Embed Size (px)
Citation preview
C L I N I C A L A N D E X P E R I M E N T A L
OPTOMETRY
Prevalence of retinal tears in an optometric population
Anthony Chapman-Davies BOptom MOptom Anka Lazarevic BOptom Lakemba
The prevalence of fresh retinal tears and acute symptomatic posterior vitreous detach- ment (PVD) was determined for a metropolitan optometric population by retrospec- tively examining the records of 2,700 consecutively presenting patients. Twentyeight cases (one per cent) harboured a retinal tear. Fourteen patients manifested operculated tears and a further 14 were found to have flap tears. Significantly more tears lay in the temporal half of the fundus ( p < 0.001). A preponderance of tears lay in the superotemporal retinal quadrant. Twenty-six patients (one per cent) presented with an acute symptomatic PVD. Of these four patients (15 per cent) had a retinal tear related to the onset of the PVD. (Clzn Exp Optom 1996; 79: 1: 12-18)
Accepted for publication: 10 November 1995
Key words: posterior vitreous detachment, retinal break, retinal tear
Retinal tears, in particular symptomatic flap or horseshoe tears, pose a direct threat to vision because a significant number of patients will subsequently de- velop a rhegmatogenous retinal detach- ment. As primary eye care providers op- tometrists should play an important role in detecting such retinal breaks and pro- viding timely referral prior to a clinical detachment occurring. Should a retinal detachment occur, prompt diagnosis and referral are imperative to increase the like- lihood of successful surgical reattachment.
The aim of this study was to estimate the prevalence of fresh retinal tears in an optometric population. It was our experi- ence that fresh retinal tears were encoun- tered commonly in optometric patients. A retrospective analysis was conducted of the records of 2,700 patients presenting consecutively for an initial optometric examination at a private Australian met- ropolitan practice. As acute symptomatic posterior vitreous detachment (PVD) is
intimately involved in the genesis of retinal tears the prevalence of this clini- cal entity was also examined.
METHOD
To estimate the prevalence of fresh retinal tears and acute symptomatic PVD in an optometric population, a retrospective survey of the records of patients present- ing consecutively over a 26month period was conducted. The prevalence of retinal detachment was also noted. The study sample comprised, after exclusions, 5,400 eyes of 2,700 patients. Only patients pre- senting for an initial optometric exami- nation were included in the study. No data were included for patients presenting for follow-up examinations. Nine patients whose ocular media precluded visualisa- tion of the fundus of one or both eyes were arbitrarily excluded from the study.
Retinal tears may be divided into operculated tears, in which a piece of
