Embed Size (px)
Citation preview
Prevalence of Asthma Symptoms in Latin America: TheInternational Study of Asthma and Allergies in
Childhood (ISAAC)
Javier Mallol, MD,1* Dirceu Sole , MD,2 Innes Asher, MD,3 Tadd Clayton, MSc,3 Renato Stein, MD,4and Manuel Soto-Quiroz, MD,5 on behalf of the Latin American ISAAC Collaborators Group
Summary. The prevalence of respiratory symptoms indicative of asthma in children from LatinAmerica has been largely ignored. As part of the International Study of Asthma and Allergies inChildhood (ISAAC), 17 centers in 9 different Latin American countries participated in the study,and data from 52,549 written questionnaires (WQ) in children aged 13–14 years and from36,264 WQ in 6–7 year olds are described here.
In children aged 13–14 years, the prevalence of asthma ever ranged from 5.5–28%, and theprevalence of wheezing in the last 12 months from 6.6–27%. In children aged 6–7 years, theprevalence of asthma ever ranged from 4.1–26.9%, and the prevalence of wheezing in the last12 months ranged from 8.6–32.1%. The lower prevalence in centers with higher levels ofatmospheric pollution suggests that chronic inhalation of polluted air in children does not con-tribute to asthma. Furthermore, the high figures for asthma in a region with a high level ofgastrointestinal parasite infestation, and a high burden of acute respiratory infections occurringearly in life, suggest that these factors, considered as protective in other regions, do not have thesame effect in this region.
The present study indicates that the prevalence of asthma and related symptoms in LatinAmerica is as high and variable as described in industrialized or developed regions of the world.Pediatr Pulmonol. 2000; 30:439–444. © 2000 Wiley-Liss, Inc.
Key words: asthma; children; epidemiology; Latin America; ISAAC; prevalence.
INTRODUCTION
Although there is a large body of information regard-ing the prevalence of asthma and other allergic diseases,most of that information comes from studies undertakenin developed countries. Those studies suggest that theprevalence of asthma in children is increasing in indus-trialized regions and also that there is wide variability inprevalence between populations.1,2
5Teaching Unit, National Hospital for Children, San Jose´, Costa Rica.
Latin American ISAAC Collaborators Group: Isabelle Romieu (Cuer-navaca, Mexico), Manuel Soto Quiroz (Costa Rica), Gherson Kukier(David, Panama); Murillo Brito, Otelo Ferreira (Recife, Brazil); LedaSolano da Couta (Salvador, Brazil); Pascual Chiarella (Lima, Peru);Francisco Caldeira (Bello Horizonte, Brazil); Dirceu Sole´, CharlesNaspitz (Sa˜o Paulo, Brazil); Nelson Rosario (Curitiba, Brazil); RenatoStein, Marcus Jones (Porto Alegre, Brazil); Jaime Guggiari (Asuncio´n,Paraguay); Dolores Holgado (Montevideo, Uruguay); Natalio Salmun,Marcelo Cohen (Buenos Aires, Argentina); Hugo Neffen, TeresitaSolıs, Cristina Cerqueiro (Rosario, Santa Fe, Argentina); Javier Mal-lol, Eliana Cortez (Santiago Sur, Chile); Ignacio Sa´nchez (SantiagoCentro, Chile); Mario Calvo (Valdivia, Chile); and Lidia Amarales(Punta Arenas, Chile).
*Correspondence to: Dr. Javier Mallol, Department of Pediatric Re-spiratory Medicine, University of Santiago de Chile, Clasificador 23,Correo 9, Santiago, Chile. E-mail: [email protected]
Received 26 June 2000; Accepted 26 July 2000.
1Department of Pediatric Respiratory Medicine, University of San-tiago de Chile, Santiago, Chile.
2Division of Allergy, Federal University of Sa˜o Paulo, Sa˜o Paulo,Brazil.
3Department of Paediatrics, University of Auckland, Auckland, NewZealand.
4Pediatric Pulmonary Unit, Catholic University, Porto Alegre, Brazil.
Pediatric Pulmonology 30:439–444 (2000)
Original Articles
© 2000 Wiley-Liss, Inc.

