Embed Size (px)
Citation preview

Ultrasound Obstet Gynecol 2010; 35: 35–41Published online 17 December 2009 in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/uog.7489
Prenatal diagnosis and outcome of partial agenesisand hypoplasia of the corpus callosum
T. GHI*, A. CARLETTI*, E. CONTRO*, E. CERA*, P. FALCO*, G. TAGLIAVINI*,L. MICHELACCI*, G. TANI†, A. YOUSSEF*, P. BONASONI‡, N. RIZZO*, G. PELUSI*and G. PILU*Departments of *Obstetrics and Gynecology, †Paediatric Radiology and ‡Pathology, University of Bologna, Bologna, Italy
KEYWORDS: callosal hypoplasia; corpus callosum; partial agenesis; prenatal diagnosis; ultrasound
ABSTRACT
Objective To present antenatal sonographic findings andoutcome of fetuses with hypoplasia or partial agenesis ofthe corpus callosum.
Methods The database of our ultrasound laboratory wassearched retrospectively for cases of hypoplasia or partialagenesis of the corpus callosum suspected at antenatalneurosonography between 1998 and 2008 and confirmedby pathology or postnatal neuroimaging. In survivinginfants, clinical follow-up had been arranged to assessneurodevelopmental outcome.
Results Nineteen fetuses with callosal underdevelopmentwere identified at a median gestational age of 22 (range,21–33) weeks and confirmed at follow-up, including 14with partial agenesis and five with hypoplasia. Amongthe 14 fetuses with partial agenesis, there were additionalbrain findings in 10, including two with absent cavumsepti pellucidi, four with mild isolated ventriculomegalyand four with cerebellar abnormalities, two of whichalso had ventriculomegaly. Pregnancy was terminatedelectively in seven of the cases with partial agenesis andthere was one neonatal death. Among the six survivinginfants, neurodevelopmental outcome was appropriate forage in three at follow up, including two cases with isolatedpartial agenesis of the corpus callosum. Among the fivefetuses with prenatally diagnosed callosal hypoplasia,additional anomalies were present in four. Two caseswere terminated electively and three were alive at thetime of writing, with a median age of 3 years. Amongthem, apparently normal neurological development wasobserved in only one case.
Conclusions An antenatal diagnosis of callosal underde-velopment is possible by expert sonography. There is often
association with other major anomalies. However, even infetuses with apparently isolated findings, the prognosis isuncertain. Copyright 2009 ISUOG. Published by JohnWiley & Sons, Ltd.
INTRODUCTION
The corpus callosum is the major junction betweenthe cerebral hemispheres, extending from the frontallobe anteriorly to above the quadrigeminal plateposteriorly. Congenital anomalies of the corpus callosumare commonly associated with other malformations,aneuploidies or genetic syndromes1–4. Furthermore, evenin cases with isolated callosal anomaly there is a highrisk of abnormal neurodevelopment5–7. Among callosalabnormalities, agenesis of the corpus callosum, whichcan be partial or complete, and callosal hypoplasia areincluded.
Prenatal diagnosis of complete callosal agenesis isfeasible from the midtrimester onwards by expertsonography. At two-dimensional (2D) ultrasound in theaxial view of the fetal head, suspicious findings areabsent cavum septi pellucidi and teardrop configurationof the lateral ventricles with possible ventriculomegaly.Antenatal diagnosis is based upon the non-visualizationof the corpus callosum at transfontanellar ultrasound ineither the sagittal or the coronal plane8,9.
More subtle findings, such as hypoplasia and partialagenesis of the corpus callosum, may also be recognizedantenatally7,10–12. In these cases sonographic diagnosisis extremely difficult because the corpus callosum isdetectable and, while it is atypical in appearance, theaxial view of the fetal head is often unremarkable. Incases of callosal hypoplasia or partial agenesis ultrasound
Correspondence to: Dr T. Ghi, University of Bologna - Obstetrics and Gynecology, Policlinico S.Orsola - Malpighi via Massarenti 13,Bologna 40100, Italy (e-mail: [email protected])
Accepted: 10 June 2009
Copyright 2009 ISUOG. Published by John Wiley & Sons, Ltd. ORIGINAL PAPER