retina is avulsed, and linear tears. Breaks were categorised as being operculated only if a definite operculum was found (Figure 1). Linear retinal tears may be described as being regular, irregular, horseshoe or straight. Horseshoe or flap tears are the most common variety of lin- ear tears (Figure 2). Hereafter, the termi- nology flap tear will be used to describe all non-operculated tears. Peripheral atrophic retinal holes and macular holes were not included in the study. Only full thickness, fresh retinal tears were counted. Patients with previously diagnosed or treated retinal tears were not included (two cases). The position of the retinal tears was recorded with respect to the four principal retinal quadrants.
Patients were deemed to have an acute symptomatic PVD only if their presenting complaint was that of the acute onset of floaters and/or photopsiae within four weeks preceding the examination. The presence of a PVD had to be confirmed
Clinical and Exoerimental ODtometrv 79.1 lanuarv-Februarv 1996
Retinal tears Chapman-Davies and Lazareuic
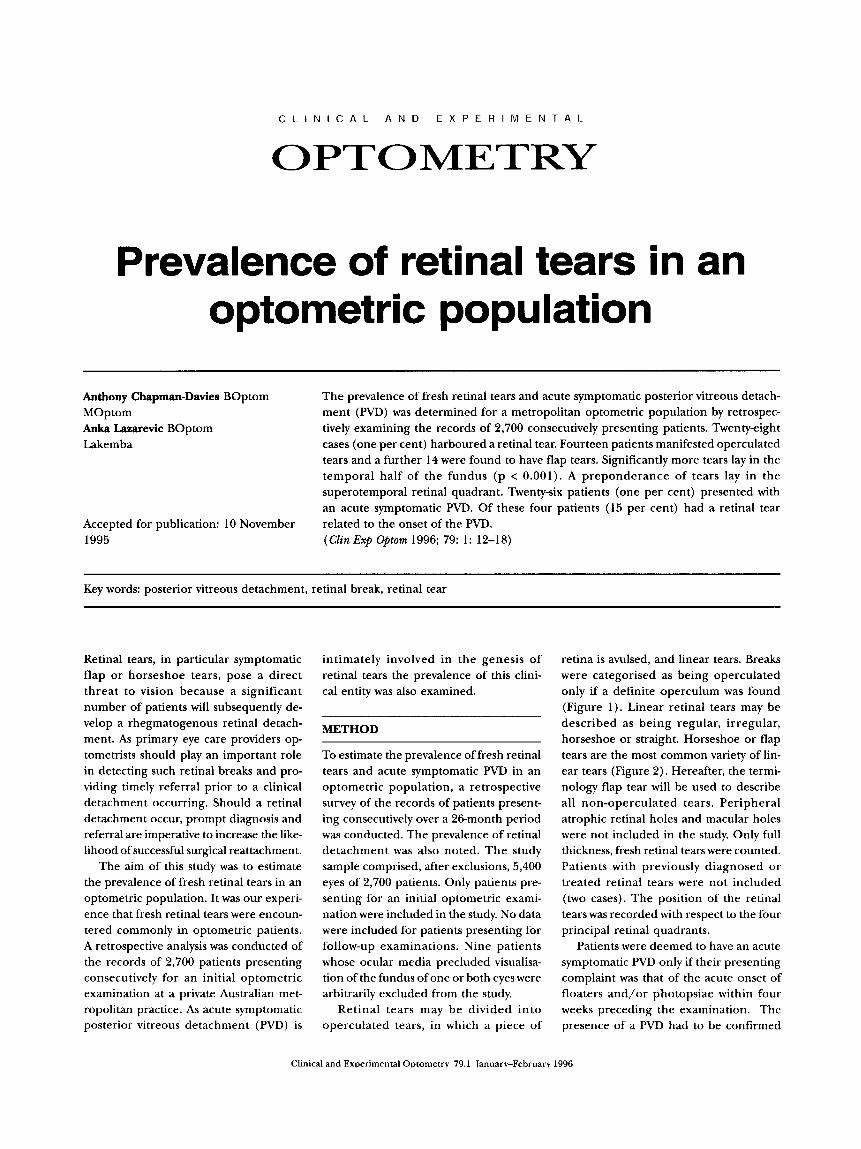
Figure 1. Small operculated retinal tear viewed through a Volk Superfield lens. The break is surrounded by a grey cuff of subretinal fluid. The operculum lies above the break at 11 o'clock and casts a shadow on the retina
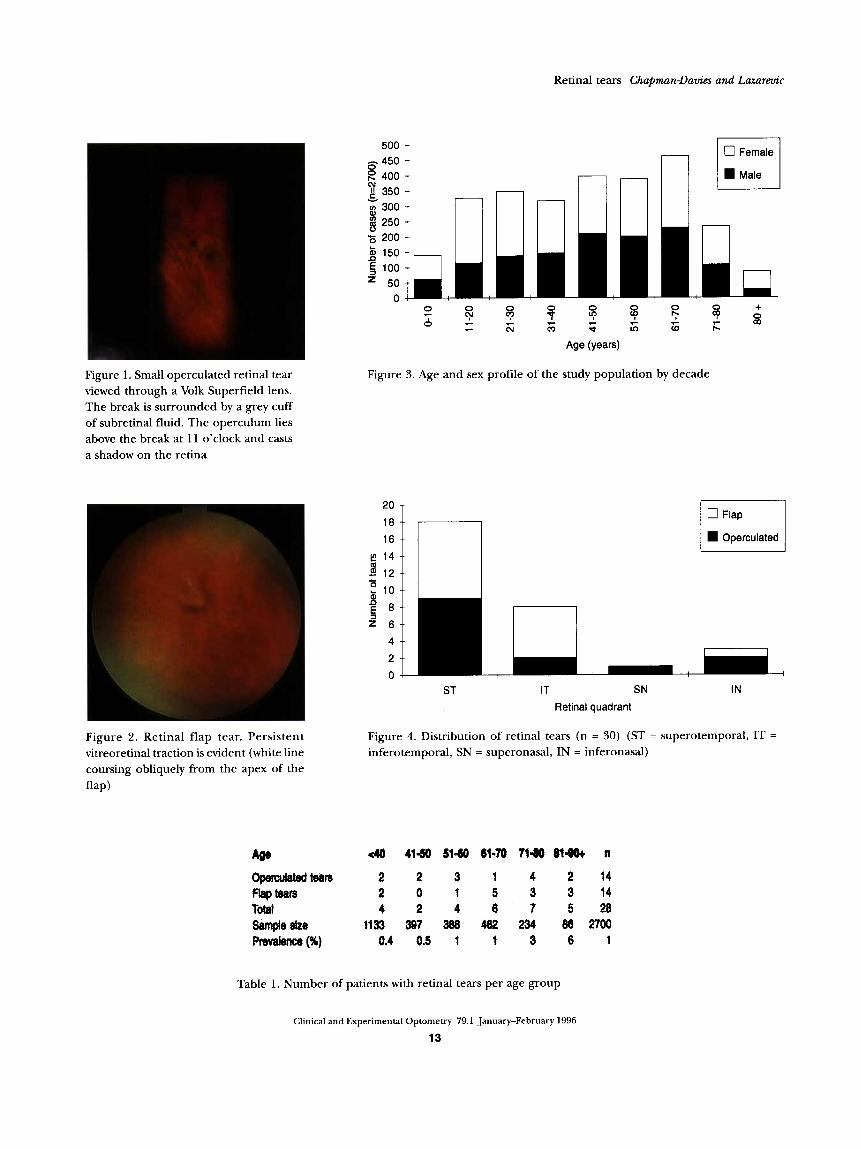
Figure 2. Retinal flap tear. Persistent vitreoretinal traction is evident (white line coursing obliquely from the apex of the flap)
8 450 400 I
N 350 --
8 300 -- 3 250 -- 5 200
150
- - v - --
a
r-
I-i Male
Age (years)
Figure 3. Age and sex profile of the study population by decade
20
16
u- B 0 q h 10
Operculated
ST IT SN IN
Retinal quadrant
Figure 4. Distribution of retinal tears (n = 30) (ST = superotemporal, IT =
inferotemporal, SN = superonasal, IN = inferonasal)
Table 1. Number of patients with retinal tears per age group
Clinical and Experimental Optometry 79.1 January-February 1996
13

Retinal tears Chapman-Davies and Lazareuic
clinically by the appearance of the char- acteristic prepapillary floater and slit lamp examination of the vitreous cavity to de- tect the posterior hyaloid membrane.
It is our practice to routinely dilate all patients unless contraindicated or imprac- tical. Asymptomatic patients were dilated with tropicamide one per cent. In symp- tomatic patients phenylepherine 2.5 per cent was also administered, unless contra- indicated.
All fundi were evaluated using binocu- lar indirect ophthalmoscopy (BIO) (Topcon IDlO) with the Volk Pan Retinal 2.2 condensing lens. Scleral depression was used in the evaluation of some peripheral retinal tears. The Goldmann three-mirror lens was used to examine peripheral lesions when greater resolution was required. Peripheral retinal examination with the Goldmann three-mirror lens was con- ducted routinely on patients with acute symptomatic PVD. Both authors are expe- rienced in the use of the examination techniques employed. All patients were examined by one or other of the authors.
