Embed Size (px)
Citation preview

PREVENZIONE DEL PREVENZIONE DEL WHEEZING WHEEZING
RICORRENTERICORRENTE
Michele Miraglia del GiudiceServizio Asma e Fisiopatologia Respiratoria Infantile
“MAURIZIO MIRAGLIA del GIUDICE”Dipartimento di Pediatria
Seconda Università di Napoli

PREVENZIONE DEL PREVENZIONE DEL WHEEZING WHEEZING
RICORRENTERICORRENTE
Chi è il bambino con wheezing ricorrente?

Che cosa è il Che cosa è il wheezingwheezing??
Il wheezing è il “sibilo”prodotto dalle turbolenze dell’aria che passa attraverso vie aeree ristrette.
....èè anatomicamente anatomicamente favorito nel bambino favorito nel bambino dal ridotto calibro dal ridotto calibro delle vie aeree e dalla delle vie aeree e dalla maggiore maggiore collassabilitcollassabilitààdelle pareti bronchiali delle pareti bronchiali durante la fase durante la fase espiratoria.. espiratoria..

Rational approach to the wheezy infantNemr S. Eid- Paediatric Respiratory Reviews 2004; 5: S77–S79
Cause di wheezing durante l’infanzia
INFIAMMAZIONI (asma, fibrosi cistica, displasia broncopolmonare)INFEZIONI (bronchiolite, pertosse, chlamydia),MALFORMAZIONI (anello vascolare, anomalie delle vie aeree, cisti broncogeniche) COMPRESSIONI ESTRINSECHE O INTRINSECHE(corpo estraneo, linfoadenopatia)REFLUSSO GASTROESOFAGEOPATOLOGIE EXTRATORACICHE

dal punto di vista clinico...dal punto di vista clinico...
Annals of Allergy. 1987;59: 334Annals of Allergy. 1987;59: 334--335 e 373335 e 373--375375
Stridore inspiratorio
Si
No Wheezing Espiratorio
1)Anello vascolare2)Tracheomalacia3)Anomalie laringee
o tracheali
Vomito
GER1)Fibrosi cistica2)Asma3)BPD4)Anomalie cardiovascolario bronchiali
Infezioniricorrenti:
1) Immunodeficit2) Sindrome
delle cigliaimmobili
++++++
Wheezing e Wheezing e asmaasma nell’infanzianell’infanziaPe
rcen
tuale
di p
azien
ti
60 -
50 -
40 -
30 -
20 -
10 -
0
51.5 %
Assenza
di
respiro
sibilan
te
15 %
Respiro
sibilan
te ad
insorgenza
tardiv
a:
3-6 an
ni13.7 %
*Resp
irosib
ilante
persiste
nte: 1-6
anni
19.8 %
Respiro
sibilan
te
transi
torio:
0-3 an
ni
*
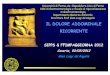
1246 neonati sono stati seguiti per 6 anni in unostudio prospettico. Martinez NEJM 1995; 332:133

Development of wheezing disorders and asthmain preschool childrenMartinez F. Pediatrics 2002; 109: 362-367
1246 1246 neonatineonati seguitiseguiti per 11 per 11 annianni in in unouno studio studio prospetticoprospettico

Lung function (V´maxFRC) at infancy and 6 years of age expressed in Z-scores by wheezing group: never wheeze; transient early wheeze;
late onset wheeze; persistent wheeze

