Embed Size (px)
Citation preview
Preoperative Management of Hypoxic Patients
R1 謝佩芳
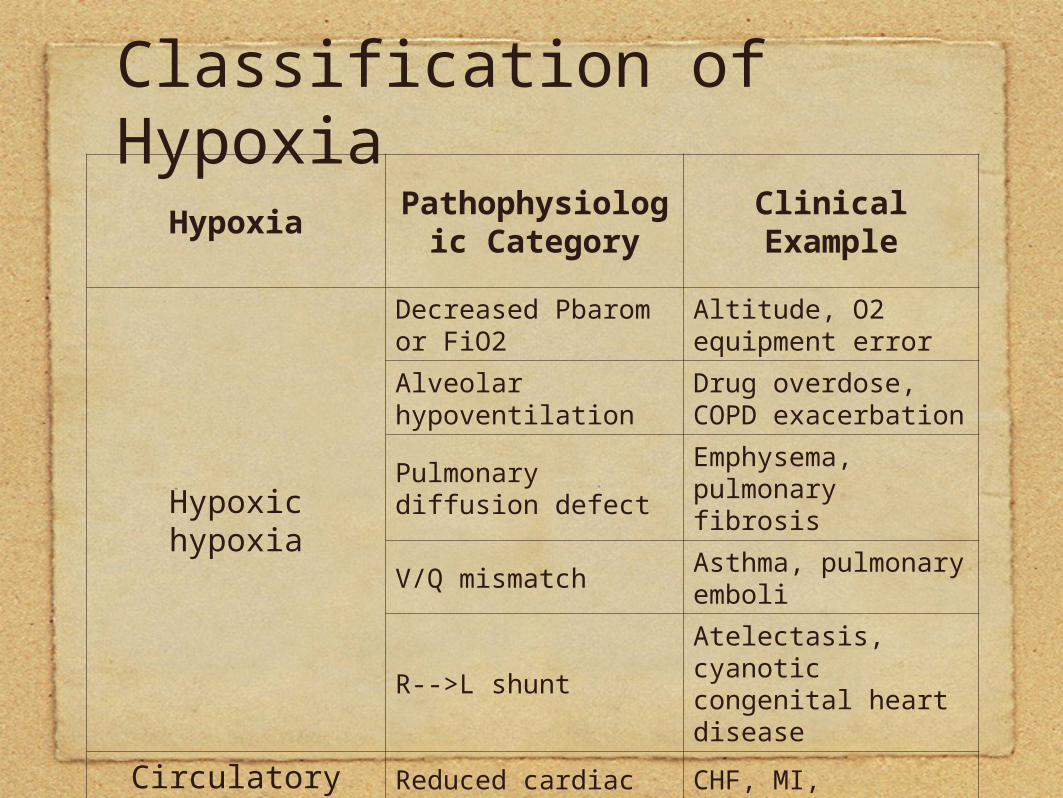
Classification of HypoxiaHypoxia
Pathophysiologic Category
Clinical Example
Hypoxic hypoxia
Decreased Pbarom or FiO2
Altitude, O2 equipment error
Alveolar hypoventilation
Drug overdose, COPD exacerbation
Pulmonary diffusion defect
Emphysema, pulmonary fibrosis
V/Q mismatchAsthma, pulmonary emboli
R-->L shuntAtelectasis, cyanotic congenital heart disease
Circulatory hypoxia
Reduced cardiac output
CHF, MI, dehydration
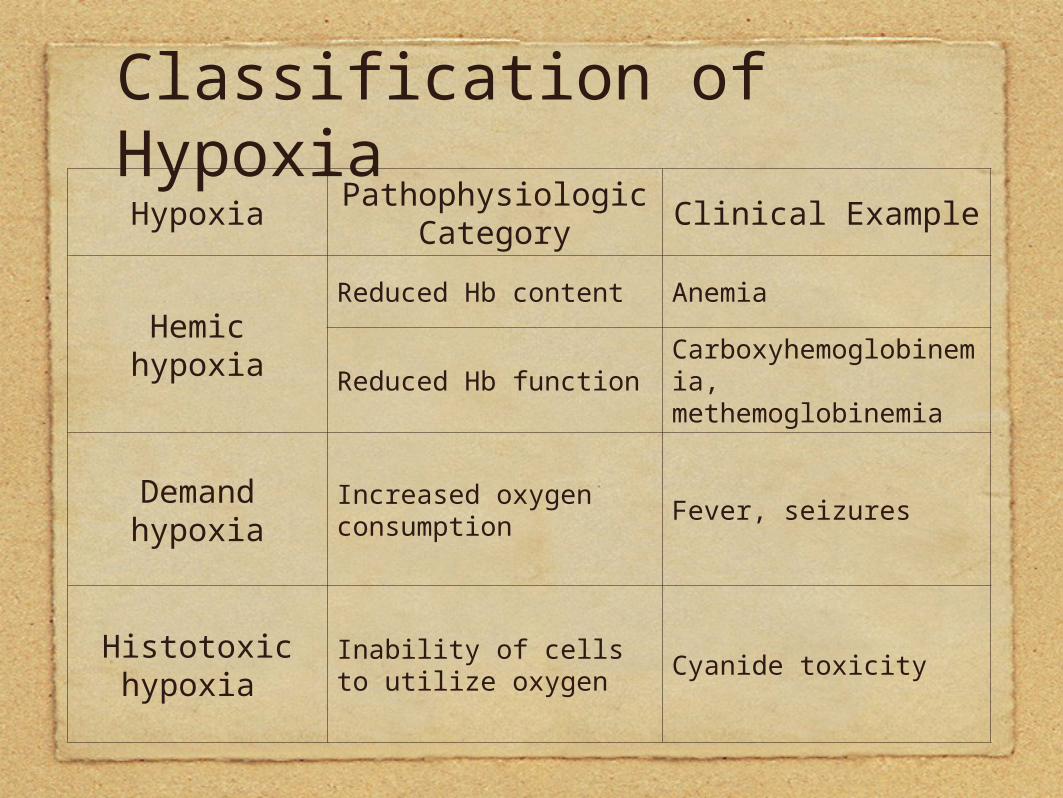
Classification of HypoxiaHypoxia
Pathophysiologic Category
Clinical Example
Hemic hypoxiaReduced Hb content Anemia
Reduced Hb functionCarboxyhemoglobinemia, methemoglobinemia
Demand hypoxia
Increased oxygen consumption
Fever, seizures
Histotoxic hypoxia
Inability of cells to utilize oxygen
Cyanide toxicity
Atelectasis and pulmonary embolism are most likely causes of the
desaturation.
Atelectasis
Preoperative Evaluation for Postoperative Pulmonary Complications
Postoperative Pulmonary Complications (PPC)
• Atelectasis
• Pneumonia
• Respiratory failure
• ARDS
• Pleural effusion
Med Clin N Am 87(2003) 153-173
Med Clin N Am 87(2003) 153-173
Med Clin N Am 87(2003) 153-173
Preoperative Evaluation for Postoperative Pulmonary Complications
Risk Reduction Strategies
Preoperative smoking cessation
Abstinence for at least 8 weeks probably decreases PPC risk
Med Clin N Am 87(2003) 153-173
Preoperative Evaluation for Postoperative Pulmonary Complications
Risk Reduction Strategies
• Perioperative lung expansion maneuvers
- Incentive spirometry
- Chest physical therapydeep breathing exercisepostural drainagepercussion and vibrationcoughsuctioningmobilization Med Clin N Am 87(2003) 153-173
Preoperative Evaluation for Postoperative Pulmonary Complications
Risk Reduction Strategies
• Perioperative lung expansion maneuvers
- Intermittent positive pressure breathing
- CPAP
• Patient education in lung maneuvers initiated preoperatively is more effective in reducing PPC versus education initiated postoperatively
Med Clin N Am 87(2003) 153-173
Preoperative Evaluation for Postoperative Pulmonary Complications
Risk Reduction Strategies
• Postoperative analgesia
• Optimizing pulmonary function in patients with COPD and asthma
• Delaying surgery for patients with acute exacerbations of chronic lung disease or URI.