RESULTS
The population comprised 2,700 patients of whom 1,224 were male (45 per cent) and 1,476 were female (55 per cent). The mean age was 45 years. Patients ranged in age from less than one year to 94 years. The fundi of 2,422 patients (90 per cent) were examined through dilated pupils. The age and sex profile for the popula- tion is given in Figure 3.
1. Operculated retinal tears Fourteen phakic patients (0.5 per cent) manifested operculated retinal tears. There were seven males and seven fe- males. The mean age was 61 years. The age distribution for these cases is given in Table 1. An obvious PVD was found in 57 per cent (8/14) of those with operculated tears. Only one patient was symptomatic and this tear was associated with an acute symptomatic PVD. None of the operc- ulated tears was referred for treatment even though one patient was symptomatic.
The distribution of the retinal breaks is given in Figure 4. Seventy-nine per cent
(11/14) of operculated tears lay in the temporal half of the fundus, with 64 per cent (9/14) being found in the supero- temporal quadrant.
Myopia of four dioptres equivalent sphere or greater was found in only two cases.
2. Flap retinal tears A total of 14 phakic patients (0.5 per cent) were found to have a flap tear. Eight were male and six were female. The mean age was 63 years. The age distribution for these cases may be found in Table 1 . Forty- three per cent (6/14) were symptomatic and 50 per cent (3/6) of these presented with an acute symptomatic PVD accord- ing to our criteria. The remainder pre- sented with symptoms of greater than four weeks duration. An overt PVD was noted in 79 per cent (11/14) ofthe patientswith flap tears.
These cases manifested a total of 16 flap tears. One patient demonstrated two flap tears in an eye with an acute symptomatic PVD and a single asymptomatic flap tear in the fellow eye. Although this patient accounted for a total of three retinal tears they were counted as one case. Another patient had a fresh tear in an eye with a previously treated flap tear.
Ninety-four per cent (15/16) of flap tears were found in the temporal retina with 56 per cent (9/16) lying in the superotemporal quadrant (Figure 4 ) . Only one case exhibited myopia of four dioptres equivalent sphere or greater.
Slit lamp fundoscopy with a Goldmann three-mirror lens was needed to confirm the presence of the flap tear in 29 per cent (4 /14 ) of cases. Two cases involved
patients with acute symptomatic PVD who harboured small tears in the oral region which were overlooked with the BIO. In the remaining two cases the three-mirror lens was employed when the BIO findings were equivocal.
