 351, 352frozen section examination 300
G
galactocele 283–284, 392, 392galactorrhea, recurrent 52–54gamma camera 308–309, 309gamma probe 308, 309gel bleed, silicone 212, 220–221,222–224, 378
gene activity profiles 21General Electric (GE) Senograph 2000 Dsystem 101
General Electric (GE) Senovision system104, 104, 105, 105, 250
genetic factors, predisposing 13–17genetic testing 14–15Giotto Image MD digital full-fieldmammography system 101–102, 102
gonadotropin agonists 34gonadotropins 159grade, tumor 22, 74–77granulation tissue, postoperative 319, 400growth factors 8–9gynecomastia 291–294, 291–295, 298,394–396, 395, 397
H
hemangioma, congenital 79–80hematoma, post biopsy 234, 234–235,239, 251, 252, 383, 383sentinel lymph node biopsy and 311
hemorrhage, spontaneous 70–71hepatic ultrasound 337, 340Herceptin see trastuzumab
heterotopic breast tissue 198, 199high-risk women 14, 15–17diagnostic investigations275–276, 390, 390
magnetic resonance imaging 206, 373screening 14, 15–16, 109
histological classification, stagingand grading 74–77
histologyapocrine carcinoma 362atypical ductal hyperplasia 35–37, 52, 53breast implants 223, 224, 379ductal carcinoma 52, 57ductal carcinoma in situ 38, 39, 40ductal papilloma 241fat necrosis 230gynecomastia 395hemangiosarcoma 402hormone-related changes 34, 170, 172intracystic papilloma 53lactating adenoma 272, 287lactation nodule 286lobular carcinoma 209lobular carcinoma in situ 39, 61mastitis 270, 273pure adenoma 164sclerosing adenosis 281seborrheic keratosis/warts 79terminal duct lobular units 23, 25, 27, 30see also biopsy
hookwires, X-shaped 300hormonal therapy, adjuvant, ductalcarcinoma in situ 303, 397
hormone-induced changes 8–9, 31,156–157, 159–192
hormone replacement therapy (HRT)11–13, 18, 18breast ultrasound 157, 174, 176–177,182–185, 187–188
effects on breast density 12, 33–34magnetic resonance imaging and 202
Horner syndrome 87, 352–354, 352–354HRT see hormone replacement therapyhuman chorionic gonadotropin (HCG) 9
I
implants, breast 212–213, 217–226, 219fibrous encapsulation 218–219,223–224, 378
folds and wrinkles 218, 377follow-up and 337inflammatory exudate 226, 378, 379leaks 221, 225, 378ruptures 212–213, 218–224, 378trophic skin changes 221, 378
imprint specimen 3IMS Giotto system 104, 104–105
Index 429

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
incidence, breast cancer 1, 1, 13inflammatory carcinoma 72–74, 73biopsy 237diagnostic options 82–84, 350–351, 351diagnostic pitfalls 327–328, 405male breast 296–297, 396, 396postpartum 283, 289–290, 394, 394
inflammatory epithelial reactions 237inflammatory exudate 226, 378, 379infraclavicular fossa 90infraclavicular lymph node metastases198, 335, 407
infraclavicular lymph nodes 408inhomogeneities, breast 46–47, 346inoculation metastasis 231, 238, 300inspection, visual 78–91, 79–89, 350–355,351, 352–354follow-up 329–335, 406–407, 408possibilities and limitations261, 262–274
see also physical examinationinsulin metabolism 8interlobular stroma 2, 23, 25adolescent girls 160imaging appearances 26, 30pregnancy and lactation 168–169
interval cancers 2, 12, 108, 127authorʼs protocol 2, 108detection by inspection andpalpation 91
previous mammograms 147, 148–153,365–370, 366, 367, 368–369
radiodense breasts 69, 127training mammogram 115–116, 355see also missed cancers
interventional procedures 230–256intracystic carcinoma 69intracystic papillary carcinoma 37intracystic papillomas 247–248, 381, 382with focal ADH 52–53, 347
intraductal and intracystic proliferation237
intraductal component, extensivesee extensive intraductal component