The prevalence of asthma in children from LatinAmerica, and from other developing regions of theworld, has been relatively overlooked. This is probablybecause of the much higher impact of acute respiratoryinfections (ARIs) on children’s respiratory health, whichrepresent the most important cause of morbidity (andmortality in infancy) due to respiratory diseases in theseregions.3 The only published information on prevalenceof asthma in Latin America reported on results of studiescarried out almost two decades ago, when the prevalenceof asthma in the countries of the region ranged from0.4–4.2%.4 However, those studies differed in the em-ployed definitions and methodology, so that comparisonson variability in symptoms and figures of prevalence arenot feasible. Recently, in a comparative study of theprevalence of respiratory symptoms related to asthma inschoolchildren from Australia, Switzerland, and Chile, itwas found that prevalence of asthma in the last 12months in Chile was as high as in Australia, being 26%,21%, and 17% for children aged 6, 12, and 16 years,respectively.5 Using a different methodology, Soto-Quiroz et al.6 found the prevalence of asthma in childrenfrom Costa Rica (Central America) to be 23.4%.
This study is part of the International Study of Asthmaand Allergies in Childhood (ISAAC) Phase I; it employsthe same validated and standardized methodology for allparticipating centers throughout the world.7 ISAACPhase I has provided an excellent opportunity to deter-mine and compare the prevalence of asthma and otherallergic conditions in different populations of the world,and particularly in developing regions where little or noinformation is available. Here we report a descriptiveanalysis of the prevalence of respiratory symptoms re-lated to asthma obtained by written questionnaires in52,549 children aged 13–14 years, and in 36,264 children6–7 years old. Data were provided by 17 centers from 9Latin American countries.
METHODS
ISAAC uses simple methods that can be employed ina standardized way at minimal cost, in as wide a range ofcenters and countries as possible and based on schoolpopulations to ensure high response rates. It was decidedthat Phase I studies would not involve sophisticated, in-vasive, or expensive tests. The methodology of ISAAChas been described elsewhere.7 The study is based on
random samples of two age groups: 13–14 years (self-completion of questionnaires) and optionally 6–7 years(parental completion of questionnaires). In both agegroups, simple one-page written core questionnaires areused for assessing symptoms of asthma, rhinitis, and ec-zema. A video asthma questionnaire has also been rec-ommended for use in 13–14 year olds.
A sample size of 3,000 per age group was recom-mended in order to provide sufficient precision for esti-mates of symptom severity, but smaller sample sizes(minimum of 1,000) were permitted for prevalence com-parisons among participant centers.
The core ISAAC questionnaires were translated fromEnglish into Spanish and Portuguese, the two languagesspoken by the surveyed populations, and were validatedbefore starting their distribution to the selected samples.Thus, some important words, such as wheezing, wereadapted to the local terminology to ensure the best com-prehension possible.
Symptom prevalence in each center was calculated bydividing the number of positive responses to each ques-tion by the number of completed questionnaires. Eachcollaborating center was responsible for completing aregistration document, as well as obtaining the necessaryEthics Committee approval prior to the start of the study.Detailed description of collaborating centers and regis-tration, sampling frame, selection of subjects, Phase Icore questionnaire modules, data management and analy-sis, quality control measures, and other methodologicalissues have been described elsewhere.7 Logistic regres-sion was used to model the relationship between the de-pendent variables (prevalence of symptoms of asthma)and the participating centers. The results of this analysisare expressed as the odds ratio (OR) for each symptomand for each center (with 95% confidence intervals; CIs)relative to a reference center (Cuernavaca, Mexico).
This paper is based on the 12-month period prevalence(current prevalence) of the core symptoms of asthma for6–7 and 13–14 year olds provided by centers from theLatin American region. The data were processed andaccepted by the ISAAC International Data Centre inAuckland up to December 1997.
RESULTS
Most of the participating centers provided data for 6–7year olds, and all provided data for 13–14 year olds.Thus, this study reports data from 52,549 written ques-tionnaires (WQ) for children aged 13–14 years, and from36,264 WQ completed by parents for children aged 6–7years.