36 Ghi et al.
diagnosis is based, respectively, on the demonstrationof a decreased thickness of the corpus callosum ora decreased thickness and abnormal shape, in themedian view. Normative charts for fetal corpus callosalbiometry have been established and are of criticalimportance in assisting the sonographer during subjectiveassessment to confirm either corpus callosal integrity orits underdevelopment13,14. Prognostic implications forfetuses with partial agenesis seem to be similar to thosefor fetuses with total agenesis1,7,15, although some claimthere to be a better outcome in the former group6. Prenataldiagnosis of callosal partial agenesis7,10,11 or hypoplasia12
has in fact been reported rarely. We therefore present theantenatal sonographic findings and outcome of a groupof fetuses in which callosal hypoplasia or partial agenesiswas recognized prenatally.
PATIENTS AND METHODS
The database of our ultrasound laboratory was searchedretrospectively for cases of hypoplasia or partial agenesisof the corpus callosum suspected at antenatal sonographybetween 1998 and 2008. Ultrasound investigationwas carried out using AU5 or Technos (Esaote,Genoa, Italy) or Voluson 730 Pro/Exp (GE Healthcare,Milwaukee, WI, USA) ultrasound machines equipped withmultifrequency transabdominal and transvaginal probes.In some cases ultrasound examination was supported bythree-dimensional (3D) and 4D technology. Accordingto our standard policy, fetal head examination wasperformed transabdominally in the axial, coronal andsagittal planes and the corpus callosum was visualizedin the median plane to permit its length and thicknessto be measured and compared with the reference charts.Partial agenesis was suspected when the corpus callosumappeared to be shaped abnormally and to be short forgestational age posteriorly and was not overlying thequadrigeminal plate. Hypoplasia was suspected whenthe corpus callosum appeared to be thin for gestationalage but of normal length. In these suspected cases, themaximum length of the corpus callosum and its widestthickness at the level of the body were measured, andif the callosal length or thickness was below the 10th
centile for gestational age of the reference charts13,14 aconclusive diagnosis of partial agenesis or hypoplasiaof the corpus callosum, respectively, was established.In cephalic-presenting fetuses whose corpus callosumwas suspicious or unclear in appearance, multiplanarneurosonography was further performed transvaginallyusing a high-frequency probe (7.5–10 MHz). In abnormalcases a more detailed scan of the fetal head was performed,including investigation of the aspect of the cavum septipellucidi and the lateral ventricles. Furthermore, colorflow mapping was used to visualize the course ofthe pericallosal arteries. A careful survey of the entirefetal anatomy including fetal echocardiography was thenperformed to rule out associated intra- or extracranialanomalies. Fetal karyotyping was offered if this had notbeen assessed previously. From 2001 onwards, antenatal
magnetic resonance imaging (MRI) was offered to confirmthe sonographic findings. This was carried out usinga 1.5T system (Signa LX, GE Healthcare) with thefetal brain being examined in a multiplanar fashion bya sequence of T2-weighted, single-shot fast-spin echoimages. The MRI examination was carried out by apediatric neuroradiologist (G.T.) assisted by one of thesonographers.
When a fetal callosal anomaly was suspected, a detailedpostnatal evaluation was carried out in order to confirmthe antenatal findings. If pregnancy termination orpostnatal death occurred, necropsy was carried out by anexpert in perinatal pathology (P.B.). In surviving infants,postnatal neuroimaging techniques such as computedtomography and MRI were used to verify antenatal brainfindings and neuropediatric follow-up was arranged inorder to assess neurodevelopmental outcome.
RESULTS
During the study period 19 fetuses with callosalunderdevelopment were identified antenatally, at amedian gestational age of 22 (range, 21–33) weeks,and confirmed at follow-up by pathology or postnatalneuroimaging, including 14 with partial agenesis and fivewith hypoplasia. Most of these cases had been referredto our laboratory due to suspicious findings at routineultrasound examination. In a few of them a detailedevaluation in our center had been arranged due toan increased risk for congenital anomalies or obstetriccomplications in the current pregnancy. Sonographicfindings and outcome of all 19 cases are summarizedin Table 1.
