Embed Size (px)
Citation preview

1304
Prehospital Thrombolysis: Beneficial Effects of Very Early Treatmenton Infarct Size and Left Ventricular Function
THOMAS LINDERER, MD, ROLF SCHRODER, MD, FACC, RICHARD ARNTZ, MD,MARIE-LUISE HEINEKING, MD, WERNER WUNDERLICH, MSc, KATHRIN KOHL, MS,FLORIAN FORYCKI, MD,* RUDOLF HENZGEN, MD,* JOACHIM WAGNER, MD*
Berlin, Germany
Ob*dws . The purpose of this study was to compare the edictsof very early ( :5 1 .5 h after symptom oelet) and later (>1 .5 up to4 h) thrombolytic therapy on infarct size, left ventricular functionand early mortality In patients with acute myocardial infarction .To start dwambolysis at the eadlest possible moment, it wasperformed In the prehospital setting. A cutoff time of 1,5 h was
vely stipulated .Shortening of ischemic time is crucial within the
lot 2 h. : reholgM thimmillolysis can reduce time to treatment andtuables very early initiation of therapy for many patients.
MAU& One hundred seventy patients received 30 mg ofanistreplase up to 4 h from symptom and by a mobile intensivecare unit physician. Infarct size was measured from cumulativerelease of alpha-hydroxybutyrate dehydrolewnl4 and left ventric .ular function was assessed by contrast anglograms 10 days afterthe infarction .
Intravenous administration of thrombolytic agents in acutemyocardial infarction has been shown to limit infarct size(1,2), preserve left ventricular function (l .-3) and improvesurvival (4-7) . Very early treatment has the potential tomaximize these beneficial effects (4,8-10) . However, rela-tively few patients are treated in the hospital within the 1st60 to 90 min of evolving infarction, Therefore, since the early190 (8,9) some centers have initiated thrombolytic therapyin the mobile intensive care unit or in the patient's homeControlled studies subsequently demonstrated the feasibil-ity, safety and significant time-saving value of prehospitalthrombolysis (11-15) . On the basis of the results of a pilotstudy (11), prehospital thrombolysis has been performed byemergency physicians in six of the seven mobile intensive
From the Division of Cardiology, Department of Medicine, KlinikumSttglitz, Free University of Berlin and the *First Department of Medicine,Krankeabars Neuk6lln, Berlin, Germany . Financial support for this studyand anistreplase were provided by SmithKline Beecham Pharmaceuticals,Munich, Germany.
Manuscript received July 7, 1992 ; revised manuscript received April 15,1993, accepted May 17, 1993,
Address fugntiogwknce . RoWSchrdder, MD, Division of Cardiology,Klindmm Steglitz, Free University Berlin, Hindenburgdamm 30, D-1000Berlin 45, Germany .
01993 by the American College of Cardiology
Results. The decision to treat on scene was correct in 98% ofpatients . There were no Weeding complications or deaths outsidethe hospital setting. t o 28 patients (17%) the isehemic process wasInterrupted . Findings with thrombolytic therapy initiated s:11 .5(96 patients) versus > 1 .5 h (74 patients) were the following: initialextent of epleardial injury, 1 .6 it 0.9 versus 1 .4 * 0.7 mV, p =N&, infarct size by cardiac enzyme release 646 it 634 versus
:t 712 Miter, p < 0 .05; ejection fraction 57 t 14% versus51 it 1316, p < 0.05; regionaldyssynevgic am 24 it 22 versus 33 t24 U, p < 0,05 ; 21-day mortality 1 of 96 versus S of 74 patients(1% vs. 7%, p < 0 .05) .
Conclusions . The data suggest that in evolving myocardialinfarction up to 4 h in duration, the start of thrombolytic therapyat sid h compared with >1.5 h limits infarct size, preserves leftventricular function and may save lives.
(J Am Coll Cardiol 1993,22 :1304-10)
JACC Vol. 22, No . 5November 1 , 1993 :1304-10
THROMBOLYSIS
care units on a routine basis since 1987 in West Berlin(16,17) .