The response rate varied among the different centers,and averaged 88% for 6–7 year olds and 95% for the13–14 year olds. For some centers the response rate forchildren aged 13–14 years was close to 100%, as they
Abbreviations
ARI Acute respiratory infectionCI Confidence intervalISAAC International Study of Asthma and Allergies in
ChildhoodWQ Written questionnaire
440 Mallol et al.
were interviewed at their classroom, and those who werenot present at that time were surveyed during the nextfew days. In general, very few children refused to answerthe questionnaires.
There were significant differences in thecurrentprevalenceof respiratory symptoms indicative of asthmabetween countries in the region and also between centersin the same country, with up to fourfold variation in theprevalence ofcurrent wheezingin both age groups. Therewas a trend for asthma prevalence to be lower in centerslocated at the extremes of latitudes (Cuernavaca, Mexicoand Punta Arenas, Chile) with higher rates at tropicallatitudes; however, this finding was not always consis-tent. No significant difference for asthma symptoms wasfound between boys and girls; thus the data from boysand girls have been pooled for subsequent analyses.
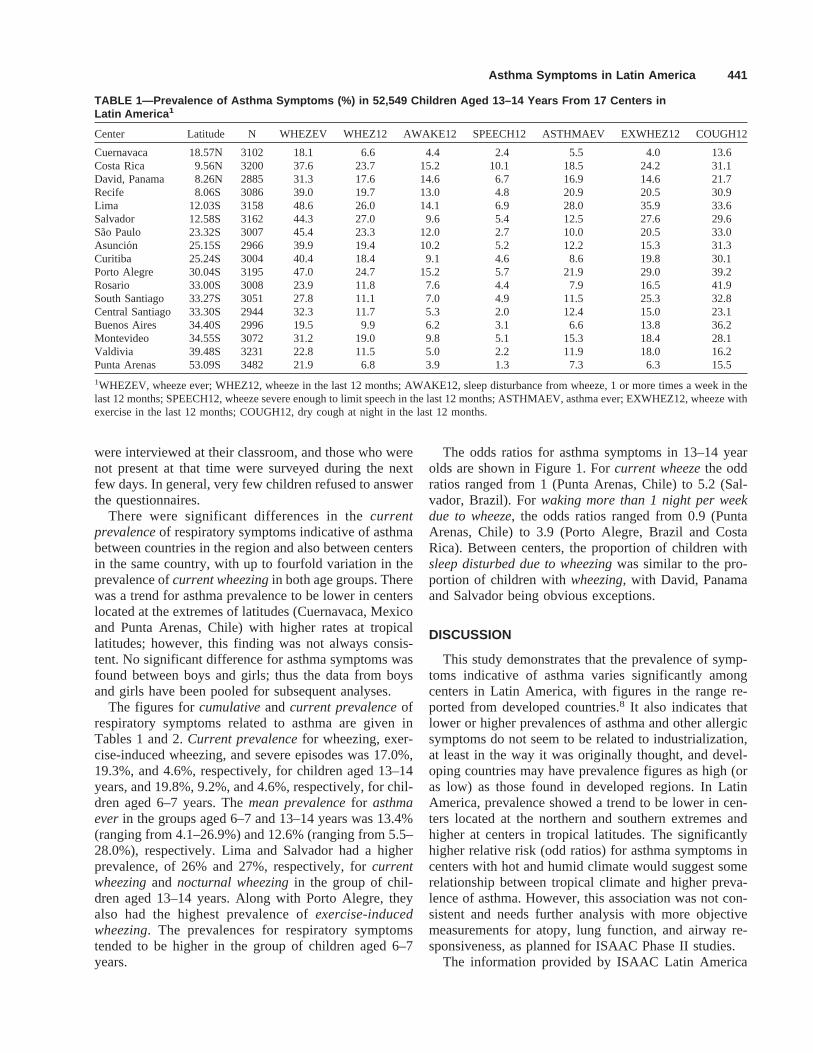
The figures forcumulativeandcurrent prevalenceofrespiratory symptoms related to asthma are given inTables 1 and 2.Current prevalencefor wheezing, exer-cise-induced wheezing, and severe episodes was 17.0%,19.3%, and 4.6%, respectively, for children aged 13–14years, and 19.8%, 9.2%, and 4.6%, respectively, for chil-dren aged 6–7 years. Themean prevalencefor asthmaeverin the groups aged 6–7 and 13–14 years was 13.4%(ranging from 4.1–26.9%) and 12.6% (ranging from 5.5–28.0%), respectively. Lima and Salvador had a higherprevalence, of 26% and 27%, respectively, forcurrentwheezingand nocturnal wheezingin the group of chil-dren aged 13–14 years. Along with Porto Alegre, theyalso had the highest prevalence ofexercise-inducedwheezing. The prevalences for respiratory symptomstended to be higher in the group of children aged 6–7years.