Development of wheezing disorders and asthmain preschool childrenMartinez F. Pediatrics 2002; 109: 362-367
FATTORI DI RISCHIO:Vie aeree ristrette
PrematuritàFumo materno durante la gravidanza e esposizione postnataleal fumo passivo maternoScolarizzazione precoce
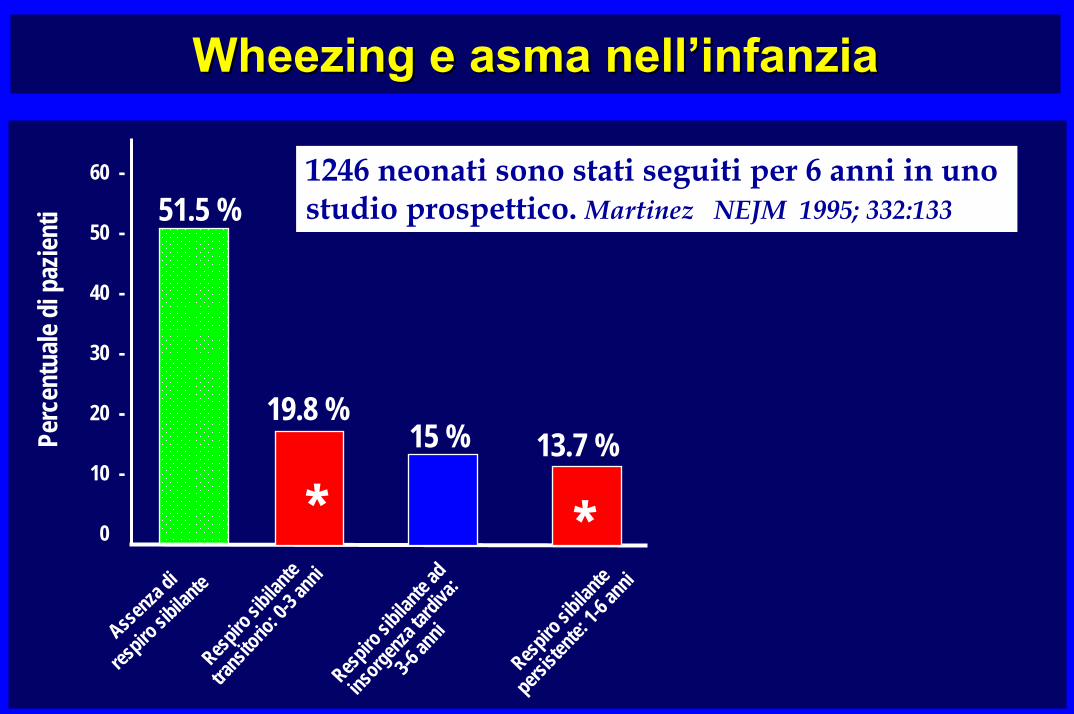
Increased incidence of asthma in children of smoking mothers Martinez F. Pediatrics 2002; 89: 21-26
*P<0.01*P<0.01
I nati da madri che hanno fumato in gravidanza almeno 10 sigarette al giorno sviluppano asma in modo significativamente maggiore rispetto ai figli di madri che hanno fumato meno o per nulla.Il fumo paterno è ininfluente.
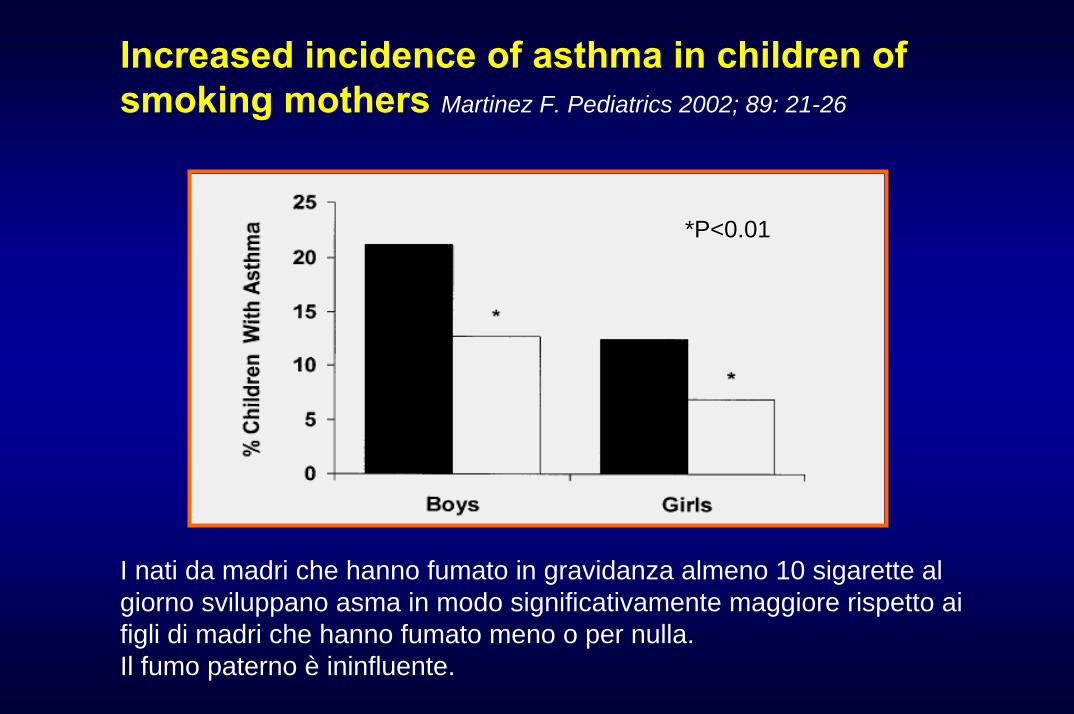
The The effecteffect of of maternalmaternal smoking on the smoking on the incidenceincidence of of asthmaasthma or or wheezingwheezing
StrachanStrachan D. D. etet Al.Al.ThoraxThorax 1998, 53, 742 1998, 53, 742

