Embed Size (px)
Citation preview

Washington, D.C. September 15, 2009
Preparing for Health ITLaying the Foundation With Quality and Process Improvement
A Panel Discussion Produced by ASQ for the 21st Century Health Care Caucus

600 N. Plankinton Ave.Milwaukee, WI 53201-3005t: 414-272-8575800-248-1946f: 414-272-1734www.asq.org
Rather than merely devising ways to pay for an existing, unsatisfactory healthcare delivery system, ASQ be-lieves that breakthroughs in healthcare reform can and should come about through the design of new ways of delivering service that are less costly and more effective. Across broad swaths of the healthcare system, there is much to gain and much waste to eliminate by using change management techniques and process improvement tools such as lean and Six Sigma to improve work and workflow and to prepare organizational cultures before we spend massive amounts on critical areas such as information technology.
This collection of information summarizes ASQ’s thinking on quality and healthcare reform, with particular attention to health IT issues. It includes case studies that offer examples of real-world improvement projects submitted by ASQ members.
The collection of actual case studies demonstrating the successful use of process improvement tools in various healthcare settings is exemplary of ASQ’s thinking on how healthcare costs can and should be reduced and healthcare quality can be improved by sustainably applying the methods that have been used for decades by other industries with considerable success. These cases are proof that identifying and eliminating the root causes of inefficiency, errors, and unsafe practices can pay huge dividends and why such activities should be adequately encouraged, supported, and incented as we seek to reform the nation’s healthcare system.
These samples include examples of the power of integrating process improvement with health information technology. ASQ believes that to do otherwise will dramatically weaken the positive impact of any programs seeking to provide support for health IT.
Also included are examples of quality and process improvement applications for improving patient safety, decreasing inpatient length of stay, decreasing waste in claims processing, and creating standardized work to improve efficiency in a family practice. The cases presented here represent improvements realized by hospitals and physician practices.
These and other case studies will be available on the ASQ Healthcare Division Web site (www.asq.org/health), where you can also find many other resources for quality improvement.
These materials are provided by ASQ and subject matter experts in the 3700-member ASQ Healthcare Divi-sion. For more than 60 years, ASQ has been a world leader in developing quality-related knowledge. Our leaders and members are ready to provide additional input and resources for improving healthcare delivery systems.
I’m sure you will find this collection useful and thought provoking.
Peter L. AndresASQ President

600 N. Plankinton Ave.Milwaukee, WI 53201-3005t: 414-272-8575800-248-1946f: 414-272-1734www.asq.org
ASQASQ is a global community of quality experts in all fields and industries. Its more than 90,000 members are dedicated to the promotion and advancement of quality tools, principles, and practices in their workplaces and their communities. Established in 1946, ASQ supports its mission by providing a wide range of resources, from certification and training to publications and conferences. Around the world, ASQ members and customers learn about and share quality management systems, tools, and practices. ASQ also develops relationships with other nonprofit organizations worldwide that have comparable missions and principles.
The Society serves as an advocate for quality as well. Its members have informed and advised the U.S. Congress, government agencies, state legislatures, and other groups and individuals on quality-related topics. ASQ has been involved with the Baldrige Award since its inception in 1988 and has been the sole administrator of the award since 1991. Headquartered in Milwaukee, Wis., ASQ is a founding sponsor of the American Customer Satisfaction Index (ACSI), a prominent quarterly economic indicator, and also produces the Quarterly Quality Report.
VisionBy making quality a global priority, an organizational imperative, and a personal ethic, ASQ becomes the community of choice for everyone who seeks quality technology, concepts, or tools to improve themselves and their world.
ASQ at a GlanceWorld Headquarters 600 North Plankinton Avenue Milwaukee, WI 53201-3005 USA Telephone +1-800-248-1946 or +1-414-272-8575 Facsimile +1-414-272-1734 Web www.asq.org Membership More than 90,000 individual members More than 800 Site, Enterprise, and K-12 members 252 geographic sections 26 topic-/industry-specific forums and divisions 18 networks Staff 200 at world headquarters; staff in China, India, and Mexico
Leadership ASQ is led by its board of directors and managed by an executive director/chief strategic officer and a management committee.
2009-10 Board of Directors—Office of the President Roberto Saco, Aporia Advisors, Inc., Chairman Peter L. Andres, Boeing Company, President E. David Spong, Boeing Company (Retired), President-Elect James J. Rooney, ABS Consulting, Treasurer
Management Paul E. Borawski, Executive Director/Chief Strategic Officer Julie Gabelmann, Executive Managing Director Christopher D. Bauman, Managing Director Robert Chalker, Global Managing Director Brian J. LeHouillier, Managing Director Michelle Mason, Managing Director Laurel Nelson-Rowe, Managing Director

Page
Improving the Pre-Empted Medication Error Reporting System 1
Reduction in the Percentage of Open Patient Encounters 11
Reducing Instrumentation in Major OR Sets 17
Improving e-Prescription Use by Patients 23
Reduction in Length of Stay for Heart Failure and Shock Patients 29
Hand-Hygiene Program to Reduce the Risk of Healthcare Associated Infections 37
Discovering the “Cost of Current Quality” in a Family Medicine Practice 43
Table of Contents
Appendix
• ASQ White Paper on Healthcare Reform—Executive Summary
• “First, Lay Groundwork for IT Adoption,” by Joseph Fortuna. Modern Healthcare, August 18, 2009
• ASQ Comments on Health IT Extension Program
• ASQ Comments on “Meaningful Use” of Electronic Health Records
• References on Health IT and Quality

Case Studies

1
© 2009 ASQ
Improving the Pre-Empted Medication Error
Reporting System at St. Charles Hospital,
Port Jefferson, NYSubmitted by:
Kathleen LeDoux, MS, RN, BC, CPHQPerformance Improvement Nurse
St. Charles HospitalPort Jefferson, NY
© 2009 ASQ
1. NAME AND LOCATION OF ORGANIZATION/FACILITY/DEPARTMENTSt. Charles Hospital, Port Jefferson, NY
2. TYPE AND SIZE OF ORGANIZATION/FACILITY/DEPARTMENT239-bed community hospital
3. FUNCTION(S)/MISSION OF ORGANIZATION/FACILITY/DEPARTMENT MAKING THE IMPROVEMENTInterdisciplinary improvement project involving the nursing and pharmacy departments that work actively together to promote patient safety as part of our Medication Safety and Usage Committee.
4. POSITION(S) OF THOSE INVOLVED IN THE PROJECTGerard Smaldino, MS, RPhKathleen LeDoux, MS, RN, BC, CPHQ
IDENTIFYING INFORMATION
Improving the Pre-Empted Medication Error Reporting System at St. Charles Hospital, Port Jefferson, NY

2
© 2009 ASQ
• Medication error reporting at St. Charles Hospital is an interdisciplinary process.
• Beginning in 2004-2005, team members from the medical staff, nursing, nursing education, pharmacy, quality, and risk management began to explore ways to recognize and improve the reporting of pre-empted errors.
• While traditional reporting via the formal occurrence reporting system was encouraged, other venues for recognition and reporting were considered.
• The team determined that certain categories in the clinical interventions performed by pharmacy and the MAR communications generated by nursing could appropriately be recognized as pre-empted medication errors.
DESCRIPTION OF THE PROBLEM
© 2009 ASQ
Project Goals1. To provide a process to ensure the correctness of the
MAR on a daily basis.2. To accurately capture clinical interventions performed
by the pharmacy staff.3. To simplify the process to communicate MAR
corrections from the nursing staff to the pharmacist.
DESCRIPTION AND QUANTIFICATION OF THE GOAL(S) AND TARGET(S) OF THE DESIRED SOLUTION

3
© 2009 ASQ
Through drill-down analysis, St. Charles determined that these two processes were means of identifying pre-empted medication errors that often went unrecognized and under-reported.
MAR COMMUNICATIONS• Beginning in 2004, St. Charles Hospital implemented the
facility-wide utilization of an electronic MAR. • This changed the way medications were transcribed to
the medication record.• When utilizing a traditional paper-based medication
record, the nurse had the primary responsibility to transcribe the patient’s medication orders to the record.
THE ROOT CAUSE ANALYSIS OF THE PROBLEM
© 2009 ASQ
MAR COMMUNICATIONS (continued)• The conversion to an electronic record generated daily,
in conjunction with the utilization of the Hard Stop, placed the emphasis for transcription on the pharmacist.
• The nurse was now required to review the printed MAR for transcription omissions or discrepancies.
CLINICAL INTERVENTIONS• Clinical Drug Interventions: Actions/interventions
between the pharmacist and the ordering clinician to either clarify, correct, or discontinue a current order to the medication profile.
• Intervention occurs prior to dispensing and administration of medications/treatments ordered.
THE ROOT CAUSE ANALYSIS OF THE PROBLEM

4
© 2009 ASQ
Changes Implemented: • Converted from a paper-based medication administration record to
an electronically generated MAR.• Converted Hard Stop distribution from the pharmacist delivering the
forms to the unit on a daily basis, to an electronically generated form.
• Educated medical, nursing, and pharmacy staff to the system changes.
• Revised the 24-hour order check process to reflect the need to review the daily generated MAR and Hard Stop.
• Initiated a MAR communication sticker to capture transcription discrepancies.
• Began breaking down the clinical intervention categories into more specific areas to promote data capture.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
© 2009 ASQ
Changes Implemented: • Reinforced to the concerned pharmacy staff the importance of
recording information when interventions occurred. • Encouraged the concerned nursing staff and pharmacy staff to
utilize the MAR communication process rather than telephone communications, which could not be tracked effectively.
• Aggregated data on a quarterly basis and reported results at theMedication Safety and Usage Committee and the Hospital-wide Performance Improvement Council meetings.
• Continue to meet on a bi-monthly basis to discuss concerns and issues related to medication management.
• Acted on nursing staff suggestions to revise the MAR communication process.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES

5
© 2009 ASQ
Changes Implemented: • Revised the process requiring the nurse who noted the discrepancy
to (a) photocopy the MAR, (b) apply a sticker to the MAR, and (c) fax the MAR to the pharmacy to, instead (a) change the sticker to a form, (b) add additional categories such as incorrect or missingallergy information, and (c) have the order number attributed to the profile entry printed on the MAR, thereby essentially eliminating the need to fax the order to the pharmacy.
• Revised data aggregation from a quarterly process to monthly results began in the second quarter of 2008.
• Continue to encourage all methods of reporting potential or actual medication errors.
• Utilize the “Good Catch” awards as an avenue to provide staff recognition.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
© 2009 ASQ
• This project did NOT require any additional staff or cost to implement.
• The processes were developed jointly by members of the Medication Safety and Usage Committee, which is an undertaking of the nursing and pharmacy departments.
• It did and continues to require staff education and reinforcement relating to the benefits of the program.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES

6
© 2009 ASQ
• These changes have yielded increased satisfaction and improved patient safety in the work flow of both departments.
• The development of this project clearly demonstrated to both departments the value of a system of checks and balances when the medication order ordering process is combined of both electronic and paper components.
• The streamlined process implemented by changing to a form over a communication sticker reduced the number of steps the nurses were required to complete to report incorrect transcription on the MAR significantly and was accepted in lieu of a formal “occurrence report.”
THE RETURN ON INVESTMENT OF THE PROJECT
© 2009 ASQ
• The utilization of an order number to track a specific entry on the pharmacy profile allowed the pharmacy to access the specific order in question immediately or alerted them to the need that the order required re-faxing.
• The revision of the clinical interventions promoted data capture without increasing the workload of the pharmacist and prohibited dispensing of anticoagulants without corresponding laboratory values, thereby significantly increasing the pharmacy's role in the patient monitored intervention category.
THE RETURN ON INVESTMENT OF THE PROJECT

7
© 2009 ASQ
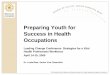
• The number of MAR communications received and clinical interventions initiated are reviewed and aggregated on a monthly basis, with quarterly reporting at the Hospital-wide Performance Improvement Council.
• Since we began tracking these efforts in 2006, we continue to see sustained reporting, with success demonstrated by the increasing number of MAR communications and clinical interventions since inception.
EFFORTS TO MONITOR AND EVALUATE THE PROCESS OVER TIME
© 2009 ASQ
Key Words:• Medication Error: The FDA defines a medication error as “any
preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient, or consumer.”
• Pre-Empted Error: The problem was found and corrected before it reached the patient.
• Clinical Drug Interventions: Actions/interventions between the pharmacist and the ordering clinician to either clarify, correct, or discontinue a current order to the medication profile. Intervention occurs prior to dispensing and administration of medications/treatments ordered.
• Medication Administration Record (MAR): Generated electronicallyon a daily basis by the Horizon Med Manager (HMM) Pharmacy System.
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS

8
© 2009 ASQ
Key Words (Continued):• Hard Stop: A system within HMM that provides a 24-hour warning
that a medication is due to expire. Expiration times are dictated by hospital or regulatory policy (e.g., controlled substance renewal is required every 72 hours). If a medication is NOT renewed by the clinician within the appropriate time frame, the medication will no longer appear on the MAR. Hard Stops are generated electronically daily on the nursing unit with the MAR.
• 24-Hour Order Check: A systematic review on a daily basis to ensure that the clinician’s orders have been transcribed to the MAR correctly.
• MAR Communications: An interdisciplinary communication tool that promotes real-time communication between the pharmacist and the nurse relating to transcription discrepancies noted in the completion of the 24-hour order check process.
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS (Continued)
© 2009 ASQ
Pharmacy Clinical Interventions:
The interventions listed below were deemed appropriate as pre-empted medication errors:
• Duplicate therapy/no indication• Contraindication due to allergy/diagnosis• Dose modification/organ impairment/age• Interaction (drug or nutrient) or incompatibility• Patient monitored (Lovenox/Cr/Cl;lytes;
Erythropoetin/Hgb; Coumadin/INR)• Drug incorrect/unclear/absent
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS (Continued)

9
© 2009 ASQ
Pharmacy Clinical Interventions (continued):
• Dose incorrect/unclear/absent• Frequency or rate incorrect/unclear/absent• Dosage form incorrect/unclear/absent• Route incorrect/unclear/absent• Duration incorrect/unclear/absent• Order clarification/communication• PRN usage indication• Range order clarification
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS (Continued)
© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS (Continued)
186
123
143
94
146
59
93
79
99
82 85
101 101
0
20
40
60
80
100
120
140
160
180
200
Num
ber R
epor
ted
2009 2008 2007 2006Time Frame
MAR Communications 2006- 2009
1st Q 2nd Q 3rd Q 4th Q

10
© 2009 ASQ
2,403
562
21532,0992,057
283 259 282 285186
280219 201
0
500
1,000
1,500
2,000
2,500N
umbe
r Rep
orte
d
2009 2008 2007 2006Time Frame
Pharmacy Clinical Interventions 2006- 2009
1st Q 2nd Q 3rd Q 4th Q
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS (Continued)

11
© 2009 ASQ
Reduction in the Percentage of Open Patient Encounters at the SMDC Clinic
in Duluth, MNSubmitted by:
Pam Helgeson-BrittonDirector of Process Excellence and Organizational Productivity
SMDC Health System, Duluth, MN [email protected]
© 2009 ASQ
THE RETURN ON INVESTMENT OF THE PROJECT
Net Return on Investment: Net Return on Investment:
OneOne--Time Net Revenue Gain of Time Net Revenue Gain of
$165,000$165,000
Reduction in the Percentage of Open Patient Encounters at the SMDC Clinic in Duluth, MN

© 2009 ASQ
1. NAME AND LOCATION OF ORGANIZATION/FACILITY/DEPARTMENT
2. TYPE AND SIZE OF ORGANIZATION/FACILITY/DEPARTMENTSMDC Health System serves a regional Midwest population of 460,000 at 17 locations with 4 fully-owned hospitals and the 400+ physician multi-specialty Duluth Clinic.
3. FUNCTION(S)/MISSION OF ORGANIZATION/FACILITY/DEPARTMENT MAKING THE IMPROVEMENTMission: To bring the soul and science of healing to the people we serve. Vision: Working together with our patients and communities, we are creating the next generation of integrated healthcare.
4. POSITION(S) OF THOSE INVOLVED IN THE PROJECTSenior Process Expert Manager Decision SupportPhysicians Clinic ManagersBusiness Analysts
IDENTIFYING INFORMATION
SMDC Health System, Duluth, MN - Health Information Services Department
© 2009 ASQ
• In the ambulatory setting, clinic practice management is integrated with the electronic health record.
• Providers determine the codes and diagnoses for patient visits as well as documenting care.
• It is the action of completing and closing the encounter with the patient that causes the coding to post the charges for the visit.
• When an encounter visit is left open, no revenue is realized for that visit.
• This affects timely billing and patient care (when documentation is not entered timely).
DESCRIPTION OF THE PROBLEM
12

© 2009 ASQ
• As the organization implemented provider-based billing at the clinic, it was even more imperative to force the timely release of the charges from closed encounters as UB04 billing did not allow for line item billing but required all charges to be posted before billing.
• Previous efforts to address this problem resulted in a one-time cleanup, but old practices resurfaced and the problem returned to former levels. No formal monitoring occurred and the focus was departmental versus system monitoring.
• Thus, the process of closing encounters was the focus of the team.
DESCRIPTION OF THE PROBLEM
© 2009 ASQ
The goal of the project was to decrease the unrealized dollars by $200,000 from $350,000.
The target, set during the process, was to decrease the percentage of open encounters in half from 0.35% to 0.17%.
DESCRIPTION AND QUANTIFICATION OF THE GOAL(S) AND TARGET(S) OF THE DESIRED SOLUTION
13

© 2009 ASQ
• The baseline was 0.35% of all encounters remained opened from a 10-day to a 180-day time period. While it appears to be a low percentage, this represented 1,600 encounters and $350,000 in unrealized charges on an ongoing basis. In-depth analysis showed this was not a system issue but more of an individual physician issue where 10-15 physician were the culprits and 2-4 departments (when physicians were combined) were causing the issue.
• The root cause analysis showed 80% of encounters were not closedbecause the documentation had yet to be completed. Without this, the encounter could not be closed. There was lack of organizational skills in completing the documentation in a timely manner within the electronic health record.
• The organization has had electronic health records for approximately 5 years. Administration had unaddressed issues with enforcing compliance. Various attempts had been made in the past to enforce compliance.
THE ROOT CAUSE ANALYSIS OF THE PROBLEM
© 2009 ASQ
• The biggest issue is that 80% of encounters are open because of the lack of documentation, which places compliance back in the hands of the physicians. Thus, strong guidelines were set by physician leadership with consequences at 7, 14, and 21 days of non-compliance. Where needed, additional organizational skills were provided to help physicians meet the required timelines forcompletion.
• The 48-hour rule for documentation to be completed was enforced.
• System-wide monitoring was implemented so that everyone in leadership was able to see the outliers and watch system improvements. The openness of system-wide monitoring has proved in the past to be a competitive tool producing results.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
14

© 2009 ASQ
• The timeliness of documentation was improved during the cleanup phase—ensuring better patient care when patients return or peers are required to treat patients.
• The captured revenue to date is $275,000, which equates to $275,000, which equates to approximately $165,000 in net paymentsapproximately $165,000 in net payments.
• This is a one-time capture of these dollars. Further ongoing compliance is required to ensure the revenue is not lost again if the volumes were allowed to rise.
• The delayed charges within provider-based billing was a key factor in increasing the AR, although small compared to the overall system.
• Less resources are required to review late charges, which often triggered manual intervention.
THE RETURN ON INVESTMENT OF THE PROJECT
© 2009 ASQ
Three reports were set up:
• System-wide department monitoring report totaled the unrealized dollars and volume of encounters not closed. This tool summed the missing revenue per department to draw attention to a vital, easily recognized impact.
• The same information was also set up to show individual physicians to help management work with those physicians not in compliance.
• Control charts tracked the baseline during the team project and continue tracking the compliance as the improvements were made.
EFFORTS TO MONITOR AND EVALUATE THE PROCESS OVER TIME
A countermeasures plan for off-specification performance was established and is implemented by physician leadership across the system.
15

© 2009 ASQ
Reasons encounters have no charges
0%10%20%30%40%50%60%70%80%90%
100%
NoDocumentation
No LOS Encounter notclosed
Physicians, NP, PAAncillary/RN/Other
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
© 2009 ASQ
Revenue fromUnrealized Charges from Open Encounters
11-180 days(Encounters still open after 10 days up to 180 days post date of service)
$0
$50,000
$100,000
$150,000
$200,000
$250,000
$300,000
$350,000
$400,000
$450,000
2/8/
2009
2/15
/200
9
2/22
/200
9
3/1/
2009
3/8/
2009
3/15
/200
9
3/22
/200
9
3/29
/200
9
4/5/
2009
4/12
/200
9
4/19
/200
9
4/26
/200
9
5/3/
2009
5/10
/200
9
5/17
/200
9
5/24
/200
9
5/31
/200
9
6/7/
2009
6/14
/200
9
6/21
/200
9
6/28
/200
9
7/5/
2009
Est Charges
Avg
Upper control limit
Lower control limit
Target (50%improvement)Target (75%improvement)
PE Team # PE 000304
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
16

© 2009 ASQ
Reducing Instrumentation in Major OR Sets for
Abdominal Colectomiesand Proctectomies at The University of Texas M.D. Anderson Cancer Center
Submitted by:Paul C. SoRelle
Program Manager, Division PublicationsOffice of Performance Improvement Unit 466
The University of Texas M. D. Anderson Cancer [email protected]
© 2009 ASQ
Net Return on Investment:Net Return on Investment:
Labor costs per case were reduced by Labor costs per case were reduced by 46%46% for for proctectomiesproctectomies and and
51%51% for for colectomiescolectomies. .
THE RETURN ON INVESTMENT OF THE PROJECT
Reducing Instrumentation in Major Abdominal OR Sets at The University of Texas M. D. Anderson Cancer Center
17

© 2009 ASQ
1. NAME AND LOCATION OF ORGANIZATION/FACILITY/DEPARTMENT The University of Texas M. D. Anderson Cancer Center, Houston/Surgical Oncology.
2. TYPE AND SIZE OF ORGANIZATION/FACILITY/DEPARTMENTCancer treatment and Research Center with 510 beds and 17,000 employees
3. FUNCTION(S)/MISSION OF ORGANIZATION/FACILITY/DEPARTMENT MAKING THE IMPROVEMENTDepartment of Surgical Oncology
4. POSITION(S) OF THOSE INVOLVED IN THE PROJECTJohn M. Skibber, MD (Surgery) LEADERVijaya Gottumukkala, MD (Anesthesiology)Carla P. Willis, RN (Nursing)Garrett Walsh, MD, Facilitator (Surgery)
IDENTIFYING INFORMATION
© 2009 ASQ
• Excessive amounts of instruments complicate the count process and may have negative impact on patient safety in the operating room.
• Reducing the number of instruments on the surgical field may yield a cost savings of labor and instrumentation.
• Before the project, one major instrument set was routinely provided for all major abdominal/pelvic cases.
• Many instruments were not used in the surgery.
• The greater number of instruments in a set, the greater chance of counting errors—which were shown to lead to reports of retained foreign objects that numbered 1,500 a year out of 28 million operations.
DESCRIPTION OF THE PROBLEM
18

© 2009 ASQ
To reduce the number of instruments in major OR sets by at least 50% during four months (October 2005 – January 2006) for abdominal colectomies (removal of a portion of the colon) and proctectomies (resection of the rectum).
DESCRIPTION AND QUANTIFICATION OF THE GOAL(S) AND TARGET(S) OF THE DESIRED SOLUTION
© 2009 ASQ
The team tracked the types of incorrect counts for two days of surgery. Of the 148, 91 dealt with instruments and 31 involved needles. Reasons for incorrect counts from root cause analysis:
• Not enough time• Opening too many supplies• No standard method of counting• Nurses feel rushed• No team effort• Inattentiveness
The team used a fish bone diagram to document reasons for “too many instruments opened and/or unused.”
THE ROOT CAUSE ANALYSIS OF THE PROBLEM
19

© 2009 ASQ
THE ROOT CAUSE ANALYSIS OF THE PROBLEM (Continued)
Competency Instrument Quality Cost
Inventory Satisfaction Safety
Too many instruments
opened/unused
Ortho or mulit-service cases - high volume of instruments/Staff Retention
Training time fornurses, techs and
sterile processing staff
Larger # of instruments detract from
paying attention to the patient and
surgeon
Control review process for set
content
Repeated reprocessing shortens lifespan of instrument
Set completenessmore likely for
smaller sets
Net margin/case
X-rays at end of case
Potential to "lose"
instruments
OR Time
Space: a. Sterile Processingb. Operating Room
Labor-Sterile Processing
Labor-Techs
Labor - Nursing
Peel pack par levels
Tracking
Surgeon preferences
Cost
Preference cards
Nursing:a. Trips to coreb. Shift changecommunication
c. Impact of surgeon
dissatisfaction
Sterile Processing
Surgeon:a. RN trips to
coreb. unavailable
itemsAnesthesiology
OR Culture
Anesthesia Time
Ergonomics:a. lighter sets
Retained foreign bodies
Count Accuracy
Staff Distractions
Communication of count at shift change
© 2009 ASQ
• The first step was for the nurses and surgical technicians to survey the surgeons’ instrument use in 12 cases.
• Many instruments were opened, counted, and then not used.
• The survey found there was very little variation in instrument use among the three surgeons who were part of the project team.
• The surgeons then agreed on a proposed set comprising any instrument they’d used even once during the 12 cases surveyed.
• Over the course of the project, the team reduced the number of instruments used in proctectectomies from 158 to 83, a 47.5% reduction. Instruments used in colectomies were reduced from 200 to 93, a 53.5% reduction.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
20