intraductal debris 29, 243–244, 380intraductal papillomassee papillomas, ductal
intralobular stroma 2, 23, 25imaging appearances 27, 30proliferation 192
intrauterine device (IUD),hormone-releasing 173
invasive carcinoma 62–77diffuse spread see diffuse carcinomasgross morphology 63–65, 64histological classification, stagingand grading 74–77
mixed (lobulated-stellate-ductal)tumors 72
not otherwise specified (NOS) 63, 74predominantly ductal growth 65–69predominantly round to lobulatedgrowth 63, 64, 69–71, 70
predominantly stellate or spiculatedgrowth 71–72
see also specific types of carcinoma
J
Japan 9
K
Kaposi sarcoma 71, 325, 329, 402, 405keloids 210, 374Klinefelter syndrome 394
L
lactating adenomas 237diagnostic challenges 283, 286–287, 393diagnostic evaluation 271–272, 388
lactationbreast ultrasound 157, 168–171diagnostic challenges 283, 283–290,392, 392–394, 393, 394
fine-needle aspiration biopsy 237see also breastfeeding
lactation nodule 285–286, 393lactiferous ducts 23, 24, 28–29latissimus dorsi flap, breast reconstruction213
LCIS see lobular carcinoma in situleukemia, chronic lymphocytic 194, 371linguine sign, ruptured implants212, 218, 378
lipomas 341, 409axillary 279, 391subcutaneous 335, 337, 407
lipomatosis, lymph node 372lobes, mammary 23, 24, 155lobular carcinoma (invasive) 31, 74biopsy 237, 258, 260–261, 383, 384, 384diffuse 72, 73, 74fine-needle aspiration biopsy 237hormone replacement therapy and 13magnetic resonance imaging 202, 204,208–209, 372, 372–373, 374, 374–375
single-view mammography plusultrasound 107
stellate 71training mammograms 120–122, 356,356–357
lobular carcinoma in situ (LCIS) 34, 58–62diagnosis 59, 60, 60–61, 350
local recurrence and follow-up 62with microcalcifications 39treatment implications 62
lobular hyperplasia (LH) 58atypical (ALH) 58lactating, with inflammation285–286, 393
lobular intraepithelial neoplasia (LIN)58–62diagnosis 59, 60, 60–61, 350treatment implications 62
lobular neoplasia 58–62lobulated tumors 63, 64, 69–71, 70lobules, mammary 23, 24, 25, 155localization see preoperative localizationlocally advanced breast cancer 325–326,403, 403–404
local recurrence 299, 338after breast reconstruction 214, 376DCIS and LCIS 62distinction from scarring 336, 409magnetic resonance imaging 202positron emission tomography227–230, 379, 379
scarring mistaken for 332–333, 406, 406lumican 33Lumisys scanner 4lumps, breast see palpable breast noduleslymphadenopathy 194–196, 198, 371, 371lymphatic enlargement 193lymph drainage, manual 400lymphedemaarm see arm edemabreast 320, 400, 400–401, 404
lymph node biopsy, sentinel see sentinellymph node biopsy
lymph node metastases 20, 21–22follow-up examination for 335, 337, 407imaging 193–198, 194–200, 371, 372positron emission tomography 379, 379tumor staging 76
lymph nodes, regional 407, 408lymphography 311
M
maceration specimen 29macromastia 188–190magnetic resonance imaging (MRI) 2, 16,202–219, 204–211aesthetic breast reconstructionand implants 212–213, 217, 218,219, 220–222, 225–226
axilla 193, 211cerebral metastases 409, 410diffuse tumors 72, 74ductal carcinoma 57, 66, 66, 69
Index430

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
ductal carcinoma in situ 40, 43–44, 207,349, 373
follow-up 62, 328, 329, 332, 336,337, 405
guided breast interventions 202–203,254–256, 255
indications 109, 201–202inflammatory carcinoma 73–74integration into digital systems 102, 103lobulated tumors 70, 71local recurrence 338possibilities and limitations261, 262–274
postoperative use 202related overtreatment 275–276, 390sensitivity and specificity 106, 201–202stellate or spiculated tumors 71–72