ExposureExposure toto siblingssiblings and day care and day care duringduring infancyinfancy and and subsequentsubsequent developmentdevelopment of of asthmaasthma and and frequentfrequent wheezewheeze. .
Ball TM. N Ball TM. N EnglEngl J J MedMed 2000;343:5382000;343:538--4343

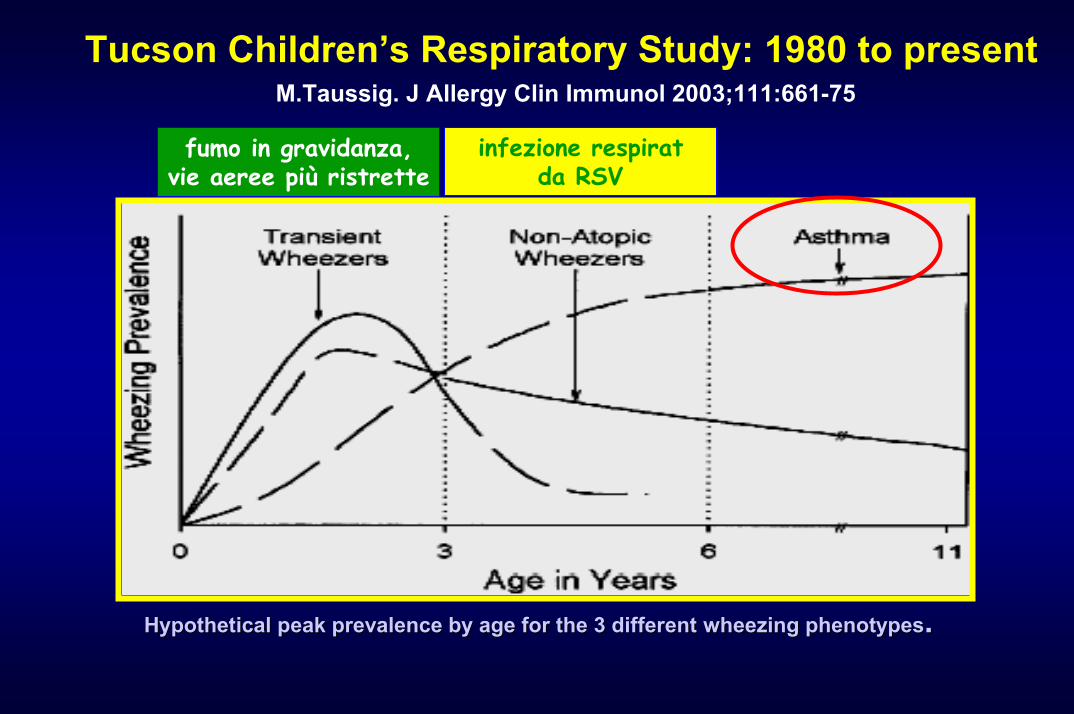
Tucson Children’s Respiratory Study: 1980 to presentM.Taussig. J Allergy Clin Immunol 2003;111:661-75
infezioni respiratorie virali (RSV),chlamydia
Vie aeree ristrettePrematurità , Scolarizzazione Fumo materno
HypotheticalHypothetical peak peak prevalenceprevalence byby ageage forfor the 3 the 3 differentdifferent wheezingwheezing phenotypesphenotypes. .

Kneyber MCJ et al. – Acta Paediatr., 2000, 89,654
RSV bronchiolitis and recurrent wheezing

Neuro inflammatory interactions and neural remodelling in RSV-infected airway da Piedimonte G. 2002
NeuroNeuro inflammatory interactions and neural inflammatory interactions and neural remodellingremodelling in RSVin RSV--infected airway infected airway dada PiedimontePiedimonte G. 2002G. 2002
RSVRSV EPITELIUMEPITELIUM
NNeurotrophineurotrophin nervenerve GGrowthrowth FFactoractor
NK 1 receptorsNK 1 receptors
T cellsT cells PMNsPMNs VesselsVessels Mast cellsMast cells
CytokinesCytokines ChemotaxisChemotaxis EdemaEdema LTsLTs
IRRITANTIRRITANTALLERGENSALLERGENSMEDIATORSMEDIATORS
SUBSTANCE PSUBSTANCE P
SENSORY NERVESSENSORY NERVES
inflammation

The risk of frequent and infrequent wheeze in children who had mild-moderate RSV LRTI The risk of frequent and infrequent wheeze in children who had mild-moderate RSV LRTI
Stein LT. Lancet 1999
Age 6 Age 8 Age 11 Age 13
4
3
2
1
0
infrequent wheezefrequent wheeze
***
***
*** **
* NS
*** p < 0,001 ** p < 0,01 * p < 0,05
Odd
s R
atio
ns (
95%
CI)
Children with a history of RSV infection had significantly lower FEV1, partly reversible by bronchodilator administration, at age 11 years.