All patients with flap tears were re- ferred to a retinal consultant for an opin- ion. Three patients refused referral, two due to poor health. Those who did attend for a retinal consultation ( 1 1 cases) had a total of 13 tears. Nine tears were treated by laser and two with cryopexy. The two remaining tears, found in an 18 and 30-year-old respectively, were left un- treated in favour of periodic monitoring in our practice. Both of these cases were asymptomatic and presented with a nor- mal vitreous gel.
3. Acute symptomatic PVD A total of 26 phakic patients (one per cent) presented with an acute sympto- matic PVD. The frequency would have been greater had a broader definition of acute PVD, including those with symp- toms of up to three months duration, been adopted. There were 11 males and 15 fe- males. The mean age was 66 years. We believe all cases involved spontaneous PVD; in no instance was there a history of contributing (including surgery) or ante- cedent trauma.
The age distribution for the cases is given in Table 2. Acute symptomatic PVD was observed in only one patient under the age of 40 years. This patient was highly myopic. The prevalence of acute sympto- matic PVD was greatest for the seventh and eighth decades.
Fifteen per cent (4/26) of the patients
m 4 0 4150 81-60 61-70 71-60 81-9Ot n
Acute PVD 1 1 2 12 9 1 26 Sample size 1133 397 388 462 234 86 2700 Prevalence (%) 0.1 0.3 0.5 3 4 1 1
Table 2. Number of patients with acute PVD per age group
Clinical and Experimental Optometry 79.1 January-February 1996
14

Retinal tears ChapmanDavies and Lazarevic
who presented with acute symptomatic PVD were found to have a fresh retinal tear. Two were male and two female. There was one case of an operculated tear and three cases with flap tears.
4. Retinal detachment During the sample period there were no cases of rhegmatogenous retinal detach- ment subsequent to a fresh retinal tear or acute symptomatic PVD. However, four cases (0.1 per cent) of previously undiag- nosed retinal detachment were identified. One patient was symptomatic. This case involved a 30-year-old male, with a low degree of myopia, who presented with a right superonasal bullous retinal detach- ment which lay to within 10 degrees of fixation. This rhegmatogenous detach- ment was the result of retinal lattice de- generation with atrophic holes.
The remaining three cases involved asymptomatic, long-standing, inferior retinal detachments. Two cases involved myopic females of 32 and 35 years of age respectively. Both patients had an inferotemporal detachment in their left eye secondary to atrophic retinal holes.
The final case involved a 71-year-old hyperopic male who manifested a right inferotemporal detachment secondary to a retinal dialysis. All cases of retinal de- tachment were referred to a retinal con- sultant. The symptomatic detachment and one case of longstanding detachment were treated surgically. The remaining two cases were referred back to our practice for conservative management.
DISCUSSION
Twentyeight optometric patients (one per cent of patients or 0.5 per cent of eyes) in this study were found to have a fresh retinal tear. The prevalence was greatest for the eighth and ninth decades (Table 1 ) . Full thickness retinal tears were found in 1.9 per cent of autopsied eyes (Straatsma and colleagues cited by Jones and Reidy'). Beyer,2 in a study of 1,700 essentially asymptomatic cases, established that 2.1 per cent had a retinal tear. Operculated tears were found in 1.2 per cent of these cases while flap tears were
seen in 0.9 per cent of patients. Okun' examined 494 consecutive eyes from 250 autopsies and found two cases of operculated tears and eight cases of flap tears.
While our study found that retinal tears occurred commonly in an optometric population, the prevalence is lower than that reported in the aforementioned stud- ies. Small retinal breaks, particularly those in the oral region, may have been over- looked as the retinal periphery was not examined routinely with the Goldmann three-mirror lens or scleral depression.
Siege1 and coworker^,^ in a study exam- ining the quality of fundus examination with and without pupillary dilatation, found two operculated and two flap tears in an optometric population comprising 500 adult subjects. From their data it is not possible to ascertain if the four tears represented four individual cases (a preva- lence of 0.8 per cent) or whether more than one tear was found in a given sub- ject. They stated that, using conventional means of fundus examination, all anoma- lies lying anterior to the clinical equator would have been missed if the pupil had not been dilated. This position is extreme as, from our experience, the fundus pe- riphery may be examined without mydriasis using indirect ophthalmoscopy, depending on pupil size and the clarity of the media. Obviously, fundoscopy is facilitated with mydriasis.
In contrast, G~tter idge,~ in a study of 1,600 consecutively presenting optomet- ric patients, found only one patient (0.06 per cent) with a previously undetected retinal tear. Fundoscopy with mydriasis was performed only on indication. From the present study and published data, this would appear to be an under- representation of the prevalence of fresh retinal tears.
This study confirms previous findings that the significant majority of retinal tears are found in the temporal half of the fundus (chi square with Yates' correction p <0.001) .2,6,7,8 In general, breaks are seen most frequently in the superotemporal quadrant followed by the inferotemporal, superonasal and inferonasal quadrants re~pectively.~ While our study confirmed
this relationship for the temporal fundus, we found more tears in the inferonasal than in the superonasal quadrant. Okun3 reported a similar finding.