When deliberating in 1988 how to prove benefit fromprehospital thrombolysis, we had to consider that a random-ized study comparing thrombolytic therapy initiated beforeor after hospital admission was no longer possible becausemost emergency physicians were already convinced of thisbenefit . It was therefore decided to compare the effects ofvery early versus later thrombolytic therapy by applyingstipulated cutoff time of 1 .5 h. Compared with in-hospitalinitiation of therapy, a much larger proportion of all patientswith acute myocardial infarction in Berlin had been candi-dates for, and actually received, very early thrombolytictherapy in the prehospital setting (16,17) . Thus, benefit fromvery early thrombolytic therapy may indirectly provideevidence of benefit from prehospital thrombolytic therapy .
Methods
This study was initiated in late 1988 by the KlinikumSteglitz and Krankenhaus Neuk6lin, serving two of sevenmobile intensive care units in Berlin, each staffed with 'ineemergency physician and two emergency medical techni-cians. Patients with symptoms typical for evolving myocar-dial infarction and diagnostic ST segment elevation on a
0735-10971931$6.00

JACC Vol. 22 . No . 5November 1, 1993 :1304-10
12-lead electrocardiogram (ECG) of at least 0 .1 mV in twolimb leads or 0 .2 mV in two contiguous chest leads wereeligible, provided that intravenous thrombolytic therapycould be initiated within 4 h of symptom onset . Exclusioncriteria were age >75 years and usual contraindications forthrombolytic therapy, in addition to cardiogenic shock, leftbundle branch block on the initial ECG, severe concomitantdiseases and inability to provide informed consent for throm-bolytic therapy in the mobile intensive care unit . In responseto the results of the Second international Study of InfarctSurvival (5), the initial upper age limit was abandoned for thelast 70 patients .
After recording the first ECG, nitroglycerin was admin-istered sublingually, a venous line inserted, appropriatecirculatory support given and morphine or diazepam injectedas needed . When ST elevation persisted on a second ECGrecording, blood samples were drawn, ant thrombolytictherapy was started . Clinical status, complications and timeintervals were recorded on a special report form .
Drug regimen . Anistreplase (30 mg) was injected intra-venously for 3 to S min, preceded by 100 mg of methyl-prednisolone. In the hospital, 250 mg of acetylsalicylic acidwas given orally or intravenously, followed by 100 mg orallydaily . Intravenous heparin was started after 6 h with a doseof 800 IU/h that was then adjusted to maintain the activatedpartial thromboplastin time at I .5 to 2 times normal . Heparininfusion was continued for at least 3 days .
Study end points . Prospectively defined primary studyend points were 1) complications and side effects of prehos-pital injection of 30 mg of anistreplase in the prehospitalsetting and during the hospital stay ; and 2) comparison ofenzyme-determined infarct size and left ventricular functionat day 10 in patients treated :51 .5 h and >1 .5 h aftersymptom onset. Secondary end points were 1) patency anddegree of stenosis at day 10, 2) incidence of reischemia andreinfarction and 3) 21-day mortality .
Electrocardiographic analysis . The size of the ischemicarea at risk was defined as the sum of ST segment elevationand depression 20 ms after the J point . The extent of theinitial epicardial injury was also quantified by counting thenumber of leads with ST elevation a.-O. I mV (18) .
Three patients with anterior myocardial infarction wereexcluded from ST segment measurements because of rightbundle branch block, and in another nine patients the initialECGs were not suitable for quantitative analysis owing tobaseline undulations or other artifacts .
Enzyme analysis. Serum enzyme activity was measuredby means of the alpha-hydroxybutyrate dehydrogenase(HBDH) opt . monotest and creatinine kinase (CK)-NAC akt .monotest, respectively (Boehringer-Mannheim) . The uppernormal value for HBDH is 140 Miter and 80 Miter for CK .The HBDH level was measured at baseline and 12, 24, 36, 48,60, 72, 96 and 120 h after the onset of symptoms. Thecumulative release of HBDH was determined centrally, aspreviously described by De Zwaan et al . (19). SignificantHBDH release was assumed only when the maximal value on
UNDERER ET AL .
1305PREHOSPITAL THROMBOLYSIS
the time-activity curve exceeded the baseline value by at least40% (e.g., baseline 100 IUAiter, maximum >140 IUAiter) .
Activity curves for HBDH could be evaluated in 151patients (including 22 patients without significant HBDHrelease) . In 19 patients, I-IBDH curves were either missing ornot evaluable (four early deaths, seven missing samples,eight hemolysis).
Creatine kinase serum activity was measured at baselineand at 14, 18 and 24 h . In addition, in 41 patients (alsoparticipating in a study on enzyme release) CK was mea-sured every 15 min for the 1st 4 h . Definite myocardialinfarction was defined by a twofold or greater increase in CKactivity above the upper limit of normal .