Differences in total serum IgE (A) and peripheral blood (PB)eosinophil levels (B) during and after the first LRI for children grouped
as to their subsequent age 6 wheezing patterns.
TheseThese data data supportsupport the the possibilitypossibility thatthat childrenchildrendestineddestined toto developdevelop persistentpersistent wheezingwheezing are are
alreadyalready ““programmedprogrammed” ” immunologicallyimmunologically beforebeforethe first LRI the first LRI toto respondrespond differentlydifferently toto a a respiratoryrespiratory
viralviral infectioninfection..

Sustained increases in numbers of pulmonary dendritic cellsafter respiratory syncytial virus infection
Marc Beyer-J Allergy Clin Immunol 2004;113:127-33
RSV infection results insustained increases in numbersof mature dendritic cells in thelung. These might well contribute tothe development of intenseairway inflammation and airwayhyperresponsiveness after RSVInfection and to enhancement ofsubsequent responses toallergen exposure.
In contrast, in influenza A virus infectionnumbers of pulmonary DCs were elevated during
the acute phase of infection only,and sensitizationand airway inflammation were induced exclusively if
allergen was administered during this phase.

VIRUS INFECTIONS, WHEEZE AND ASTHMAVIRUS INFECTIONS, WHEEZE AND ASTHMA
PAEDIATRIC RESPIRATORY REVIEWS (2003) 4, 184PAEDIATRIC RESPIRATORY REVIEWS (2003) 4, 184––192192
Tucson Children’s Respiratory Study: 1980 to presentM.Taussig. J Allergy Clin Immunol 2003;111:661-75
fumo in gravidanza,vie aeree più ristrette
infezione respiratda RSV
HypotheticalHypothetical peak peak prevalenceprevalence byby ageage forfor the 3 the 3 differentdifferent wheezingwheezing phenotypesphenotypes. .

Lung function (V´maxFRC) at infancy and 6 years of age expressed in Z-scores by wheezing group: never wheeze; transient early wheeze;
late onset wheeze; persistent wheeze

Tucson Children’s Respiratory Study: 1980 to presentM.Taussig. J Allergy Clin Immunol 2003;111:661-75
fumo in gravidanza,vie aeree più ristrette
infezione respiratda RSV
presenza di atopia
HypotheticalHypothetical peak peak prevalenceprevalence byby ageage forfor the 3 the 3 differentdifferent wheezingwheezing phenotypesphenotypes. .

CRITERI Minor1) Rinite allergica2) Respiro sibilante
(in assenza di infezionirespiratorie)
3) Eosinofilia (> 4%)
59% rischio di asma
76% sviluppo di asma
DUE
Major1) Asma familiare2) Eczema3) Atopia
+oppure
ALMENO UNO
• respiro sibilanteprecoce
• respiro sibilanteprecoce frequente
(>3 episodi nell’anno precedente)
CRITERI DI RISCHIO DI ASMA Castro-Rodriguez et al., AJRCCM 2000CRITERI DI CRITERI DI RISCHIO DI ASMARISCHIO DI ASMA CastroCastro--Rodriguez et al., AJRCCM 2000Rodriguez et al., AJRCCM 2000

PREVENZIONE DEL PREVENZIONE DEL WHEEZING WHEEZING
RICORRENTERICORRENTE
Chi è il b. con wheezing ricorrente?La prevenzione non La prevenzione non farmacologicafarmacologica

STRATEGIES FOR PREVENTING WHEEZING AND ASTHMA IN SMALL CHILDREN. Wickman Allergy 2003;58:742STRATEGIES FOR PREVENTING WHEEZING AND ASTHMA IN SMALL CHILDREN. Wickman Allergy 2003;58:742
RECURRENT WHEEZING AT 2 YRSRECURRENT WHEEZING AT 2 YRS
living according to guidelinesYES NO*
30-
20-
10-
0
12,6%24,1%
• Birth cohort 4089 ch• Families who lived according the Swedishprimary preventionguidelines:
1.breastfeeding2.no tabacco smoke3.good ventilation &
reduced dampness
*NO=exposed to >2 risk factors