Few tears were found in patients un- der 40 years of age. Sixty four per cent (18/28) of retinal tears were found in in- dividuals over 60 years of age. In view of the intimate relationship between PVD and the development of retinal tears, this relationship is expected.
A PVD occurs when the vitreous cor- tex separates from the sensory retina and optic disc. If the separation extends to the ora serrata, the detachment is said to be complete. Should the separation involve a discrete region it is termed incomplete. PVD can be further subcategorised into those with or without collapse of the vit- reous gel. The most common form of de- tachment is a complete PVD with collapse of the vitreous gel.'(' Clinically, one sees the characteristic prepapillary floater com- prised of epipapillary glial tissue avulsed from the disc. The prepapillary opacity may assume the form of a perfect annu- lus or Weiss ring (Figure 5) . With the slit lamp the posterior hyaloid membrane appears as a grey, wrinkled structure drap ing down from the superior vitreous base (Figure 6). Posterior to the hyaloid mem- brane lies the optically dark liquified vit- reous. PVD usually results from the normal
ageing processes of the vitreous gel, syneresis and synchysis, although it may occur secondary to trauma or posterior uveitis.' It is more common in myopic or aphakic eyes.' The prevalence of PVD be- comes noteworthy (over 20 per cent) in the seventh decade and rises to over 60 per cent by the ninth de~ade .~ ,"
PVD is the principal predisposing phenomenon in the development of rhegmatogenous retinal detachment.12 In patients with retinal compromise, such as lattice degeneration or vitreoretinal tufts, PVD may lead to the formation of a retinal break. Lattice degeneration was found in 29 per cent (4/14) of patients with flap tears in this study. PVD may occur insidi- ously, without giving rise to symptoms, or it may assume an acute form characterised by the sudden onset of floaters and/or
Clinical and Experimental Optometry 79.1 January-February 1996
15
Retinal tears Chapman-Davies and Lazarevic
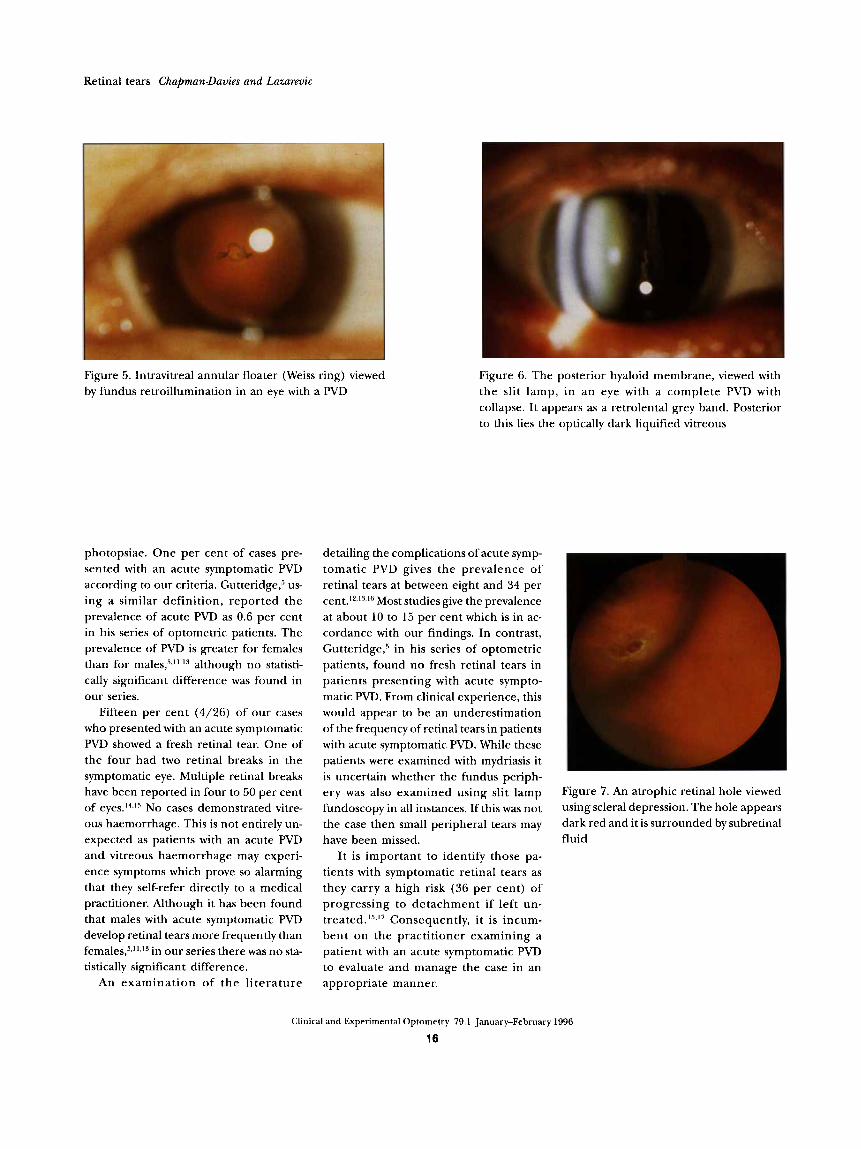
Figure 5. Intravitreal annular floater (Weiss ring) viewed by fundus retroillumination in an eye with a PVD
photopsiae. One per cent of cases pre- sented with an acute symptomatic PVD according to our criteria. Gutteridge,' us- ing a similar definition, reported the prevalence of acute PVD as 0.6 per cent in his series of optometric patients. The prevalence of PVD is greater for females than for males,',",'3 although no statisti- cally significant difference was found in our series.