Quantitative anglographic analysis . Angiography was per-formed in 141 patients 10 ± 4 days after infarction . Angio-graphic studies were unavailable in 9 of 96 patients treatedwithin 90 min of symptom onset and in 20 of 74 treated later .Reasons were death in one patient treated early and fivepatients treated later and refusal or advanced age in symptom-free patients in 23 others without angiogrdphic studies .
The percent lumen diameter of the infarct-related coro-nary artery stenosis was measured with an automated edgedetection system (MIP-D, Kontron) . An infarct-related ar-tery was judged patent if the perfusion grade was Thrombol-ysis in Myocardial Infarction trial (TIMI) grade 3 .
Ventriculography was not performed in 1 patient becauseof renal failure and was not adequate for quantitative anal-ysis in 13 patients . Global ejection fraction and regional leftventricular wall motion abnormalities were evaluated aspreviously described (1,8) .
Protocol violation. Protocol was violated in three cases :one patient had cardiogenic shock and two patients in thelate treatment group had an earlier onset of infarction thanwas presumed on the scene (7 and 8 h, respectively) . Allthree patients were included in the analysis .
Another two patients had a clear misdiagnosis. Onepatient with anterior ST segment elevation had severe leftventricular hypertrophy from aortic valve stenosis and acutepulmonary edema; the other had inferior ST elevation due toacute alcoholic pancreatitis . Both suffered no harm fromprehospital thrombolytic therapy . They were excluded fromfurther analysis .
Statistical analysis. Group differences were assessed bythe separate variance estimate t or chi-square test for con-tinuous or dichotomous variables, respectively. Two-tailedp values < 0.05 were considered significant . In-hospitalmortality was subjected to stepwise multivariate logisticregression (BMDP LIZ). Variables entered were early andlate treatment, gender, age (560 and >60 years), history ofdiabetes, hypertension, previous myocardial infarction andlocation of index infarction (Table 1) . All variables areexpressed as mean value ± SD .
On the basis of the findings of time-dependent differencesin HBDH release in a previous study (20) for an assumedsignificant difference in HBDH release of 30% between theearly and the late treatment groups, tile necessary sample

1306
LINDERER ET AL .PREHOSPITAL THROMBOLYSIS
Table 1 . Baseline Characteristics
Values presented are mean value t SD or number (%) .
size was estimated to be -100. After inclusion of thisnumber of patients there was a significant difference inHBDH release but not for left ventricular function . Thus, itwas decided to prolong patient enrollment for another year .The study protocol was approved by the Ethical Committeeof the Klinikum Steglitz, Free University of Berlin .
Results
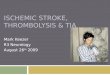
Patient chamcteristks (Tables 1 and 2) . Between late 1988and mid-1990, 170 patients were enrolled in the study . Onaverage, 25 min was needed to start thrombolytic therapy . In96 patients (56%), thrombolysis could be initiated within1 .5 h (in 50 within I h) (early treatment group) and in 74between >1 .5 and 4 h after symptom onset (late treatmentgroup) (Fig . 1). There was no difference in medical historyand index infarct location between the two groups . Therewere more women in the late treatment group . The meantime interval between onset of symptoms and emergency callwas 73 ± 49 min for women and 54 ± 48 min for men (p =103), Because the mean Me was 65 ± 10 years for womenand 59 :t I I years for men (p = 0.002), the average age washigher in the late treatment group . Of 13 patients >75 years
Table 2. Time Intervals
Values presented are mean value ± SD. ICU = intensive care unit (in thehospital) .
JACC Vol . 22, No . 5November 1 . 1993 :1304-10
old, 7 were women, and all were in the late treatment group .Of the six older men, three were treated early and three late .
Critical events (Table 3) . Prehospital ventricular fibrilla-tion occurred four times before and four times after injectionof anistreplase and was treated successfully by defibrillationin all patients. Symptomatic bradycardia in nine patients(severe sinus bradycardia in six and second- or third-degreeatrioventricular block in three) was managed by intravenousatropine and in three patients by temporary pacing . Hypo-tension after anistreplase injection, as previously defined inthe APSAC Intervention Mortality Study (6), occurred in 19patients . All received intravenous fluids, and catecholamineswere given additionally in 11 . Minor allergic reactions, suchas shivering and rash, occurred in three patients .
