Embed Size (px)
Citation preview


Preoperative Evaluation
Lateral compartment lymph nodes are easier to detect and are amenable to FNA
Central compartment lymph nodes are much more difficult to detect and FNA (Tg washout testing is compromised)

Som et al, AJR 174:837 2003
Surgical Levels of the Neck
See insert in back of syllabus.

Surgical Compartments of the Neck
Compartment I Submandibular to the hyoid bone
Compartments II, III, IV From the vascular bundle deep to the SCM Division by hyoid and cricoid
Compartment V Posterior to the SCM
Compartment VI The “central compartment”

Cervical Lymph Nodes
• Approximately 300 lymph nodes in the normal neck.
• Typically can identify 6 – 20 nodes by ultrasound.
• Nodes are more prominent following infections, mononucleosis, dental procedures and in Hashimoto’s thyroiditis.

Differentiated Thyroid Cancer
63,000 New cases of DTC in 2014 1,890 Deaths predicted in 2014 Mortality essentially unchanged over
past 30 years Unproved assumption: Early
detection and treatment of cervical metastases will affect mortality Mortality versus Morbidity

Preoperative Imaging
WDTC clinically involves lymph nodes in approximately 20% of patients . (Micrometastases in up to 90%)
Pre-op US identifies suspicious Lateral neck nodes in approximately 14% of cases.
Surgical management is altered in the presence of lateral neck metastases
○ Near total Thyroidectomy○ Central Neck Dissection! (ATA Guidelines 2009)○ Lateral Neck Dissection
Kouvaraki, Surgery 2003 134:946; Stulak, Arch Surg 2006 141:489

Preoperative Imaging Alternatives
Ultrasound evaluation is uniquely operator dependent
Sensitivity of CT, MRI and PET is less Ultrasound versus CT
Characteristics of benign/suspicious nodules Contrast interference with RAI ablation Expense and time Visualization behind trachea and TE groove

And, if pre-op US NOT performed . . .
17 patients underwent reoperation for thyroid cancer MD Anderson <6months after initial surgery
Kouvaraki Surgery 2004 136:1183
PRE-OP US would have prevented 70% or the reops!!!

Recurrences occurred significantly more often if ultrasound demonstrated abnormal nodes preoperatively1
1Ito, World J Surg 2005; 2Ito, World J Surg 2004
560 patients underwent thyroidectomy and modified neck dissection
Role for Preoperative Ultrasound Nodal Evaluation
Recurrence rate
US Neg 3.1%
US Pos 24.8%
US neg LNs455 pts
US + LNs105 pts

Does lateral neck dissection alter the outcome for preoperative US positive for
lymph nodes?
Prophylactic lateral neck dissection does NOT improve recurrence free survival for patients
with preoperative US negative for lymph nodes1
1Ito, World J Surg 2004

For “macroscopic” lateral lymph node metastases, modified neck dissection at time of initial thyroidectomy improves survival
Noguchi, Arch Surg, 1998 133 276-280

Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer 2009
R21. Preoperative neck ultrasound for the contralateral lobe and cervical (central and bilateral) lymph nodes is recommended for all patients undergoing thyroidectomy for malignant cytologic findings on biopsy – Recommendation B
R22. Routine preoperative use of other imaging studies (CT, MRI, PET) is not recommended –Recommendation E
THYROID, 2009 19:1167 www.thyroid.org

Pre-op evaluation of central compartment
Metastatic paratrachael lymph node
Carotid
Thyroid nodule

Preoperative Evaluation of Lateral Compartment
48yo female with cystic nodule right lobe (N) and lymph node in neck (LN)
Needle washout from lymph node Tg=24.3ng/ml
N
C
LNFNA cytology of nodule and lymph node negative

Post-operative Ultrasound Evaluation for the Surveillance of Patients with Low Risk (Stage I and II) Thyroid Cancer

Tests Used in Post-0perative Thyroid Cancer SurveillanceTests Used in Post-0perative Thyroid Cancer Surveillance
Thyroglobulin
131I or 123I Whole Body Scan
Ultrasound