magnetic resonance mammography (MRM)seemagnetic resonance imaging
magnification mammography 40, 41, 50,55, 59
male breast 291–295see also gynecomastia
male breast cancer 295, 296–298, 396,396–397
MammaCare 78mammography 91–147authorʼs policy 2, 109axillary 193–198, 194–200BIRADS classification 99breast densitysee density, mammographic breast
breast implants 212–213case presentations and interpretation110, 111–126
compression trauma 17conventional film-screen 100craniocaudal view 93–94, 94, 106diffuse lobular carcinoma 74digital see digital mammographydiscomfort 92double reading 109–110ductal carcinoma 66, 66, 68, 69ductal carcinoma in situ 38, 39, 40, 43follow-up 62, 328, 330–334, 406, 406future trends 105–109history of development 107–108hormone-induced changes and 31inflammatory carcinoma 73, 73–74lobular carcinoma in situ 39, 60, 60lobulated tumors 69, 71magnification 40, 41, 50, 55, 59male breast 291–292, 293–294,296–298, 396, 396
mediolateral (oblique) view95, 95–96, 106
palpable nodules 91, 117physician training 4possibilities and limitations 261,262–274
pregnant women 285–286, 393preoperative localization300, 301–305
procedure and organization 92–93quality control 93–97screening see screening, breast cancersensitivity and specificity 91single-view 1, 2, 4–5, 92,105–107, 109high-risk patients 16, 109plus sonography 1, 2, 5–6, 105–107,107, 193
versus two-view 105–107, 107standard protocol 91–92stellate or spiculated tumors 71–72terminal duct lobular units 23, 28two-viewrecommended use 109versus single-view 105–107, 107
versus ultrasound 106, 156, 157–158younger women 275
mastectomymorbidity related to 5scarring after subcutaneous293–294, 396
mastitis 211, 375, 375acute 264, 385granulomatous 267–270, 385–386,386–388
lymphocytoid 272–273, 388–389plasma cell 262, 384–385
mastodynia 90–91medullary carcinoma 69, 70differentiation from LCIS 59, 350
menopauseage at 9breast ultrasound 157, 174–176, 179–180hormone replacement therapysee hormone replacement therapy
symptom relief 11, 13TDLU changes 31
menstrual cyclebreast ultrasound 157, 163–167magnetic resonance imaging and 203numbers during lifetime 9TDLU changes 31, 32timing of breast examination 8, 91
metastasescutaneous 351secondary breast 71
metastatic breast carcinoma338, 340–341, 342–344, 409–410, 410
microcalcifications see calcificationsmicroradiography, terminal duct lobularunits 23, 26, 27–28, 30
milk, inspissated or caseated 283–284,392, 392
Million Women Study (MWS)3, 11, 12
Mirena 173missed cancers 12, 108, 128cases 147, 148–153, 365–370, 366, 367,368–369
over numerous biopsies 339, 409training mammogram 115–116, 355see also interval cancers
mixed (lobulated-stellate-ductal) tumors64, 72, 72
Model Project on Quality Assurance inBreast Diagnosis and Treatment 109
modulation transfer function 101mortality, breast cancer 1, 1, 7, 43MRI seemagnetic resonance imagingmucinous carcinoma 69biopsy 259, 384invading nipple 89, 355treatment-related errors 314–315,399, 399
mucocele of nipple 89, 355multifocal carcinomas 63breast reconstruction after216–217, 376
screening pitfalls 138, 142–143, 361,361, 363–364, 364
sentinel lymph node biopsy and311
N
National Cancer Institute, US 340neurinoma, axillary 198, 371neurodermatitis 81, 350neurological disorder 271–272, 388nevipapillomatous nevus cell 150, 366pigmented 141–142
nippleabsent 134, 360, 360deviation 88, 354, 354–355mucocele of 89, 355retraction 66, 296
nipple discharge 90, 172comedocarcinoma 67diagnostic tests 262–263, 384–385ductal carcinoma 54, 66ductography 245, 246, 246–247,380–382
male breast 294, 296papilloma removal 252–253postoperative 323, 401, 401