There were no bleeding complications or deaths outsidethe hospital setting . The 21-day mortality rate was 31% .One patient in the early treatment group and 5 in the latetreatment group (including I of the 13 patients >75 years old)died (p < 0 .05). Multivariate analysis revealed only time tothrombolytic therapy as a significant independent predictorof mortality at 21 days . Causes of death were cardiogenicshock in four patients, cardiac rupture in one and suddendeath on day 5 in one .
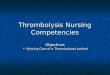
Interrupted iscbemic events (Table 4, Fig . 2). An enzymerelease typical for myocardial infarction was observed in 140patients . In 129, HBDH increased significantly, and in I Iwith insufficient HBDH samples, CK increased at leastfourfold. Of 30 patients without a significant increase incardiac enzymes, 28 had a persistent significant ST segmentelevation in the prehospital ECG . The CK time-activitycurve showed a slight increase not exceeding twice the upperlimit of normal in 19 patients and was classified as an"interrupted ischemic event ." It remained flat in nine andwas classified as a "probable interrupted ischemic event ."Two patients had only a slight ST segment elevation and noCK increase . Their condition was probably misdiagnosedbecause the final diagnosis remained unclear . Consideringalso the two clearly misdiagnosed and therefore excludedpatients (see Methods section on protocol violation), thedecision to initiate thrombolysis on the scene was correct in168 (98%) of 172 patients . Angiography was performed in 22patients, and 21 had coronary artery lesions . Only onepatient (one of the two with a probable misdiagnosis) hadapparently normal coronary arteries on angiography .
Infarct size (Table 5). The cumulative HBDH release was751 ± 669 lU/liter in all patients . The level was significantlylower in the early treatment group, even when only patientswith definite HBDH release were evaluated . The maximalCK value was only insignificantly lower in the early treat-ment group .
Angiographic findings at day 10 (Tables 6 to 8). Globaland regional ejection fraction were significantly improved inthe early treatment group . The overall patency rate was 71%(100 of 141 patients). In the early treatment group, there wasa trend toward a higher patency rate and a significantly largerproportion of residual stenosis <50% . The mean diameter
Time to Treatment
03 h(n = to
>15 h(n = 74) p Value
Age (yr) 58 ±11 64 ± 10 < 0 .001Female 16 (11) D (31) < 0 .05Infarct location
Anterior 45(47) 36 (49)Inferior 51(53) 38(51) NS
HistoryHypertension 27(28) 24(32) NSDiabetes 12(13) 12(l6) NSPrevious infarction 14(15) 17(23) NS
Time to Treatment
All Patients sl,5 h >1.5 hOnset of symptoms to
ambulance call (min)58 t 30 25 t 16 103 ± 43
Ambulance call to arrivalM patient's site (min)
12 6 12±6 13±7
Duration until anistreplaseinjection (min)
25 10 25 ± 11 26 ± 10
Transportation time toICU (min)
22 9 23 ± 10 22 t 8
Symptom onset to start of%mbolysis (h)
1.7 0.8 1 .0 ± 0.3 2 .5 ± 1 .1

JACC Vol. 22, No . 5November 1, 1993 :1304-00
Figure 1 . Frequency distribution of the timebetween onset of symptoms and start of throm-bolysis. Bars represent relative frequency dis-tribution ; solid circles represent cumulativefrequency distribution . Pts . = patients.
100Z Pta .
90
80 -1
70 -~
60 ~
50 -
40 -
30 -
20 -1
stenosis in patients with significant lesions was not different(59 ± 9% in the early treatment group and 58 ± 8% in the latetreatment group) .
In 'Table 7 data are provided with respect to patency ofthe infarct-related artery . Vessel patency was associatedwith a significantly better left ventricular function than thatassociated with persistent vessel occlusion, and there was astrong trend toward a smaller enzyme-determined infarctsize in the group with a patent infarct-related artery . Wheneurly and late treatment were compared in patients withpersistent patency, no significant difference in leftventricular function could be demonstrated, and the 24%difference in enzyme-determined infarct size was not statis-tically significant (Table 8) .
DiscussionIn Berlin, prehospital thrombolysis has been performed
routinely since 1987 (16,17). Most patients in the hospital
Table 3. Critical Events
10 _+
0 -Onset of pain totreatment [min]
UNDERER ET AL .
