Embed Size (px)
DESCRIPTION
Measuring Investment in Human Capital Formation: An Experimental Analysis of Early Life Outcomes Orla Doyle, Colm Harmon, James Heckman, Caitriona Logue, Seong Moon UCL, 25 th -26 th June 2012. Preparing for Life Programme. - PowerPoint PPT Presentation
Citation preview

+
Measuring Investment in Human Capital Formation: An Experimental Analysis of Early Life Outcomes
Orla Doyle, Colm Harmon, James Heckman, Caitriona Logue, Seong MoonUCL, 25th-26th June 2012

+ Preparing for Life Programme
One of the first experimental early childhood intervention in Ireland
Funded by Irish Government (DCYA) & The Atlantic Philanthropies
Community-led initiative operated by Northside Partnership in Dublin ~ 6,400 inhabitants 33% dependent on social welfare 60% live in social housing (>3 times national average) 47% lone mothers (29% national average) 16% unemployed (3 times national average) 66% early school leavers (38% national average) 5% third level education (29% national average)
Source: Census (2006)- CSO
Belief within the community that children were lagging behind their peers

+ Design of PFL
Aim: Improve levels of school readiness by assisting parents in developing skills to prepare their children for school
Bottom-up approach: community initiative involving 28 community groups, service providers, & local representatives
Theoretical Framework: Grounded in several psychological theories of development including the theory of human attachment, socio-ecological theory of development and social-learning theory
Evaluation: Randomised Control Trial design

+Design of Preparing for Life

+ PFL EvaluationImpact Evaluation Data collection: Pre-intervention (baseline), 3 mnts (WASI), 6mths,
12mths, 18mths, 24mths, 3yrs, 3.5yrs, 4yrs
Informant: Mother is the primary informant, but also fathers, child, other independent data sources (birth records)
Implementation Evaluation Aim: Delve into the blackbox of programme effectiveness & evaluate fidelity
to the PFL model
Data collection:1. Implementation data on the Database Management System 2. Focus groups with participants3. Semi-structured interviews with mentors/IO

+ Recruitment
Eligibility Criteria: Cohort of pregnant women residing in PFL catchment area between Jan
2008-August 2010 (32 months) Includes preparious and non-preparious women
Recruitment: Maternity hospital at first booking visit (b/w 12-26 weeks) Within the local community
Population-based recruitment rate, based on all live births during the recruitment phase, was 52%

+Computerized Randomisation Procedure
Unconditional probability randomisation strategy
After informed consent obtained, mother ask to press the key to allocate her assignment condition
Evaluation & Implementation team automatically received an email with the assigned PFL ID number and treatment condition
Preserves the integrity of the procedure as no opportunity for recruiter to intentionally influence assignment
115 allocated to High treatment group 118 allocated to Low treatment group

+ Baseline Data Collection
Conducted post randomisation, pre intervention Baseline data wave completed in August, 2010
123 measures: Demographics & SES, health behaviour & pregnancy, parenting, social support, psychological assessments (maternal well-bring, personality traits, self-esteem, self efficacy, attachment, time preferences)
Interviews conducted PFL High treatment group: 104 PFL Low treatment group: 101
Used to determine the effectiveness of the randomisation procedure

+ Methodology
Permutation based hypothesis testing (Heckman et al. 2010) Classical hypothesis tests unreliable when the sample size is small and the
data are not normally distributed Permutation test are distribution free, thus suitable in small samples Based on the assumption of exchangeability between treatment
conditions under the null hypothesis
Stepdown procedure (Romano & Wolf, 2005) Ignoring the multiplicity of tests may lead to the rejection of “too many”
null hypotheses Test multiple hypotheses simultaneously by controlling overall error rates
for vectors of hypotheses using the family-wise error rate (FWER) as a criterion
Less conservative & more powerful than other methods as takes account of statistical dependencies between tests

+ Summary of Permutation Tests Examining Differences at Baseline
Proportion of Measures Not Significantly Different at Baseline
Topic PFL Low – PFL High
Family Socio-demographics 33/33 (0%)
Maternal Well-being 24/24 (0%)
Maternal Health & Pregnancy 35/35 (0%)
Parenting & Childcare 10/13 (74%)
Social Support 17/18 (94%)
Total NOT Statistically Different 119/123 (97%)
Randomisation worked!

+ Permutation Tests Comparing Baseline Differences in Selected Family Socio-Demographics
Low Treatment – High Treatment
InstrumentN
(nLOW/ nHIGH)
MLOW
(SD)MHIGH
(SD)p Effect Size
(d)
Mother’s Age 205(101/104)
25.30(5.99)
25.46(5.85)
ns .03
First-time Mothers 205(101/104)
0.50(0.50)
0.54(0.50)
ns .09
Mother Married 205(101/104)
0.18(0.38)
0.14(0.35)
ns .09
Mothers with Junior Certificate Qualification or Lower
205(101/104)
0.40(0.49)
0.34(0.47)
ns .12
Mothers with Primary Degree 205(101/104)
0.03(0.17)
0.03(0.17)
ns .01
Mothers Unemployed 205(101/104)
0.41(0.49)
0.43(0.50)
ns .05
Annual Income of Working Mothers (in Euros)
75(38/37)
19,602(8,093)
19,224(9,851)
ns .04
Fathers Unemployed 198(97/101)
0.31(0.46)
0.43(0.50)
ns .24
Residing in Social Housing 204(101/103)
0.55(0.50)
0.55(0.50)
ns .00
In Possession of a Medical Card 205(101/104)
0.66(0.47)
0.60(0.49)
ns .14

+ Analysis of 6 Month Outcome Data
Test for treatment effects across 8 main domains including 160 measures Child development Child health Parenting Home environment Maternal health Social support Childcare & service use Household factors & SES
25 Step-down categories defined
258 interviews conducted PFL High treatment group: 84 PFL Low treatment group: 90
12