© 2009 ASQ
Labor costs per case were reduced by 46% Labor costs per case were reduced by 46% for for proctectomiesproctectomies and 51% for and 51% for colectomiescolectomies. .
THE RETURN ON INVESTMENT OF THE PROJECT
© 2009 ASQ
• After implementation of the reduced sets, the team has documented instances where additional instruments were needed and made adjustments to the sets.
• The Perioperative Enterprise has expanded the project to look at other surgical sets.
• For example, a cart with instruments and supplies for a mastectomy had 108 line items with total quantity of 148 pieces before improvement.
• Now the cart has 20% line items with a reduction of 34% in totalquantity of pieces.
• Along with the reduction in items, there is also savings in labor, supplies, and sterilization cost.
EFFORTS TO MONITOR AND EVALUATE THE PROCESS OVER TIME
21

© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
22

© 2009 ASQ
Improving e-Prescription
Use by Patients
Submitted by:Denis J. Devos, P.Eng
Mercy Physician Community PHO Port Huron, MI
© 2009 ASQ
DESCRIBE THE PROBLEM YOU WERE ADDRESSINGMany people are still calling the Doctor’s office for Prescription refills when they should be calling their pharmacy.Two scenarios: a.) The Pharmacy tells them to call the Doctor
b.) The patient calls the Doctor first instead of their pharmacy.
DESCRIBE AND QUANTIFY THE RETURN ON INVESTEMNT OF THE PROJECT IN PRODUCTIVITY, QUALITY INCREASES, COST AND WASTE REDUCTIONS, IMPROVED SATISFACTION, ETC.Patients report better understanding of e-prescriptions and higher satisfaction. Cost Reductions of about $18,750/year of staff time and $18,750/year of physicians’ time. This frees up time for 250 more patient visits per year.
DESCRIBE YOUR ROOT CAUSE ANALYSIS OF THE PROBLEM YOU WERE ADDRESSING.
The problem needed to be broken into two halves, with different root causes. “Five Why” and “Is-Is Not”methodologies were used. The root cause for a.) is a lack of training or diligence at the pharmacies.The root cause for b.) is lack of awareness among patients and a leniency in our office to enforce these requirements out of a motivation by our staff to be “patient-focused”.
DESCRIBE THE ACTIONS TAKEN TO ADDRESS EACH THE ROOT CAUSE(S) OF THE PROBLEM. INCLUDE THE TOOLS USED; PERSONNEL, RESOURCE AND TIME REQUIREMENTS, AND COSTS OF IMPLEMENTATION.a.) – Advising patients that their pharmacy made an error and asking for the name of the pharmacy. For repeat offenders, pharmacies’ names are elevated to the PHO level for follow up with their management.b.) – Create a consistent message to be used by all staff and the two doctors to gently reinforce the message of refills through e-prescriptions. Also, add a reminder message to the answering machine to reinforce the message.
DESCRIBE YOUR EFFORTS TO MONITOR AND EVALUATE THE PROCESS OVER TIMEWe have been following up with each receptionist and Office Manager every Friday for the past three months to assess progress
Office Manager, MA, Receptionists
Mercy PHO Port Huron, MI
DESCRIBE AND QUANTIFY (IF POSSIBLE) THE GOAL(S) AND TARGET(S) OF YOUR DESIRED SOLUTION
Anecdotally, it is reported that about 50% of patients are calling the Doctor’s Office for refills when they should be calling their pharmacy.
Our goal is to reduce these calls to about 10%, recognizing that some older patients will continue to call our office
Improving e-Prescription Use by Patients
23

© 2009 ASQ
THE RETURN ON INVESTMENT OF THE PROJECT
Net Return on Investment: Net Return on Investment: $37,500/year (staff time)$37,500/year (staff time)
OROR250 more patients seen per year250 more patients seen per year
Improving e-Prescription Use by Patients
© 2009 ASQ
1. NAME AND LOCATION OF ORGANIZATION/FACILITY/DEPARTMENTMercy-Physician Community PHO
2. TYPE AND SIZE OF ORGANIZATION/FACILITY/DEPARTMENTPrimary Care Office – Two doctors for Internal Medicine
3. FUNCTION(S)/MISSION OF ORGANIZATION/FACILITY/DEPARTMENT MAKING THE IMPROVEMENT
Support Staff
4. POSITION(S) OF THOSE INVOLVED IN THE PROJECT1 Office Manager (LEADER)2 Medical Assistants 2 Receptionists1 Quality Improvement Coach (QIC – Facilitator)
IDENTIFYING INFORMATION
24

© 2009 ASQ
• This doctor’s office had been using e-prescriptions for one year at the time of this project.
• Many people (up to 50% of patients) were still calling the doctor’s office for prescription refills when they should be calling their pharmacy.
• We identified two scenarios: 1.) The patient calls the pharmacy and they instruct the patient to call the doctor.2.) The patient calls the doctor’s office first instead of their pharmacy.
DESCRIPTION OF THE PROBLEM
© 2009 ASQ
• Anecdotally, it is reported that about 50% of patients are calling the doctor’s office for refills when they should be calling their pharmacy.
• Our goal was to reduce these calls to about 10%, recognizing that some older patients will continue to call our office.
• Conservatively, staff spend about 60 minutes per day talking to patients who are calling for prescription refills when they should be calling their pharmacy. The two doctors spend about 15 minutes per day talking to patients about this or advising the staff.
DESCRIPTION AND QUANTIFICATION OF THE GOAL(S) AND TARGET(S) OF THE DESIRED SOLUTION
25

© 2009 ASQ
The problem needed to be broken into two halves, with different root causes. The “Five Whys” and the “Is-Is Not” problem solving methodologies were used.
The root causes:1.) Lack of training or diligence at the pharmacies.
2.) Lack of awareness among patients and a leniency in our office to enforce these requirements out of a motivation by our staff to be patient-focused. This leniency is exaggerated by a lack of a consistent message from our staff to patients when they call.
THE ROOT CAUSE ANALYSIS OF THE PROBLEM
© 2009 ASQ
Root Cause 1Advising patients that their pharmacy made an error and asking for the name of the pharmacy. For repeat offenders, pharmacies’ names are elevated to the PHO level for follow-up with their management.
Root Cause 2Create a consistent message to be used by all staff and the two doctors to gently reinforce the message of refills through e-prescriptions. A flow chart was created and distributed to all staff and doctors. Training was conducted to ensure they understood how to use the consistent message. Also, we added a reminder message to the answering machine to reinforce to patients that their refills should be made through their pharmacy.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
26

© 2009 ASQ
Savings:
1. Receptionist, MA time taking phone calls:Approximately 300 minutes/week or 250 hours/year.If staff overhead = $75 per hour, cost = $18,750 per yearcost = $18,750 per year
2. Physicians instructing staff or taking phone calls:Approximately 75 minutes/week or 62.5 hours/year.If physician overhead = $300 per hour, cost = $18,750 yearcost = $18,750 year
More important: 62.5 hours per year of physicians’ time translates into 250 more patient visits per year.
Note: The members of the practice staff report increased satisfaction as they are not filling their days with these unnecessary telephone calls.
THE RETURN ON INVESTMENT OF THE PROJECT
© 2009 ASQ
• The quality improvement coach has been following up with each receptionist and office manager every Friday for the past three months to assess progress.
• Each member of the staff reports significant reductions and satisfaction that the consistent message and new answering machine language have solved the problem. Staff members report that calls have dropped to no more than six per week.
EFFORTS TO MONITOR AND EVALUATE THE PROCESS OVER TIME
27

28

© 2009 ASQ
Reduction in the Length of Stay (LOS) for Heart
Failure and Shock Patients (DRG 127)
Admitted to a Medium-Sized Hospital
J. Er RalstonVP and Client Relationship Executive
Juran Healthcare [email protected]
Joe DeFeoPresident, Juran Institute
Juran Healthcare [email protected]
Submitted by:
© 2009 ASQ
THE RETURN ON INVESTMENT OF THE PROJECT
Net Return on Investment:Net Return on Investment:• The pilot project was successful in reducing the average length of stay
at the hospital by nearly 50%, from 5.18 days on average to just 2.6. Further, 91% of patients were discharged in 4.1 days or less, anincrease of 34% from the original figure of 57%.
• The sustainability of this endeavor is what counts. After the pilot program ran its course, the improvement of statistics in the DRG 127 unit of this hospital continues to be outstanding.
• To this day, more than 80% of all inpatients leave the hospital before the 98-hour mark, and at an average of 3.6 days, the baseline of stay remains well below the Centers of Medicare & Medicaid geometric mean average of 4.1 days.
Reduction in the Length of Stay (LOS) for Heart Failure and Shock Patients (DRG 127) Admitted to a Medium-Sized Hospital
29

© 2009 ASQ
1. NAME AND LOCATION OF ORGANIZATION/FACILITY/DEPARTMENTJuran Client – Medium-sized Acute Care Hospital
2. TYPE AND SIZE OF ORGANIZATION/FACILITY/DEPARTMENTMedium-sized
3. FUNCTION(S)/MISSION OF ORGANIZATION/FACILITY/DEPARTMENT MAKING THE IMPROVEMENTThe project goal was to increase the percentage of patients with DRG 127 (heart failure and shock) that are discharged in less than 4.1 days to 95% in six months for a process sigma level of 3.18.
5. POSITION(S) OF THOSE INVOLVED IN THE PROJECTDirector of Quality – LEADERVP of Clinical Operations – Co-ChampionChief Nursing Officer – Co-ChampionClinical and Support Personnel (Representing nursing, physicians, case management, and finance)
IDENTIFYING INFORMATION
© 2009 ASQ
• A medium-sized acute care hospital wanted to decrease the amount of time that its DRG 127 patients (heart failure and shock) spent in care.
• The hospital had an average length of stay (ALOS) of 5.18 days, 1.08 days longer than the geometric mean length of stay, 4.1 days.
• In a one-year period this hospital saw 491 patients admitted to its DRG 127 division and only 280 of those patients, just 57%, were discharged in less than 98 hours. (4.1 days)
• The process sigma at this rate was 1.68. • This inefficiency resulted in an increased risk for negative
patient outcomes due to delays in the delivery of care as well as an increase in the overall cost of care.
DESCRIPTION OF THE PROBLEM
30

© 2009 ASQ
• The target goal of the project was to decrease the length of stay for inpatients in the DRG 127 unit from 5.18 days to less than 4.1 days.
• This decrease in allotted stay time would increase the amount of patients leaving the hospital in under 4.1 days from a very average 57% to an exemplary 95%.
DESCRIPTION AND QUANTIFICATION OF THE GOAL(S) AND TARGET(S) OF THE DESIRED SOLUTION
© 2009 ASQ
Initially, the Juran facilitated team came up with 18 hypothetical root causes to the problem. Following extensive data analysis, the team found 7 root causes that revealed themselves as the vital few problems driving the extended stay time. They were:
• CHF standard orders not used (no parameters)
• Delay between discharge order to time patient leaves floor
• Patient stay included a weekend
• Patient becomes deconditioned because of lack of activity
• Practices were not based on gold standards
• Patients held after meeting InterQual discharge criteria
• Inpatient holding process was not standardized
THE ROOT CAUSE ANALYSIS OF THE PROBLEM
31

© 2009 ASQ
Juran defined a possible solution strategy for each of the vital few root causes. Below is the analysis:
CHF standard orders – Reduce variation in practices by developing order set and interdisciplinary pathway and providing for education of physicians and hospital staff in their use.
Delay in DC order to leave floor – Develop a better communication process in relationship to anticipated discharge date/needs starting at day one of admission.
Weekend Stay – Develop staffing/resources plan to support CHF standard orders and pathway including scripting to facilitate use and discharge, and improving team-based communication and handoff for weekend stays. Standardize use of interdisciplinary pathway-based contingency DC orders.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
© 2009 ASQ
Patient deconditioning – Develop plan for activity and trigger for when a physical therapy evaluation is needed based on lack of progression of activity status.
Lack of gold standards – Create Gold Standards via standard orders and clinical pathway.
InterQual criteria – Utilize QMCs to address when discharge InterQualcriteria are met.
Patient holding – Develop ways to get patient out of the ED faster; improve and expedite care for patients who are held.
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
32

© 2009 ASQ
• The pilot project was successful in reducing the average length of stay at the hospital by nearly 50%, from 5.18 days on average to just 2.6. Further, 91% of patients were discharged in 4.1 days or less, an increase of 34% from the original figure of 57%.
• The sustainability of this endeavor is what counts. After the pilot program ran its course, the improvement of statistics in the DRG 127 unit of this hospital continues to be outstanding.
• To this day, more than 80% of all inpatients leave the hospital before the 98-hour mark, and at an average of 3.6 days, the baseline of stay remains well below the Centers of Medicare & Medicaid geometric mean average of 4.1 days.
THE RETURN ON INVESTMENT OF THE PROJECT
© 2009 ASQ
A control plan was developed to ensure the improvements and gains were sustained over the long term. Key elements included the control subjects (length of stay, readmission rate, and proven Xs), measurements (sensor, frequency, sample size), and actions (criteria for taking action, responsibilities). Most control subjects were monitored every two weeks, with criteria for action based on performance relative to specifications and statistical process control charts.
EFFORTS TO MONITOR AND EVALUATE THE PROCESS OVER TIME
33