1307PREHOSPITAL THROMBOLYSiS
'30 s60 X 90 e-120 !!; 150 X180 0210 >210
because of acute myocardial infarction make use of themobile intensive care unit . More than one half are seen firstby the primary care physician outside the hospital settingwithin 1 .5 h from symptom onset and therefore are candi-dates for very early thrombolytic therapy (17) .
The present study was undertaken to prove the benefitobtained from very early thrombolysis by using a prospec-tively stipulated cutoff point of 1 .5 h. Enzyme-determinedinfarct sb e was significantly smaller, left ventricular func-tion at day 10 significantly better and early mortality signif-icantly lower in the early treatment group . As in previousstudies (9,10,12-14,21,22), thrombolysis in the prehospitalsetting was safe . As with in-hospital thrombolysis (23),treatment of a few misdiagnosed patients is unavoidablewhen overall benefit from speedy thrombolysis is to beachieved .
Infarct size and preservation of left ventricular function .Direct effects of thrombolytic therapy in terms of limitationof infarct size may be evaluated by quantitative measure-ments of cardiac enzyme release (1,2,10,20), whereas the useof maximal CK activity as an index of infarct size (14,22)may be less appropriate, because this measure is known tobe further elevated by effective thrombolysis (1) . Theamount of cumulative HBDH release in our study wassimilar to that in the active treatment groups of two larger
Table 4. Patients without Significant Increase ofCardiac Enzymes
Time to Treatment
:51 .5 h >1 .5 h
No . % No .
%
PrehospitalVentricular fibrillation 6 6 2
3Hypotension I 1 8
1Bradycardia 7 7 2
3Allergy 2 2 1
1In the hospitalDeath I I 5
7Reinfarction 4 4 4
5
Reischemia 8 8 5
6Bleeding 5 5 3
4Coronary angioplasty 25 26 19
26Coronary artery bypass grafting 10 10 9
12
Time to Treatment
S13 h >1 .5 h
No. No .
%
Total 18 19 12
16
Interrupted isehemic event 10 10 9
12
Probably interrupted ischemic event 7 7 2
2
Probable misdiagnosis 1 1 1

1308
LINDERER BT AL .PREHOSPITAL THROMBOLYSIS
controlled thrombolysis trials and clearly less than in thecorresponding control groups (2,20) . The difference in en-zyme-determined infarct size of 27% in favor of the earlytreatment group in the present study fits well with thetime-dependent decreasing magnitude of limitation of infarctsize in controlled studies, where data subdivided by timefrom symptom onset are provided for the 1st 3 to 4 h(1,11,20) .
The issue of preservation of left ventricular function ismore complex (24-27). Improved function several days afterthe acute event depends not only on direct salvage ofmyocardium but, in addition, on whether sustained patencyof the infarct-related artery is achieved, preventing infarctexpansion and left ventricular dilation (27-30) .
As evidenced by the data in Tables 7 and 8, improved left
T
S. Comparison of Infarct Size
CK - creatine kinase; HBDH = cumulative alpha-hydroxybutyratedeh release ; HBDH increased = cumulative HBDH release inpatients with significant enzyme increase; Pts = number of patients; BST =sum of ST segment elevation and depression in the prehospital electrocardio-gram; ST t = ST segment elevation.
0
! f
0
1
2
3
4
10
16
22
28
1 Start drowtng samples
(hrs]1 .3 hrs after onset of palm
JACC Vol. 22 . No . 5November 1 . 1993 :1304®10
Figure 2 . Serial creatine kinase (CPK) measurements ina patient with an interrupted ischemic event .
ventricular function at day 10 in the early treatment group isrelated mainly to a larger proportion of patients with a patentinfarct-related artery and to a lesser extent to actual salvageof ischemic myocardium. Studies in which thrombolysis wasinitiated before or after hospital admission also showedimproved left ventricular function when prehospital throm-bolysis was associated with a higher patency rate at the timeof later catheterization (10) but did not show significantdifferences when patency rates were the same (14,22) .
In-hospital mortality. There is evidence to suggest that,as in the present study, early in-hospital mortality is favor-ably influenced by salvage of ischemic myocardium(2,3,21,31), whereas left ventricular function after severaldays and, thus, later in-hospital and long-term mortalitydepend more on vessel patency (25,28,29) . Although greatcaution is necessary in interpreting conventionally signifi-
Table 6. Angiographic Findings
IRA = infarct-related artery ; Pts = number of patients ; TIMI = Throm-bolysis in Myocardial Infarction trial .