nipple–pectoral line (NPL) 93, 94nodules, palpable breastsee palpable breast nodules
not otherwise specified (NOS),invasive carcinoma 63, 74
Nottingham Prognostic Index 74, 75nutritional supplements 90
Index 431

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
O
obesity 8, 33oil cysts, postoperative 278–279, 391breast surgery for benign lesion316–317, 400
reduction mammoplasty 317–318, 400oral contraceptives 7–8, 9, 10, 18, 18breast ultrasound 165, 178–180
orange-peel skin 72–73, 73male breast 296–297, 396postoperative lymphedema 320, 400
osteoporosis 11ovarian cancer 14, 15ovulation inhibitors 7–8
P
PACS (picture archiving and communicationsystem) 100, 105
Paget carcinoma 37screening pitfalls 144, 364, 364
Paget disease 350, 355male breast 295
pain, breast 90–91diagnostic evaluation 271–272, 388
palpable breast nodules 69–70, 90, 91atypical ductal hyperplasia 36–37diagnostic evaluation 262–264, 266,268–270, 384–385, 386, 386–388
ductography 247–248fibrocystic change 175–176fine-needle aspiration biopsy 91, 236,237, 257, 383
follow-up 332–333, 406, 406hormone-related 168–169, 173magnetic resonance imaging205, 208–209, 373
male breast 291–292, 294, 296mammography 91, 117postpartum 283–284, 392, 392vacuum biopsy 238–239younger women 277–279, 281–282,391, 391, 392, 392
palpation, breast 78–91follow-up 335, 407, 408possibilities and limitations261, 262–274
see also physical examinationpapillary ductal carcinoma 67papillomasdigital imaging 243–244, 251ductal 243–244, 246–247, 380, 381–382,381–382
ductography 243–245, 246, 246–248,380–381
fine-needle aspiration 237intracystic see intracystic papillomas
macro- and microanatomy 241vacuum biopsy removal 238, 246, 251,252–253, 380, 383
papillomatous carcinoma 69papillomatous nevus cell nevus, benign150, 366
paraffin-block radiography 51, 307parasternal lymph nodes 408patent blue dye 308, 311peau d’orange see orange-peel skinpectoral lymph nodes 408perioperative management 299–314personalized medicine 21PET see positron emission tomographyPGMI quality rating system 93–95photographs, digital 90physical examination 78–91, 79–89,350–355, 351, 352–354optimal timing 8, 91possibilities and limitations261, 262–274
single-view mammography/ultrasoundwith 1, 106–107, 107
picture archiving and communicationsystem (PACS) 100, 105
pigmented nevi 141–142plasma cell mastitis 262, 384–385plasminogen activator inhibitor (PAI) 74pN classification 76polymastia completa 199polythelia 199positron emission tomography (PET)227, 227–230, 379, 379–380follow-up 337lymph node metastases 193, 407, 407postpartum and postoperativechanges 288, 393, 393
preoperative staging 73postirradiation changes 351postmenopausal womenbreast ultrasound 157, 174–188mammographic density and cancer risk33
postoperative changes 328–341precancerous lesions 34–35pregnancyafter breast surgery 277–278, 391, 391age at first 9breast changes 157, 168–170diagnostic challenges 283, 283–290,392, 392–394, 393, 394
fine-needle aspiration biopsy 237, 283tumor removal during 288, 393, 393
premenopausal women 275breast ultrasound 156–157, 161–173diagnosis of breast cancer 16magnetic resonance imaging 203mammographic density and cancer risk33
screening 6see also younger women
premenstrual syndrome, breast ultrasound157, 163–164, 166–167, 191–192
preoperative localization 299–305computed tomography (CT)-guided304–305, 398
mammography-guided 300, 301–305problems 314–315, 399, 399ultrasound-guided 304–305, 305, 398
progesterone 31, 159progestins 9, 11–12, 173prognostic factors 20–22prolactin 9, 34proliferation of breast parenchyma,grading 192
