Embed Size (px)
Citation preview

J
O
Ph
HYYHHTT
a
ARRAA
KHWJ
I
dtpa
dT
h0
ARTICLE IN PRESSG ModelJCC-874; No. of Pages 6
Journal of Cardiology xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Journal of Cardiology
jo ur nal home page: www.elsev ier .com/ locate / j j cc
riginal article
resentations and outcomes of patients with acute decompensatedeart failure admitted in the winter season
idehiro Kaneko (MD, PhD) ∗, Shinya Suzuki (MD), Masato Goto (MD), Takuto Arita (MD),asufumi Yuzawa (MD), Naoharu Yagi (MD), Nobuhiro Murata (MD), Junji Yajima (MD),uji Oikawa (MD), Koichi Sagara (MD), Takayuki Otsuka (MD), Shunsuke Matsuno (MD),iroto Kano (MD), Tokuhisa Uejima (MD), Kazuyuki Nagashima (MD),ajime Kirigaya (MD), Hitoshi Sawada (MD, FJCC), Tadanori Aizawa (MD, FJCC),akeshi Yamashita (MD, FJCC)
he Cardiovascular Institute, Tokyo, Japan
r t i c l e i n f o
rticle history:eceived 17 December 2013eceived in revised form 23 February 2014ccepted 18 March 2014vailable online xxx
eywords:eart failureinter
apanese
a b s t r a c t
Background: Seasonal variations in cardiovascular disease is well recognized. However, little is knownabout the presentations and outcomes of Japanese heart failure (HF) patients in the winter season.Methods and results: We used a single hospital-based cohort from the Shinken Database 2004–2012,comprising all new patients (n = 19,994) who visited the Cardiovascular Institute Hospital. A total of 375patients who were admitted owing to acute decompensated HF were included in the analysis. Of thesepatients, 136 (36%) were admitted in winter. Winter was defined as the period between December andFebruary. The HF patients admitted in winter were older, and had a higher prevalence of hypertensionand diabetes mellitus than the patients admitted in other seasons. Patients with conditions categorizedas clinical scenario 1 tended to be admitted more commonly in winter. HF with preserved left ventricularejection fraction (LVEF) was more common in HF patients admitted in winter than in those admitted inother seasons. Beta-blocker use at hospital discharge was more common in the patients admitted in otherseasons. Kaplan–Meier curves and log-rank test results indicated that the incidences of all-cause death,cardiovascular death, and HF admission were comparable between the patients admitted in winter and
those admitted in other seasons.Conclusions: HF admission was frequently observed in the winter season and HF patients admitted in thewinter season were older, and had higher prevalence of hypertension and diabetes mellitus, and pre-served LVEF suggesting that we might need to pay more attention for elderly patients with hypertension,diabetes mellitus, and HF with preserved LVEF to decrease HF admissions in the winter season.© 2014 Japanese College of Cardiology. Published by Elsevier Ltd. All rights reserved.
ntroduction
The seasonal variation in the incidence of various cardiovasculariseases is well established [1–4]. The environmental tempera-
Please cite this article in press as: Kaneko H, et al. Presentations andadmitted in the winter season. J Cardiol (2014), http://dx.doi.org/10.1
ure is associated with this variability, as cardiovascular eventseak in winter. The physiologic consequences of a cold climatere thought to result in increased coronary risk factors and might
∗ Corresponding author at: The Department of Cardiovascular Medicine, The Car-iovascular Institute, 3-2-19, Nishiazabu, Minato-ku, Tokyo 106-0031, Japan.el.: +81 3 3408 2151; fax: +81 3 3408 2159.
E-mail addresses: [email protected], [email protected] (H. Kaneko).
ttp://dx.doi.org/10.1016/j.jjcc.2014.03.004914-5087/© 2014 Japanese College of Cardiology. Published by Elsevier Ltd. All rights re
also cause clinical deterioration in patients with heart failure (HF).Skin cooling has been shown to increase systemic vascular resis-tance [5], heart rate [6], plasma norepinephrine concentration [7],circulating levels of vasoconstrictor peptides [8], and blood pres-sure (BP) [9]. In keeping with these changes, BP is higher in winter[10]. Cold can also induce myocardial ischemia [11]. All of theseeffects could clearly lead to worsening of HF. However, little isknown about the clinical characteristics and outcomes of JapaneseHF patients admitted in winter. In the present study, we aimed to
outcomes of patients with acute decompensated heart failure016/j.jjcc.2014.03.004
elucidate the characteristics and clinical outcomes of patients withacute decompensated HF admitted in winter by examining datafrom our hospital-based cohort selected from the Shinken Database2004–2012.
served.