Time to Treatment
s1 .5 h >1 .5 h
Mean Valuet SD Pts
Mean Value± SD Pts
pValue
Angiography(day)
II t 5 87 10 t 3 54 NS
13ietaion fraction 57 t 14 81 51 t 13 46 < 0.05(0/0)
Dyssynergic area(U)
24 t 22 81 33 t 24 46 < 0.05
IRA TIMI flowgrade 3
65(75%) 35 (65%) NS
Stenosis <50% 14(16%) 20%) < 0.05
Time to Treatment
s1.5 h >1.S h
Mean Valuet SD Pts
Mean Valuet SD Pts
pValue
2:ST (mV) 1 .6 t 0.9 89 1 .4 t 0.7 69 NSST t (no, of
leads)5.1 t 1 .8 91 4 .7 t 1 .8 70 NS
HBDH (lU0iter) 646 t 634 85 8 6 t 712 66 c 0.05HBDH increased
(lU/liter)774 t 618 71 1.01 ± 672 58 < 0.05
Maximal CK(lulliter)
691 t 659 95 857 t 683 70 NS

JACC Vol. 22, No . 5November 1, 1993 :1304-10
Table 7. Analysis According to Patenc :' of theInfarct-Related Vessel
Abbreviations as in Tables 5 and 6.
cant mortality differences in small study groups, a findingsimilar to that in this study was previously reported forprehospital thrombolysis (21) and, moreover, a lower mor-tality in patients treated very early is supported by theresults of large mortality trials (4,5) .
Interrupted ischemic event . In patients with intermittentor incomplete coronary artery occlusion, thrombolysis maydissolve the threatening thrombus and thereby interrupt theischemic event (8) . In this regard, thrombolysis seems to bemore effective than anticoagulant therapy because 17% ofpatients in this study lacked enzyme release compared with7% of the "placebo" group in the Intravenous Streptokinasein Acute Myocardial Infarction trial (1) who received vigor-ous anticoagulant therapy . Because the incidence of inter-rupted ischemic events was not different between the earlyand late treatment groups (Table 4), the time delay may beless critical .
Limitations of the study . I) The early treatment groupcomprised younger patients and fewer women . This majorimbalance was caused by the fact that women with infarctiovare on average older than men, and delay in time to treat-ment is longer in women . The multivariate model s, :ectedonly time to treatment as an independent predictor ofmortality . Considering the small sample size, however, itmight be questioned whether any multivariate analysis will
Table 8 . Analysis of Patients With a Patent Infarct Vessel(TIMI 3) by Titne to Treatment
Abbreviations as in Tables 5 and 6 .
LINDERER ET AL .
1309PREHOSPITAL THROMBOLYSIS
adequately take such imbalance into account . Infarct size,which is the primary end point . is not related to age orgender, but, rather, to the initial ischemic area at risk . In thisrespect, the trend to a larger sum of initial ST segmentdeviations (Table 5) may reflect even potentially largerinfarcts at baseline (18,32) in the early treatment group .2) Angiographic data are less complete in the late (73%)compared with the early (91%) treatment group, which wasonly partially due to differences in mortality . Because therewas a trend toward higher HBDH release in patients in thelate treatment patients without angiography compared withthose with angiography (1,013 + 997 vs . 858 t 637), we haveno reason to assume that the poorer outcome in terms of leftventricular function in the late treatment group was due tothe exclusion of patients with smaller infarctions .
Conclusions . For direct salvage of jeopardized myocar-dium, shortening of ischemic time is critical within the 1st 2 h(11,15,20), whereas a I -h time gain may generate only marginalbenefit after 3 h . Therefore, the many patients who seekmedical attention very early (P) are entitled to prompt institu-tion of thrombolytic therapy. This can be effectively providedfor by prehospital initiation of thrombolytic therapy (17) . In theusual clinical setting, the in-hospital times to treatment stillcontinue to be long (15,33,34) . However, even if the in-hospitaltime delays are substantially shortened, there remains thetransportation time to hospital, which, especially in a ruralenvironment, may be of major importance .
We thank the medical, nursing and medical technician staff of both mobileintensive care units and hospital intensive care units for their help during thisstudy .