STRATEGIES FOR PREVENTING WHEEZING AND ASTHMA IN SMALL CHILDREN. Wickman Allergy 2003;58:742STRATEGIES FOR PREVENTING WHEEZING AND ASTHMA IN SMALL CHILDREN. Wickman Allergy 2003;58:742
YES NO*
20-
10-
06,8%
17,9%
ASTHMA AT AGE 2ASTHMA AT AGE 2
living according to guidelines
• Birth cohort 4089 ch• Families who lived according the Swedishprimary preventionguidelines:
1.breastfeeding2.no tabacco smoke3.good ventilation &
reduced dampness
*NO=exposed to >2 risk factors

STRATEGIES FOR PREVENTING WHEEZING AND ASTHMA IN SMALL CHILDREN. Wickman Allergy 2003;58:742STRATEGIES FOR PREVENTING WHEEZING AND ASTHMA IN SMALL CHILDREN. Wickman Allergy 2003;58:742
REDUCTION OF ASTHMA AT 2 YRS
living according to guidelinesYES NO*
30-
20-
10-
05,3%
10,5% 9,1%
27,3%
YES NO*
HEREDITY FOR ALLERGIC DISEASESHEREDITY FOR ALLERGIC DISEASESnegative positivenegative positive
• Birth cohort 4089 ch• Families who lived according the Swedishprimary preventionguidelines:
1.breastfeeding2.no tabacco smoke3.good ventilation &
reduced dampness
*NO=exposed to >2 risk factors

Eighteen-month outcomes of house dust mite avoidance and dietary fatty acid modification in the Childhood AsthmaPrevention Study (CAPS) Mihrshahi JACI 2003;111:162
Eighteen-month outcomes of house dust mite avoidance and dietary fatty acid modification in the Childhood AsthmaPrevention Study (CAPS) Mihrshahi JACI 2003;111:162
• 616 pregnant women were randomized to an HDM avoidance intervention, comprising the use of impermeable mattress covers and an acaricide or control and the use of an oil supplement, margarines, and cooking oils containing high levels of omega-3 fatty acids or control.
• Atopic status was measured by skin prick testing. Symptoms, diagnoses, and medication histories were elicited by means of parental interviews.
• Outcomes were assessed at 18 months.
•• 616 pregnant women616 pregnant women were randomized to an HDM avoidance intervention, comprising the use of impermeable mattress covers and an acaricide or control and the use of an oil supplement, margarines, and cooking oils containing high levels of omega-3 fatty acids or control.
•• AtopicAtopic statusstatus was measured by skin prick testing. Symptoms, diagnoses, and medication histories were elicited by means of parental interviews.
•• Outcomes were assessed at 18 Outcomes were assessed at 18 months.months.
% REDUCTION OF ANY WHEEZE IN OIL SUPPLEMENTEDOIL SUPPLEMENTED
0 –
10-
-9.8P =0.02

PREVENZIONE DEL PREVENZIONE DEL WHEEZING WHEEZING
RICORRENTERICORRENTE
Chi è il b. con wheezing ricorrente?La prevenzione non farmacologicaLa prevenzione La prevenzione farmacologicafarmacologica
antistaminiciantistaminici

CETIRIZINE IN THE PREVENTION OF ASTHMA IN CHILDREN WITH ATOPIC DERMATITIS Warner JO JACI 2001; 108: 929 CETIRIZINE IN THE PREVENTION OF ASTHMA IN CHILDREN WITH ATOPIC DERMATITIS Warner JO JACI 2001; 108: 929
.placebo .cetirizine1.0 -0.9 -0.8 -0.7 -0.6 -0.5 -0.4 -0.3 -0.2 -0.1 -Pr
obab
ility
ford
evel
opin
g
6 12 18 24 30 36treatment mo
.. . . . .. . . . . .
follow up mo
p=0.008
Risk of developing asthma in children with AD and ↑ IgE for grass pollen
(0.25 mg/Kg x2)