ING ModelJ
2 f Card
M
S
CawhlohpJiweawaaeld
E
t
D
cdlmdcdeotaAme
ARTICLEJCC-874; No. of Pages 6
H. Kaneko et al. / Journal o
ethods
tudy patients
The Shinken Database includes all patients who visited theardiovascular Institute in Tokyo, Japan (“Shinken” is a Japanesebbreviation for the name of the hospital), and excludes patientsho are foreign travelers and those with active cancer. Thisospital-based database was established to investigate the preva-
ence and prognosis of cardiovascular diseases in the urban areasf Japan [12,13]. The registry began in June 2004, and patientsave been continually registered to the database annually. Theresent study analyzed data from this database collected between
une 2004 and March 2013 (Shinken Database 2004–2012) andncluded 19,994 new visiting patients. Among them, 537 patients
ere admitted to our institute due to acute decompensated HF. Wexcluded HF patients with primary valvular heart disease (n = 138)nd acute coronary syndrome (n = 24). Valvular heart diseaseas defined as long-standing mitral or aortic valve involvement,
s documented by physical examination and echocardiography,ngiography, or history of surgical repair. Finally, 375 patients werexamined in the present study (Fig. 1). These patients were fol-owed up for an average period of 857 ± 846 days. Winter wasefined as the period between December and February.
thics
The ethical committee of the Cardiovascular Institute approvedhis study, and all the patients provided written informed consent.
ata collection
For each patient, after undergoing electrocardiography andhest radiography, cardiovascular status was evaluated by echocar-iography, an exercise test, 24-h Holter recordings, and blood
aboratory data, as prescribed by the attending physician, within 3onths after the first visit. As initial clinical parameters, collected
ata included gender, age, body mass index, drug information, andoexisting conditions, including hypertension, atrial fibrillation,iabetes mellitus, and dyslipidemia. In most patients, additionalchocardiographic parameters included left ventricular diameterf the diastole (LVDd), LV diameter of the systole (LVDs), interven-ricular septum thickness (IVST), posterior wall thickness (PWT),
Please cite this article in press as: Kaneko H, et al. Presentations andadmitted in the winter season. J Cardiol (2014), http://dx.doi.org/10.1
nd LV ejection fraction (LVEF) using M-mode echocardiography.nemia was defined as a hemoglobin level of <11 g/dL. An esti-ated glomerular filtration rate (eGFR) was calculated using the
GFR equation for the Japanese population: eGFR = 194 × (serum
The Shinken Database 2004-2012(n=19,994)
Acute Decompensated Heart Failure Admission(n=537)
Examined in the Present Study(n=375)
Primary Val vular Di sease(n=138)
Acute Coronary Syndrome(n=24)
Fig. 1. Patient flow chart of the present study.
PRESSiology xxx (2014) xxx–xxx
creatinine)−1.094 × (age)−0.287 × (0.739, if the patient is female)[14]. A baseline eGFR < 60 mL min−1 1.73 m−2 was used to definechronic kidney disease (CKD) [15]. Idiopathic dilated cardiomy-opathy was diagnosed by the presence of global LV dilatationwith impaired systolic function occurring in the absence of knowncardiac causes. Hypertrophic cardiomyopathy was diagnosed byechocardiography when hypertrophy (IVST or PWT > 12 mm) with-out hypertension was present. We defined HFpEF patients as HFpatients with preserved LVEF (i.e. LVEF > 50%), and HFrEF patientsas HF patients with reduced LVEF (i.e. LVEF ≤ 50%), as previouslydescribed [16,17]. Patients were divided into three groups by clin-ical scenario (CS): CS1, systolic BP (SBP) at admission >140 mmHg;CS2, ≥100 mmHg; CS3, <100 mmHg [18]. We confirmed the deathsof study patients by the medical records of our hospital or by theinformation obtained during follow-up. We defined cardiovasculardeath as death resulting from acute myocardial infarction, suddencardiac death, death due to heart failure, death due to stroke, ordeath due to other cardiovascular causes [19]. We confirmed HFevents (HF requiring hospitalization or death due to HF) that wereclassified as per the International Classification of Diseases, 10threvision, code I50, using the medical records of our hospital or bythe information obtained from follow-up.