protective factors, breast cancer 9psoriasis 81, 350
Q
quality assurance, breast cancer follow-up337–338
quality control, mammography 93–97questions, from patients 3
R
radiation dosemammography 101, 102–103, 129pregnant woman 285–286, 393sentinel lymph node biopsy 311
radiation-induced breast cancer 16, 16radiation-induced telangiectasiawith fibrosis 330–331, 405
radiodermatitis 325, 402, 403radiographyductal carcinoma in situ 38, 39, 40invasive carcinoma types 62–65, 64lobular carcinoma in situ 39see also mammography
radiolabeled colloid 308, 311radionuclide bone scans 337, 340radiotherapycerebral metastases 410, 410ductal carcinoma in situ 45, 397high risk gene carriers 17Kaposi sarcoma after 329, 405lymph node metastases 312–313,398–399, 399
morbidity related to 5raloxifene 34reconstruction, breast 212–213, 214,216–217, 219, 376, 377follow-up after 337see also implants, breast
recurrence, local see local recurrence
Index432

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
reduction mammoplasty 87, 352–354,352–354postoperative problems 317–318,321–322, 400, 401
sentinel lymph node biopsy after 311REM (reticular erythematous mucinosis)syndrome 87, 352
residual tumor, after incomplete excision319, 324, 400, 402
retroareolar regionlobar anatomy 155palpation 90
risk assessment, breast cancer 15risk factors for breast cancer 7–19
S
sarcoidosis 196, 371sarcoma 71scalloped margins 63, 65scarringafter subcutaneous mastectomy293–294, 396
after tumor excision surgery 314–315,332–333, 337, 399, 399, 406, 406
distinction from local recurrence336, 409
scintigraphy, sentinel lymph node308–310, 309, 310, 312–313
scleroderma, circumscribed 82, 350sclerosing adenosis 118, 355biopsy 260–261, 384younger women 280–281, 392
screening, breast cancer 127–147combined sonographic/mammographic193
digital mammography unit130–132, 131, 132
follow-up investigations 265, 272–273,385, 388–389
intervals 92missed cases 147, 148–153, 365–370,366, 367, 368–369
new approach 1–2, 4–5, 129–130pitfalls 132–133, 133–147quality issues 3–4recommendations 109, 130risks and benefits 127–129women at high risk 14, 15–16, 109
seborrheic keratosis/warts 79, 350self-examination, breast 15–16, 16, 78Senograph 2000 D system, GeneralElectric 101
senology 108Senovision system, General Electric104, 104, 105, 105, 250
sentinel lymph node biopsy (SLNB)4, 22, 307–313, 398–399, 399
contraindications 311errors 310, 324, 402follow-up 337lobular carcinoma 383, 384results 311–313safety and complications 311technique 308–310, 309, 310, 312–313
seroma, postoperative 319, 323, 401, 401shingles 85, 350, 351, 351silicone, free intramammary injections212, 215, 376
silicone breast implants 212follow-up and 337gel bleed 212, 220–221, 222–224, 378inflammatory exudate 226, 378, 379leaks 221, 225, 378ruptures 212–213, 218–224, 378
skeletal examinations 337, 340skeletal metastasis 341, 409skin lesions 136, 360, 360smoking 10–11, 18snowstorm pattern, ruptured implants212, 219, 225, 378
soybean oil breast implants212, 218, 224, 377
soy products 9specimen radiography 305–307, 306core biopsies 232, 249ductal carcinoma in situ 38, 39, 51, 52,55, 57, 62
lobular carcinoma in situ 39, 60, 62specimen sonography 305spiculated tumors 63, 65, 70, 71–72sports activities 14, 17, 17–18, 33stellate tumors 63, 64, 65, 71–72stereotactic biopsy see digital stereotacticbiopsy
stereotactic localization, digital300, 301–305
stress, emotional 18supraclavicular fossa 90supraclavicular lymph node metastases198, 335, 407
supraclavicular lymph nodes 408Sure Touch System 1survival rates 22syncope, during interventional procedures234, 249–250