1.0 -0.9 -0.8 -0.7 -0.6 -0.5 -0.4 -0.3 -0.2 -0.1 -Pr
obab
ility
ford
evel
opin
g
6 12 18 24 30 36
. . . . . .
. . . . . .p=0.04
Risk of developing asthma in children with AD and ↑ IgE for mites.placebo .cetirizine (0.25 mg/Kg x2)
treatment mo follow up mo
CETIRIZINE IN THE PREVENTION OF ASTHMA IN CHILDREN WITH ATOPIC DERMATITIS Warner JO JACI 2001; 108: 929 CETIRIZINE IN THE PREVENTION OF ASTHMA IN CHILDREN WITH ATOPIC DERMATITIS Warner JO JACI 2001; 108: 929
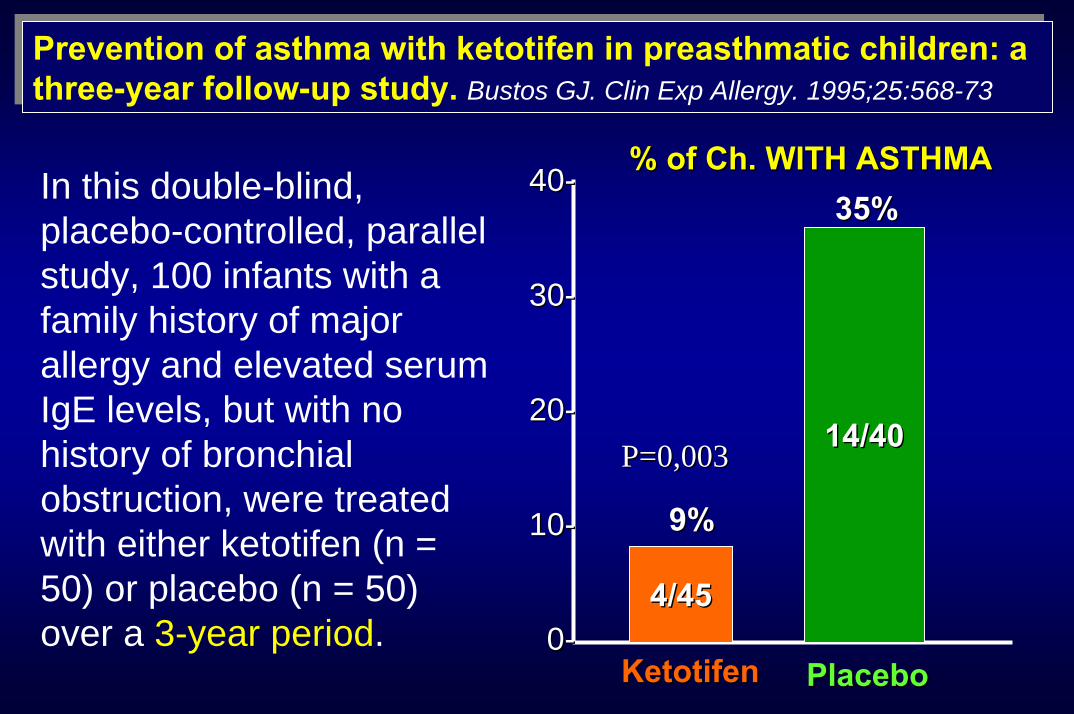
Prevention of asthma with ketotifen in preasthmatic children: a three-year follow-up study. Bustos GJ. Clin Exp Allergy. 1995;25:568-73Prevention of asthma with ketotifen in preasthmatic children: a three-year follow-up study. Bustos GJ. Clin Exp Allergy. 1995;25:568-73
4040--
3030--
2020--
1010--
00--4/454/45
14/4014/40
9%9%
35%35%
KetotifenKetotifen PlaceboPlacebo
P=0,003P=0,003
%% ofof ChCh. WITH ASTHMA. WITH ASTHMAIn this double-blind, placebo-controlled, parallel study, 100 infants with a family history of major allergy and elevated serum IgE levels, but with no history of bronchial obstruction, were treated with either ketotifen (n = 50) or placebo (n = 50) over a 3-year period.

PREVENZIONE DEL PREVENZIONE DEL WHEEZING WHEEZING
RICORRENTERICORRENTE
Chi è il b. con wheezing ricorrente?Quando iniziare la prevenzione?La prevenzione non farmacologicaLa prevenzione La prevenzione farmacologicafarmacologica
antistaminicicorticosteroidicorticosteroidi

Effectiveness of prophylactic inhaled steroids inchildhood asthma: A systemic review of the literature Calpin JACI 1997; 100: 452
Effectiveness of prophylactic inhaled steroids inEffectiveness of prophylactic inhaled steroids inchildhood asthma: A systemic review of the literature childhood asthma: A systemic review of the literature CalpinCalpin JACI 1997; 100: 452JACI 1997; 100: 452
0-10 --20 --30 --40 --50 --60 --70 -
40 -30 -20 -10 -0
From 1966 to 199694 studies on ICS vs placebo
- 50 %- 37 %
- 68 %
Systemic steroidsSymptoms β2 use
Mean increasein PEFR (L)
38 (L)

Persistent wheezing in infants with an Persistent wheezing in infants with an atopicatopic tendency tendency responds to inhaled responds to inhaled fluticasonefluticasone.. ChavasseChavasse Arch Arch DisDis Child. 2001;85:143Child. 2001;85:143--8.8.