Patient follow-up
The health status, incidence of cardiovascular events and mor-tality of patients are maintained in the database by linking thesedata to the medical records of the hospital and through study doc-uments that were sent one a year to those who stopped hospitalvisits or who were referred to other hospitals.
We excluded the follow-up data obtained after April 1, 2013from data analysis. Therefore, the end of the follow-up period wasdefined as one of the following: (1) the date of death, if the datewas before March 31, 2013; (2) the final hospital visit or the finalresponse to our study documents involving prognosis with confir-mation of being alive before March 31, 2013; (3) March 31, 2013,when the date of death, the final hospital visit, or the final responseto our study documents involving prognosis was later than April 1,2013.
Statistical analysis
Categorical and consecutive data regarding patient backgroundare presented as numbers (%) and means ± standard deviation,respectively. The chi-square test was used for comparisonsbetween groups, and the unpaired t-test was used for compari-son of consecutive variables. Long-term, event-free survival wasestimated using Kaplan–Meier curves and the log-rank test toassess the significance of differences between the two groups.Logistic regression analysis was used to identify the determinantsof HF patients in the winter season. Univariate and age-adjustedCox regression analysis were performed to clarify the associationbetween HF admission in the winter season and long-term clinicaloutcomes. A probability value of <0.05 was considered to indi-cate a statistically significant difference. Statistical analyses wereperformed using SPSS (SPSS Inc., Chicago, IL, USA), version 19.0software.
Results
Patient characteristics
outcomes of patients with acute decompensated heart failure016/j.jjcc.2014.03.004
Among the 375 patients with HF, 136 (36%) were admit-ted in winter, and 239 patients (64%) were admitted in theother seasons. The distribution of the admission month among

ARTICLE IN PRESSG ModelJJCC-874; No. of Pages 6
H. Kaneko et al. / Journal of Cardiology xxx (2014) xxx–xxx 3
0
10
20
30
40
50
60
Mon
Num
ber
of p
atie
nts
nth a
ttodovTdhbapiaaTa
U
vps(h(
M
avcsa
D
i
the HF patients admitted in winter, and in 10% (0.8%) of thoseadmitted in the other seasons. Cardiovascular death occurred in6.6% of the patients in winter, and 7.5% of patients in the otherseasons. Readmission for HF occurred in 25% of the patients
Table 1Characteristics of patients.
Other seasons(n = 239)
Winter season(n = 136)
p-Value
Age (years) 67 ± 14 70 ± 13 0.034Male 72% 68% 0.412BMI (kg/m2) 24 ± 4.6 25 ± 4.3 0.295Hypertension 54% 65% 0.025Dyslipidemia 28% 37% 0.079Diabetes mellitus 24% 35% 0.023Hyperuricemia 23% 24% 0.909Cigarette smoking 39% 43% 0.397CKD 13% 16% 0.460Anemia 21% 18% 0.390ICM 30% 28% 0.655DCM 23% 16% 0.099HCM 2.5% 4.4% 0.315HHD 4.6% 8.8% 0.101AF 36% 40% 0.474WBC (/�L) 7570 ± 2925 7857 ± 3408 0.394CRP (mg/dL) 1.7 ± 3.4 1.9 ± 4.2 0.578BNP (pg/mL) 874 ± 902 859 ± 874 0.877
CSI 29% 39% 0.051II 63% 55% 0.111III 7% 6% 0.705
Fig. 2. Distribution of mo
he study patients is shown in Fig. 2. The HF patients admit-ed in the winter season were older than those admitted in thether seasons (70 ± 13 years vs. 67 ± 14 years, p = 0.034). Gen-er difference was not seen between the two groups. Patientsf winter season had a higher prevalence of hypertension (65%s. 54%, p = 0.025) and diabetes mellitus (35% vs. 24%, p = 0.023).he prevalence rates of ischemic cardiomyopathy, dilated car-iomyopathy, hypertrophic cardiomyopathy, and hypertensiveeart disease were comparable between the two groups. Whitelood cell counts (7570 ± 2925 �L vs. 7857 ± 3408 �L, p = 0.394)nd C-reactive protein levels (1.7 ± 3.4 mg/dL vs. 1.9 ± 4.2 mg/dL,
= 0.578) at admission were comparable between the patientsn winter and other seasons. B-type natriuretic peptide levels atdmission were also comparable between the patients in winternd other seasons (859 ± 874 pg/mL vs. 874 ± 902 pg/mL, p = 0.877).he condition classified as CS1 tended to be more common in winterdmission group (39% vs. 29%, p = 0.051) (Table 1).
