Embed Size (px)
Citation preview
Presented by Sally MoonClinical Nurse Specialist
Recovering the Paediatric patient

SESSION OVERVIEW -
• How do Children differ from Adults
• Principles of Post Anaesthetic Nursing Care
• Complications in Recovery
• Recovery discharge criteria
• Practical tips and ideas

HOW ARE CHILDREN DIFFERENT ?
RESPIRATORY SYSTEMSmaller airways
Narrow nasal passages
Large tongue
Larger prominent occiput / short neck
Larynx high & anterior ( level c2-c3)
Cricoid ring narrowest point
Compliant rib cage
CARDIOVASCULAR SYSTEM
Metabolic rate
Cardiac Output
Heart Rate / Oxygen consumption
Fixed stroke volume
Smaller circulating volume
Glucose requirement
TEMPERATURE REGULATION
Surface area per kg
Children lose heat more rapidly
Metabolic rate
Insufficient body fat
Infants cannot shiver

RENAL SYSTEM
Decreased capacity to excrete free water
Neonatal kidney GFR
sodium excretion / concentrating ability
POST ANAESTHETIC CAREConscious state
Oxygen saturations
Heart rate
Respiratory rate
Temperature
Blood pressure
Wound site / iv site
Pain score
COMPLICATIONS IN RECOVERY
Airway obstruction
PONV
Pain
Hypothermia
Hypovolaemia
Emergence Delirium

RESPIRATORY ASSESSMENT
Patency of Airway
Rate / depth respirations
Symmetry of Chest Expansion
Gag protective reflexes
Colour
Presence stridor /wheeze
Oxygen Saturation

SIGNS & SYMPTOMS AIRWAY OBSTRUCTION
Inspiratory stridor
Snoring
Increased work of breathing
Absent /silent respirations
Head bopping
CAUSES…..
MAINTAINING AIRWAY PATENCY
Backward head tilt
Chin lift
Jaw support
Suction airway secretions
Positioning
Oral / nasal airway
Bag & mask

LARYNGOSPASMDefined by forceful closure of vocal
cords which prevents respirationMore common in childrenMore common if URTIMore common if laryngeal stimulationManaged by positive airway
ventilation/100% oxygenRemove stimulusDrugs
PONV
Distressing for paediatric patients
More common after 2 of years age
Prophylactic anti-emetics regularly used
Additional therapy prescribed “just in case”
More common in children who suffer motion sickness
Squint surgery / ENT
PONV -
Metoclopramide
Dexamethasone
Granisetron
Droperidol
Promethazine
Post-operative Nausea & Vomiting guideline available on RCH website/Anaesthesia & Pain Management
PAIN MANAGEMENTPain is subjective and can be
influenced by many factors
AnxietyPrevious experiencePeri operative educationAnaesthetic & pain relief givenChilds age

PAIN
Appropriate pain tools for assessment
Wong-Baker / Flacc
Premedication
Local anaesthetic
Regional block /Epidural
Opioid infusions / pca
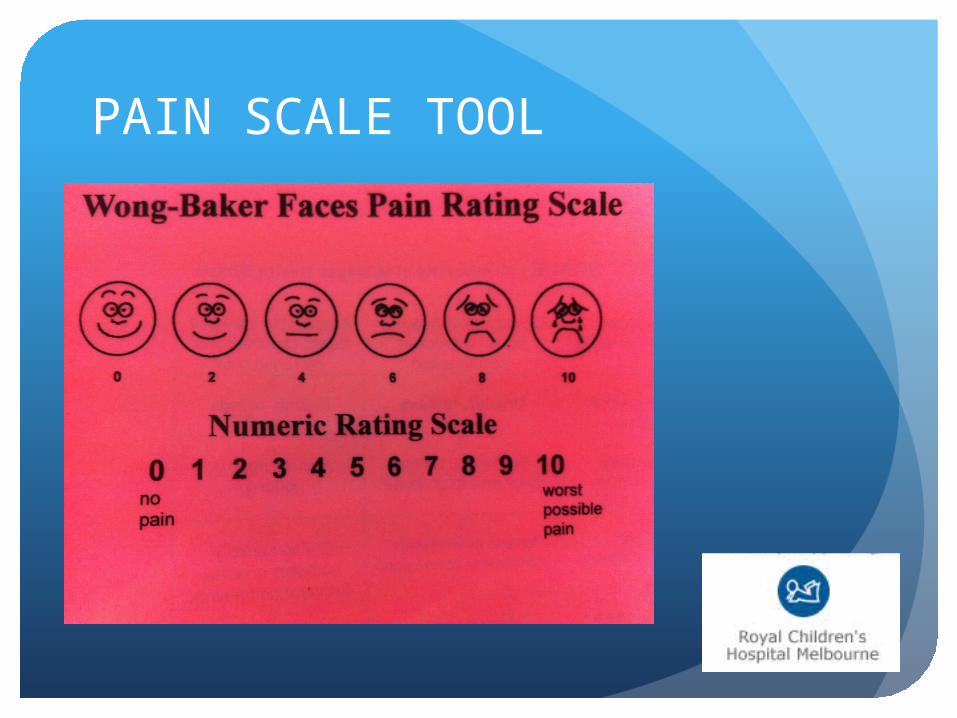
PAIN SCALE TOOL
PAIN

HYPOTHERMIA
Children more susceptible
Greater surface area
Can result in delayed awakening, cardiac irritability & respiratory depression
Neonates ,cerebral palsy, extensive surgery at greatest risk
HYPOTHERMIACAUSES –
Intraoperative exposure
Deliberate cooling (Neuro/Cardiac)
Poor thermoregulatory systems (Neonates)
TREATMENT –
Active warming ( Blanket /Bair hugger)
Warm fluids
Constant monitoring

HYPOVOLAEMIAPre op factors
Intra op fluid management
WATCH FOR
Obvious bleeding, wound / drain
Tachycardia (SMALLER CIRCULATING VOLUME)
Hypotension
CRT prolonged
EMERGENCE DELIRIUMState in which the child is
agitated,inconsolable,typically thrashing
Children do not recognise people /familiar objects
Greater incidence in children (1-5 years)
Safety
Carers
PSYCHOSOCIAL Waking up in Recovery can be
frightening
Separation anxiety
Re-orientate / Reassure
Use child’s name
Reunite family as soon as safe to do so
RECOVERY DISCHARGE CRITERIA
Sedation score 2 or less ( UMSS )
Pain under controlNo active vomitingVital sign assessments within
MET Criteria
RECOVERY DISCHARGE CRITERIA
If vital sign assessments are outside MET Criteria then MET discharge Criteria form completed
Oxygen order completed if necessary
Surgeon has spoken to parents

TIPS & TRICKS !!!






Questions