Among the 14 fetuses with partial agenesis, therewere additional brain findings in 10, including twowith absent cavum septi pellucidi, four with mild tear-drop isolated ventriculomegaly (< 15 mm), and fourwith abnormalities of the cerebellum-posterior fossacomplex, two of which also had ventriculomegaly. Infour fetuses there was also hypoplasia of the remainingportion of the corpus callosum which was associatedwith absence of the splenium. Of these, three werediagnosed prior to fetal viability and one was recognizedat 33 weeks of gestation in a patient who had beenreferred on suspicion of fetal ventriculomegaly. Followingsonographic diagnosis, fetal brain MRI was performed infour cases and in all it confirmed the ultrasound findings.In the whole group, additional extracranial anomalieswere recognized in two fetuses, including one with astructural heart defect who was diagnosed postnatallywith Cri du Chat syndrome (5 p- deletion) and onewith apparently isolated polyhydramnios which turnedout postnatally to be caused by choanal atresia in thesetting of CHARGE (callosal hypoplasia, choanal atresia,micrognathia) syndrome.
Of the 14 cases with prenatally diagnosed partialagenesis of the corpus callosum, the pregnancy wasterminated electively in half, including five cases with
Copyright 2009 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2010; 35: 35–41.

Partial agenesis and hypoplasia of the corpus callosum 37
Tab
le1
Sum
mar
yof
sono
grap
hic
findi
ngs
and
outc
ome
in19
case
sw
ith
callo
salp
arti
alag
enes
isor
hypo
plas
ia
Cas
eW
eek
Indi
cati
onfo
rso
nogr
aphy
Cor
pus
callo
sum
/CSP
appe
aran
ceA
ddit
iona
lson
ogra
phic
findi
ngs
Out
com
e
Par
tial
agen
esis
ofth
eco
rpus
callo
sum
122
Ven
tric
ulom
egal
yM
issi
ngsp
leni
um,C
SPpr
esen
tT
eard
rop-
shap
edve
ntri
cles
,mild
vent
ricu
lom
egal
yL
ive
birt
h,at
10ye
ars
deve
lope
dm
ulti
ple
intr
acra
nial
lipom
asan
dse
izur
es2
21V
entr
icul
omeg
aly
Mis
sing
sple
nium
,CSP
pres
ent
Ven
tric
ulom
egal
y,D
andy
–Wal
ker
com
plex
TO
P3
22V
entr
icul
omeg
aly
Mis
sing
sple
nium
,CSP
pres
ent
Ven
tric
ulom
egal
y,D
andy
–Wal
ker
com
plex
TO
P4
22V
entr
icul
omeg
aly
Mis
sing
sple
nium
,CSP
pres
ent
Tea
rdro
p-sh
aped
vent
ricl
es,m
ildve
ntri
culo
meg
aly
TO
P
521
Ven
tric
ulom
egal
yM
issi
ngsp
leni
um,C
SPpr
esen
tT
eard
rop-
shap
edve
ntri
cles
,mild
vent
ricu
lom
egal
yT
OP
621
Prev
ious
pret
erm
birt
hM
issi
ngsp
leni
um,C
SPpr
esen
tN
one
Liv
ebi
rth,
norm
alde
velo
pmen
tat
8ye
ars
722
Abn
orm
alca
rdia
cfin
ding
sM
issi
ngsp
leni
um,C
SPpr
esen
tD
OR
V,I
UG
R,h
ypop
last
icce
rebe
llum
Liv
ebi
rth,
chro
mos
omal
anom
aly
(5p-
),ne
onat
alde
ath
at1
mon
th8
21C
onsa
ngui
neit
yM
issi
ngsp
leni
um,C
SPpr
esen
tN
one
TO
P9
21D
rug
cons
umpt
ion
Mis
sing
sple
nium
,<th
ickn
ess
ofC
C,
Non
eT
OP
CSP
abse
nt10
22Po
lyhy
dram
nios
Mis
sing
sple
nium
,<th
ickn
ess
ofC
C,
Poly
hydr
amni
osL
ive
birt
h,at