Fifteen per cent (4/26) of our cases who presented with an acute symptomatic PVD showed a fresh retinal tear. One of the four had two retinal breaks in the symptomatic eye. Multiple retinal breaks have been reported in four to 50 per cent of eye^.'^,'^ No cases demonstrated vitre- ous haemorrhage. This is not entirely un- expected as patients with an acute PVD and vitreous haemorrhage may experi- ence symptoms which prove so alarming that they self-refer directly to a medical practitioner. Although it has been found that males with acute symptomatic PVD develop retinal tears more frequently than female^,'^",'^ in our series there was no sta- tistically significant difference.
An examination of t he l i terature
Figure 6. The posterior hyaloid membrane, viewed with the slit lamp, in a n eye with a complete PVD with collapse. It appears as a retrolental grey band. Posterior to this lies the optically dark liquified vitreous
detailing the complications of acute symp- tomatic PVD gives the prevalence of retinal tears at between eight and 34 per ~en t . ' * . ' ~ , ' ~ Most studies give the prevalence at about 10 to 15 per cent which is in ac- cordance with our findings. In contrast, Gutteridge,' in his series of optometric patients, found n o fresh retinal tears in patients presenting with acute sympto- matic PVD. From clinical experience, this would appear to be an underestimation of the frequency of retinal tears in patients with acute symptomatic PVD. While these patients were examined with mydriasis it is uncertain whether the fundus periph- ery was also examined using slit lamp fundoscopy in all instances. If this was not the case then small peripheral tears may have been missed.
It is important to identify those pa- tients with symptomatic retinal tears as they carry a high risk (36 per cent) of progressing to detachment if left un- treated.l5.I7 Consequently, it is incum- bent on the practitioner examining a patient with an acute symptomatic PVD to evaluate and manage the case in an appropriate manner.
Figure 7. An atrophic retinal hole viewed using scleral depression. The hole appears dark red and it is surrounded by subretinal fluid
Clinical and Experimental Optometry 79.1 January-February 1996
16

Retinal tears Chapman-Dauies and Lazarevic
The history should not only include reference to the onset and duration of symptoms but also to the exact nature of the photopsiae and/or entopsiae them- selves. While the experience of photop- siae in such patients is indicative of vitreoretinal traction, it is not directly as- sociated with the finding of retinal breaks. The frequency of retinal tears is greatest in patients reporting both photopsiae and floaters when compared with those who experience either symptom in isola- tion.I2>l6 The location of the photopsiae provides scant clinical evidence of the like- lihood of a retinal tear or its potential lo- cation. The majority of patients experi- ence photopsiae in the temporal visual field of the symptomatic eye while the majority of tears are found in the tempo- ral retina.I6 Patients who describe a dif- fuse scattering of minuscule 'dots' in their visual field (myiodesopsia) have a high fre- quency (52 per cent) of retinal tears.I6
Fundoscopy should be performed with a BIO and maximal mydriasis. Ideally, the pupils should be dilated with tropica- mide one per cent in combination with phenylepherine 2.5 per cent, unless contra-indicated. Medium to large tears will normally be readily apparent. Scleral depression may be used to highlight breaks in the retina by increasing the con- trast between the intact retina and the break (Figure 7). The procedure for scleral depression has been elucidated previously in this journal." If a vitreous haemorrhage is apparent, then the patient should be assumed to have a retinal tear until proven to the contrary." The preva- lence of retinal tears in such eyes is be- tween 70 and 90 per ~ent . '~ , ' ' . l~
Provided no obvious retinal breaks are discovered, the fundus periphery should then be re-examined under higher mag- nification, using slit lamp fundoscopy, to search for small retinal tears. Particular attention should be given to the superotemporal retinal quadrant. The Goldmann three-mirror lens proves exem- plary for this task. In our study, 50 per cent (2/4) of retinal tears in patients present- ing with acute symptomatic PVD were missed with the BIO and were detected only with the Goldmann three-mirror
lens. The overwhelming majority of retinal tears are less than one quarter of a disc diameter in size.2 The morbidity of small symptomatic tears should be consid- ered no less than for their larger counter- parts, as any retinal break, regardless of size, type or location, may, given the a p propriate pathophysiological circum- stances, lead to retinal detachment6 The progression to retinal detachment may be greater for smaller breaks.I5
The vitreous cavity ought to be searched carefully with the slit lamp for the presence of cells, particularly red blood cells and pigment. The greater the density of cells, the more likely a retinal break will be present.16 A positive Shafer's sign (pigment cells in the vitreous) is vir- tually pathognomonic of a retinal tear or deta~hment . '~
Similarly, the asymptomatic eye should be examined carefully as retinal breaks are found in between two and four per cent of fellow eyes.12J6 Provided no overt retinal tears are discovered, the patient should be re-evaluated periodically. Delayed retinal breaks may occur up to six months following the acute onset of ~ymptoms.'~'~ Our office protocol provides for patients with acute symptomatic PVD to be re- examined after two to four weeks and then, depending on symptoms and the overall clinical picture, periodically until the sixth month.