+ Attrition & Disengagement up to 6 months
Official dropout between baseline - 6 months: High treatment – 13% Low Treatment – 6%
Disengagement between baseline - 6 months : High treatment – 9% Low Treatment – 10%
Baseline Characteristics Associated with Attrition
VariablesHigh Treatment
Group Low Treatment
Group p p
Weeks in preg. at programme entry 0.651 0.563
Mother's age 0.505 0.063
Partnered 0.410 0.503
Married 0.541 0.699
Living with parent(s) 0.477 0.556
First time mother 0.629 0.073
Low education 0.121 0.131
Mother employed 0.010** 0.772
Saves regularly 0.337 0.545
Social housing 0.639 0.759
Cognitive Resources (WASI) at 3MO 0.570 0.097
Physical Health Condition 1.000 0.511
Mental Health Condition 0.760 0.197
Smoking during pregnancy 1.000 0.367
Drinking during pregnancy 0.439 0.308
Drug ever used 0.159 0.675
Vulnerable attachment (VASQ) 0.324 0.622
Positive parenting attitudes (AAPI) 0.565 0.757
Self efficacy (Pearlin) 0.263 0.389
Self esteem (Rosenberg) 0.096 0.717
Knowledge of infant development 0.731 0.003**

+
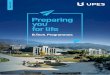
ASQ Scores & Difficult Temperament
N(nHIGH/ nLOW)
MHIGH
(SD)MLOW
(SD)Individual
Test p1
Step Down Testp2
Effect Sized
ASQ Gross Motor Score 173(83/90)
40.78(11.93)
38.50(12.99)
ns ns 0.18
ASQ Communication Score 173(83/90)
53.07(7.84)
51.78(8.49)
ns ns 0.16
*Difficult Temperament 173(83/90)
11.70(5.71)
12.21(5.50)
ns ns 0.09
ASQ Personal Social Score 172(82/90)
46.52(12.09)
45.94(13.57)
ns ns 0.05
*ASQ Social-Emotional 173(83/90)
14.76(10.68)
15.17(13.75)
ns ns 0.03
ASQ Fine Motor Score 173(83/90)
50.84(9.46)
51.39(10.17)
ns ns 0.06
ASQ Problem Solving 173(83/90)
51.87(9.39)
52.56(9.92)
ns ns 0.07
Notes: 1 one-tailed (right-sided) p value from an individual permutation test with 1000 replications. 2 one-tailed (right-sided) p value from a Step Down permutation test with 1000 replications. * indicates the variable was reverse coded for the testing procedure. ‘ns’ indicates the variable is not statistically significant.
RESULTS FOR HIGH & LOW TREATMENT GROUPS: CHILD DEVELOPMENT

+ Summary of Six Month Results
Proportion of Measures Significantly Different at Six Months
Domain PFL Low – PFL High Step Down categories
Child Development 0% (0/13) 0/2
Child Health 10% (3/30) 0/3
Parenting 23% (5/22) 1/5 (PSI)
Home Environment & Safety 36% (8/22) 1/2 (HOME)
Maternal Health 5% (1/20) 1/4 (Health)
Social Support 38% (5/13) 0/2
Childcare & Service Use 7% (1/14) 0/2
Household Factors & SES 0% (0/26) 0/5
Total Statistically Different 14% (23/160) 3/25 categories

+ Summary of 6 month results
Majority of the results for High V’s Low are in hypothesized direction
A few significant differences identified (14%)
In line with other home visiting programmes

+ Additional Analysis
Interaction & Subgroup analysis Gender, lone parents v partnered parents, first time v non first time
parents, high versus low IQ mothers, high v low family risk
Programme appears to benefit high IQ mothers, families with multiple children & families with multiple risks
Analysis of engagement (treatment intensity) On average, high treatment group received 14 home visits of ~1 hr in
duration= total treatment = 14 hours
Higher maternal IQ & vulnerable attachment style & joined programme earlier associated with higher engagement, while smoking during pregnancy associated with lower engagement

+Contamination in RCTs
Contamination occurs when the control groups either actively or passively receive the intervention intended for the treatment group (Cook & Campbell, 1979)
Potential for contamination is high in PFL Members of the treatment and control groups may be friends, neighbours,
colleagues, same family!
Community comparison group used to safeguard against contamination
Included a range of direct (‘blue-dye’) in each survey

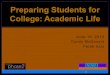
+ Contamination in PFL
Heard the phrase MHIGH
(SD)MLOW
(SD)MLFP
(SD)Low – High
pHigh –
Comparisonp
Low – Comparison
p
Mutual Gaze0.59(0.49)
0.08(0.27)
0.04(0.19) <0.01 <0.01 ns
Circle of Security0.49(0.50)
0.12(0.33)
0.05(0.21) <0.01 <0.01 ns
If contamination DID NOT take place: • High & Low treatment group will differ in their responses • Low treatment group will not differ from comparison group• High treatment group will differ from the comparison group
Contamination Questions in 6 month PFL survey
Little evidence of contamination among treatment groups Evidence of absorption of PFL knowledge among high treatment group

+ Update on PFL
Oldest PFL child is almost 4 years and old & youngest is 13 months
18, 24, & 36 month surveys are currently in the field
12 month results available during Summer
Over 1,500 interviews conducted as part of impact evaluation
Conducted four school readiness surveys with junior infant cohorts in 2008, 2009, 2010, 2011
Conducted focus groups with low & high treatment groups & semi-structured interviews with all PFL mentors
Evaluation will continue until all children start school
Programme website: www.preparingforlife.com
Evaluation website: http://geary.ucd.ie/preparingforlife/