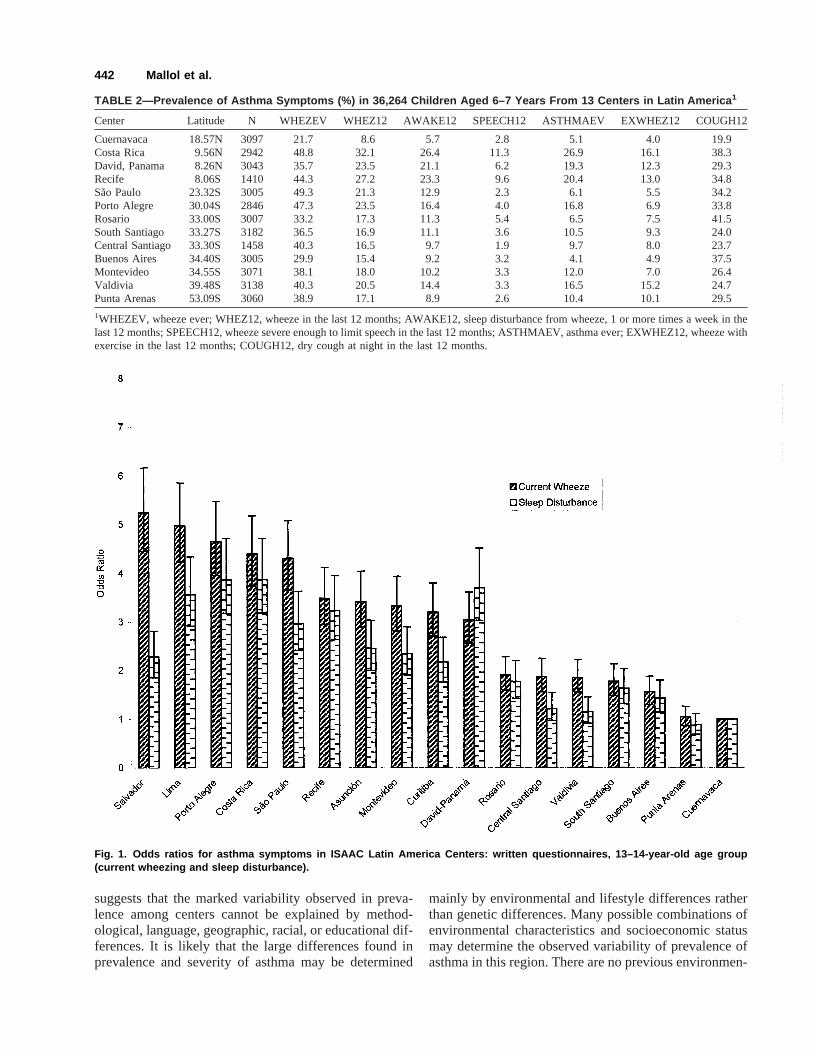
The odds ratios for asthma symptoms in 13–14 yearolds are shown in Figure 1. Forcurrent wheezethe oddratios ranged from 1 (Punta Arenas, Chile) to 5.2 (Sal-vador, Brazil). Forwaking more than 1 night per weekdue to wheeze, the odds ratios ranged from 0.9 (PuntaArenas, Chile) to 3.9 (Porto Alegre, Brazil and CostaRica). Between centers, the proportion of children withsleep disturbed due to wheezingwas similar to the pro-portion of children withwheezing,with David, Panamaand Salvador being obvious exceptions.