ltrasound cardiography
Ultrasound echocardiography revealed that LVDd (53 ± 10 mms. 56 ± 11 mm, p = 0.014), and LVDs (41 ± 14 mm vs. 45 ± 14 mm,
= 0.013) were smaller in HF patients in winter than those in othereasons. LVEF was greater in HF patients in the winter season47 ± 21% vs. 39 ± 20%, p = 0.001). The prevalence of HFpEF wasigher in HF patients in the winter season (46% vs. 30%, p = 0.002)Table 2).
edication at hospital discharge
The use of beta-blockers was more common in the HF patientsdmitted in the other seasons than in those admitted in winter (71%s. 60%, p = 0.032). The use of other cardiovascular drugs includingalcium channel blockers, rennin-angiotensin-system inhibitors,tatins, loop diuretics, aldosterone antagonists, digitalis, nitrate,nd amiodarone was comparable between the two groups (Table 3).
Please cite this article in press as: Kaneko H, et al. Presentations andadmitted in the winter season. J Cardiol (2014), http://dx.doi.org/10.1
eterminants of heart failure in winter
Multivariate logistic regression analysis (step-wise model)ncluding following covariates age ≥75 years, hypertension,
th
mong the study patients.
diabetes mellitus, and HFpEF demonstrated that diabetes mellitus[odds ratio (OR) 1.698, 95% confidence interval (CI) 1.064–2.708,p = 0.026] and HFpEF (OR 1.969, 95% CI 1.264–3.067, p = 0.003) wereindependent determinants of HF admission in winter (Table 4).
Clinical outcomes
All-cause death (in-hospital death) occurred in 9.6% (1.5%) of
outcomes of patients with acute decompensated heart failure016/j.jjcc.2014.03.004
BMI, body mass index; CKD, chronic kidney disease; ICM, ischemic cardiomyopa-thy; DCM, idiopathic dilated cardiomyopathy; HCM, hypertrophic cardiomyopathy;HHD, hypertensive heart disease; AF, atrial fibrillation; WBC, white blood cell count;CRP, C-reactive protein level; BNP, brain natriuretic peptide; CS, clinical scenario.Data are expressed as mean ± standard deviation, or percentage.
ARTICLE ING ModelJJCC-874; No. of Pages 6
4 H. Kaneko et al. / Journal of Card
Table 2Ultrasound cardiography findings.
Other seasons(n = 239)
Winter season(n = 136)
p-Value
IVST (mm) 9.8 ± 4.6 10.1 ± 2.7 0.533PWT (mm) 9.0 ± 1.9 9.2 ± 2.0 0.258LVDd (mm) 56 ± 11 53 ± 10 0.014LVDs (mm) 45 ± 14 41 ± 14 0.013LVEF (%) 39 ± 20 47 ± 21 0.001
HFpEF 30% 46% 0.002HFrEF 70% 55% 0.002
LAD (mm) 44 ± 9.5 44 ± 9.2 0.480
IVST, interventricular septum thickness; PWT, posterior wall thickness; LVDd, leftventricular end-diastolic dimension; LVDs, left ventricular end-systolic dimension;LVEF, left ventricular ejection fraction; HFpEF, heart failure with preserved left ven-tricular ejection fraction; HFrEF, heart failure with reduced left ventricular ejectionfraction; LAD, left atrial dimension. Data are expressed as mean ± standard devia-tion.
Table 3Medication at hospital discharge.
Other seasons(n = 237)
Winter season(n = 134)
p-Value
Beta-blockers 71 60 0.032CCBs 30 36 0.212RAS-Is 75 72 0.566Statins 30 32 0.608Loop diuretics 77 81 0.306Aldosterone antagonist 47 38 0.102Digitalis 16 15 0.778Nitrate 12 7 0.115Amiodarone 7.6 4.5 0.241
CCB, calcium-channel blocker; RAS-I, renin-angiotensin system inhibitor. Data areexpressed as percentages.
Table 4Determinants of winter heart failure.