ReferencesI . Tlie 1SAM Study Group . A prospective trial of intravenous streptokinase
in acute myocardial infarction (ISAM) Mortality, morbidity, and infarctsize at 21 days . N Engl J Med 1986 .314 :1465-71 .
2 . Van de Werf F. Lessons from the European Cooperative RecombinantTissue-Type Plasminogen Activator (rt-PA) Versus Placebo Trial . J AmColl Cardiol 1988;12 :14A-9A
3 . White HD, Norris F ' Brown MA, et al . Effect of intravenous streptoki-nase on left ventricular function and early survival after acute myocardialinfarction . N Engl J Med 1987-,317 ;850-5.
4 . Gruppo Italiano per to Studio Della Streptochinasi Nell'infarto Mio-cardico (GISSI). Effectiveness of intravenous thrombolytic treatment inacute myocardial infarction . Lancet 1986 ;1 :397-402 .
5 . ISIS-2 (Second International Study of Infarct Survival) CollaborativeGroup . Randomized trial of intravenous streptokinase . oral aspirin . bath,or neither among 17,187 cases of suspected acute myocardial infarction :ISIS-2 . Lancet 1988 ;2 :349-60 .
6 . AIMS Trial Study Group . Effect of intravenous APSAC on mortality afteracute myocardial infarction : preliminary report of a placebo-controlledclinical trial . Lancet 1988l :545-9.
7 . Wilcox RG, von der Lippe G . Olsson CG, Jensen G, Skene AM, HamptonJR. Trial of tissue plasminogen activator for mortality reduction in acutemyocardial infarction, Lancet 1988 ;2 :525-30 .
8. Schroder R, Biamino G, von Leitner ER, et al . Intravenous short-terminfusion of streptokinase in acute myocardial infarction . Circulation1983 ;67 :536-48 .
9. Koren G, Weiss AT, Hasin Y, et al . Prevention of myocardial damage inacute myocardial ischemia by early treatment with intravenous streptoki-nase . N Engl J Med 1985 ;313 :1384-9 .
TIMI Flt . v Grade
TIMI 3 TIMI 0 to 2
Mean ± SD Pts Mean ± SD Pts p Value
Total patients 100 41EST (mV) 1 .5 t 0 .8 95 1 .5 t 0.8 37 0.96HBDH (IUAiter) 641 t 579 92 837 ± 663 41 0.09Ejection fraction 58 t 13 91 46 t 15 36 < 0.001
Dyssynergic area(U)
22 ± 21 91 41 ± 24 36 < 0.001
Time to Treatment
sl .5 h >1 .5 h
Mean t SD Pts Mean t SD Pis p Value
Total patieuts 65 35
EST (mV) 1 .6 ± 0.9 61 1 .5 ± 0 .7 34 0.69HBDH (IU/liter) 574 ± 593 57 751 ± 547 35 0.15
Ejection fraction 59 ± 13 67 56 ± 12 30 0 .29
Dyssynergic area(U)
21 ± 21 61 24 ± 19 30 0 .44

1 310
LINDI RER ET AL .PREHOSPITAL THROMBOL rSIS
10. McNeill Al, Cunningham SR, Flannery DJ, et al . A double blind placebocontrolled study of early and late administration of recombinant tissueplasminogen activator in acute myocardial infarction . Br Heart J 1989;61 :316-21 .
I I . Schrdder R . Importance of time window in thrombolytic treatment . In:Chamberlain DA . Julian DG . Sleight P. editors . The Management ofAcute Myocardial Ischemia . London: Chapman and Hall Medical, 1990:65-75 .
12. Castaigne AD, Hervi C, Duval-Moulin AM, et al . Prehospital use ofAPSAC: results of a placebo-controlled study . Am J Cardiol 1989;64:30A-3A .
13. EMIP Subcommittee. Potential time saving with prehospital interventionin acute my
infarction. Ear Heart J 1989 ;9:118-24 .14. Roth A, Bafbash GJ . Hod H, et al. Should thrombolytic therapy be
administered in the mobile intensive care unit in patients with evolvingmyocardial infarction? A pilot study. J Am Coil Cardiol 191;15 :912-6 .
15 . Weaver WD. Eisenbeerg MS . Martin JS. et al, Myocardial infarctionTd and Intervention Project-Phase 1: patient characteristics andfeasibility of prehospital initiation of thrombolytic therapy . J Am CollCardiol 190-0:92-31 .
