Embed Size (px)
Citation preview

Preventing adolescent alcohol and drug use:Universal Approaches
Clare J. Mackie, Ph.D.Lecturer
Addictions DepartmentInstitute of Psychiatry, KCL

Outline
Lecture 1: Universal
Lecture 2: Selective
Lecture 3: Indicated

Learning outcomes
Aim: To provide an overview of some key issues in the prevention of adolescent alcohol and drug use After attending this lecture students should be able to: Outline the underlying risk and protective factors of
early onset adolescent alcohol and drug use Describe the main differences between universal,
selective and indicated prevention programs Outline the major ways that preventing alcohol and
drug use is implemented in schools Highlight the main issues or barriers to
implementation of school-based drug prevention programs

Lecture 1: Universal Prevention ProgramsPlan 1. Overview of different prevention strategies2. Prevalence of alcohol and drug use in
adolescence3. Why are adolescents vulnerable to alcohol
and drug use? 4. Different universal prevention programs 5. Effectiveness 6. Summary and Conclusions

1. Intervention strategies
The continuum of care model –Institute of Medicine (USIP –Mrazek & Haggerty, 1994)

1. Intervention strategies
Prevention strategy
Target Population
Examples Negative Effects
Cost
Universal General Public Childhood immunisation
Low Cost per individual is low
Selective Individuals with a higher risk of developing the disorder
Preschool programs for children in low SES areas
Minimal or low
Moderate costs
Indicated High risk individual with minimal or some evidence of disorder –do not make diagnostic criteria
Parental-child training for behavioural difficulties
Some risk May be high
Mrazek & Haggerty (1994)

1. Intervention strategies
Universal prevention
Addresses general public or the segment of the entire population with average probability of developing the disorder
Selective Prevention
Specific sub-population with risk significantly above average, imminently or over lifetime
Indicated Prevention
Addresses identified individuals with minimal but detectable signs or symptoms of a disorder
Revised Institute of Medicine Classification of Prevention approaches (Springer & Philips, 2007)

1. Intervention strategies
Indicated
Selective
Universal Prevention
Early Intervention
TREATMENT
Likelihood of developing problems

1. Intervention strategiesSummary
Universal programs Aim to reach the general population in a defined
setting E.g. School education in schools
Selective programs Target high risk groups who are yet to show
problematic behaviour – E.g. Children of alcoholics
Indicated programs Programs for individuals who are showing early signs
of problematic behaviour – E.g. Brief interview to reduce alcohol use (e.g. CBT
or MI)

2. Prevalence and trends of alcohol and drug use in young
people
European School Project on Alcohol and Drugs (ESPAD; Hibell, 2007) www.espad.org 14-16 years of age
UK has the amongst the highest rates of drunkenness, binge drinking and alcohol consumption in Europe
75% had 1 episode of drunkenness, 1/3 had 20 or more episodes in their lives
Half were intoxicated in the last month and a ¼ intoxicated in at least 3-times
Trends: more people drink regularly (once a week). Weekly drinkers drink more. Regular young drinkers drink more per session (Binge drinking).
Change in types of drinks (alcopops).

2. Prevalence and trends of alcohol and drug use in young
people ESPAD survey (Hibell et al., 2004) showed that for 15-
16yrs the prevalence of cannabis use increased from 3-44% between 1995-2007
2-36% of students report cannabis use in the previous 12 months
Lifetime prevalence of cannabis use is 38%, in the past year 31% and in the past month 20%
In all countries males reported higher use than females
The number of young people reported being offered cannabis increased from 46% in 2002 to 50% in 2004.
The number of young people who reported knowing someone who used cannabis increased from 65% to 68% in the same period
In the UK, LSD, ecstasy and amphetamines are the next most prevalent drugs with an 8% prevalence



2. Prevalence and trends of alcohol and drug use in young people

U.S. Statistics suggest similar trends: Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. Monitoring the Future national results on adolescent drug use: Overview of key findings, 2006. (NIH Publication No. 07-6202). National Institute on Drug Abuse, 2007.Canada:

Journal of Substance Abuse, 2001

3. Adolescent Development
‘Adolescents make a lot of decisions that the average 9-year old would say was a dumb
thing to do’ (Ronald E. Dahl, NYAS Magazine, 2003
Why are adolescents susceptible to alcohol and drug use? Adolescents are highly vulnerable to social influences,
have lower tolerance levels and become dependent at lower doses than adults (Fowler et al., 2007).
Early onset also heightened risk of developing addictive disorders and other internalising/ externalising disorders (Grant & Dawson, 1998).
More severe, complex course of disorder with significant health and social consequences.