OR 95% CI p-Value
Diabetes mellitus 1.698 1.064–2.708 0.026HFpEF 1.969 1.264–3.067 0.003
Logistic regression analysis for heart failure admission in winter. OR, odds ratio;Cf
a(td(aCt90(fw
TC
D
I, confidence interval; HFpEF, heart failure with preserved left ventricular ejectionraction.
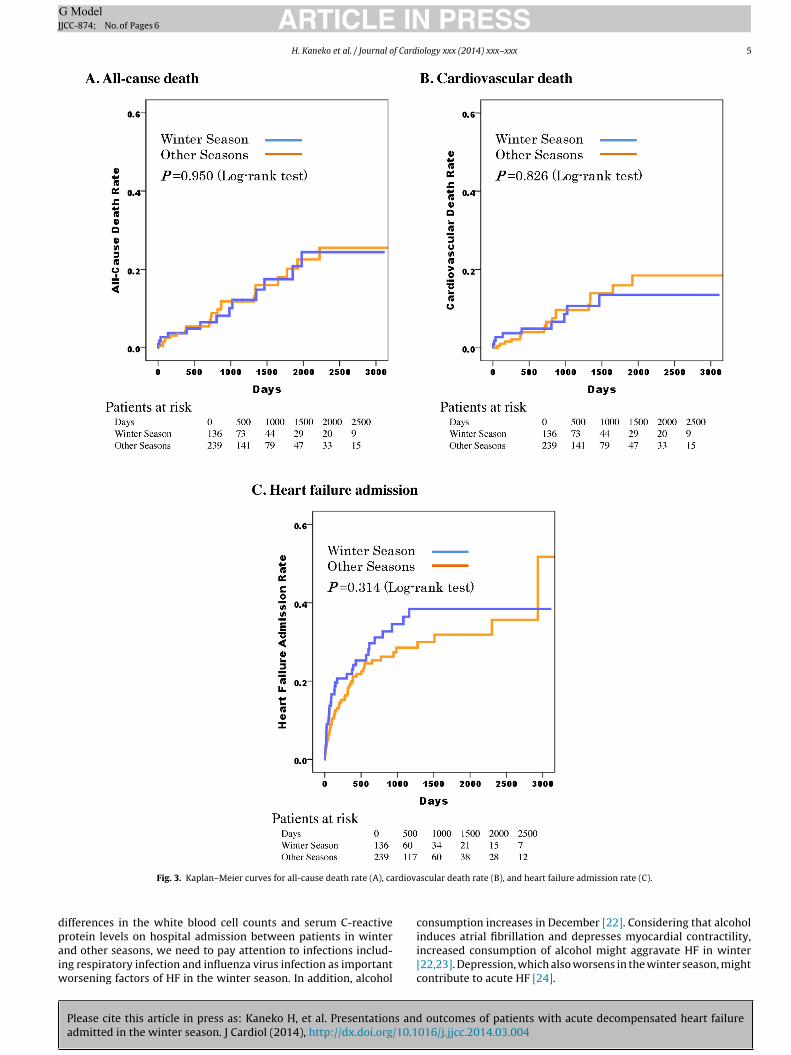
dmitted in winter and 22% of the patients in the other seasonsTable 5). Kaplan–Meier curves and log-rank test showed thathe incidences of all-cause death (Fig. 3A, log-rank p = 0.950), car-iovascular death (Fig. 3B, log-rank p = 0.826), and HF admissionFig. 3C, log-rank p = 0.314) of the patients admitted in winternd the other seasons. Similar to Kaplan–Meier curves, unadjustedox regression analysis demonstrated that HF admission in win-er was not significantly associated with all-cause death (HR 0.979,5% CI 0.498–1.923, p = 0.950), cardiovascular disease death (HR.914, 95% CI 0.411–2.036, p = 0.826), and heart failure admission
Please cite this article in press as: Kaneko H, et al. Presentations andadmitted in the winter season. J Cardiol (2014), http://dx.doi.org/10.1
HR 1.247, 95% CI 0.810–1.919, p = 0.315). Even after adjustmentor age, HF admission in winter was not significantly associatedith all-cause death (HR 0.923, 95% CI 0.470–1.815, p = 0.817),
able 5linical outcomes.
Other seasons(n = 239)
Winter season(n = 136)
p-Value
All-cause death 10 9.6 0.880In-hospital death 0.8 1.5 0.566Cardiovascular death 7.5 6.6 0.742Heart failure admission 22 25 0.533
ata are expressed as percentages.