Detection of LN metastasesWBS vs. Neck US
0102030405060708090
100
Sen
siti
vity
(%
)
Fr aso l dat i Paci n i To r l on t ano
WBSUS
Frasoldati et al, Cancer 2003; Pacini et al, J Clin Endocrinol Metab 2003; Torlontano et al, J Clin Endocrinol Metab 2004

Diagnosis of Recurrent DTC in 51 of 494 Patients
• 131I Whole Body Scan 23 (45%)• Tg > 2ng/ml (off T4 therapy) 29 (57%)• Tg detectable “ 34 (67%)• Ultrasound 48 (94%)
Frasoldati, et al; Cancer 2003

Morbidity of thyroid withdrawal Expense Poor sensitivity (60-75%)
lack of transmembrane sodium iodide symporter expression (especially with BRAF/RAS mutation)
Iodine contamination
Insufficient TSH stimulation
“Stunning” Potential for causing growth?
Withdrawal versus Thyrogen
Limitations of Whole Body ScansLimitations of Whole Body Scans

R48a Following surgery, cervical ultrasound to evaluate the thyroid bed and central and lateral cervical nodal compartments should be performed at 6 to 12 months and then periodically, depending on the patients’ risk for recurrent disease and thyroglobulin status. Recommendation B
ATA guidelines 2009

14 14
68
87
0
20
40
60
80
100
Perc
ent
(%)
In i t ial Surgery Reoperat ion
MD Ander son Mayo
Does US change surgery?Imaging of nonpalpable nodes
Kouvaraki, Surgery 2003 134:946; Stulak, Arch Surg 2006 141:489

Where do we look for metastatic lymph nodes?

Locations of PTC nodal recurrences
Ipsilateral ONLY, 12%
Central and bilateral,
13%
Central ONLY, 22%
Bilateral only, 1%
Central and ipsilateral,
52%
“skip metastases”
Leboulleux J Clin Endocrinol Metab 2005
87% involveCentral LNs

Post-operative Ultrasound Evaluation Both the central compartment and the lateral
compartments of the neck are easily surveyed with US in the post-op thyroid cancer patient
FNA using US guidance allows both cytology and analysis for thyroglobulin without regard to thyroglobulin antibody

Post-operative Neck

Characteristics of Benign Lymph NodesCharacteristics of Benign Lymph Nodes
Flattened or oval shape (AP/T <0.5) Echogenic (hilar) line Hilar vascular flow on Doppler Size varies with compartment and is
less important than morphology. Border definition also less important.

The Hilar Line A normal node can be split down the
central hilum. Hilum contains fat and vessels A normal hilar line can be thin or thick,
and can be central or eccentric/diagonal. The presence of a hilar line is
reassuring.

Normal lymph node- hilus

Normal Lymph Nodes

Normal Node with Broad Central Hilum

Normal Lymph Node

Normal Lymph NodeNormal hilar blood flow

Node ShapeVariations
Central Compartment Paratracheal nodes
Post surgical neck Loss of usual tissue planes
Hashimoto’s Matted Inflammatory

Paratracheal NodesHashimoto’s Thyroiditis

Hashimoto’s Thyroiditis

Node Size Variations
Is there an absolute size limitation? Compartments III, IV○ 5 mm AP (?) NO!!
Compartment II○ 8 – 10 mm AP (?) NO!!!
Role for repeat evaluation over time Reactive nodes vary over time without
progressive growth.