1ye
arC
HA
RG
E(c
allo
sal
CSP
abse
nthy
popl
asia
,cho
anal
atre
sia,
mic
rogn
athi
a)sy
ndro
me,
men
tald
elay
1121
Enl
arge
dci
ster
nam
agna
Mis
sing
sple
nium
,<th
ickn
ess
ofC
C,
Dan
dy–W
alke
rco
mpl
exL
ive
birt
h,at
3ye
ars
mot
orde
velo
pmen
tde
lay
CSP
pres
ent
1233
Ven
tric
ulom
egal
yM
issi
ngsp
leni
um,<
thic
knes
sof
CC
,T
eard
rop-
shap
edve
ntri
cles
,L
ive
birt
h,no
rmal
deve
lopm
ent
at2
year
sC
SPpr
esen
tve
ntri
culo
meg
aly
1321
Prev
ious
preg
nanc
yw
ith
IUG
RM
issi
ngsp
leni
um,C
SPpr
esen
tN
one
Liv
ebi
rth,
norm
alde
velo
pmen
tat
3ye
ars
1423
Incr
ease
dnu
chal
tran
sluc
ency
thic
knes
sM
issi
ngsp
leni
um,C
SPpr
esen
tN
one
TO
P
Hyp
opla
sia
ofth
eco
rpus
callo
sum
1533
Hyd
rone
phro
sis
<th
ickn
ess
ofC
C,
Poly
hydr
amni
os,u
nila
tera
lren
alag
enes
is,
Liv
ebi
rth,
esop
hage
alat
resi
a,ve
scic
oure
tera
lC
SPpr
esen
thy
drou
rete
rone
phro
sis
and
meg
acys
tis
reflu
x,no
rmal
deve
lopm
ent
at8
year
s16
21M
ater
nald
iabe
tes
<th
ickn
ess
ofC
C,
Non
eT
OP
CSP
smal
l17
32R
educ
edcr
ania
lcir
cum
fere
nce
<th
ickn
ess
ofC
C,
Hem
imeg
alen
ceph
aly
Liv
ebi
rth,
at3
year
sse
vere
CSP
pres
ent
neur
odev
elop
men
tald
elay
and
seiz
ures
1832
Con
sang
uine
ity
<th
ickn
ess
ofC
C,
Ven
tric
ulom
egal
y,te
tral
ogy
ofFa
llot,
Liv
ebi
rth,
at3
year
sPe
na-S
hoke
irty
pe2
CSP
pres
ent
unila
tera
lren
alag
enes
issy
ndro
me
1922
Susp
icio
nof
CH
D<
thic
knes
sof
CC
,Si
ngle
umbi
lical
arte
ry,h
eart
righ
t–le
ftT
OP
CSP
pres
ent
vent
ricu
lar
disp
ropo
rtio
n,IU
GR
<,d
ecre
ased
;CC
,cor
pus
callo
sum
;CH
D,c
onge
nita
lhea
rtdi
seas
e;C
SP,c
avum
sept
ipel
luci
di;D
OR
V,d
oubl
eou
tlet
righ
tve
ntri
cle;
IUG
R,i
ntra
uter
ine
grow
thre
stri
ctio
n;T
OP,
term
inat
ion
ofpr
egna
ncy.
Copyright 2009 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2010; 35: 35–41.

38 Ghi et al.
additional brain findings (two with abnormalities ofthe cerebellum–posterior fossa complex, one withabsent cavum septi pellucidi and two with isolatedventriculomegaly). Of the remaining seven fetuses, sixwere delivered near term and were alive at the time ofwriting, with a median age of 3 (range, 1–10) years andthe one suffering from 5p- deletion died shortly after birth.Among the six surviving infants, neurodevelopmentaloutcome was reported to be appropriate for age in three,while there were neurological abnormalities present in theother three, including one case with mild motor delayassociated with Dandy–Walker complex, one case withseizures due to multiple intracranial lipomas detected afterbirth and one case with severe mental retardation in whomCHARGE syndrome was recognized postnatally becauseof associated findings (choanal atresia, micrognathia). Inthe two cases with isolated partial agenesis of the corpuscallosum in which the pregnancy was not terminated,neurological outcome of the infant was reported to benormal at follow-up (one at 3 and one at 8 years).