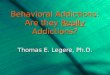
The above composite MRI image shows top-level views of the sequence of gray matter maturation over the brain. Researchers have found gray matter volume increases at earlier ages following a subsequent decline into puberty, correlating with advanced cognitive abilities. This signals the greater organisation of the brain (Gogtay, 2004)

3. Adolescent Development
Adolescence is a period of brain transformation Peak period of neural reorganisation, with the
development of the prefrontal cortex. Extensive myelination enabling faster processing and
online planning Earlier development of the nucleus accumbens, part
of the brains reward system relative to the orbitofrontal cortex, responsible for decision making is responsible for adolescents risky behaviour (Garavan, 2005)

3. Adolescent DevelopmentThe brain
(Tapert & Schweinsburg, 2005)

To summarise
Adolescents in the UK are consuming extensive amounts of alcohol, in particular binge drinking compared to other European countries
Adolescence is a particular period of developmental susceptibility – Social influence – Neural changes which can increase reward
susceptibility, impulsive and risk taking behaviour.– Earlier the onset of SUD more complex the course
and more comorbid problems arise

4. Current approaches to Universal prevention
Drug knowledge
School-based alcohol and drug prevention programs
Information dissemination and fear arousal Students are taught about the dangers of
tobacco, alcohol or drug use in terms of adverse health, legal consequences
Conceptually based on a cognitive model of drug use- assumes that individuals will make a rational decision about using drugs.
Fear-arousal techniques to scare students into avoiding drug use.


4. Current approaches to prevention Drug knowledge
Effectiveness Evaluation studies show impact
on attitudes and knowledge, but fail to show a reduction in alcohol/drug use
Some studies show increased drug use

4. Current approaches drug prevention
Affective education
Affective education models Assume that promoting personal
affective development in students will reduce the likelihood of drug abuse – Decision making– Effective communication – Assertiveness– Norm-setting messages
E.g. material showing those who drink, so in a responsible manner

4. Current approaches drug prevention
Affective education
Effectiveness No impact on drug use Exercises designed to increase
self-awareness, but no evidence to show that these exercises had an impact on the reduction of drug use.– Failure to show understanding of the
role of social influence in adolescent drug use

4. Current approaches to drug prevention
Social Competence
Social Influence approaches Recognition of the importance of
psychosocial factors in the imitation of drug use
Smoking prevention field- adolescent cigarette smoking was the result of influences from peers and media
Social factors plays a part in the initiation of SUD –through modelling behaviour (Bandura, 1977 social learning theory)


4. Current approaches to drug prevention
Social Competence Psychological inoculation
– Non-smokers were inoculated against pro-smoking messages by exposing students to strong pro-smoking messages then teaching students to deal with such influences
Correcting normative expectations – Collection of saliva samples of objective smoking
behaviour – Providing actual smoking prevalence rates in each
classroom Social resistance skills training
– Teach students to avoid high-risk situations, give knowledge, confidence to deal with peer pressure,
– Aware of pro-smoking messages in the media

4. Current approaches to drug prevention
Social competence
Effectiveness Studies have demonstrated the effectiveness
of prevention programs that have utilised resistance skills training.
Most studies have focused on smoking prevalence – Studies report a reduction of smoking prevalence
of 30-50% after initial intervention.– Reduction of smoking onset 30-40% when
comparing proportion of new smoking in the experimental versus control groups.
– However, fewer behavioural effects for alcohol than tobacco use.
– Longer term follow-ups show a degrading of prevention effects