Large Benign Node - Compartment 2

Compartment 3 - Benign

Compartment 3 – Benign – 6 months later

Compartment 3 – Benign – 6 months later
10/07
4/08

Papillary Carcinoma Small round nodes - Benign

Papillary Carcinoma Small round nodes - Benign

Characteristics of Metastatic Lymph NodesCharacteristics of Metastatic Lymph Nodes
Absent echogenic (hilar) line
Rounded appearance AP/T>.5 (transverse view)
Jugular displacement
Calcifications
Cystic necrosis
Chaotic vascularization

Characteristics of Malignant Nodes
Disordered vascularity 86% 82% Microcalcifications 45% 100% Cystic Degeneration 11% 100% Absence of Hilar Line 95% 20% Hypoechoic Echotexture 39% 18%
From Susan Mandel 2008Leboulleux JCEM 2007Ahuja, Clinical Radiology 2001
Sensitivity Specificity

Malignant Node: AP/T >0.5

Malignant Nodes AP/TV >0.5

Malignant Node

Jugular Displacement
Calcification

Jugular Displacement

Cystic Necrosis
Enhancement

Heterogeneous Echogenicity
Calcifications

Papillary Carcinoma – Tall Cell – Calcified Node

Papillary Carcinoma – Node – Chaotic Vascularity

Metastatic Papillary Carcinoma
Central Lateral

Lymph node in central compartment

Compartment 3 - Malignant

Central Compartment Node hypoechoic

Malignant Node hyperechoic

Malignant Node – Anaplastic CA

Malignant Node – Hurthle Cell CA

Chaotic vascularization

What do we do when US detects an abnormal LN?
R48b If a positive result would change management, ultrasonographically suspicious lymph nodes greater than 5 – 8 mm in the smallest diameter should be biopsied for cytology with thyroglobulin measurement in the needle washout fluid. Recommendation A ATA Guidelines 2009
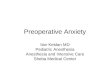
Boi, J Clin Endocrinol Metab, 2006
86
100
81
100
0102030405060708090
100Se
nsit
ivit
y (%
)
TG Ab+ TG Ab-
Pat ients' Ab status
Cyt o FNA Tg
Detection of malignancy in 40 LNs after US guided FNA

143 Consecutive Patients with Stage I and II Papillary CancerJune 2003-November 2004
41 patients had 1 or more suspicious lymph nodes and underwent UG-FNA.
14 patients had positive cytology and/or Tg washout.
Baskin, Thyroid 14:11:2004

Recurrent Cancer PatientsRecurrent Cancer Patients
22 M 1 14.2 - + 39.950 M 13 <0.3 + + 24.953 F 12 <0.3 - + 19.851 F 20 <0.3 - + 10.536 M 2 <0.3 + + 67.540 M 7 19. - - 50052 M 5 1.8 - - 44354M 4 8 - - 87.548F 1 <0.3 + - 24.332F 18 0.8 - + 10,93643F 2 0.6 - + 6.657F 13 <0.3 - - 23771F 15 1.3 - + 1.554F 36 11.5 - + 2
Age/sex Years Tg Tg AB Cytology FNA-Tg

The challenge of minimal residual/recurrent disease
left
CA
IJ
right
CAIJ

R48c Suspicious lymph nodes less than 5-8 mm in diameter may be followed without biopsy with consideration for intervention if there is growth or if the node threatens vital structures. Recommendation C
ATA guidelines 2009

Differential Diagnosis of Cervical Lymph Nodes
Benign – Reactive Thyroid Cancers Cervical Lymphoma Chronic Lymphocytic Leukemia Metastases from other Cancers Sarcoid