DISCUSSION
This study demonstrates that the prevalence of symp-toms indicative of asthma varies significantly amongcenters in Latin America, with figures in the range re-ported from developed countries.8 It also indicates thatlower or higher prevalences of asthma and other allergicsymptoms do not seem to be related to industrialization,at least in the way it was originally thought, and devel-oping countries may have prevalence figures as high (oras low) as those found in developed regions. In LatinAmerica, prevalence showed a trend to be lower in cen-ters located at the northern and southern extremes andhigher at centers in tropical latitudes. The significantlyhigher relative risk (odd ratios) for asthma symptoms incenters with hot and humid climate would suggest somerelationship between tropical climate and higher preva-lence of asthma. However, this association was not con-sistent and needs further analysis with more objectivemeasurements for atopy, lung function, and airway re-sponsiveness, as planned for ISAAC Phase II studies.
The information provided by ISAAC Latin America
TABLE 1—Prevalence of Asthma Symptoms (%) in 52,549 Children Aged 13–14 Years From 17 Centers inLatin America 1
Center Latitude N WHEZEV WHEZ12 AWAKE12 SPEECH12 ASTHMAEV EXWHEZ12 COUGH12
Cuernavaca 18.57N 3102 18.1 6.6 4.4 2.4 5.5 4.0 13.6Costa Rica 9.56N 3200 37.6 23.7 15.2 10.1 18.5 24.2 31.1David, Panama 8.26N 2885 31.3 17.6 14.6 6.7 16.9 14.6 21.7Recife 8.06S 3086 39.0 19.7 13.0 4.8 20.9 20.5 30.9Lima 12.03S 3158 48.6 26.0 14.1 6.9 28.0 35.9 33.6Salvador 12.58S 3162 44.3 27.0 9.6 5.4 12.5 27.6 29.6Sao Paulo 23.32S 3007 45.4 23.3 12.0 2.7 10.0 20.5 33.0Asuncion 25.15S 2966 39.9 19.4 10.2 5.2 12.2 15.3 31.3Curitiba 25.24S 3004 40.4 18.4 9.1 4.6 8.6 19.8 30.1Porto Alegre 30.04S 3195 47.0 24.7 15.2 5.7 21.9 29.0 39.2Rosario 33.00S 3008 23.9 11.8 7.6 4.4 7.9 16.5 41.9South Santiago 33.27S 3051 27.8 11.1 7.0 4.9 11.5 25.3 32.8Central Santiago 33.30S 2944 32.3 11.7 5.3 2.0 12.4 15.0 23.1Buenos Aires 34.40S 2996 19.5 9.9 6.2 3.1 6.6 13.8 36.2Montevideo 34.55S 3072 31.2 19.0 9.8 5.1 15.3 18.4 28.1Valdivia 39.48S 3231 22.8 11.5 5.0 2.2 11.9 18.0 16.2Punta Arenas 53.09S 3482 21.9 6.8 3.9 1.3 7.3 6.3 15.5
1WHEZEV, wheeze ever; WHEZ12, wheeze in the last 12 months; AWAKE12, sleep disturbance from wheeze, 1 or more times a week in thelast 12 months; SPEECH12, wheeze severe enough to limit speech in the last 12 months; ASTHMAEV, asthma ever; EXWHEZ12, wheeze withexercise in the last 12 months; COUGH12, dry cough at night in the last 12 months.