16, Linker T, Arm HR, SchrOder R. Prkklinische Thrombolyse bei akutemM
infarct . Ditch Med Wochenschr 1991 :116 :18817 .17. Arntz HR, Stem R. hinderer T, Schrttder R . Efficiency of a physician .
operated mobile intensive care unit for prehospital thrombolysis in acutemyocardial infarction . Am J Cardiol 1992 :70:417-20,
I8 . Wilkms JL, Willems RJ . Willems GM, Aaitold AE. Van de Werf F .Versstraote M . Significance of initial ST segment elevation and depressionfar the management of thrombolytic therapy in acute myocardial infarc-tion, Circulation 1990;82 :1147-58 .
19. De Zwaan C, Willems GM, Vermeer F, et al . Enzyme tests in theevaluation of thmmbolysis in acute myocardial infarction . Br Heart J1 ' :59, 17543 .
20. Simoons ML, Serruys PW, van den Brand M, et al . Early thrombolysis inacute myocardial infarction : limitation of infarct size and improvedsurvival . J Am Coll Cardiol 1 :7 :717-28.
21 . Barbash GI, Roth A, Hod H . et al . Improved survival but not leftventricular function with early and prehospital treatment with tissueplasminogen activator in acute myocardial infarction . Am J Cardiol1990 ;66:261-6.
22. Schofer J, Buttner J . Geng G, et al . Prehospital thrombolysis in acutemyocardial infar^tion . Am J Cardiol 1'x;66:1429 .33,
23. Petch MC . Dangers of thrombolysis . Br Med J 1990;300:483 .24. Braunwald E . Myocardial reperfusion, limitation of infarct size, reduction
of left ventricular dysfunction, and improved survival . Should the para-digm be expanded? Circulation 1989 ;79:'41-4 .
2S . Schrdder R . Neuhaus KL, Linderer T, Btvggenrann T, Tehbe U . Weg-sc :ha ider K . Impact of late coronary artery reperfusiona on left ventricularfunction one month after acute myocardial infarction (results from theISAM Study) . Am J Cardiol I 9 ;64 :878-P4 .
26 . Topol F.J, Califf KM. Tissue plasminogen activator : why the backlash?J Am Coll Cardiol 1989 ;13 :1477-80.
27, Van de Werf F. Discrepancies between the effects of coronary reperfu-sion on survival and left ventricular function. Lancet 1989.1 :1367-9.
28 . Smalling RW, Fuentes F, Matthews MW, et al . Factors affecting outcomeof coronary rcpet1usion with intracoronary streptokinase in acute myo-cardial infarction. Am J Cardiol 1987 :59:505-12 .
29 . Topol EJ, Califf RM . George BS, Kerciakes DJ, Lee KL, for the TAMIStudy Group . Insights derived from the Thrombolysis and Angioplasty inMyocardial Infarction (TAM[) trials . J Am Coll Cardiol 1988 ;12 ; 24A-31 A .
30. 1 'efler MA . Lamas GA . Vnughan DE, Parisi AF, Braunwald E . Effect ofcaptopril on progressive ventricular dilatation after anterior myocardialinfarction . N Engl J Med 1988:319:80-6 .
31 ~ Meinertz T . Kasper W, Sclaumaa:her M, Just HJ . The German MulticenterTrial of Anisoylated Plasminogen Streptokinase Activator Complex Ver .sus Heparin for Acute Myocardial Infarction . Am J Cardiol 1988-,62 :347-51 .
32. Schr6der R, Linderer T. Brlggcmann T . Neuhaus KL . Tebbe U . Weg-scheider K. Controversial indications . Rationale for thrombolysis: laterthan 4-6 h from symptom onset, and in patients with smaller myocardialinfarction . Eur Heart J 1941);11 :19-28 .
33 . Dcoarey AJ, Michelson EL, Weber FJ . Dreifus LS. Thrombolytic therapyof acute myocardial infarction : emerging challenge of implementation.J Am Coll Cardiol 1987 ;10 :1357-60 .
34. Kerciakes DJ . Weaver WD, Anderson JL, et al . 'Time delays in thediagnosis and treatment from acute myocardial infarction : a tale of eightcities . Report from the Pre-hospital Study Group and the Cincinnati HeartProject . Am Hear J 1990 ;120 :773-80.
JACt' Vol . 22 . No. SNovember 1 . 1993 :1304-10