Cervical Lymphoma

Cervical Lymphoma

Chronic Lymphocytic Leukemia

Chronic Lymphocytic Leukemia

Breast metastases to Cervical Compartment IV

Breast Cancer Compartment IV
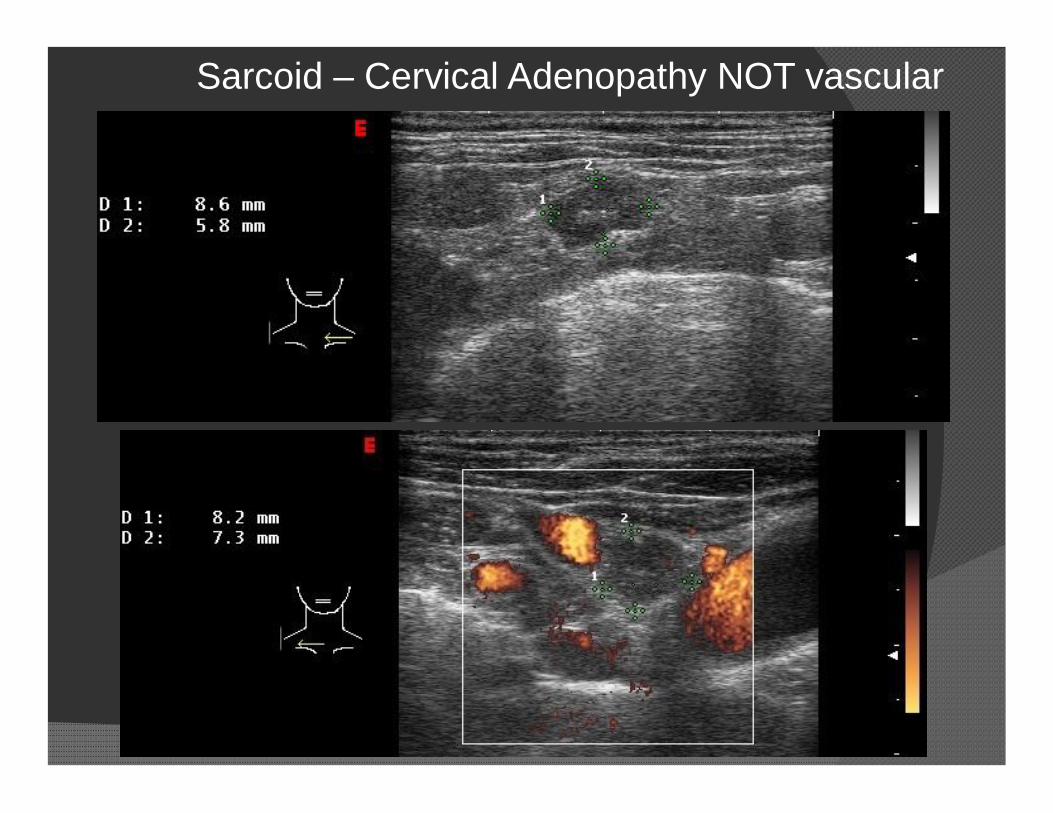
Sarcoid – Cervical Adenopathy NOT vascular

Role of cross sectional imaging in setting of rising thyroglobulin:
Neck MRI or CT with contrast for clinically occult nodesRetropharynxParapharyngeal space Low cervical lymph nodesMediastinum
Consider in patients with prior metastatic LNs in anterior cervical compartments
Kaplan, Mandel J Neuroradiol, 2009

History of thyroid cancer, rising thyroglobulinLeft retropharyngeal lymph node
CT guided FNA
Kaplan, Mandel J Neuroradiol, 2009

ATA Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid CancerULTRASOUND
R21. Preoperative neck ultrasound for the contralateral lobe and cervical (central and especially lateral neck compartment) lymph nodes is recommended for all patients undergoing thyroidectomy for malignant cytologic findings on biopsy. US guided FNA of sonographically suspicious lymph nodes should be performed to confirm malignancy if this would change management.
– Recommendation B
THYROID 2009 Volume 19:1167

ATA Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer
ULTRASOUND• 48a. Following surgery, cervical US to evaluate the thyroid bed
and central and lateral cervical nodal compartments should be performed at 6 -12 months and then periodically, depending on the patient’s risk for recurrent disease and TG status. Recommendation B
• 48b. If a positive result would change management utrasonographically suspicious lymph nodes greater than 5-8 mm in the smallest diameter should be biopsied for cytology with Tg measurement in the needle washout fluid. Recommendation A
• 48c. Suspicious lymph nodes less than 5-8 mm in the largest diameter may be followed without biopsy with consideration for intervention if there is growth or if the node threatens vital structures. Recommendation CTHYROID 2009 Volume 19:1167