© 2009 ASQ
YesNo
14
12
10
8
6
4
2
0
W a s the Pa t ie nt a n ER Hold Pt?
Tota
l Day
sBoxplot of Total Day s
Practical conclusion: Patients held in ED have a longer LOS than patients who go immediately to an inpatient floor.
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
© 2009 ASQ
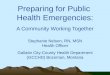
C a te go ry S a tF r iT huW e dT ueM onS un
6000
5000
4000
3000
2000
1000
0
Val
ue
E xp ec tedO b ser v ed
C ha r t o f O bs e r v e d a nd E x pe c te d V a lue s
Practical conclusion: The frequency of CHF-related tests is dependent on the day of week. Orders for tests occur less frequently on Saturday and Sunday, and more often on Monday and Tuesday.
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
34

© 2009 ASQ
Q 2 -20 09Q 1 -200 9Q 4 -200 8Q 3 -2 008Q 2 -200 8Q 1 -2 00 8
5 .5
5 .0
4 .5
4 .0
3 .5
3 .0
2 .5
2 .0
P o st-P ilo t T im e P erio d
LOS
(Day
s)
5 .18
2 .6
T im e S e rie s P lo t o f LO S
B ase line
Lev e l a ch ie v ed in p ilo t
To date, the average length of stay has been reduced 31%, from 5.18 days to 3.6 days, and continues to drop toward the level shown possible in the pilot.
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
35

36

© 2009 ASQ
Planning and Implementation of a Multidimensional Hand-Hygiene Program to Reduce
the Risk of Healthcare Associated Infections (HAI)
at Rapid City Regional Hospital (RCRH)
Submitted By:
Beth Boersma, LPN, CICInfection Control Assistant, RCRH, [email protected]
J.M. Keegan, MDChief Medical Officer,
Regional Health, Rapid City Regional Hospital
© 2009 ASQ
THE RETURN ON INVESTMENT OF THE PROJECT
NET PROJECT SAVINGS: NET PROJECT SAVINGS:
$291,450$291,450
Planning and Implementation of a Multidimensional Hand-Hygiene Program at RCRH
37

© 2009 ASQ
1. NAME AND LOCATION OF ORGANIZATION/FACILITY/DEPARTMENT
2. TYPE AND SIZE OF ORGANIZATION/FACILITY/DEPARTMENTRapid City Regional Hospital (RCRH) is a 326-bed, not-for-profit community acute care hospital, cancer care facility, and inpatient rehab facility.
3. FUNCTION(S)/MISSION OF ORGANIZATION/FACILITY/DEPARTMENT MAKING THE IMPROVEMENTRCRH is a community not-for-profit healthcare facility providing acute care to a geographically wide-spread area (250-mile radius); it also provides medical training for family practice medicine.
.4. POSITION(S) OF THOSE INVOLVED IN THE PROJECT
Infection Control Nurse - LEADER8 primary team members 8 other intermittent members representing all hospital patient-care departments
IDENTIFYING INFORMATION
Rapid City Regional Hospital – Rapid City, SD,
© 2009 ASQ
DESCRIPTION OF THE PROBLEM
A multidimensional hand-hygiene program was needed to improve hand-hygiene adherence at RCRH in accordance with The Joint Commission (TJC) Patient Safety Goal #7:
Reduce the risk of healthcare associated infections (HAI).
38

© 2009 ASQ
DESCRIPTION AND QUANTIFICATION OF THE GOAL(S) AND TARGET(S) OF THE DESIRED SOLUTION
Initial compliance with hand-hygiene standards was 57% (2004 baseline).
The improvement goal was established at 90% or better for the project beginning in 2005.
The initial HAI rate in 2004 was 4.3 per 1,000 patient-days.
No specific target rate was established; the desire was to achieve a level as close to 0.0 as possible.
© 2009 ASQ
THE ROOT CAUSE ANALYSIS OF THE PROBLEM
The primary reasons for non-compliance were established through direct observations, literature search, and 1:1 interviews with clinical staff.
The three primary reasons for non-compliance were identified as:
1. Takes too much time2. Dry, cracked hands from too much washing and
use of soap3. Non-supportive culture
39

© 2009 ASQ
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
ISSUE TOOLS USED “SOLUTION” PERSONNEL TIME REQUIRED COST OBSTACLES
Takes too much time
1:1 Interviews; brainstorming
Make alcohol hand rubs available: pocket-size, wall mount, and free standing
Purchasing, infection control, administration,
department directors
Initial supplies = 1 day (from warehouse
supply); gradual increase in
supplies over 3 years
Approximately $3300/month
Cost, labor (for installing
dispensers)
Soap is too drying
1:1 interviews; brainstorming
Make alcohol hand rubs available: pocket-size, wall mount, and free standing;
increase availability of hospital-approved lotion
Purchasing, infection control, administration,
department directors
Initial supplies = 1 day (from warehouse
supply); gradual increase in
supplies over 3 years
See above, plus additional cost
of lotion (roughly
$175/month)
Cost, labor (for installing dispensers)
Non-supportive
culture
Brainstorming Secured administration support; provided education (posters,
etc); 1:1 encouragement; infection control hot-line to
report non-compliances (non-punitive); hold physicians
accountable by informing CMO of non-compliances
Medical staff, infection control, administration,
department directors
Continual and on-going
Data not available –
most cost was for assorted
posters
Resistance to change
© 2009 ASQ
THE RETURN ON INVESTMENT OF THE PROJECT
Hand washing compliance: 2004 = 57% • 2008 = 91%
Hospital Acquired Infections (rate per 1,000 patient-days): 2004 = 4.33 • 2008 = 3.41 (21% reduction)
2005 average cost of HAI = $15,275 (conservative estimate, national)
Actual RCRH reduction in HAI from 2004 – 2008 = 30 cases at $15,275/case = $458,250 avoided cost
Total cost of materials and supplies from step 5 for 4 years = $166,800ROI = 458,250/166,800 = 2.75 275%
NET PROJECT SAVINGS = $291,450NET PROJECT SAVINGS = $291,450
40

© 2009 ASQ
EFFORTS TO MONITOR AND EVALUATE THE PROCESS OVER TIME
Individual departments audited and observed clinical personnel compliance in normal performance of duties.
Data was submitted to a central source for compilation monthly.
This process has been maintained throughout the past four years and is an ongoing activity.
HAI data is collected centrally, on a monthly basis, as part of normal infection control surveillance throughout the hospital.
© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
Hand Washing Monitoring FormMonth of Audit _______________________ Floor/Dept. Audit _________________________Tasks = # of opportunities to wash hands (If you cannot see it, do not record it) Soap and Water or Alcohol foamIf hand washing occurs, place a check mark ( ) in the appropriate column. If not, place a (0) in it.
41

© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
42

© 2009 ASQ
Discovering the “Cost of Current Quality”(COCQ) in a Family Medicine Practice
Submitted by:Michelle Valentine, MS
© 2009 ASQ
THE RETURN ON INVESTMENT OF THE PROJECT
Net Return on Investment:Net Return on Investment:
$90,000$90,000
Getting to Standardized Work at Waterford Medical Associates: The Dream Book
43

© 2009 ASQ
1. NAME AND LOCATION OF ORGANIZATION/FACILITY/DEPARTMENTSt. Johns Family Medical Associates
2. TYPE AND SIZE OF ORGANIZATION/FACILITY/DEPARTMENTModerate-sized Family Practice
3. FUNCTION(S)/MISSION OF ORGANIZATION/FACILITY/DEPARTMENT MAKING THE IMPROVEMENTProvision of Family Medical Care
4. POSITION(S) OF THOSE INVOLVED IN THE PROJECTCharlene DeBets – Supervisor (LEADER)Nicholas Urbanczyk – Physician Jennifer Wride – RNNashelle Simpson – BillerStephanie Nimmons – COA Michelle Valentine – Process Improvement Coach
IDENTIFYING INFORMATION
© 2009 ASQ
• The practice was asked to identify the most difficult, problematic, and least-liked process.
• All present at an all-staff meeting identified the processing of patient forms as being the most troublesome, e.g., processing forms brought to the practice by patients for completion by the practice staff (work-comp forms, disability forms, school physical forms, etc.).
• Patients were even leaving the practice because they could not get their forms in time.
• Process was taking up to two weeks to complete.
• Considerable physician time was tied up completing these forms.
DESCRIPTION OF THE PROBLEM
44

© 2009 ASQ
• Reduce the physician and staff time required for completing patient forms.
• Improve the throughput time required for completing patient forms.
• Reduce the stress on staff of having to interface with dissatisfied patients.
• Demonstrate the value of process improvement tools in a medical practice.
DESCRIPTION AND QUANTIFICATION OF THE GOAL(S) AND TARGET(S) OF THE DESIRED SOLUTION
© 2009 ASQ
The process used to process patient forms was inefficient, error-prone, and redundant.
THE ROOT CAUSE ANALYSIS OF THE PROBLEM
45

© 2009 ASQ
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
Creation of a value stream map of the current process identifying the wastes, redundancies, and delays in the process, i.e., the “cost of current quality.”
Management of Patient Medical FormsManagement of Patient Medical Forms
Receive form when
patient presen
ts
Receive form from
patient in
room
Inquire Re:DX
codes
Inbox message:
Is form complete
d?
Receive
patient phone call: Is form ready
?
MA distributes form to
doctor boxReceiv
e Form
By Mail / Fax
Form is
placed in MA box
Inbox message:
Is form
completed?
Doctorcompletes
form
Receive call
about form error
Receive form from
patient in
room
Receives finished
form from
doctor
Contact patient to pick up
form
Formerror
Receive call:
Is formready?
Fileform
at frontdesk
Give form
topatient
Inbox message
to doctor Re:
error
Is form
ready?Inquireaboutform
Inquireaboutform
Correction
done/ form
completed
Patientcalls Re:
Formstatus
Receivecall
complaintRe:
Form status
Current StateCurrent State
© 2009 ASQ
Creation of a value stream map of the current process, i.e., the “cost of current quality.”
Management of Patient Medical FormsManagement of Patient Medical Forms
Receive
Form When Patien
t Prese
ntsReceive
Form From Patien
t in Room
Inquire Re:DX
codes
In Box Message:Is Form
Completed?
Receive
patient
phone call: Is form ready
?
MA Distributes Form
To Doctor
BoxRecei
ve Form
By Mail / Fax
Form Is
Placed In MA Box
In Box Message:
Is Form
Completed?
DoctorCompletes
Form
Receive Call
About Form Error
Receive
Form From Patien
t in Room
Receives Finished
Form From
Doctor
Contact Patient to Pick up Form
Formerror
Receive Call:
Is FormReady?
Fileform
at frontdesk
Give form
topatient
Inbox Message
To Doctor re:
Error
Is Form
Ready?InquireAboutForm
InquireAboutForm
Correction
Done / Form
Completed
Patientcalls Re:
Formstatus
Receivecall
complaintRe:
form statusCurrent StateCurrent State
Practice Performance in the Current State
First Time Quality (FTQ) [% of time process is right the first time]: 1%Value/cost of total physician time spent/year in process = $ 130,000Value/cost of total staff time spent/year in process = $ 39,780
Value/cost of total practice time spent/year in process = $ 169,780
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
46

© 2009 ASQ
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
Instruction of practice staff in the use of some process improvement
tools for waste reduction
© 2009 ASQ
Working together, the practice staff used process improvement tools to dramatically improve the process:
Management of Patient Medical Management of Patient Medical FormsForms
END
Future StateFuture State
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
47

© 2009 ASQ
Working together, the practice staff used process improvement tools to dramatically improve the process:
Future State
Practice Performance in the Future State
First time quality (FTQ) = 72% !!!Value/cost of total physician time spent/year in process = $ 69,333This represented a hard savings of 2 full hours of physician time every day!
Value/cost of total staff time spent/year in process = $ 11,115This represented a hard savings of 5 full hours of staff time every day!
Value/cost of total staff time spent/year in process= $ 80,448PLUS: Process throughput time for forms was cut in half!
ACTIONS TAKEN TO ADDRESS THE ROOT CAUSE(S) OF THE PROBLEM, RESOURCES REQUIRED, AND OBSTACLES
© 2009 ASQ
THE RETURN ON INVESTEMENT OF THE PROJECT
Improvement in FTQ: From 1% to 72% Physician Time Cost Reduction/Year = $ 60,667Staff Time Cost Reduction/Year = $ 28, 665Total Practice Cost Reduction/Year = $ 89,332Percent Cost Reduction/Year = 52%
• There is documented proof of $90,000 in hard dollar annual savings from having “leaned” just one irksome process [a process that is common to ALL primary care practices!].
• Energized staff and physicians are eager for more improvement.
• Can be done without outside help.
48

© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
49

© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
1. 1. Were you aware of process flow mapping before you Were you aware of process flow mapping before you participated?participated?Biller: I heard things about it, but never really got information as to what
it was all about.Doc: NoCOA: Just a littleNurse: Not reallyP.Mgr.: Some
2. 2. Was the process we chose to look at relevant?Was the process we chose to look at relevant?Biller: Oh yes, it was so relevant. It was actually the perfect process.Doc: Yes, it was one of the frustrating paperwork issues in the office.COA: YesNurse: YesP.Mgr.: Yes, the staff chose the process that frustrated them a lot.
Results of Post-Intervention Staff Evaluation Survey
© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
3. Was the process fun?3. Was the process fun?Biller: It was a lot of fun, most of all very interesting. Doc: YesCOA: Yes, it’s almost like starting a new career.Nurse: YesP.Mgr.: Michelle made learning fun and rewarding.
4. Was the process valuable to you?4. Was the process valuable to you?Biller: It was so valuable to me; I plan to do a value stream mapping on
my personal life.Doc: Yes, to improve work flow, MA time management – focus patient
care issues.COA: Yes, it made a lot of sense; also a lot of knowledge was put into
this project.Nurse: Very much so.P.Mgr.: It pinpoints the root cause so you can remove waste.
Results of Post-Intervention Staff Evaluation Survey
50

© 2009 ASQ
5. Was the process valuable to the practice?5. Was the process valuable to the practice?Biller: It is definitely valuable to the practice; it will help eliminate wasted
time and chaos.Doc: Need to examine, work burden may have shifted to medical
records.COA: The process was very valuable and will most definitely keep our
customers happy with our practice.Nurse: AbsolutelyP.Mgr.: Yes, we will use it over and over again to continue to remove
waste from our daily processes.
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
Results of Post-Intervention Staff Evaluation Survey
© 2009 ASQ
6. Do you understand more about finding and dealing with waste?6. Do you understand more about finding and dealing with waste?Biller: I have learned so much. I have more knowledge of the process
coming out.Doc: Yes, finding waste is easy; dealing with waste is the trouble.COA: Yes, the process will most definitely cut cost and waste.Nurse: YesP.Mgr.: Absolutely! FTQ and error proofing should be everyday terms.
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
Results of Post-Intervention Staff Evaluation Survey
51

© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
Results of Post-Intervention Staff Evaluation Survey7.7. Are you interested in participating in more process improvement Are you interested in participating in more process improvement
activities at the practice?activities at the practice?Biller: I wouldn’t mind being a part of that.Doc: Yes, I have several in mind.COA: Whatever makes our practice stand out.Nurse: Sure, anytime.P.Mgr.: We’re not going to stop now that we have the tools.
© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
Results of Post-Intervention Staff Evaluation Survey8.8. Are you interested in learning more about process Are you interested in learning more about process
improvement?improvement?Biller: Yes, I would love to learn more and to apply it to the workplace.
If it will better our practice and make our customers feel better, then it is well worth the effort.
Doc: I feel that I have enough tools to go forward.COA: YesNurse: YesP.Mgr.: Anything that helps us to achieve and maintain excellence is
worth learning.
52

© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
Results of Post-Intervention Staff Evaluation Survey9.9. Did you learn anything?Did you learn anything?
Biller: I’ve learned a lot. How much time is being wasted, and how much unnecessary rework we do here in the practice. Value stream mapping is forever needed to have success or be successful in your practice, business, and/or company.
Doc: Yes: (a) a problem of complexity can be slimmed down and (b) to take one problem at a time.
COA: This waste process was very helpful to take an inventory on yourlife as well. You can take this process to make changes in your as well.
Nurse: Yes: Anyone can help make changes and improve processes.P.Mgr.: Yes: It isn’t hard to break down the parts of a process and build it
the best way.
© 2009 ASQ
10.10. What did you like best about the process?What did you like best about the process?Biller: I liked that it would cut down on a lot of wasted time, stress,
and chaos. That is saves money, time, and everyone will be happy.
Doc: Looking at a simple, frustrating problem and developing a simple solution.
COA: I like that this process will benefit throughout your daily process as well as your weekly process.
Nurse: It actually works and improves office flow.P.Mgr.: How easy it actually is to see where we need to eliminate waste.
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
Results of Post-Intervention Staff Evaluation Survey
53

© 2009 ASQ
ILLUSTRATIONS OF THE PROBLEMS AND/OR SOLUTIONS
Results of Post-Intervention Staff Evaluation Survey11.11. What did you like least about the process?What did you like least about the process?
Biller: After learning what this was all about and the knowledge I have gained from this entire process, there is nothing that I least like about it. The whole process was fun and interesting.
Doc: We need to be careful not to just shift the “work burden” to another area in the office.
COA: Everything was great. The process itself will save a lot of time.Nurse: Well, no one really likes homework, do they?P.Mgr.: Nothing to dislike about the process. Honing up on my computer
skills to present a nice layout is necessary.
54

Appendix

Executive Summary ASQ White Paper on Healthcare Reform July 16, 2009 The need for reforming how our country delivers healthcare seems to be well accepted by most if not all stakeholders. The difficult question is how can the delivery of healthcare be reformed to provide the most value to the most number of people in our country at the least cost. Congress is currently consumed by looking for ways to finance the projected $1 trillion ten-year cost of healthcare legislation on the table. But rather than merely devising ways to pay for an existing, unsatisfactory product, ASQ believes that breakthroughs in healthcare reform can and should also come about through the design of a new product that is less costly and more effective. We therefore feel that more attention ought to be paid to efforts to improving the process of care by asking and demanding answers to such questions as
1. “How to rationalize the processes of care?” and 2. “How to remove the many forms of waste?” (which by some estimates consumes up to
60 cents of every health care dollar spent in the United States). There are many, many questions such as these but there are five areas we find most troubling in the health care sector and which we feel are most in need of serious attention:
� WWaste: ASQ believes there should be meaningful incentives and requirements for waste reduction embedded in whatever healthcare reform legislation emerges from Congress. Such measures should be aimed at minimizing or eliminating overuse, underuse, and mis-use of health care, and at creating a culture of sustainable process improvement and quality management throughout the healthcare sector.
� IIncentive al ignment: ASQ believes that legislation must address the lack of standards (and thus accountability) for excellence and cost-effectiveness in the administrative side of healthcare. We also believe there ought to be provisions to support demonstrations and rapid adoption of proven methods for incenting financial accountability for excellence in operations and results in all aspects of healthcare (clinical and operational).
� IInformation technology implementation: To fully and sustainably capitalize on the coming investment of stimulus dollars in health IT, steps must first be taken to re-engineer healthcare practice environments (including their cultures) for increased efficiency, quality, satisfaction, and optimum preparedness for the introduction of new technologies. ASQ believes legislation must assist and encourage providers to lay the groundwork for successful IT implementation by making processes and workflow lean and robust and fashioning cultural environments where these new technologies can take root.

� SSustainable cul ture change: ASQ believes that the most critical need of all in healthcare reform is for meaningful, lasting changes in the deeply embedded cultures related to health and healthcare in this country. These changes include adoption of different behaviors and attitudes regarding personal health; adoption of participatory, team-based models focused not on blame for wrong-doing but on joint problem solving to avoid repetition of adverse effects; and rapid evolution to a culture of quality and continuous improvement.
� WWorkforce education and expectations: ASQ believes legislation needs to address preparation of the 21st century healthcare workforce for new realities, roles and responsibilities. Reengineering of the education and training of providers should accommodate not only new clinical thinking and procedures but a new focus on the patient, on populations, on culture change, on process improvement and quality management, on team-based care and thinking, on cost containment, on cultural competence, on prevention and chronic care management, and on the widespread and pervasive use of health information technology.
These five areas are covered in more depth in an ASQ white paper on healthcare reform. Lastly, ASQ believes that legislation must encourage and assist the healthcare sector to utilize the quality principles of process and continuous improvement by calling for training and consultations in the use of appropriate tools and by providing that federal funds tied to the sector require their use. Specific activities that healthcare reform legislation should promote include:
� Development, evaluation, testing, and deployment of valid measures and metrics for the evaluation of the non-clinical, operational performance and efficiency of health care providers;
� Support for training to improve the knowledge and skills of health care stakeholders (at all levels and settings) in the concepts and sciences of continuous quality and process improvement, culture change, and sustainability;
� Use of recognized, proven quality and process improvement tools and methodologies for the analysis and evaluation of excess operational wastes, poor sustainability, poor transferability, and/or other functional or operational process deficiencies.
Paying appropriate attention to these steps for improving the process of care has the potential to free up sufficient resources to meet the wide-ranging aims of healthcare reform in the United States. For further details on how process improvement can be used to reform the healthcare system, please contact John Ryan at ASQ headquarters ([email protected] or telephone 1-800-248-1946 ext. 7244) and request a copy of ASQ’s comprehensive Healthcare Reform White Paper.

9/9/09 11:47 AMFirst, lay groundwork for IT adoption - Modern Healthcare
Page 1 of 3file:///Volumes/PUBLIC/4%20Case%20Studies%20HC/Final/Appendices/F…20groundwork%20for%20IT%20adoption%20-%20Modern%20Healthcare.htm
Joseph Fortuna
Reprinted with permission.
Article published August 18, 2009
First, lay groundwork for ITadoptionBy Joseph FortunaPosted: August 18, 2009 - 9:00 am EDT
There are few healthcare organizations that are fully prepared to adoptthe kind of health information technology, or HIT, systems that areneeded to take healthcare quality and patient safety to the next level.Across broad swaths of the healthcare system, there is much to gainand much waste to eliminate by using lean processes to improve workand workflow before we spend massive amounts on informationtechnology.
Healthcare is one of the last of this country's major economic sectors to effectively andpervasively embrace and adopt the use of information technology. The government's stimulusact attempts to address this situation with far-reaching provisions promoting HIT. Thesesweeping provisions acknowledge that much of the planning for health reform in this country willdepend on the ability to effectively deploy HIT expeditiously and effectively.
The new policy directions, backed up by billions of dollars in funding, have the potential to puthealthcare on the fast track to embrace, deploy and spread effective and efficient use of healthIT as quickly and completely as possible.
Many things need to be done in a systematic fashion to prepare for this rapid infusion of dollarsand culture-changing technology. Understanding three key principles will help enhance thesuccessful introduction of this far-reaching technological change.
First, HIT and related technologies are potentially effective tools to be used in the quest forbetter, more cost-effective and more accessible healthcare, but they cannot and should not be

9/9/09 11:47 AMFirst, lay groundwork for IT adoption - Modern Healthcare
Page 2 of 3file:///Volumes/PUBLIC/4%20Case%20Studies%20HC/Final/Appendices/F…20groundwork%20for%20IT%20adoption%20-%20Modern%20Healthcare.htm
better, more cost-effective and more accessible healthcare, but they cannot and should not beexpected, by themselves, to achieve those results.
Second, the business environments into which health IT is to be introduced should be fullyprepared for the change. In many cases, the first and most-effective thing to be done in apractice is to rationalize the process flow of the work. Even the best health IT modalities will notwork as designed if the business environment where they are placed is operating in an earliercentury.
Third, change is difficult, and nowhere more so than in medical practices that are overburdenedwith waste, paperwork, thinning profit margins and inadequate time to provide care. Thoseassisting practices to implement anything new, be it HIT, patient-centered medical home oranything else, must spend time understanding the environments they are working in and thepeople who work in those environments, and helping them to adopt and embrace change andto adopt new cultures—cultures of quality, continuous improvement, patient-centeredness andpatient safety.
One of the linchpins in the national strategy of effecting widespread adoption of health IT—theRegional Health IT Extension Center program—offers many opportunities to put theseprinciples to work.
Through RHITEC, healthcare providers all over the country could be assisted in a number ofways: In analyzing, assessing and—where necessary—re-engineering their practiceenvironments and cultures for increased efficiency, quality, satisfaction and optimumpreparedness for the introduction of new information technologies; in making the right choicesfor their practices and facilities from among the numerous genres of electronic functionality thatexist; in thoroughly preparing their environments and their personnel for the technical and socialchanges introduced by the adoption of the correct technology for them; in comparison shoppingfrom among the many brand choices for their chosen technology; in successfully negotiatingwith the vendors of such products; and, finally, in monitoring the use and effectiveness of theseimportant resources.
The proven and validated tools, philosophies and methodologies of quality management,change management and process improvement can be of immense help in the work of theRHITEC program. The American Society for Quality, whose members have been using themeffectively for decades in many industries and environments all over the world, has urged theOffice of the National Coordinator for Health Information Technology to take these factors intoconsideration in its efforts to plan and coordinate successful adoption of new informationtechnologies.
To fully and sustainably capitalize on the coming investment of stimulus dollars in health IT,these steps must first be taken to re-engineer healthcare practice environments (including theircultures) for increased efficiency, quality, satisfaction and optimum preparedness for theintroduction of new technologies. ASQ quality coaches, who have been volunteering their timeand expertise, are demonstrating success assisting physician practices in rationalizing the flowof work.
We'll just be throwing money down a hole if we fail to lay the groundwork for successful ITimplementation by making processes lean and robust and fashioning cultural environmentswhere these new technologies can take root.