PRESSiology xxx (2014) xxx–xxx
cardiovascular death (HR 0.860, 95% CI 0.386–1.916, p = 0.712), andHF admission (HR 1.216, 95% CI 0.790–1.871, p = 0.375) (Supple-mentary Table 1).
Discussion
The present study reports the data from an observational cohortof HF patients that was analyzed to determine the characteris-tics and outcomes of acute decompensated HF patients who wereadmitted in winter. The major findings of the present study wereas follows:
(1) Admission for HF occurred frequently in winter (136/375, 36%).(2) The HF patients admitted in the winter season were older than
those admitted in the other seasons. The prevalence of hyper-tension and diabetes mellitus was greater in the patients in thewinter season. The CS1 classification tended to be more com-mon and LVEF was higher in the patients admitted in winterthan in those admitted in other seasons.
(3) Kaplan–Meier curves and log-rank test results showed the inci-dences of all-cause death (log-rank p = 0.950), cardiovasculardeath (log-rank p = 0.826), and hospital admission for HF (log-rank p = 0.314) in the patients admitted in winter and otherseasons.
In the present study, HF admission was commonly observed inwinter (36%) when compared with the other seasons, which was inagreement with a previous study [20]. HF patients admitted in thewinter season were older than those admitted in the other seasons.Furthermore, patients in the winter season more frequently hadhypertension and diabetes mellitus compared with those admit-ted in the other seasons. Interestingly, HF patients in winter had ahigher prevalence of HFpEF than HF patients in the other seasons.As older age, hypertension, and diabetes mellitus are well-knownclinical features of HF with preserved LVEF [17], our results suggestthat HFpEF is an important clinical presentation of HF patients inthe winter season.
Despite these differences in patient characteristics, clinicaloutcomes including in-hospital mortality, long-term mortality,long-term cardiovascular mortality, and occurrences of re-admission for HF were comparable between the HF patientsadmitted in winter and the other seasons. Since HF patients inwinter were older than those admitted in the other seasons, weperformed an age-adjusted Cox regression analysis. Even afteradjustment for age, HF admission in winter was not significantlyassociated with long-term outcomes. Because the HF patientsadmitted in winter had diabetes mellitus more frequently, wemight expect these patients to have worse clinical outcomes thanthose admitted in the other seasons. On the other hand, the patientsadmitted in winter were more likely to have a CS1 condition, whichwas thought to be associated with clinical outcomes more favorablethan other CS categories.
The results of the present study are in keeping with the sea-sonal variation observed in other cardiovascular diseases such asacute coronary syndrome and sudden death [1,4]. Consequently,these cardiovascular diseases might share common mechanismsthat exacerbate the amplitude of the seasonal variation of othercardiovascular syndromes. For example, the hemodynamic stressesand neurohumoral activation that accompany lower temperaturesmight exacerbate HF, induce myocardial ischemia, and precipitatearrhythmias [6–11]. Furthermore, both ischemia and arrhyth-
outcomes of patients with acute decompensated heart failure016/j.jjcc.2014.03.004
mias could worsen HF. Other mechanisms could also underliethe seasonal variation in HF. For example, respiratory infection,especially those related to influenza, are more frequent in winterand could precipitate HF [21]. Although there were no significant
ARTICLE IN PRESSG ModelJJCC-874; No. of Pages 6
H. Kaneko et al. / Journal of Cardiology xxx (2014) xxx–xxx 5
rdiova
dpaiw
Fig. 3. Kaplan–Meier curves for all-cause death rate (A), ca
ifferences in the white blood cell counts and serum C-reactive
Please cite this article in press as: Kaneko H, et al. Presentations andadmitted in the winter season. J Cardiol (2014), http://dx.doi.org/10.1
rotein levels on hospital admission between patients in winternd other seasons, we need to pay attention to infections includ-ng respiratory infection and influenza virus infection as important
orsening factors of HF in the winter season. In addition, alcohol
scular death rate (B), and heart failure admission rate (C).
consumption increases in December [22]. Considering that alcohol
outcomes of patients with acute decompensated heart failure016/j.jjcc.2014.03.004
induces atrial fibrillation and depresses myocardial contractility,increased consumption of alcohol might aggravate HF in winter[22,23]. Depression, which also worsens in the winter season, mightcontribute to acute HF [24].