Of the five fetuses with prenatally diagnosed callosalhypoplasia, there were additional findings in four,including a case with hemimegalencephaly and three withmultiple anomalies involving either the brain or othersystems (one with ventriculomegaly, tetralogy of Fallotand unilateral renal agenesis, one with esophageal atresiaand one with single umbilical artery, congenital heartdisease and intrauterine growth restriction). Notably,the cavum septi pellucidi appeared normal in the fourcases with additional findings and was small in theonly case in which callosal hypoplasia appeared isolated.Fetal MRI was additionally performed in three cases andconfirmed the ultrasound findings. Of the whole group,two cases including the one with no additional findingswere detected in the second trimester and were terminatedelectively. The other three were diagnosed sonographicallyin the third trimester; these were delivered near term andwere alive at the time of writing, with a median age of3 (range, 3–8) years. Among them, apparently normalneurological development was observed only in theinfant with esophageal atresia, who underwent surgicalrepair. Both the infant with hemimegalencephaly and theone with tetralogy of Fallot showed severe neurologicalimpairment at follow-up. In the latter, Pena–Shokeir type2 syndrome was diagnosed after birth.
DISCUSSION
The corpus callosum may be imaged antenatally by tar-geted multiplanar sonography from the midtrimester8,9.Focusing the ultrasound beam on the sagittal suture of thefetal head, the entire length of the corpus callosum maybe displayed as a sonolucent band demarcated superiorlyand inferiorly by two echogenic lines (Figure 1). Recentlythe development of 3D ultrasound has provided severaladvantages in the study of the fetal central nervous sys-tem (CNS). Thanks to volume sonography, starting froman axial section of the fetal head, which is usually easyto obtain, it is possible to achieve a median view of the
brain and to visualize antenatally anomalies of the corpuscallosum or other midline structures. Moreover, since 3Dultrasound has been implemented by the static volumecontrast imaging (VCI) modality, the image quality ofreconstructed planes such as the sagittal one has greatlyimproved16,17.
On this basis prenatal assessment of the corpuscallosum has become part of expert fetal scanning,evaluation involving not only its presence, but also itssize and aspect. At prenatal ultrasound a fully developedcorpus callosum is seen to overlay the quadrigeminalplate of the mesencephalon in the median view of thefetal brain. However, when dealing with the suspicionof callosal underdevelopment, either partial agenesisor hypoplasia, normative charts of its length andthickness are available for comparison13,14. If thesebiometric parameters are below the normal range anobjective diagnosis of callosal underdevelopment maybe established prenatally. Moreover, a deviation in thenormal course of the pericallosal arteries is reported to bean additional sign of corpus callosal partial agenesis11.In such cases the arteries closely follow the contourof the corpus callosum at its anterior part (the genuand the body), but take an upward direction at thelevel of the missing splenium. As previously suggested11,those indirect sonographic findings, which are commonlyreported in fetuses with complete callosal agenesis, wereencountered inconsistently in this series of fetuses withpartial agenesis or hypoplasia. A small or absent cavumsepti pellucidi or colpocephaly were in fact detectableonly in a small proportion of our cases, and we failedto demonstrate the other indirect signs of absent corpuscallosum, such as an enlarged and upward displacedthird ventricle, radial appearance of the medial sulciand incomplete cingulate gyrus11. A likely explanationis that in cases of absent corpus callosum most of thesefindings are due to defective or abnormally orientedinterhemispheric bundles, whereas in cases with partialagenesis or hypoplasia, normal appearance of the cavumsepti pellucidi or the lateral ventricles may reflect a minordisruption of the midline fibers.
Partial agenesis of the corpus callosum results from anarrest of growth which occurs between 12 and 18 weeks ofgestation and usually involves the dorsal part or splenium,with the more anterior callosal segments being preserved.Indeed, callosal ontogenesis is currently believed to startin the 11th week at the level of the anterior portion ofthe body. From there development of the entire corpuscallosum takes place in a bidirectional fashion, frontwardto form the genu and the rostrum and backward tocomplete the body and the splenium18. Whether callosalpartial agenesis represents a true malformation or isthe consequence of a disruptive event is uncertain6.An association with interhemispheric arachnoid cyst,holoprosencephaly, asymmetric ventriculomegaly andmigration disorders is reported19,20.