4. Current approaches to drug prevention
Competence–Enhancement
Implicit in social influences approaches are the assumption that adolescents do not want to smoke/ take drugs For some students drugs may have an
instrumental value such as reducing anxiety, low self-esteem. – Competence-enhancement approaches emphasise
generic personal and social skills in combination with resistance skills.
– Drug use behaviour is learned through a process of modelling, imitation and reinforcement and thus influences pro-social beliefs.
– These factors along with poor personal and social skills will increase an adolescents susceptibility to social influences to favour drug use

4. Current approaches to drug prevention
Competence–Enhancement
Methods Emphasis on generic personal self-
management skills and social skills – Decision making skills – Problem-solving skills – Cognitive skills for resisting media influences – Enhancing self-esteem – Coping strategies for deal with anxiety – Assertiveness skills

Life skills training (Botvin et al., 1995; 2000;
2007) Designed to reduce the risks associated with
alcohol, tobacco and drug use 3 components
– Drug resistance skills – Personal self-management – General social skills
Cognitive behavioural skills 15 1-hour in-class sessions Manual based

Life skills training Outcomes
Botvin et al., (1995) 3597 adolescents from 56 schools
in USA 52% male, 91% white, mean age
18.06 yrs – 6-year follow-up – A significant reduction in weekly and
monthly cigarette use– No significant impact on alcohol use

Life skills training Outcomes
Botvin et al., (2000)– Subsample of 447 participants
answered a questionnaire on illicit drug use
– 92% white, 40% male– Mean age 18.1 year – Follow-up 6.5 years

Life skills training Outcomes
Drug use Intervention group
Control group
P-value
Cannabis 2.05 2.40 .07
Cocaine 0.72 0.73 .37
Inhalants 0.71 0.73 .66
Nonmedical pill use
0.72 0.72 .94
Heroin 0.70 0.72 .0001
Hallucinogens
0.73 0.75 .002
Total illicit drug use
5.59 6.05 .045

Strengthening Families program (SFP)
Universal prevention program designed for use with all pupils between 10-14 years to increase resilience and reduce risk factors for alcohol and SUD (and delinquency etc)
3 broad areas are addressed– Family functioning
Communication between parents and children – Resisting peer pressure – Stress management
7 2hr sessions– One hour with pupils and parents separately – One hour with both pupils and parents together
6-12 months later there are 4 booster sessions

Strengthening Families program (SFP)
Theoretical model
Biopsychosocial model – Skills and resources possessed by families
can ‘buffer’ other stresses Resiliency model (Kumpfer and Richardson)
– ‘protective processes’, nurturing life skills in young people
Family process model– Impact of economic stress on parents and
subsequent effects on mental health

Strengthening Families Program Outcomes
(Spoth et al., 2009)
1,309 eligible families with 11-12 year olds.
238 families were allocated to SFP 221 were allocated to a comparison
family program (preparing for the drug free years: PDFY) in 5 2-hour weekly sessions
208 were controls Follow-ups were at 6, 18, 30, 48, 72
months

Strengthening Families Program
Outcomes
Variable RRR (%) RRR (%)
SFP V’s control
PDFY v’s Control
Drunkenness
19 9
Alcohol problems
23 11
Cigarettes 23 11
Illicit drugs 31 16
RRR: Relative Reduction Rate: The estimated proportion of control cases that could have been
prevented had those individuals been in the intervention condition

Barriers to implementation and effectiveness
(Spoth and Redmond, 2000)
Time demands and scheduling Family member resistance Mental health of the family
member – Not shown to impact on outcome or
attrition Legitimacy beliefs (Spoth et al.,
1997)

5. EffectivenessAlcohol
Foxcroft et al., (2003) reported on the effectiveness of primary prevention of alcohol misuse in young people
56 studies were examined with a range of alcohol use variables
Short-term (1 year)– 15 studies were partially effective – 24 non-significant outcomes – 4 studies increased drinking – There were no difference between content as all focused
on knowledge and social skills Medium-term (1-3 years)
– 12 studies were partially effective – 19 non-significant outcomes – 2 studies increased drinking