ING ModelJ
6 f Card
C
mHihps
S
stmstastt
C
HpLps
A
f(d
A
t
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
ARTICLEJCC-874; No. of Pages 6
H. Kaneko et al. / Journal o
linical implications
The results of the present study have clinical significance andight affect HF management. Considering that almost 40% of theF admissions in this study occurred in winter, increased vigilance
n winter is warranted in clinical practice. Moreover based on theigher prevalence of older age, hypertension, and CS1 in the HFatients seen in winter, BP control should be closely monitored inuch patients, especially among the elderly.
tudy limitations
The present study had several limitations. Our hospital is aingle-department cardiovascular facility; therefore, the results ofhis study cannot be generalized to all medical centers. Further-
ore, the sample size of the present study was limited, and thus, thetatistical power might not be strong enough for any negative datao be conclusive. As described above, the inflammatory markers ondmission were comparable between HF patients in the winter sea-on and in the other seasons. However, further studies are neededo clarify the association between infection and HF admission inhe winter season.
onclusions
HF admission was frequently observed in the winter season andF patients admitted in the winter season were older, had higherrevalence of hypertension and diabetes mellitus, and preservedVEF. Therefore, we might need to pay more attention to elderlyatients with hypertension, diabetes mellitus, and HF with pre-erved LVEF to decrease HF admissions in the winter season.
cknowledgments
We thank Shiro Ueda and Nobuko Ueda of Medical Edge Co Ltd,or assembling the database by Clinical Study Supporting SystemCliSSS), and Ineko Hayakawa, Hiroaki Arai, and Hiroshi Aoki forata management and system administration.
ppendix A. Supplementary data
Supplementary data associated with this article can be found, inhe online version, at http://dx.doi.org/10.1016/j.jjcc.2014.03.004.
eferences
[1] Marchant B, Ranjadayalan K, Stevenson R, Wilkinson P, Timmis AD. Circadianand seasonal factors in the pathogenesis of acute myocardial infarction: theinfluence of environmental temperature. Br Heart J 1993;69:385–7.
[2] Ornato JP, Peberdy MA, Chandra NC, Bush DE. Seasonal pattern of acute myocar-dial infarction in the National Registry of Myocardial Infarction. J Am CollCardiol 1996;28:1684–8.
[3] Spencer FA, Goldberg RJ, Becker RC, Gore JM. Seasonal distribution of acute
Please cite this article in press as: Kaneko H, et al. Presentations andadmitted in the winter season. J Cardiol (2014), http://dx.doi.org/10.1
myocardial infarction in the second National Registry of Myocardial Infarction.J Am Coll Cardiol 1998;31:1226–33.
[4] Arntz HR, Willich SN, Schreiber C, Bruggemann T, Stern R, Schultheiss HP. Diur-nal, weekly and seasonal variation of sudden death. Population-based analysisof 24,061 consecutive cases. Eur Heart J 2000;21:315–20.
[
PRESSiology xxx (2014) xxx–xxx
[5] Keatinge WR, McIlroy MB, Goldfien A. Cardiovascular responses to ice-coldshowers. J Appl Physiol 1964;19:1145–50.
[6] Hayward JM, Holmes WF, Gooden BA. Cardiovascular responses in man to astream of cold air. Cardiovasc Res 1976;10:691–6.
[7] Westheim A, Os I, Thaulow E, Kjeldsen SE, Eritsland J, Eide IK. Haemodynamicand neurohumoral effects of cold pressor test in severe heart failure. ClinPhysiol 1992;12:95–106.
[8] Rodriguez-Garcia JL, Paule A, Dominguez J, Garcia-Escribano JR, Vazquez M.Effects of the angiotensin II antagonist losartan on endothelin-1 and norepi-nephrine plasma levels during cold pressor test in patients with chronic heartfailure. Int J Cardiol 1999;70:293–301.
[9] Raven PB, Wilkerson JE, Horvath SM, Bolduan NW. Thermal, metabolic, and car-diovascular responses to various degrees of cold stress. Can J Physiol Pharmacol1975;53:293–8.
10] Minami J, Kawano Y, Ishimitsu T, Yoshimi H, Takishita S. Seasonal variationsin office, home and 24 h ambulatory blood pressure in patients with essentialhypertension. J Hypertens 1996;14:1421–5.
11] Lassvik CT, Areskog NH. Angina in cold environment. Reactions to exercise.Br Heart J 1979;42:396–401.