Prenatal diagnosis of fetal callosal underdevelopmentremains a difficult task with only few cases of partialagenesis reported in the literature10,11,20,21. In fetuses with
Copyright 2009 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2010; 35: 35–41.

Partial agenesis and hypoplasia of the corpus callosum 39
Figure 1 Brain of a 21-week fetus with normal corpus callosum at ultrasound (a) and pathology (b) examinations: the rostrum (1), genu (2),body (3) and splenium (4) are indicated. The corpus callosum appears of normal length, overlying posteriorly the quadrigeminal plate (QP).
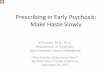
Figure 2 Brain of a 21-week fetus with partial agenesis of the corpus callosum at ultrasound (a), magnetic resonance imaging (b) andpathology (c) examinations: only the rostrum (1), genu (2) and body (3) are visible; the splenium is missing. The corpus callosum is shortposteriorly and does not seem to overlay the quadrigeminal plate (QP).
Figure 3 Reconstruction of the median plane from an ultrasoundvolume of the brain in a 21-week fetus with partial agenesis of thecorpus callosum (CC) and Dandy–Walker complex. The CCappears short and thin, the cerebellar vermis (V) is hypoplastic andthere is a wide communication between the 4th ventricle and thecisterna magna (*).
Figure 4 Median view of fetal brain at transvaginal power Dopplerexamination in a 21-week fetus with partial agenesis of the corpuscallosum (CC): the pericallosal artery (PA) strictly follows thecontour of the anterior part of the CC but takes an upwarddirection at the level of the missing splenium.
Copyright 2009 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2010; 35: 35–41.

40 Ghi et al.
Figure 5 Reconstruction of the median plane from an ultrasoundvolume of the brain in a 21-week fetus with callosal hypoplasia.The corpus callosum (CC) appears thin but normal in length(arrows).
partial callosal agenesis a shorter corpus callosum maybe demonstrated at ultrasound or MRI and eventuallyconfirmed at pathology (Figures 2 and 3). In our series,antenatal diagnosis of partial agenesis was suspected atgray-scale ultrasound, but our confidence was increasedby Doppler imaging, which additionally documented anabnormal course of the pericallosal arteries in all cases(Figure 4).
Callosal hypoplasia is a developmental disorder thatmay be induced by teratogens (radiation, alcohol)or compression (e.g. intracranial masses, obstructivehydrocephalus)4,12. Rather than a primary malforma-tive abnormality callosal hypoplasia is more likely todepend upon an external factor affecting the num-ber and size of callosal axons. This is apparentlyconfirmed by our experience since callosal hypopla-sia was often associated with additional brain anoma-lies. At prenatal ultrasound, callosal underdevelopmentwas suspected when callosal thickness in the medianplane was below the normal range provided by nor-mative charts. This was seen both at 2D and 3Dultrasound in our series (Figure 5). To date, only afew cases of callosal hypoplasia have been detectedantenatally12,22.
In cases of abnormal callosal findings at ultrasound,MRI was offered (from 2001) to confirm sonographicfindings. MRI is considered by some to be the mostaccurate technique for investigating the fetal CNS anddetecting antenatally subtle cerebral anomalies23–25. Infetuses with suspected callosal anomalies, it is worthyof recommendation in order to reinforce a difficultsonographic diagnosis and at the same time to excludepossible additional cerebral anomalies which may beoverlooked at ultrasound but may affect the outcomeconsiderably. As previously reported26, in this studyexpert sonography and MRI performed equally well in theprenatal assessment of midline brain anomalies and in nocase did the addition of MRI change the sonographicdiagnosis. Furthermore, antenatal ultrasound findings
regarding the corpus callosum were in all casesconsistent with findings at postnatal neuroimaging orpathology.