BronchoalveolarBronchoalveolar lavagelavage findings suggest two different forms of findings suggest two different forms of childhood asthma. childhood asthma. Stevenson ECStevenson EC. . ClinClin ExpExp AllergyAllergy 1997;27:10271997;27:1027--3535
This study has investigated the cellular constituents of BAL fluid in 95 children with a history of atopic asthma, non-asthmatic atopic children or viral associated wheeze.RESULTS: during relatively asymptomatic periods there is on-going airways inflammation, as demonstrated by eosinophiland mast cell recruitment, in children with asthma and atopy but not in children with viral associated wheeze or atopy alone.
This study has investigated This study has investigated the cellular constituents of the cellular constituents of BAL fluid in 95 children with a BAL fluid in 95 children with a history of history of atopicatopic asthma, nonasthma, non--asthmatic asthmatic atopicatopic children or children or viral associated wheeze.viral associated wheeze.RESULTSRESULTS: during relatively : during relatively asymptomatic periods there asymptomatic periods there is onis on--going airways going airways inflammation, as inflammation, as demonstrated by demonstrated by eosinophileosinophiland mast cell recruitment, in and mast cell recruitment, in children with asthma and children with asthma and atopyatopy but not in children with but not in children with viral associated wheeze or viral associated wheeze or atopyatopy alone.alone. Eosinophil (P < or = 0.005) and mast cell (P < or = 0.05) numbers
were significantly elevated in the group with atopic asthma

Inhaled steroids for Inhaled steroids for epidosodicepidosodicviral wheeze of childhoodviral wheeze of childhoodMcKean The Cochrane Library, Issue 1, 2001
DatiDati di 5 trials di 5 trials cliniciclinici in in etàetà pediatricapediatrica
OORR
AlteAlte dosidosial al bisognobisogno di CSI di CSI (1.6 (1.6 --2.25 mg/die) 2.25 mg/die)
11
0.530.530.820.82
BasseBasse dosidosi di di mantenimentomantenimento di CSI di CSI
(400 µg/die) (400 µg/die)
• Alte dosi al bisogno di CSI rappresentano una strategiaparzialmente efficace per la terapia del wheezing virale di tipo episodico-lieve
• Non c’è alcunadimostrazione di efficaciadella terapia di mantenimentocon CSI a basse dosi
Richiesta di steroidi per os
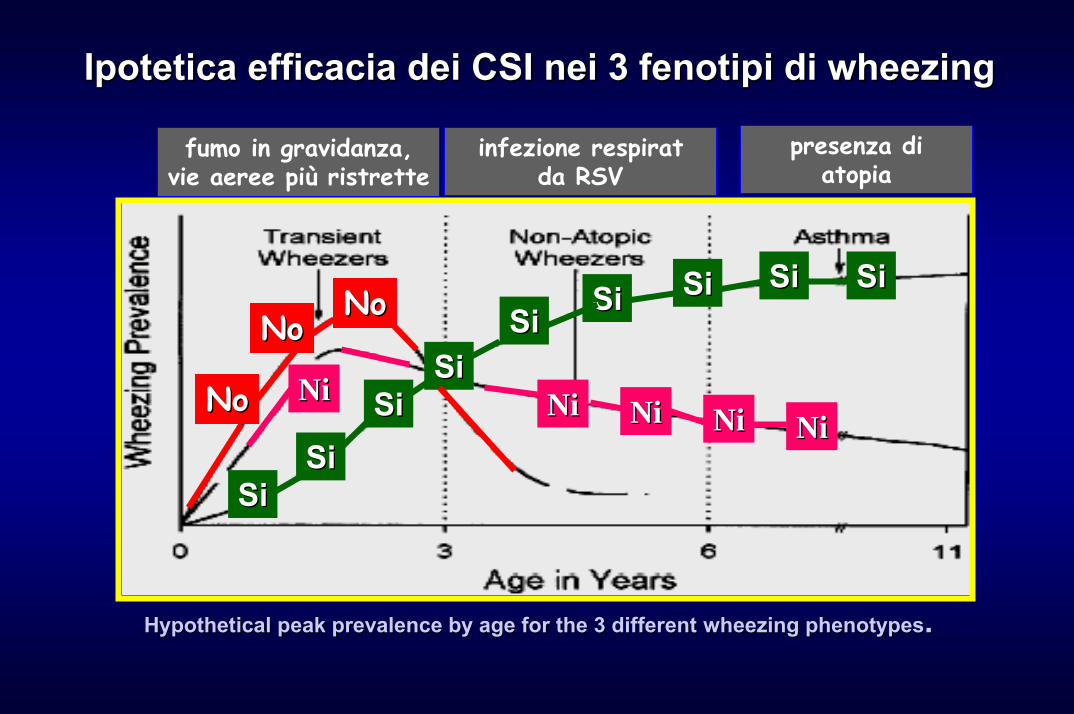
Ipotetica efficacia dei CSI nei 3 fenotipi di Ipotetica efficacia dei CSI nei 3 fenotipi di wheezingwheezing
fumo in gravidanza,vie aeree più ristrette
infezione respiratda RSV
presenza di atopia
SiSiSiSi
SiSiSiSi
SiSi SiSi SiSi SiSi SiSi
NoNo
NoNoNoNo
NiNiNiNiNiNi NiNi NiNi
HypotheticalHypothetical peak peak prevalenceprevalence byby ageage forfor the 3 the 3 differentdifferent wheezingwheezing phenotypesphenotypes. .