9/9/09 11:47 AMFirst, lay groundwork for IT adoption - Modern Healthcare
Page 3 of 3file:///Volumes/PUBLIC/4%20Case%20Studies%20HC/Final/Appendices/F…20groundwork%20for%20IT%20adoption%20-%20Modern%20Healthcare.htm
where these new technologies can take root.
Joseph Fortuna, a physician, is chairman-elect of the healthcare division of the AmericanSociety for Quality.
What do you think? Post a comment on this article and share your opinion with other readers.Submit your comments to Modern Healthcare Online at [email protected] be sure to include your hometown and state, along with your organization and title.
Related ArticlesMedical-device maker Delcath to add jobs in NY September 04, 2009CCHIT splits EHR certification into two tiers September 04, 2009AHRQ to survey docs, providers on e-prescribing September 04, 2009Pharmacists ask HHS to change HITECH provisions September 04, 2009Failed Minnesota health software ends up in court September 04, 2009More Related Articles >>
Modern Healthcare is the industry's most trusted, credible and relied-upon news source. In print and online, ModernHealthcare examines the most pressing healthcare issues and provides executives with the information they needto make the most informed business decisions and lead their organizations to success. It's for this reason ModernHealthcare is deemed a "must-read publication" by the who's who in healthcare.
For more healthcare business news, visit http://www.modernhealthcare.com/.

June 10, 2009 Office of the National Coordinator for Health Information Technology 200 Independence Ave, SW., Suite 729D Washington, DC 20201 Attention: Health IT Extension Program Comments. [email protected]
Dear Sir/Madam: I am writing as President of the American Society for Quality (ASQ) in response to your notice on May 28, 2009 in the Federal Register1 announcing the draft description of the program for establishing regional centers to assist providers seeking to adopt and become meaningful users of health information technology, as required under Section 3012(c) of the Public Health Service Act, as added by the American Recovery and Reinvestment Act of 2009 (Pub. L. 111-5) (ARRA) and soliciting comments on that draft description. The American Society for Quality (ASQ) is a community of more than 90,000 quality experts in all sectors of the economy whose members are dedicated to the promotion and advancement of quality and process improvement tools, principles, and practices in their workplaces and in their communities. By making quality a priority, an organizational imperative, and a personal ethic, ASQ has become the community of choice for all who seek quality technology, concepts, or tools to improve themselves and their world. ASQ also administers the Malcolm Baldrige National Quality Program (MBNQP) under a contract with the National Institute of Standards and Technology (NIST). As America engages in a long overdue dissection, analysis, and restructuring of the ways in which we prevent disease, receive and finance healthcare, and manage and utilize health care technology, ASQ stands as a valued partner for those struggling to control runaway health care costs, deploy useful technologies, make health care safer, and improve accessibility to high quality, cost-efficient care. Put simply, and paraphrasing a well known advertising slogan, “We do not provide healthcare. We help those that do, do it better.” Nowhere is this slogan more applicable than in the evolving world of Health IT(HIT). Healthcare is one of the last of this country’s major economic sectors to effectively and pervasively embrace and adopt the use of information technology. We believe that thanks to your efforts and the efforts of others healthcare is now on a fast track to embrace, deploy and spread effective and efficient use of Health IT as quickly and completely as possible.
1 Federal Register: May 28, 2009 (Volume 74, Number 101)] [Notices] [Page 25550-25552]

Much of the planning for health reform in this country will depend on our ability to effectively deploy HIT expeditiously and effectively. It is a situation not unlike that which obtained when John Kennedy promised America that we would have a man on the moon within ten years. In signing the ARRA (which provides considerable funding and logistical support for Health IT), President Obama must have had similar thoughts in mind about the implementation of Health IT, only with a much shorter timetable. One of the lynchpins in this national strategy of effecting widespread adoption of health IT is the very program that is described in the above-referenced public notice, the Regional Health IT Extension Center Program (RHITEC). Through this program health care providers all over the country could be assisted
� in analyzing, assessing and—where necessary—re-engineering their practice environments and cultures for increased efficiency, quality, satisfaction, and optimum preparedness for the introduction of new information technologies;
� in making the right choices for their practices and facilities from among the numerous genres of electronic functionality that exist;
� in thoroughly preparing their environments and their personnel for the technical and social changes introduced by the adoption of the correct technology for them;
� in comparison shopping from among the many brand choices for their chosen technology;
� in successfully negotiating with the vendors of such products, and, finally, � in monitoring the use and effectiveness of these important resources.
We at ASQ applaud this important effort and are writing to offer some modest suggestions for enhancing its success. These suggestions are based on the experiences and training of our ASQ members and the ASQ Quality Body of Knowledge (QBOK) which have together resulted in considerable success in many, many industries and environments all over the world that have faced similar challenges. These suggestions center around a few key principles:
� HIT and related technologies are potentially effective tools to be used in the quest for better, more cost-effective, and more accessible health care. They cannot and should not be expected, by themselves, to achieve those results.
� Consultation and assistance in healthcare environments should strive first to create fertile ground for the sowing of the seeds of health IT. The best health IT modalities will not work if the business environment into which they are placed is operating in an earlier century. In some cases the most effective thing to be done in a practice is to rationalize the process flow of the work.
� “Change is hell” and nowhere is it more hellish than in medical practices that are overburdened with waste, paperwork, thinning profit margins, and inadequate time to provide care. Those assisting practices to implement anything new, be it HIT, patient-centered medical home, or anything else, must spend time understanding the environments they are working in and the people who work in those environments, and helping them to adopt and embrace change and to adopt new cultures, e.g. cultures of quality, continuous improvement, patient-centeredness, patient safety, etc.

� The proven and validated tools, philosophies, and methodologies of quality management, change management, and process improvement can be of immense help in the work of the RHITEC Program. ASQ and its 90,000 members have been using them effectively for decades and stand ready to assist the ONC to incorporate them successfully into the work of RHITEC.
As evidence of our commitment in this regard ASQ and its geographically-based Sections are working with regional health care coalitions in several areas of the country to launch its “New Marshall Plan” under which, after comprehensive training about the medical practice environment, ASQ volunteer process engineers, change agents, and quality managers can, using a standardized work plan, assist practices and their staffs in interested communities to analyze and improve practice process flows, eliminate waste, reduce costs, and seamlessly introduce new functionalities such as HIT, Patient Centered Care, patient safety, etc. One such program in Michigan has already resulted in a reduction in one primary care practice of $90,000 annually in just one of their office processes, giving them 2 more hours of physician time and 6 more hours of medical assistant time each day. This was achieved by the staff themselves after a brief orientation to the process improvement tool that was used: value-stream mapping (VSM). VSM is familiar to every process engineer in industry. A hallmark of these programs is that the volunteers are there not as consultants, but as coaches and mentors. They are giving the practices a fishing pole and teaching them to fish, not giving them fish to eat. As plans evolve for this new and exciting program we would welcome the opportunity to advise you and your staff in the construction of its activities. We hope that you will also find the attached comments helpful in your work of rolling out this program. Should you have questions or wish to discuss any of these comments and suggestions from ASQ, please contact John Ryan of our headquarters staff--email [email protected] or telephone 800-248-1946 ext. 7244. Sincerely,
Roberto M. Saco President American Society for Quality

Comments from ASQ On the Draft Description of the Program for Establishing
Health Information Technology Regional Extension Centers
June 10, 2009
Submitted to the Office of the National Coordinator for Health Information Technology Pursuant to solicitation for comments in Federal Register [DOCID:fr28my09-67]
Pages 25550-25552

[Federal Register: May 28, 2009 (Volume 74, Number 101)] [Notices] [Page 25550-25552] From the Federal Register Online via GPO Access [wais.access.gpo.gov] [DOCID:fr28my09-67] ======================================================================= ----------------------------------------------------------------------- DEPARTMENT OF HEALTH AND HUMAN SERVICES Office of the National Coordinator for Health Information Technology; Health Information Technology Extension Program ACTION: Notice and request for comments. ----------------------------------------------------------------------- SUMMARY: This notice announces the draft description of the program for establishing regional centers to assist providers seeking to adopt and become meaningful users of health information technology, as required under Section 3012(c) of the Public Health Service Act, as added by the American Recovery and Reinvestment Act of 2009 (Pub. L. 111-5) (ARRA). DATES: All comments on the draft Plan should be received no later than 5 p.m. on June 11, 2009. ADDRESSES: Electronic responses are preferred and should be addressed to [email protected]. Written comments may also be submitted and should be addressed to the Office of the National Coordinator for Health Information Technology, 200 Independence Ave, SW., Suite 729D, Washington, DC 20201, Attention: Health IT Extension Program Comments. FOR FURTHER INFORMATION CONTACT: The Office of the National Coordinator for Health, Information Technology, 200 Independence Ave, SW., Suite 729D, Washington, DC 20201, Phone 202-690-7151, E-mail: [email protected]. SUPPLEMENTARY INFORMATION:
I. Background The American Recovery and Reinvestment Act of 2009 (Pub. L. 111-5) (ARRA) includes
provisions to promote the adoption of interoperable health information technology A to
promote meaningful use of health information technologyB
1 to improve the quality and
value of American health careC
. These provisions are set forth in Title XIII of Division A and
1 Unintended Consequences of In fo rmation Technologies in Health Ca re —An Inte ractive Sociotechnical Analysis, Michael I. Harrison, PhDa,
*, Ross Koppel, PhDb and Shirly Bar-Lev, PhDc,, Journal of the American Medical In fo rmatics Association 2007;14(5):542-549

Title IV of Division B, which may together be cited as the ``Health Information Technology for Economic and Clinical Health Act'' or the ``HITECH Act''. The ARRA appropriates a total of $2 billion in discretionary funding, in addition to incentive payments under the Medicare and Medicaid programs for providers' adoption and meaningful use of certified electronic health record technology. Providers that seek to adopt and effectively use health information technology (health IT) face a complex variety of tasks. Those tasks include assessing needs, selecting and negotiating with a system vendor or reseller, and implementing workflow changes to improve
clinical performance and, ult imately, outcomesD
. Past experiences have shown that without robust technical assistance, many EHRs that are purchased are never installed or are not used by some providers. Section 3012 of the Public Health Service Act (PHSA), as added by the HITECH Act, authorizes a Health Information Technology Extension Program to make assistance available to all providers, but with priority given to assisting specific types of providers. By statute, the health information technology extension program (or ``Extension Program'') consists of a National Health Information Technology Research Center (HITRC) and Regional Extension Centers (or ``regional centers''). The major focus for the Centers' work with most of the providers that they serve will be to help to select and successful ly implement certif ied e lectronic health records
(EHRs)E. While those providers that have already implemented a basic EHR may not require
implementation assistance, they may require other technical assistance to achieve
``meaningful user' ' statusF
. All regional centers will assist adopters to effectively meet or exceed the requirements to be determined a ``meaningful user'' for purposes of earning the incentives authorized under Title IV of Division B. Lessons learned in the support of providers, both before and after their initial implementation of the EHR, will be shared among the regional centers and made publicly available. The HITECH Act prioritizes access to health information technology for uninsured, underinsured, historically underserved and other special-needs populations, and use of that technology to achieve reduction in health disparities. The Extension Program will include provisions in both the HITRC and regional centers awards to assure that the program addresses the unique needs of providers serving American Indian and Alaska Native, non-English-speaking and other historically underserved populations, as well as those that serve patients with maternal, child, long-term care, and behavioral health needs. II. Detailed Explanation and Goals of the Program The HITECH Act directs the Secretary of Health and Human Services, through the Office of the National Coordinator for Health Information Technology (ONC), to establish Health Information Technology Regional Extension Centers to provide technical assistance and disseminate best practices and other information learned from the Center to support and accelerate efforts to adopt,implement and effectively ut i l ize health information
technologyG
. In developing and implementing this and other programs pursuant to the HITECH Act, ONC is consulting with other Federal agencies with demonstrated experience and expertise in information technology services, such as the National Institute of Standards and Technology. We propose that the goals of the regional center program should be to:
--Encourage adoption of electronic health recordsH
by clinicians and hospitals;