Finally, the symptoms of retinal detach- ment should be discussed with the patient. It is imperative to emphasise the impor- tance of returning immediately if the symptoms change in nature or frequency in the eye with the acute PVD. Further- more, the patient should be advised to return without delay should symptoms develop in the contralateral eye. Compli- cations of acute symptomatic PVD which are patent in the first eye are often mim- icked in the fellow
The management of patients who har- bour a retinal tear is essentially governed by whether they are symptomatic. While the classification of tears on the basis of symptomatic versus asymptomatic is arbi- trary, it does hold clinical merit when one examines the natural history of retinal tears. Obviously, other clinical factors
must also be given consideration. Breaks in the superior half of the fundus, those associated with a subclinical detachment (in which sub-retinal fluid extends for more than one disc diameter from the break), a history of retinal detachment in the fellow eye, lattice degeneration, mod- erate to high myopia and aphakia should excite greater clinical concern.
The risk of a symptomatic operculated tear progressing to a retinal detachment is relatively low, about 12 to 16 per cent, as vitreoretinal traction is released once the portion of retina is a v u l ~ e d . ' ~ ~ " ~ ~ ~ In our study, one patient had a symptomatic operculated tear. This patient was not re- ferred for treatment as the tear was small, there was no significant accumulation of subretinal fluid and the break was located inferiorly. If a symptomatic operculated tear is large, superiorly located or if there is a subclinical detachment, referral is warranted.
Ninety-three per cent (13/14) of our patients with operculated tears were asymptomatic with the break being found incidentally during routine BIO. A number of studies have shown that asymp tomatic operculated tears do not progress to de ta~hment .~ , '~ .~ ' At the time of writing, none of the operculated retinal tears in our study had progressed to a retinal de- tachment. Nevertheless, patients with operculated retinal tears should be re- evaluated routinely, depending on the individual clinical circumstances.
Operculated tears need to be differen- tiated from simple peripheral atrophic retinal holes (Figure 7 ) . The latter are readily diagnosed by the conspicuous lack of an operculum either in close proxim- ity to the break or lying more remotely in the vitreous cavity. Although they repre- sent the most common type of retinal break,2 atrophic holes were not counted in the present study. Such holes are found in about seven per cent of eyes.2 The risk of progression to a detachment is low (six per cent) .I5 Consequently, such breaks usually may be managed conservativelyvia periodic observation.
Patients with fresh symptomatic flap tears should be referred promptly to a retinal consultant as the risk of retinal
Clinical and Experimental Optometry 79.1 January-February 1996
17

Retinal tears Chapman-Davies and Lazareuic
detachment is at least 35 per ~ent.", '~,*' ' Forty-three per cent of our patients with flap tears were symptomatic. The poor prognosis for these tears is related to per- sistent vitreoretinal traction (Figure 2). Untreated symptomatic breaks which progress to retinal detachment usually do so within six weeksL5 Once treated, the detachment rate for symptomatic flap tears is zero to 19 per cent.20
The natural history of asymptomatic flap retinal tears is less certain. Davis15 found between 23 to 40 per cent of such tears progress to detachment. In contrast, Byer6aZ1 reported that no asymptomatic flap tears progressed to retinal detach- ment. None of the untreated flap retinal tears in our study, whether symptomatic or not, had progressed to a retinal detach- ment at the time ofwriting. While the risk of retinal detachment in patients with asymptomatic flap tears is less than for their symptomatic counterparts, we feel that it is prudent to refer patients with such tears to a retinal consultant for an opinion, particularly if there is a sub- clinical detachment.