Asthma Symptoms in Latin America 441
suggests that the marked variability observed in preva-lence among centers cannot be explained by method-ological, language, geographic, racial, or educational dif-ferences. It is likely that the large differences found inprevalence and severity of asthma may be determined
mainly by environmental and lifestyle differences ratherthan genetic differences. Many possible combinations ofenvironmental characteristics and socioeconomic statusmay determine the observed variability of prevalence ofasthma in this region. There are no previous environmen-
TABLE 2—Prevalence of Asthma Symptoms (%) in 36,264 Children Aged 6–7 Years From 13 Centers in Latin America 1
Center Latitude N WHEZEV WHEZ12 AWAKE12 SPEECH12 ASTHMAEV EXWHEZ12 COUGH12
Cuernavaca 18.57N 3097 21.7 8.6 5.7 2.8 5.1 4.0 19.9Costa Rica 9.56N 2942 48.8 32.1 26.4 11.3 26.9 16.1 38.3David, Panama 8.26N 3043 35.7 23.5 21.1 6.2 19.3 12.3 29.3Recife 8.06S 1410 44.3 27.2 23.3 9.6 20.4 13.0 34.8Sao Paulo 23.32S 3005 49.3 21.3 12.9 2.3 6.1 5.5 34.2Porto Alegre 30.04S 2846 47.3 23.5 16.4 4.0 16.8 6.9 33.8Rosario 33.00S 3007 33.2 17.3 11.3 5.4 6.5 7.5 41.5South Santiago 33.27S 3182 36.5 16.9 11.1 3.6 10.5 9.3 24.0Central Santiago 33.30S 1458 40.3 16.5 9.7 1.9 9.7 8.0 23.7Buenos Aires 34.40S 3005 29.9 15.4 9.2 3.2 4.1 4.9 37.5Montevideo 34.55S 3071 38.1 18.0 10.2 3.3 12.0 7.0 26.4Valdivia 39.48S 3138 40.3 20.5 14.4 3.3 16.5 15.2 24.7Punta Arenas 53.09S 3060 38.9 17.1 8.9 2.6 10.4 10.1 29.5
1WHEZEV, wheeze ever; WHEZ12, wheeze in the last 12 months; AWAKE12, sleep disturbance from wheeze, 1 or more times a week in thelast 12 months; SPEECH12, wheeze severe enough to limit speech in the last 12 months; ASTHMAEV, asthma ever; EXWHEZ12, wheeze withexercise in the last 12 months; COUGH12, dry cough at night in the last 12 months.
Fig. 1. Odds ratios for asthma symptoms in ISAAC Latin America Centers: written questionnaires, 13–14-year-old age group(current wheezing and sleep disturbance).
442 Mallol et al.

tal studies that allow for comparisons with ISAAC re-sults within this region. However, studies9,10 have sug-gested that there are regional risk factors for thedevelopment of asthma and rhinitis in Western Europe.Similarly, other standardized studies in children in otherregions5,11–14have found significant regional differencesin the prevalence of respiratory symptoms.
The prevalence of asthma symptoms tended to behigher in poorer areas, suggesting that socioeconomicstatus is a major risk factor for the high prevalence ofasthma in Latin America. Latin American countries havemarked differences in economical, cultural, and environ-mental conditions, between them and also within theirpopulations. This could contribute to the observed vari-ability in the prevalence of asthma symptoms. A lowerprevalence of asthma had been observed in Hispanicsliving in USA compared with those who lived in theirnative countries,15 supporting the influence of socioeco-nomic status and its associated environmental risk fac-tors.
The marked differences in the prevalence of asthmabetween populations who share a similar ethnic back-ground, and now living in Africa or on the Iberian pen-insula (Spain and Portugal), and in Latin America,8,16
would support the role of environmental factors as de-terminants for the mentioned differences. The prevalencefor wheezing in the last 12 months was lower in Portugal(9.3%, range: 7.4-11.1%) than in Brazilian centers 22.6%(range: 18.4–27.9%); the same occurred between Spain(10.2%, range: 5.5–15.4%) and the other Spanish-speaking Latin American centers (15.0%, range: 6.6–26%). Higher prevalence of asthma was observed inlocalities with a significant black-race population com-pared with the markedly lower prevalences in Africa.Thus, it does not appear that genetic factors are involvedas major determinants for the variations observed in de-veloping Latin American regions. Instead, a strong andsustained environmental influence in which allergens,pathogenic agents, climate, eating habits, lifestyles, andair, water, and food pollution are all factors playing arole.
The prevalence of symptoms of asthma was similar, oreven lower, in some centers with well-known high levelsof air pollution, such as Santiago de Chile, Sa˜o Paulo,and Buenos Aires when compared to centers with muchlower air pollution in the same or different countries.This observation was previously found in Germany17 andin Chile,18 and suggests no causal relationship betweenatmospheric pollution and asthma prevalence in children.