• No clear role for prophylactic antibiotic use.
Med Clin N Am 87(2003) 153-173
Pulmonary Embolism
Venous Thromboembolism (VTE)
The cornerstone of VTE diagnosis is clinical suspicion.
Because the first manifestation of VTE may be fatal pulmonary embolism (PE), patients with suspected VTE should be anticoagulated until the diagnosis is excluded.
Med Clin N Am 86(2002) 731-748
Diagnosis of VTE
Duplex ultrasonography
Contrast venography or MR venography
Patient with suspected PE:
• Lung ventilation and perfusion scan
• Helical CT
Med Clin N Am 86(2002) 731-748
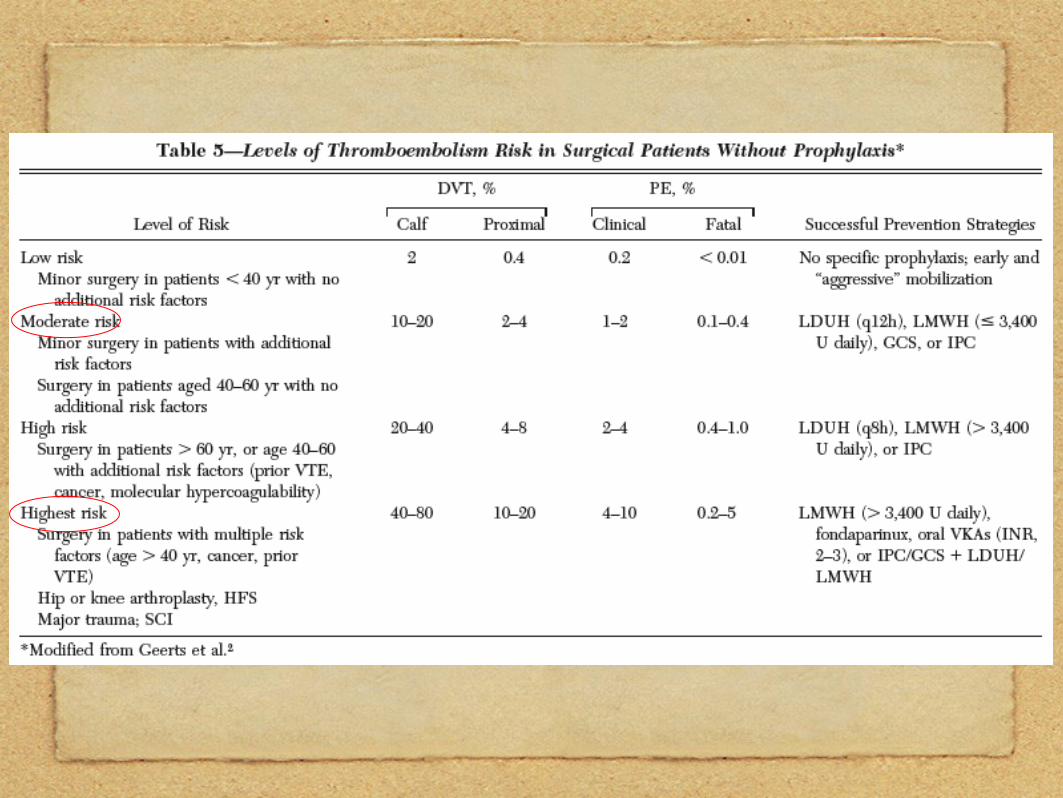
Prevention of Venous Thromboembolism
Chest 2004; 126:338S-400S
The Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy
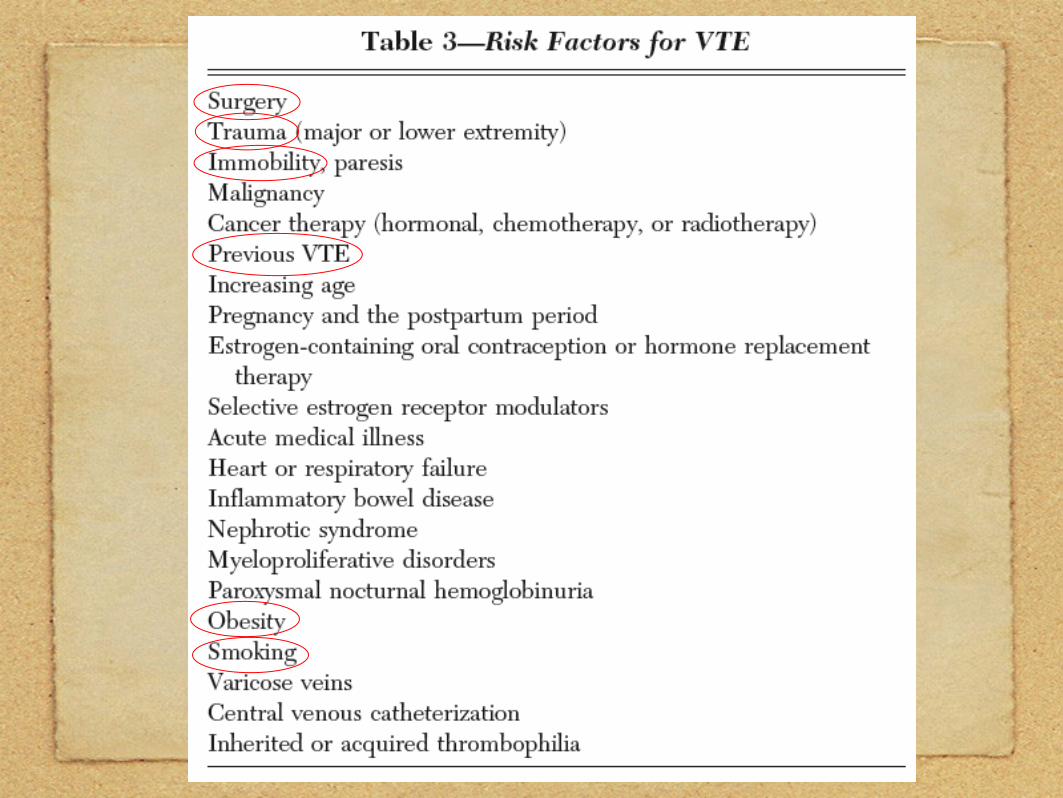
Recommendations: Trauma
Factors with increased risk of VTE:• Spinal cord injury• Lower extremity or pelvic fracture• Need for a surgical procedure• Increasing age• femoral venous line insertion or
major venous repais• Prolonged immobility• longer duration of hospital stay
Recommendations: TraumaWe recommend that all trauma patients with at least one risk fector for VTE receive thromboprophylaxis, if possible