12] Suzuki S, Yamashita T, Ohtsuka T, Sagara K, Uejima T, Oikawa Y, Yajima J, KoikeA, Nagashima K, Kirigaya H, Ogasawara K, Sawada H, Aizawa T. Prevalence andprognosis of patients with atrial fibrillation in Japan: a prospective cohort ofShinken Database 2004. Circ J 2008;72:914–20.
13] Kaneko H, Koike A, Senoo K, Tanaka S, Suzuki S, Nagayama O, Sagara K,Otsuka T, Matsuno S, Funada R, Uejima T, Oikawa Y, Yajima J, Nagashima K,Kirigaya H, et al. Role of cardiopulmonary dysfunction and left atrial remod-eling in development of acute decompensated heart failure in chronic heartfailure with preserved left ventricular ejection fraction. J Cardiol 2012;59:359–65.
14] Matsuo S, Imai E, Horio M, Yasuda Y, Tomita K, Nitta K, Yamagata K, TominoY, Yokoyama H, Hishida A. Revised equations for estimated GFR from serumcreatinine in Japan. Am J Kidney Dis 2009;53:982–92.
15] Tonelli M, Jose P, Curhan G, Sacks F, Braunwald E, Pfeffer M. Proteinuria,impaired kidney function, and adverse outcomes in people with coronarydisease: analysis of a previously conducted randomised trial. BMJ 2006;332:1426.
16] Goda A, Yamashita T, Suzuki S, Ohtsuka T, Uejima T, Oikawa Y, Yajima J, KoikeA, Nagashima K, Kirigaya H, Sagara K, Ogasawara K, Isobe M, Sawada H, AizawaT. Heart failure with preserved versus reduced left ventricular systolic func-tion: a prospective cohort of Shinken Database 2004–2005. J Cardiol 2010;55:108–16.
17] Kaneko H, Suzuki S, Yajima J, Oikawa Y, Sagara K, Otsuka T, Matsuno S, KanoH, Uejima T, Koike A, Nagashima K, Kirigaya H, Sawada H, Aizawa T, YamashitaT. Clinical characteristics and long-term clinical outcomes of Japanese heartfailure patients with preserved versus reduced left ventricular ejection frac-tion: a prospective cohort of Shinken Database 2004–2011. J Cardiol 2013;62:102–9.
18] Mebazaa A, Gheorghiade M, Pina IL, Harjola VP, Hollenberg SM, Follath F,Rhodes A, Plaisance P, Roland E, Nieminen M, Komajda M, Parkhomenko A,Masip J, Zannad F, Filippatos G. Practical recommendations for prehospital andearly in-hospital management of patients presenting with acute heart failuresyndromes. Crit Care Med 2008;36:S129–39.
19] Kaneko H, Yajima J, Oikawa Y, Tanaka S, Fukamachi D, Suzuki S, Sagara K, OtsukaT, Matsuno S, Funada R, Kano H, Uejima T, Koike A, Nagashima K, Kirigaya H,et al. Impact of aging on the clinical outcomes of Japanese patients with coro-nary artery disease after percutaneous coronary intervention. Heart Vessels2013;29:156–64.
20] Stewart S, McIntyre K, Capewell S, McMurray JJ. Heart failure in a cold climate.Seasonal variation in heart failure-related morbidity and mortality. J Am CollCardiol 2002;39:760–6.
21] Fleming DM. The contribution of influenza to combined acute respiratory infec-tions, hospital admissions, and deaths in winter. Commun Dis Public Health2000;3:32–8.
22] Kupari M, Koskinen P. Seasonal variation in occurrence of acute atrial fibril-lation and relation to air temperature and sale of alcohol. Am J Cardiol1990;66:1519–20.
23] Conway N. Haemodynamic effects of ethyl alcohol in patients with coronary
outcomes of patients with acute decompensated heart failure016/j.jjcc.2014.03.004
heart disease. Br Heart J 1968;30:638–44.24] Jiang W, Alexander J, Christopher E, Kuchibhatla M, Gaulden LH, Cuffe MS,
Blazing MA, Davenport C, Califf RM, Krishnan RR, O’Connor CM. Relationship ofdepression to increased risk of mortality and rehospitalization in patients withcongestive heart failure. Arch Intern Med 2001;161:1849–56.





