There were often additional malformations at intra- orextracranial locations associated with callosal underde-velopment and, in our experience, some of these fetusesturned out to be affected by a chromosomal or geneticdisorder. In view of this finding, whenever callosal under-development is suspected, a careful survey of the entirefetal anatomy and prenatal karyotyping are warranted.Moreover, the risk of an underlying genetic syndromethat may be disclosed only after birth should always bementioned when counseling the prospective parents. Onthe other hand, as suggested by our data, partial agen-esis or hypoplasia of the corpus callosum may occur inisolation. In these cases, neurological outcome is reportedby some to be similar to that in cases with absent corpuscallosum1,7,15, while according to others a worse out-come should be expected for cases with complete agenesisdue to the greater disruption of neuronal function6. Volpeet al.11 recently reported neurodevelopmental delay in twoof eight cases of apparently isolated partial callosal agen-esis. In our series the limited number of surviving infantswith isolated underdevelopment of the corpus callosumdoes not allow us to draw any conclusions. Further studiesare warranted to establish whether, in cases of apparentlyisolated callosal underdevelopment, expert sonographymay help in detecting antenatally those fetuses that arelikely to show an adverse outcome after birth. More-over, particularly in these cases, prolonged and carefulneurological follow-up of the surviving children wouldbe desirable to fully understand the long-term impact ofcallosal dysgenesis on quality of life and to give reliableinformation to prospective parents.
In conclusion, our study confirms that a reliablediagnosis of partial callosal agenesis or callosal hypoplasiacan be achieved antenatally by expert sonography. Inall cases in this series prenatal diagnosis was confirmedeither at pathology or postnatal evaluation. Thereis apparently an association with major intra- andextracranial anomalies, and possibly with chromosomalor genetic disorders. However, due the paucity of casesreported in literature, even in fetuses with apparentlyisolated findings the prognosis remains uncertain.
REFERENCES
1. Shevel MI. Clinical and diagnostic profile of agenesis of thecorpus callosum. J Child Neurol 2002; 17: 896–900.
2. Fratelli N, Papageorghiou AT, Prefumo F, Bakalis S, Hom-fray T, Thilaganathan B. Outcome of prenatally diagnosedagenesis of the corpus callosum. Prenat Diagn 2007; 27:512–517.
3. Vergani P, Ghidini A, Strobelt N, Locatelli A, Mariani S,Bertalero C, Cavallone M. Prognostic indicators in the prenataldiagnosis of agenesis of corpus callosum. Am J Obstet Gynecol1994; 170: 753–758.
4. Davila-Gutuerrez G. Agenesis and dysgenesis of the corpuscallosum. Semin Pediatr Neurol 2002; 9: 292–301.
5. Pilu G, Sandri F, Perolo A, Pittalis G, Grisolia G, Cocchi G,Foschini MP, Salvioli GP, Bovicelli L. Sonography of fetal
Copyright 2009 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2010; 35: 35–41.

Partial agenesis and hypoplasia of the corpus callosum 41
agenesis of the corpus callosum: a survey of 35 cases. UltrasoundObstet Gynecol 1993; 3: 318–329.
6. Goodyear PWA, Bannister CM, Russell S, Rimmel S. Outcomein prenatally diagnosed fetal agenesis of the corpus callosum.Fetal Diagn Ther 2001; 16: 139–145.
7. Moutard ML, Kieffer V, Feingold J, Kieffer F, Lewin F, Adams-baum C, Gelot A, Campistol I Plana J, van Bogaert P, Andre M,Ponsot G. Agenesis of corpus callosum: prenatal diagnosis andprognosis. Childs Nerv Syst 2003; 19: 471–476.
8. Visentin A, Pilu G, Falco P, Bovicelli L. The transfrontal view:a new approach to the visualization of the fetal midline cerebralstructures. J Ultrasound Med 2001; 20: 329–333.
9. Gerbasky SS, Gerbasky KS, Bowerman RA, Silver TM. Agen-esis of the corpus callosum. Sonographic features. Radiology1984; 151: 443–448.
10. Lockwood CJ, Ghidini A, Aggarwal R, Hobbins JC. Antenataldiagnosis of partial agenesis of the corpus callosum: a benigncause of ventriculomegaly. Am J Obstet Gynecol 1988; 159:184–186.