Factors predicted to be protective for asthma becausethey might predispose to a Th1 type of immune responseearly in life do not seem to play that role in LatinAmerica, where gastrointestinal bacterial infections,parasite infestation, poor hygiene, a high number of chil-dren per family, and a high burden and severity of acute
viral infection in infancy are common. All the mentionedfactors affect children from the first months of life, par-ticularly in the more underprivileged localities. In spiteof the prevalence of these supposedly protective factors,the prevalence of respiratory symptoms related to asthmain this region is at least as high as those found by ISAACin centers from developed countries. Furthermore, it wasrecently suggested that endemic intestinal helminthic in-festations can increase the clinical symptoms of asthma19
because total IgE and respiratory symptoms of asthmasignificantly decreased after treating patients who wereinfested byAscaris lumbricoideswith antihelminthicmedications.
The number of children per family in this region ishigher than in developed regions (about 3–4 children perfamily), and crowding is quite common in poor urbanand rural areas, such that the number of children living inthe same house may be even larger than in more devel-oped regions of the world. The number of acute viralrespiratory infections has been reported to be similar tothat occurring in developed regions of the world,3,20 butit should be taken into account that the whole number ofregistered episodes of acute respiratory infections in theregion may be lower than the actual incidence because ofpoor reporting.
Performing ISAAC Phase I in Latin America has pro-vided an opportunity to test the universality of hypoth-eses on protective or detrimental factors for the preva-lence of respiratory symptoms indicative of asthma inchildhood. Many of the hypotheses that seemed reason-able in developed regions do not appear to work in thisregion and possibly in other developing areas of theworld. For example, in most developing communities,colonization withHaemophilus influenzaeor Streptococ-cus pneumoniaeoccurs during the first months of life,and it may be useful to study the protective role of bac-terial colonization of the upper airway tract or gastroin-testinal tract on allergic symptoms through childhood.This raises the question: does swallowing of upper air-ways secretions, which are rich in bacterial agents, helpto induce a stronger Th1 response in infants whose air-ways are colonized very early in infancy?
Latin America is a region with an increasing numberof its countries defined as “transitional economies,” withsubstantial variation in lifestyles, urbanization, and in-equalities of income. Such a region would be ideal forresearch on potentially causative, or protective risk fac-tors associated with asthma in childhood. The danger offuture rapid increases in the prevalence of asthma inthese developing communities, as they increase theirstandard of living, would give an excellent opportunity toinvestigate possible causes of rising prevalence, andhopefully to reverse the continuing upward trend inasthma rates in industrialized countries and developingcountries.
Asthma Symptoms in Latin America 443

CONCLUSIONS
The prevalence of respiratory symptoms related toasthma in children from Latin America is high and quitesimilar to that reported from industrialized countries.There is significant variability in the prevalence ofasthma between participating centers, with a trend to-ward higher figures in centers with a tropical climate.This study also suggests that factors thought to be pro-tective against asthma, such as a higher number of chil-dren per family, a higher number of acute viral respira-tory infections and gastrointestinal parasites, and poorhygiene, do not seem to play a protective role in thisregion. Conversely, these factors seem to act as risk fac-tors for asthma and suggest that the socioeconomic statusof populations is playing a mayor role in the high preva-lence of asthma symptoms in this region.
The present study indicates that asthma can no longerbe considered a minor health problem in Latin America;we suggest that health authorities implement and supportefficient and effective national and regional asthma pro-grams, in order to lessen morbidity and mortality, as wellas to modernize diagnosis and treatment strategies. It islikely that the coexistence of a high prevalence of asthmawith other major respiratory health problems, such asARIs, may increase morbidity and mortality in childrendue to respiratory conditions in Latin America.
REFERENCES
1. Robertson CF, Sennhauser FH, Mallol J. The change in preva-lence and severity of asthma in developed and developing coun-tries. In: Phelan PD, editor. Clinical paediatrics: asthma. London:Bailliere Tindall; 1995. p 253–275.
2. Robertson CF, Heycok E, Bishop J, Nolan T, Olinsky A, PhelanPD. Prevalence of asthma in Melbourne schoolchildren: changesover 26 years. Br Med J [Clin Res] 1991;302:1116.