T
tamoxifen 14, 34TDLUs see terminal duct lobular unitsterminal duct lobular units (TDLUs) 3, 23adolescents 156, 159–161anatomy 23, 24–25, 155grading of proliferation 192histology 23, 25, 27, 30
hormone-induced changes 31, 32, 157,159, 163–192
imaging appearances 23, 26–30maturation 9, 10sonographic examination 155, 156,157–158
thermoablation probes 238thyroid disease 90tibolone 11, 12, 34, 187–188tick bite 135, 360, 360TNM classification 75–76tomosynthesis, digital 4, 109TRAM flap breast reconstruction213, 214, 376, 377
tranquilizers 90transverse rectus abdominis myocutaneousflap see TRAM flap
trastuzumab 6, 342–344, 409–410, 410trauma, breastas cause of breast cancer 17, 17–18granulomatous mastitis after 267–268,385–386
treatment, breast cancer 5, 5–6, 299–314metastatic disease 340–341preoperative localization 299–305reactions, complications and errors313–314, 314–328
triple-test protocol 235, 236trophic skin changes 221, 378tubular carcinomas 71, 237tubulolobular carcinoma, multifocal216–217, 376
tumorbiology 7–19doubling time 20–21growth rates 20–21, 69size 20–21, 22
tumor markerselevated levels 227–228, 335, 379measurement on follow-up 337
U
UICC staging system 76ultrasound, breast 153–193automated examination 1axillary 193–198, 194–200basic breast structures and variants156–193
BIRADS score 156breast density and 33, 192breast implants 212, 213diffuse tumors 72, 74ductal carcinoma 66, 66, 68, 69ductal carcinoma in situ 40early detection/screening 1–3, 153–154examination technique 154–156, 155follow-up 62, 328, 331, 336, 337
Index 433

Barth, Diagnosis of Breast Diseases (ISBN 978-3-13-143831-7), © 2010 Georg Thieme Verlag KG
ultrasoundfuture outlook 193hepatic 337, 340hormone-induced changes31, 32, 156–157
indications for 154inflammatory carcinoma 73, 73–74integration into digital systems 102, 103lobular carcinoma in situ 60, 61lobulated tumors 69–70, 71local recurrence 338male breast 292palpable nodules 91physiological parenchymal changes 2possibilities and limitations261, 262–274
sensitivity and specificity 106single-view mammography plus1, 2, 4–5, 105–107, 107, 193
specimen 305stellate or spiculated tumors 71–72terminal duct lobular units 23, 25–26,27–28, 30, 155, 156
versus mammography 106, 156,157–158
ultrasound-guided interventionalprocedures 235–246comparative evaluation 251–254, 254core needle biopsy 237–238fine-needle aspiration 235–237, 236vacuum biopsy 238–239, 240–241
ultrasound-guided localization 304–305,305, 398
undetected cancers seemissed cancersurokinase plasminogen activator (uPA)74
V
vacuum biopsy (VB) 3, 231calcifications 69complications 231, 234, 234–235cost saving potential 239digital stereotactic (D-VB) 104, 105,105, 233, 250–251
failures 230–231follow-up 336, 409indications 230, 238magnetic resonance imaging (MRI)-guided 254–256
papilloma removal 238, 246, 251,252–253, 380, 383
ultrasound-guided (SO-VB) 238–239,240–241
versus other biopsy methods251–254, 254
Van Nuys index 58vasovagal reactions, during interventionalprocedures 234, 249–250
VB see vacuum biopsyvenous stenosis, arm swelling193, 197, 371
visual inspection see inspection, visualvitamin A 8vitiligo 141–142, 363, 363
W
warts, skin 136, 360, 360Willebrand–von Jürgens syndrome 235wires, localization 299–300Womenʼs Health Initiative (WHI) study3, 11, 12
X
xenoestrogens 9X-shaped hookwires 300
Y
younger womenbreast cancer 16, 161–162breast ultrasound 156–157, 159–167diagnostic investigations 275, 275–282,390–392, 391, 392
magnetic resonance imaging 201, 203mammography 275see also adolescent girls; premenopausalwomen
Index434