--Assist clinicians and hospitals to become meaningful users of electronic health
recordsI; and
--Increase the probability that adopters of electronic health record systems wi ll
become meaningful users of the technologyJ
. The HITECH Act states that ``the objective of the regional centers is to enhance and promote the adoption of health information technology through-- (A) Assistance with the implementation, effective use, upgrading, and ongoing
maintenanceK
of health information technology, including electronic health records, to healthcare providers nationwide;
(B) broad participation of individuals from industryL
, universities, and State governments; (C) active dissemination of best pract ices and research on the implementation,
effective use, upgrading, and ongoing maintenance of health information
technology, including electronic health recordsM
, to health care providers in order to improve the quality of healthcare and protect the privacy and security of health information;
(D) participation, to the extent practicable, in health information exchangesN
; (E) utilization, when appropriate, of the expertise and capability that exists in Federal agencies
other than the Department; and (F) integration of health information technology, including electronic health records,
into the init ia l and ongoing training of health professionals and others in the healthcare industry that would be instrumental to improving the quality of healthcare through the smooth and accurate electronic use and exchange of
health informationO
.' ' To achieve the centers' statutory objectives, we propose to establish regional centers to offer to all providers in a designated region access to information and to some level of assistance. The regional centers will become, upon award, members of a consortium that will be coordinated and facilitated by the Health Information Technology Research Center (HITRC) that the Secretary is directed to establish by Section 3012(b) of the PHSA as added by the HITECH Act. Whereas research and analysis of best practices regarding health IT utilization rests primarily with the HITRC, dissemination and implementation of those best practices learned from the HITRC will rest with the regional centers. Per Section 3012(c)(4) of the PHSA as added by the HITECH Act, each regional center shall ``aim to provide assistance and education to all providers in a region but shall prioritize any direct assistance first to the following:
� Public or not-for-profit hospitals or critical-access hospitals. � Federally qualified health centers (as defined in section 1861(aa)(4) of the Social Security Act). � Entities that are located in rural and other areas that serve uninsured, underinsured, and
medically underserved individuals (regardless of whether such area is urban or rural). � Individual or small group practices (or a consortium thereof) that are primarily focused on
primary careP
.'' Regional centers will therefore, as a core purpose of their establishment, furnish d irect,
individualized, and (as needed) on-site assistance to individual providersQ
. This intensive assistance is, per statute, to be prioritized to providers identified in the statute. We expect

that on-site assistance will be a key service offered by the regional centers to providers prioritized by the statute for direct assistance, and will represent a significant portion of the regional centers' activities. Because of the nationwide scope of the Medicare and Medicaid payment incentives for adoption and meaningful use of certified EHRs, the Extension Program should provide at least a minimal level of technical assistance across the nation. We propose that the minimal level of support must include the provision of unbiased information on mechanisms to exchange health information in compliance with applicable statutory and regulatory requirements, and information to support the effective integration of health information exchange
activit ies into practice workflowR
. It is expected that each regional center will provide technical assistance within a defined geographic area, and that each defined geographic area will be served by only one center. At a minimum, the support should consist of materials designed to be widely and rapidly disseminated, both for provider self-study and for use by entit ies other than regional centers that have an interest and the
abil ity to provide some assistance and information to providers adopting health ITS
. As required by Section 3012(c)(8) of the Public Health Service Act as added by the HITECH Act, all regional centers will be evaluated to ensure they are meeting the needs of the health
providersT
in their geographic area in a manner consistent with specified statutory objectives. All lessons learned from these efforts will be exchanged across regional centers, and with other stakeholders, including but not limited to other federal programs, to promote the availability of highly effective support to providers across the nation. All regional centers will be expected to use the lessons learned as important, but not the only, information to guide their internal self-evaluation and ongoing improvement processes. A. Criteria for Determining Qualified Applicants Section 3012(c)(2) of the PHSA as added by the HITECH Act requires that: ``Regional centers shall be affiliated with any United States-based nonprofit organization, or group thereof, that applies and is awarded financial assistance under this section. Individual awards shall be decided on the basis of merit.'' In addition, we propose the following requirements and preference criteria. Required Criteria may include: 1. Define the geographic region and the provider population within that region it proposes to serve. 2. Describe proposed levels and approaches of support for prioritized and other providers to be
served. 3. Address how the applicant would structure its organization and staffing to enable providers
served to have ready access to reasonably local health IT ``extension agents'' and provide training and on-going support for these critical workers.
4. Demonstrate the capacity to facilitate and support cooperation among local providers, health systems, communities, and health information exchanges.
5. Demonstrate that the applicant is able to meet the needs of providers prioritized for direct assistance by Section 3012(c)(4) of the PHSA as added by the HITECH Act.
6. Propose an efficient and feasible strategy to furnish deep special ized expertise ( in such areas as organizational development, legal issues, privacy and security, economic and financing issues, and evaluation) broadly to all providers served and intensive, individualized, `` local' ' presence from an interdisciplinary
extension agent to smaller groups of providers assigned to individual agentsU
. Preference Criteria may include:

We propose to give preference to proposed regional center organizational plans and implementation strategies incorporating multi- stakeholder collaborations that leverage local resources. The local stakeholders and resources that applicants may wish to consider including in some combination, though not limited to, the following: 1. Public and/or private universities with health professions, informatics, and allied health
programs; 2. state or regional medical/professional societies and other provider organizations; 3. federally recognized state primary care associations; 4. state or regional hospital organizations; 5. large health centers and networks of rural and/or community health centers; 6. other relevant health professional organizations; 7. the regionally relevant state Area Health Education Center(s); 8. health information exchange organizations serving providers in theregion; 9. the Medicare Quality Improvement Organization(s)(QIO(s) serving providers that the proposed
regional center aims to serve; 10. state and tribal government entities in the center's geographic service area including, but not
limited to, public health agencies; libraries and information centers with health professional and community outreach programs; and
11. consumer/patient organizations 12. Add #12: associations of quali ty and process improvement professionals (such as
the American Society for Quality [ASQ]) with collect ive and individual expertise in work organization, STS, quality management, process improvement, culture
change, change management, and related sciencesV
.
As noted below, we propose to give preference to applicants identifying viable sources of matching funds. Viable sources could include grants from states, non-profit foundations, and payment for services from providers able to make such payment. For example, Medicaid providers could choose to contract with a regional center in lieu of a corporate vendor for implementation and meaningful use support services, for which costs are reimbursable under Section 1903 of the Social Security Act, as amended by the HITECH Act. A regional center could also, theoretically, seek to establish itself as a first-choice source of assistance that would realize net retained earnings on service to non-prioritized providers and use those retained earnings as a source of matching funds for its grant-funded activities. B. Maximum Support Levels Expected To Be Available to Centers Under the Program Given current national economic conditions, we propose to exercise the option in the HITECH Act to not require matching funds for awards made in FY 2010. We will encourage use of matching funds and the coordination of existing resources to strengthen proposals for regional centers and potentially expand the number of providers that can be assisted. Review criteria may be established that give preference to proposals including matching funds but that do not automatically preclude otherwise technically meritorious proposals that do not include matching funds. We propose using ARRA funding for two-year awards made in FY2010 and furnishing providers in awardees' areas with robust support. While we expect the actual ARRA funding awarded per center will vary based on the number and types of providers proposed to be served, and the amount of matching funds proposed by each regional center, we anticipate an average award value on the order of $1 million to $2 million per center. The maximum award value we anticipate making available to any one regional center is $10 million. Funding may also be approximately allocated to the regional

centers in relative proportion to the numbers of prioritized direct assistance recipients identified in the HITECH Act. C. Procedures To Be Followed by the Applicants Timelines This notice makes public and invites comments on the draft description of the regional centers program and is not a solicitation of proposals to serve as extension centers under this program. The Federal Government will award funding for the regional centers through a solicitation of proposals, after considering the comments obtained through this notice. The availability of this solicitation will be broadly announced through appropriate and familiar means, including publication in the Federal Register of a Notice of the solicitation's availability. This announcement of the solicitation will provide further details on the finalized requirements and application process for regional centers, pursuant to and in compliance with all applicable statutes and regulations, including but not limited to the Paperwork Reduction Act (44 U.S.C. 3501 et seq.). Applicants well prepared to provide robust extension services will likely need at least two months to provide high quality proposals. It is expected, however, that other potential applicants will need more time to prepare proposals. We propose to make initial awards for regional centers as early as the first quarter of FY2010 and continuing through the fourth quarter of FY2010. Multiple, closely spaced proposal submission dates will be established to allow each geographic area to begin receiving benefit of a regional center as soon as possible. We believe this approach is necessary to allow areas with well prepared applicants to begin work sooner, without excluding from consideration those areas where the best applicants require more time to convene a multi-stakeholder collaboration to develop a robust proposal that includes a viable organizational plan and implementation strategy. We solicit comment on our phased approach to proposal submission dates and issuance of awards. The target timeframe for awards is intended to enable regional centers to begin supporting provider adoption in time for providers to receive incentive payments with respect to Fiscal Year (hospitals) or Calendar Year (physicians) 2011 and 2012, when potential Medicare incentives are greatest. D. Comments on Draft Description ONC requests comments on this draft description of the regional centers within the Extension Program. Please send comments to the address, for receipt by the due date, specified at the beginning of this notice. Dated: May 22, 2009. Charles P. Friedman, Deputy National Coordinator for Health Information Technology. [FR Doc. E9-12419 Filed 5-27-09; 8:45 am] BILLING CODE 4150-45-P
ENDNOTES: Comments from ASQ

A Suggests acknowledgement of the fact that there is an array of available health
information technology (EMR, Population/Patient Registr ies, e-Prescribe, portals, RHIO’s, etc.) and buy-in that the ideal state is for these technologies to be synergistical ly inter connected within and among points in the health care continuum.
B Needs to encompass not only the act of hands-on work with the devices but � how the technology is incorporated into the overall socia l-technical system
(STS) into which it is being placed � the degree of preparedness of the practice for automation: work-flow
optimization, etc. � proper attention to human factors engineering � making practice-status appropriate choices of technology that are supportive of
the goals and time-appropriate objectives of the practice: not “too much, too soon”
� the “state of the practice” should be assessed by a validated, standardized pre- technology assessment tool (such as that used by MPRO in MI)
� Where there are gaps in readiness of the practice for automation, the Extension Center should provide education, train ing, and in-practice assistance modeled after industry-proven process improvement tools and methodologies ( lean, value-stream mapping, 5S, DMAIC, FMEA, etc.) to ensure the complete readiness of the practice for whatever technology choices they make. MPRO in MI has the prototype for this.
C
Health information technology is only a tool to be used to achieve these goals. Alone it wil l not get us there. It is not the magic bullet. Of equal, if not greater, importance are establishing a culture of quality and process improvement at all levels; using proven tools to sustainably identify and el iminate waste, errors, redundancy and reduce costs in the infra-structure of healthcare; and establishing metrics for success and incentives not only for clinical performance of providers and practices, but also for operational performance. At present there are no such universally accepted operational metrics, guidelines or standards.
D The order of activit ies proposed herein needs to be adjusted.
1. The first task should be to assess the state of the practice or environment into which the technology is being introduced. How is i t currently functioning operationally, cl inical ly, f inancially, and customer-wise? Are there waste redundancy, error, customer dissatisfaction, sub-optimization of clin ical outcomes or f inancial performance, cul ture issues, etc., that suggest some pre-technology pre-engineering needs to be done prior to the introduction of technology? Do we want to instal l a Corvette engine into a go-cart? Human factors engineering and STS should also be addressed as part of this task.

2. The second task is to assess which technology(s) would best sui t the practice
at its stage of maturity and development, and how and when phasing in of technology should occur. Is it an EMR with all of the bells and whistles that should go in f irst? Or is it a s impler and less expensive all-patient, a ll-payer registry that is connected with a RHIO to track the practice's whole pat ient population allowing them to monitor for quality improvement purposes the status of all patients with chronic diseases whose condit ion(s) are not controlled or whose preventive care (e.g. Screening Mammogram) are overdue? Also to be considered in performing this task is the appropriate staging of the acquisit ion and deployment of technologies. “Too much too soon” is—tragically—not uncommon.
3. Upon completion of the first two tasks including the choice of certain technologies the work of interfacing with vendors, negotiating for price and value [don't forget interfaces!], training and start-up will begin. This is cri t ical ly important (as is the final coat of paint on a room) but can fall far short of expectations unless the pre-work is done and done right (much like the most important part of any painting job: prep work).
E That may be so, but as indicated above and by previous experience the greatest reason for HIT failure has not been poor choices of vendor/hardware (though they have contributed to many failures), but poor and/or incomplete preparation of the environment which has led to increased time constraints, customer dissatisfaction, dis-use, under-use, and mis-use of even the right technology for the practice.
F See Comment B
G See Comment B H Electronic health records should, at minimum, include population/pat ient registr ies
and EMRs. I See Comments B and D
J See Comments B and D
K Need to add pre-engineering and functionality selection to th is l is t
L Including the loan from industry of volunteer or “released time” process engineers through the ASQ Marshall Plan as well as sustainable services avai lable through retrained, laid-off process and quality engineers from industries affected by the downturned economy.
M Should read “active, continuous col lection, storage, cataloging and free and user-fr iendly written and onl ine disseminat ion of best practices and research on the implementation, effective use, upgrading…”

N Change to read “focused on patient-centered primary care”
O Should read “integration of health information technology, including electronic health records, as well as course material on process improvement, physician/practice culture change, waste reduction…”
P Change to read “focused on patient-centered primary care”
Q See Comment K
R Agree completely with the priority p laced on process flow. As indicated in other comments above, the minimum support level also should include a pre-technology assessment and attention to making proper functionality choices that are correctly sequenced. Also desirable would be at tention to the culture change and STS issues that are always part of the introduct ion of anything new, especially something as complicated as some of HIT can be.
S See Comment L above
T Add “and other stakeholders such as consumers.”
U Should add to the areas of required specialized expertise the following: “physician/practice culture change that values continuous quality improvement, quality management systems, process improvement, STS Thinking, human factors engineering, clinical and operational metrics for success.”
V Add #12: associations of qual ity and process improvement professionals (such as the American Society for Quality [ASQ]) with collect ive and individual expertise in work organization, STS, quality management, process improvement, culture change, change management, and related sciences.