5. EffectivenessAlcohol
3 studies were identified as effective over the long term (3 years)
1. Strengthening families program (SFP, Spoth 2001). – The Number needed to Treat for SFP over 4yrs for 3
alcohol initiation behaviours (alcohol use, alcohol use without permission and first drunkenness) was 9 (for every 9 individuals who receive the intervention there will be one fewer person who increases their alcohol use)
2. Life skills Training (Botvin 1995) knowledge, social and life skills. Sig effect on attitudes, knowledge and drunkenness.
3. Schinke (2000) a culturally and community focused preventative intervention for native American youth. 7% reduction in weekly alcohol use
Studies over the short and medium term were not able to establish effectiveness

5. EffectivenessDrug use
Faggiano et al., (2008) reviewed the evidence for effectiveness of universal school-based drug use prevention
29 RCTs of which 28 were conducted in the USA
Focused on – first time usage,– the prevalence of use, – Drug use knowledge – Drug use attitudes – Drug use problems/behaviours

5. EffectivenessDrug use
Comparison Outcome Effect size References
Skills vs Usual Curricula Cannabis use Relative risk (RR) = 0.82
Botvin et al., (1995)
Affective vs usual Curricula
Cannabis use p =.004 1yr p=.0003 2 yr
Hansen et al., (1998)
Stimulant drugs P < .05 at 1 yr Sexter et al., (1984)
Knowledge vs Usual Curricula
Drug knowledge Standard Mean Difference (SMD) = 0.91
Corbin et al., (1993)
Skills vs affective Self-efficacy Weighted Mean Difference = 1.9
Jones et al., (1990)
Skills vs knowledge Cannabis use P <.05 at 1yrP >.05 at 2yr
Hansen et al., (1991)
Affective vs Knowledge Drug knowledge SMD = .60 Corbin et al., (1993)
Decision-making skills
SMD = 1.2 Jones et al., 1995)

5. EffectivenessConclusions
Skills based programs – have a positive effect on both mediating variables (e.g. drug
knowledge, decision-making) compared to usual curricula. – Skills based 20% reduction in cannabis at post-test and a 55%
reduction in hard drug use.
Affective programs – improve decision-making skills
Drug knowledge– Improved drug knowledge – but similar to usual curricula in drug outcomes

5. Effectiveness Delivery method
Delivery method is a critical ingredient in the successful programs. – Interactive V’s Non-interactive
Interactive method allows for exchange of ideas
Allows adolescents to practice newly acquired skills and receive feedback
Interactive content (e.g. Computer programs) allows feedback during the exercises
Non-interactive methods are better suited in early adolescence

5. Effectiveness Delivery method
-0.1
-0.05
0
0.05
0.1
0.15
0.2
All programs
Non-interactive
Interactive
Overall program effect and effect
by delivery method (Tobler et al.,
2000)

5. Effectiveness Delivery method
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
Non-interactive Interactive
Attitudes
Cannabis use
Drug use attitudes and cannabis use for 19 programs
that included both measures (Tobler et
al., 2000)

5. Effectiveness Delivery method
-0.1
-0.05
0
0.05
0.1
0.15
0.2
0.25
Non-interactive Interactive
Tobacco
Alcohol
Cannabis
Type of alcohol and drug for all
programs (Tobler et al., 2000)

6. Summary and Conclusions
The prevalence of alcohol and cannabis use are increasing in the UK
Adolescents who begin their onset early in development are at risk of developing associated social and health-related problems
Current knowledge-based prevention programs implemented in UK classrooms are not effective in reducing alcohol and drug use
Social competence programs with interactive delivery are shown to be most effective compared to usual curriculum, affective and knowledge based programs

6. Summary and Conclusions The majority of these interventions are conducted in
the US where abstinence is the main goal This may not be the target outcome for drinking
behaviour in other countries where the emphasis is on sensible drinking
However: only 14% of programs are effective in
decreasing substance use (Ennett et al., 2003) Insufficient resources to implement long-term
programs Lack of teacher training to deliver Adaptation of programs to the UK population