3. Lopez-Antunano FJ. Epidemiologı´a de las infecciones respirato-rias agudas en nin˜os: panorama regional. In: Benguigui Y, editor.Respiratory infections in children. Washington, DC: PAHO (SerieHCT/AIEPI-1); 1997. p 3–24.
4. Carrasco E. Epidemiological aspects of asthma in Latin America.Chest 1987;91:93–96.
5. Robertson CF, Bishop J, Sennhauser FH, Mallol J. Internationalcomparison of asthma prevalence in children: Australia, Switzer-land, Chile. Pediatr Pulmonol 1993;16:219–226.
6. Soto-Quiroz M, Bustamante M, Gutie´rrez I, Hanson LA, Stran-
negard IL, Karlberg J. The prevalence of childhood asthma inCosta Rica. Clin Exp Allergy 1994;24:1130–1136.
7. Asher MI, Keil U, Anderson HR, Beasley R, Crane J, Martinez F,Mitchell EA, Pearce N, Sibbald B, Stewart AW, Strachan D,Weiland SK, Williams HC. International Study of Asthma andAllergies in Childhood (ISAAC): rationale and methods. EurRespir J 1995;8:483–491.
8. ISAAC Steering Committee. World-wide variations in the preva-lence of asthma symptoms: the International Study of Asthma andAllergies in Childhood (ISAAC). Eur Respir J 1998;12:315–335.
9. European Community Respiratory Health Survey (ECHRS).Variations in the prevalence of respiratory symptoms, self-reported asthma attacks, and use of asthma medication in theEuropean Community Respiratory Health Survey (ECHRS). EurRespir J 1996;9:687–695.
10. Burney PGJ, Luczynska C, Chinn S, Jarvis D. The EuropeanCommunity Respiratory Health Survey. Eur Respir J 1994;7:954–960.
11. Asher MI, Pattemore PK, Harrison AC, Mitchell EA, Rea HH,Stewart AW, Woolcock JA. International comparison of theprevalence of asthma symptoms and bronchial hyperresponsive-ness. Am Rev Respir Dis 1998;138:524–529.
12. Burr ML, Limb ES, Andrae S, Barry DMJ, Nagel F. Childhoodasthma in four countries: a comparative study. Int J Epidemiol1994;23:341–346.
13. Pearce N, Weiland SK, Keil U, Langridge P, Anderson HR, Stra-chan D, Bauman A, Young L, Gluyas P, Ruffin D, Crane J,Beasley R. Self-reported prevalence of asthma symptoms in chil-dren in Australia, England, Germany and New Zealand: an inter-national comparison using the ISAAC protocol. Eur Respir J1993;6:1455–1461.
14. Leung R, Ho P. Asthma, allergy and atopy in three south-eastAsian populations. Thorax 1994;49:1205–1210.
15. Carter-Pokras OD, Gergen PJ. Reported asthma among PuertoRican, Mexican-American, and Cuban children, 1982 through1984. Am J Public Health 1993;83:580–582.
16. Keeley DJ, Neil P, Gallivan S. Comparison of the prevalence ofreversible airways obstruction in rural and urban Zimbabweanchildren. Thorax 1991;46:549–553.
17. Oyarzun M, Pino P, Ancic P, Mun˜oz M, Olaeta I, Cardenas S.Bronchial hyperresponsiveness and air pollution: the baseline of acohort study in Chilean schoolchildren. Am Rev Respir Dis 1993;147:826.
18. von Mutius E, Fritzch C, Weiland SW, Ro¨ll G, Magnussen H.Prevalence of asthma and allergic disorders among children inunited Germany: a descriptive comparison. Br Med J [Clin Res]1992;305:1395–1398.
19. Lynch NR, Palenque M, Hagel I, DiPrisco MC. Clinical improve-ment of asthma after anthelmintic treatment in a tropical situation.Am J Respir Crit Care Med 1997;156:50–54.
20. Denny FW. The clinical impact of human respiratory virus infec-tions. Am J Respir Crit Care Med [Suppl] 1995;152:5–12.
444 Mallol et al.