CONCLUSION
One to two per cent of patients harbour a retinal tear. These breaks may be silent or heralded by symptoms of floaters and/or photopsiae. Management of these cases will normally be dependent on whether the patient is symptomatic. Depending on the inherent clinical characteristics of each case, the breaks may be managed conservatively, via periodic observation, or referral for prophylactic laser or cryopexy may be mandated. The prompt recogni- tion and management of fresh retinal tears which have already progressed to a clinical detachment are paramount to in- crease the prospect of successful surgical reattachment.
Primary eye care practitioners will also be confronted by patients presenting with acute symptomatic PVD. About 15 per cent of these patients will have a peripheral retinal tear. It is imperative that these tears, particularly flap tears, be diagnosed as they carry a significant risk of progressing to a retinal detachment if left untreated.
ACKNOWLEDGEMENT This study was inspired by Emeritus Pro- fessor H Barry Collin. I thank Mr Paul Pavlou of the CCLRU for enlarging the photographs used in Figures 1, 5 and 6.
REFERENCES 1.
2.
3.
4.
5.
6 .
7.
8.
9.
Jones WL, Reidy RW. Atlas of the Periph- eral Ocular Fundus, Boston: Butterworth Publishers, 1985: 134, 148, 150. Byer NE. Clinical study of retinal breaks. Trans Amer Acad Ophthalmol Otolaryngol
Okun E. Gross and microscopic pathology in autopsy eyes, part 111. Retinal breaks with- out detachment. AmerJOphthalmol1961; 51:
Siege1 BS, Thompson AK, Yolton DP, Reinke AR, Yolton FU. A comparison of diagnostic outcomes with and without pupillary dilata- tion. JAmer Optom Assoc 1990; 61: 25-34. Gutteridge IF. The prevalence of posterior vitreous detachment-a prospective study in an optometric patient population. Clin Exp Optom 1993; 76: 8-16. Byer NE. Prognosis of asymptomatic retinal breaks. Arch Ophthalmoll974; 92: 208-210. Tulloh CG. Distribution of holes and tears in primary retinal detachment. Bn't J Ophthalmoll965; 49: 413-431. Shapland CD. Retinal detachment and Gonin's operation. Trans Ophthalmol Sac UK
Duke-Elder S, Dobree JH. Diseases of the Retina. In: Duke-Elder S. ed. System of Ophthalmology Vol X. London: Henry Kimpton, 1967: 790.
1967; 71: 461-472.
369-389.
1932; 52: 170-185.
10. Alexander LJ. Primary Care of the Poste- rior Segment, East Norwalk Appleton and Lange, 1989: 212-213.
11. Foos RY, Wheeler NC. Vitreoretinal junc- ture synchisis senilis and posterior vitreous detachment. Ophthalmology 1982; 89: 1502- 1512.
12. Hikichi T, Trempe CL. Relationship be- tween floaters, light flashes, or both, and complications of posterior vitreous detach- ment. AmerJOphthalmoll994; 117: 593-598.
13. Novak MA, Welch RB. Complication of acute symptomatic posterior vitreous detach- ment. AmerJOphthalmol1984; 9 7 308-314.
14. Halpern JI. Routine screening of the retinal periphery. Amer J Ophthalmol 1966; 62:
15. Davis MD. Natural history of retinal breaks without detachment. Arch Ophthalmoll974;
16. Boldrey EE. Risk of retinal tears in patients with vitreous floaters. Amer J Ophthalmol 1983; 96: 783-787.
17. Colyear BH, Pischel DK. Clinical tears in the retina without detachment . Amer JOphthalmoll956; 41: 773-791.
99-102.
92: 183-194.
18. Shuey NH, Anderson AJ, Siderov J. Scleral indentation: a review of the procedure and indications for use. ClinExp Optom 1995; 78: 108109.
19. Chapman-Davies A. Shafer's sign and asso- ciated retinal tear. Clin Exp Optom 1993; 76: 174176.
20. Benson WE. Retinal Detachment Diagno- sis and Management, 2nd ed. Philadelphia: JB Lippincott Company, 1988: 193-194.
21. Byer NE. The natural history of asympto- matic retinal breaks. Ophthalmology 1982; 89: 1033-1039.
Author's address: A Chapman-Davies 44 The Boulevarde Lakemba NSW 2195 AUSTRALIA
Clinical and Experimental Optometry 79.1 January-February 1996
18



























![$PQZSJHIU …ousar.lib.okayama-u.ac.jp/files/public/5/56175/...rhages, retinal pigment epithelial tears, and/or chorio-capillaris atrophy [9-11]. The risk of serious complica-tions](https://img.pdfslide.net/doc/110x75/5e274ba9c8f801547e287b2d/pqzsjhiu-ousarlibokayama-uacjpfilespublic556175-rhages-retinal-pigment.jpg)