In the absence of major contraindication (intracranial bleeding, ongoing and uncontrolled bleeding, uncorrected major coagulopathy, incomplete SCI with suspected or proven perispinal hematoma...), we recommend that clinicians use LMWH prophylaxis starting as soon as it is considered safe to do so.
Recommendations: Trauma
We recommend that mechanical prophylaxis with intermittent pneumatic compression (IPC), or possibly with graduated compression stocking (GCS) alone, be used if LMWH prophylaxis is delayed or if it is currently contraindicated due to active bleeding or a high risk for hemorrhage
Recommendations: Trauma
We recommend DUS screening in patients at high risk for VTE and who have received suboptimal prophylaxis or no prophylaxis
We recommed against the use of inferior vena cava filters (IVCFs) as primary prophylaxis in trauma patients.
Recommendations: Trauma
We recommend the continuation of thromboprophylaxis until hospital discharge, including the period of inpatient rehabilitation.
We suggest continuing prophylaxis after hospital discharge with LMWH or a VKA (target INR, 2.5; INR range, 2.0 to 3.0) in patients with impaired mobility.
As for this patient...Atelectasis
• Perioperative lung expansion maneuvers
Pulmonary embolism
• undergo further examination to exclude or confirm this diagnosis
• Thromboprophylaxis with anticoaulant or mechanical prophylaxis