11. Volpe P, Paladini D, Resta M, Stanziano A, Salvatore M, Quar-antelli M, De Robertis V, Buonadonna AL, Caruso G, Gen-tile M. Characteristics, associations and outcome of partialagenesis of the corpus callosum in the fetus. Ultrasound ObstetGynecol 2006; 27: 509–516.
12. Paupe A, Bidat L, Sonigo P, Lenclen R, Molho M, Ville Y.Prenatal diagnosis of hypoplasia of the corpus callosumin association with non-ketotic hyperglycinemia. UltrasoundObstet Gynecol 2002; 20: 616–619.
13. Malinger G, Zakut H. The corpus callosum: normal fetaldevelopment as shown by transvaginal sonography. AJR Am JRoentgenol 1993; 161: 1041–1043.
14. Achiron R, Achiron A. Development of the human fetal corpuscallosum: a high-resolution, cross-sectional sonographic study.Ultrasound Obstet Gynecol 2001; 18: 343–347.
15. Mordefroid M, Grabar S, Andre Ch, Merzoug V, Moutard ML,Adamsbaum C. Agenesie partielle du corps calleux de l’enfant.J Radiol 2004; 85: 1915–1926.
16. Pilu G, Segata M, Ghi T, Carletti A, Perolo A, Santini D,Bonasoni P, Tani G, Rizzo N. Diagnosis of midline anomaliesof the fetal brain with the three-dimensional median view.Ultrasound Obstet Gynecol 2006; 27: 522–529.
17. Vinals F, Munoz M, Naveas R, Giuliano A. Transfrontalthree-dimensional visualization of midline cerebral structures.Ultrasound Obstet Gynecol 2007; 30: 162–168.
18. Kier EL, Truwit CL. The normal and abnormal genu of thecorpus callosum: an evolutionary, embryologic, anatomic,and MR analysis. AJNR Am J Neuroradiol 1996; 17:1631–1641.
19. Fuchs F, Moutard ML, Blin G, Sonigo P, Mandelbrot L. Prena-tal and postnatal follow-up of a fetal interhemispheric arachnoidcyst with partial corpus callosum agenesis, asymmetric ventricu-lomegaly and localized polymicrogyria. Case report. Fetal DiagnTher 2008; 24: 385–388.
20. Barkovich AJ. Apparent atypical callosal dysgenesis: analysisof MR findings in six cases and their relationship toholoprosencephaly. AJNR Am J Neuroradiol 1990; 11:333–339.
21. Volpe P, Campobasso G, De Robertis V, Rembouskos G.Disorders of prosencephalic development. Prenat Diagn 2009;29: 340–354.
22. Chadie A, Radi S, Trestard L, Charollais A, Eurin D, Ver-spyck E, Marret S; Haute-Normandie Perinatal Network. Neu-rodevelopmental outcome in prenatally diagnosed isolatedagenesis of the corpus callosum. Acta Paediatr 2008; 97:420–424.
23. Glenn OA, Goldstein RB, Li KC, Young SJ, Norton ME,Busse RF, Goldberg JD, Barkovich AJ. Fetal magnetic resonanceimaging in the evaluation of fetuses referred for sonographicallysuspected abnormalities of the corpus callosum. J UltrasoundMed 2005; 24: 791–804.
24. Levine D, Cavazos C, Kazan-Tannus JF, McKenzie CA, DialaniV, Robson CD, Robertson RL, Poussaint TY, Busse RF,Rofsky NM. Evaluation of real-time single-shot fast spin-echoMRI for visualization of the fetal midline corpus callosumand secondary palate. AJR Am J Roentgenol 2006; 187:1505–1511.
25. Barkovich AJ. Magnetic resonance imaging: role in theunderstanding of cerebral malformations. Brain Dev 2002; 24:2–12.
26. Malinger G, Lev D, Lerman-Sagie T. Is fetal magnetic resonancesuperior to neurosonography for detection of brain anomalies?Ultrasound Obstet Gynecol 2002; 20: 317–321.
Copyright 2009 ISUOG. Published by John Wiley & Sons, Ltd. Ultrasound Obstet Gynecol 2010; 35: 35–41.