June 26, 2009 Office of the National Coordinator for Health Information Technology 200 Independence Avenue, S.W. Suite 729D Washington DC 20201 Attn: HIT Policy Committee—Meaningful Use Comments Dear Sir/Madam: I am writing as president of the American Society for Quality (ASQ) in response to the request by the Office of the National Coordinator for Health Information Technology (ONC) for comments on the preliminary definition of “meaningful use,” as presented to the HIT Policy Committee on June 16, 2009. The Centers for Medicare & Medicaid Services (CMS) is authorized under the American Recovery and Reinvestment Act to provide a reimbursement incentive for physician and hospital providers who are successful in becoming “meaningful users” of an electronic health record (EHR). These incentive payments begin in 2011 and gradually phase down. Starting in 2015, providers are expected to have adopted and be actively utilizing an EHR in compliance with the “meaningful use” definition or they will be subject to financial penalties under Medicare. ASQ is a community of more than 90,000 quality experts in all sectors of the economy whose members are dedicated to the promotion and advancement of quality and process improvement tools, principles, and practices in their workplaces and in their communities. ASQ also administers the Malcolm Baldrige National Quality Program (MBNQP) under a contract with the National Institute of Standards and Technology (NIST). As America engages in a long overdue dissection, analysis, and restructuring of the ways in which we prevent disease, receive and finance healthcare, and manage and utilize health care technology, ASQ stands as a valued partner for those struggling to control runaway health care costs, deploy useful technologies, make health care safer, and improve accessibility to high quality, cost-efficient care. Put simply, and paraphrasing a well known advertising slogan, “We do not provide healthcare. We help those that do, do it better.” Nowhere is this slogan more applicable than in the evolving world of health IT (HIT). Healthcare is one of the last of this country’s major economic sectors to effectively and pervasively embrace and adopt the use of information technology. We believe that thanks to your efforts and the efforts of others healthcare is now on a fast track to embrace, deploy and spread effective and efficient use of health IT as quickly and completely as possible. We also believe that the definition of “meaningful use” will be a powerful tool in driving effective,

HIT Policy Committee—Meaningful Use Comments Page 2 of 5
successful use of these tools and in making them a permanent part of the healthcare armamentarium. Therefore, we at ASQ applaud your effort to define the concept of “meaningful use” of health IT. We are writing to offer some modest suggestions for enhancing the success of your effort to define this term. These suggestions center on a few key principles:
� While HIT and related technologies are potentially effective tools to be used in the quest for better, more cost-effective, and more accessible health care, they are not “magic bullets” and cannot and should not be expected, by themselves, to achieve those results.
� While it is critical to have explicit rules and measures that serve as minimum standards for the functionality and performance of health IT modalities in affecting the provision and efficacy of clinical services, one should not forget or de-emphasize the ability of these tools to monitor and assess the improvement of the non-clinical services provided in physicians’ offices and hospitals. This is especially important since much of the waste -- and thus, costs -- in healthcare is generated on the administrative side of care provision.
� “Meaningful use” of health IT begins and is affected by events that occur well before the actual purchase and “go-live” of these tools. How successfully the following questions are answered may affect “meaningful use” every bit as much as how well the software and hardware are configured and function:
o How well is the practice organized? o How smoothly does it operate? o Is it ready for health IT? o How prepared are the staff for using the tools and/or the change that such use
will entail? o How was the decision made as to which functionality is best for the practice?
The best health IT modalities will not work if the business environment into which they are placed is operating in an earlier century.
� Change is difficult, and nowhere more so than in medical practices that are overburdened with waste, paperwork, thinning profit margins, and inadequate time to provide care. The cultural issues in a practice or hospital can dramatically affect the successful implementation of health IT and should be addressed in defining “meaningful use.”1
� The proven and validated tools, philosophies, and methodologies of quality management, change management, and process improvement can be of immense help in the work of deploying health IT. If the term “meaningful use” suggested the use
1 Unintended Consequences of In formation Technologies in Health Ca re —An Inte ractive Sociotechnical Analysis, Michael I. Harrison, PhDa,
*, Ross Koppel, PhDb and Shirly Bar-Lev, PhDc,, Journal of the American Medical In fo rmatics Association 2007;14(5):542-549

HIT Policy Committee—Meaningful Use Comments Page 3 of 5
of such tools in preparing for, implementing, and monitoring the performance of the health IT modalities supported under the ARRA, the chances for successful, more cost-efficient implementations would be enhanced.
� Failure to address some of these operational infrastructure aspects of “meaningful use” could lead to the dis-use, mis-use, and under-use of health IT that has plagued the efforts to gain its acceptance in the clinical realm.
With these principles in mind, we offer the following suggestions relating to the definition of ”meaningful use”:
1. To be considered a “meaningful user” a practice or hospital must show evidence that the environment into which the technology will be placed is adequately prepared and ready to accept the sometimes considerable changes that result from the deployment:
a. Was (or has) the process flow in the practice been “optimized” and/or “leaned” using proven methods for achieving this such as those used in conjunction with the DOQ-IT Program in Michigan (http://www.mpro.org/prevention.htm), to take full advantage clinically and operationally of the installation? Doing otherwise may be likened to putting a Corvette engine in a go-cart.
b. There is a large pool of talented individuals with training and experience in process engineering and quality management who might be available to assist in this activity, perhaps in conjunction with the RHITECs which are also supported under the ARRA.
c. An additional resource might be the ASQ’s “New Marshall Plan” under which, after comprehensive training about the medical practice environment, ASQ volunteer process engineers, change agents, and quality managers can, using a standardized work plan, assist practices and their staffs in interested communities to analyze and improve practice process flows, eliminate waste, reduce costs, and seamlessly introduce new functionalities such as HIT, Patient Centered Care, patient safety, etc.
d. Since the adoption of new technology implies changes in behavior, have the office and/or hospital staff been fully acculturated to the introduction of the technology using proven methods for achieving this, and are they committed to its full use?
e. Was careful consideration given to the human factors engineering concerns introduced by deployment of the health IT?
2. To be considered to be in “meaningful use” the technology being supported should be judged to be the right tool(s) for the environment into which it is being placed:
a. Was careful and deliberate, informed thought given by the practice or hospital to the choice of health IT functionalities?
b. Was (were) the right tool(s) chosen? c. How was that determined? d. Who was available to assist the practice/hospital in making those choices? e. Is there a carefully thought out plan for orderly progression of functionality to
meet the objectives of the Act? f. Was careful consideration given to the feasibility of and costs associated with
effecting user-friendly interfaces between the new technology and the existing

HIT Policy Committee—Meaningful Use Comments Page 4 of 5
health IT related technologies in the practice/hospital (e.g. lab, radiology, referral sources, etc.) and in the community (i.e. RHIO)?
3. To be considered to be in “meaningful use” the technology must be effective not only clinically, but operationally in helping to reduce costly operational and administrative errors, waste, and redundancy:
a. Are there effective, valid, and accurate measures to determine the performance of the technology in operational areas as well as in the clinical areas?
b. Will those measures such as those in Appendix A below be considered alongside the clinical measures listed in the matrix when judging “meaningful use”?
4. To be considered in “meaningful use” there must be a defined, written, and properly executed plan in place in the practice/hospital receiving support for covered health IT for continuous and rigorous evaluation of its use, its performance (clinically and operationally), barriers to success, its costs and net value, etc.
As plans evolve for this important definition ASQ and its members would welcome the opportunity to advise you and your staff as to how some of our suggestions can be efficiently and effectively implemented. Should you have questions or wish to discuss any of these comments and suggestions from ASQ, please contact John Ryan of our headquarters staff--email [email protected] or telephone 800-248-1946 ext. 7244. Sincerely,
Roberto M. Saco President American Society for Quality Attachment—Appendix A: Draft Non-Clinical Metrics

HIT Policy Committee—Meaningful Use Comments Page 5 of 5
APPENDIX A Draft Non-Clinical Metrics
All should be reported with fiscal YTD average, last completed month, and an indication of trend or as a run chart
� Scheduled pat ients per phys ic ian per o Session o Hour
� Days to th ird avai lable of f ice v is i t o New pat ients o Establ ished pat ients
Prevent ive v is i t Management v is i t Procedure v is i t Other c lass of v is it
� Panel s ize (var ious methodologies) � Revenue per
o Encounter o wRVU
� wRVU per encounter � Effect ive convers ion factor ( revenue per tRVU) � Non-phys ic ican salary pract ice expense per
o Encounter o wRVU o Session o Day
� Non-phys ic ian salary margin ( revenue – expense) � Percent incent ive payment received

ASQ – 21st Century Health Caucus Seminar Preparing for Health IT: I t ’s No Slam Dunk!
2103 Rayburn House Office Build ing Tuesday, September 15, 2009
3:30–5:30 PM EDT
REFERENCES
1. “First, Lay Groundwork for IT Adoption,” Joseph Fortuna, August 18, 2009, modernhealthcare.com: http://www.modernhealthcare.com/article/20090818/REG/308189976
2. ASQ White Paper on Health Reform: http://www.asq.org/advocacy/issues-actions/20090806-quality-healthcare-reform.html?WT.mc_id=EM3680M&WT.dcsvid=1405223990
3. ASQ Comments on “Meaningful Use”: http://www.asq.org/advocacy/issues-actions/20090806-quality-healthcare-reform.html?WT.mc_id=EM3680M&WT.dcsvid=1405223990
4. ASQ Comments on RHITEC: http://www.asq.org/advocacy/issues-actions/20090806-quality-healthcare-reform.html?WT.mc_id=EM3680M&WT.dcsvid=1405223990
5. “Unintended Consequences of Information Technologies in Health Care—An Interactive Sociotechnical Analysis,” Michael I . Harrison, Ph.D., Ross Koppel, Ph.D., and Shir ly Bar-Lev, Ph.D., Journal of the American Medical Informatics Association, 2007, 14(5):542-549.
6. Physicians and Ambulatory Electronic Health Records, David W. Bates, HEALTH AFAIRS 2005, 2 4(5):1180-1189.
7. DOQ-IT University: http://www.mpro.org/pdf/DOQ%20IT%20U_July%202008.pdf 8. How to Map Your Office Process:
http://www.providersedge.com/ehdocs/ehr_presentations/Physician_Office_Quality_ Improvement-How_to_Map_Your_Office_Process.pdf
9. “Preparing for Implementing an Electronic Medical Record: Technology Alone Is Not the Answer,” Cynthia A. Ethier, Beacon Partners: http://www.beaconpartners.com/press_room/articles/preparingforimplement.htm
10. “Systems for Medical Practice in the 21st Century: EHRs, e-Prescribing and the Medical Home,” Maria E. Rudolph, MPH: http://www.acponline.org/about_acp/chapters/md/rudolph.ppt
11. “e-Health: Making Healthcare Better for European Citizens: An Action Plan for a European e-Health Area,” Commission of the European Communities: http://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=COM:2004:0356:FIN:EN:PDF
12. “Preparing for EHR Adoption,” Dr. Rob Lamberts: http://trusted.md/blog/dr_rob_lamberts/2006/04/17/preparing_for_emr_adoption
13. “Training Your Staff for EMR,” Peter Pollack: http://www.medicalpracticetrends.com/management/training-staff/
14. “You Can’t Just Flip a Switch,” Alice Loveys, MD and Leigh Burchell: http://www.allscriptscenter.com/NR/rdonlyres/FC8D0845-A576-4D16-A376-CD8BC7D34635/0/HowtoPrepareforEMRArticle.pdf
15. AHRQ-National Resource Center for HIT Web Conference, “Socio-Technical Aspects of Health IT,” March 28, 2007; http://healthit.ahrq.gov/images/mar07sociotechnicalwebconf/ socio_technical_aspects_of_health_it/socio_technical_files/textmostly/slide1.html
16. “Electronic Healthcare Records,” John M. Buell, Healthcare Executive, Sept./Oct. 2009, pp. 8-19.