PREVENZIONE DEL PREVENZIONE DEL WHEEZING WHEEZING
RICORRENTERICORRENTE
Chi è il b. con wheezing ricorrente?Quando iniziare la prevenzione?La prevenzione non farmacologicaLa prevenzione La prevenzione farmacologicafarmacologica
AntistaminiciCorticosteroidiCorticosteroidiAntileucotrieni Antileucotrieni

IncreasedIncreased production of IFNproduction of IFN-- γγ and and cysteinylcysteinylleukotrienesleukotrienes in in virusvirus--inducedinduced wheezingwheezing
SchaikSchaik etet al J ALLERGY CLIN IMMUNOL 2000; 103:630al J ALLERGY CLIN IMMUNOL 2000; 103:630--66
• Concentrazione dei cisteinilleucotrieni nelle secrezioni respiratorie di soggetti con wheezing virus indotto e nei soggetti controllo
• Le colonne rappresentano il valore medio della concentrazione dei leucotrieni in soggetti con infezioni delle vie aeree superiori , un episodio primario di bronchiolite o wheezing ricorrente

IncreasedIncreased production of IFNproduction of IFN-- γγ and and cysteinylcysteinylleukotrienesleukotrienes in in virusvirus--inducedinduced wheezingwheezing
SchaikSchaik etet al al -- J ALLERGY CLIN IMMUNOL 2000; 103:630J ALLERGY CLIN IMMUNOL 2000; 103:630--66
• Correlazione tra laconcentrazione di IFN-γ ecisteinil LT nelle secrezioni respiratorie di soggetti con wheezing virus indotto
• La concentrazione di IFN- γpuò aumentare il rilascio dicisteinil LT
• l’ IFN- γ attiva e prolunga la sopravvivenza degli eosinofili e aumenta il rilascio di LT da queste cellule

Montelukast nella Prevenzione degli Episodi di Riacutizzazione Asmatica in Bambini dai 2 ai 5 Anni
Valutare l’effetto del trattamento per 12 mesi con Montelukast, rispetto al placebo, sulla frequenza degli episodi di riacutizzazione in bambini asmatici di età compresa tra 2 e 5 anni
Bisgaard H. et al. Montelukast reduces asthma exacerbations in 2- to 5- year-old children with intermittent asthma. Am J Respir Crit Care Med, 2005; 171: 315-22.

Episodio di Riacutizzazione Asmatica
Definito come: • 3 giorni consecutivi con:
- Sintomi diurni (punteggio medio delle risposte a 4 domande giornaliere sui sintomi diurni ≥1 ogni giorno) e- ≥ 2 trattamenti con beta-agonisti ogni giornooppure
• Ricorso ai corticosteroidi per via inalatoria (≥3 giorni consecutivi) o ai corticosteroidi per via orale (≥1 giorno)oppure
• Ospedalizzazione per asmaBisgaard H. et al. Montelukast reduces asthma exacerbations in 2- to 5- year-old children with intermittent asthma. Am J Respir Crit Care Med, 2005; 171: 315-22.

Criteri di Inclusione• Età 2–5 anni• Prestudio
– Asma intermittente scatenato da infezione delle vie aeree superiori (anche raffreddore comune)
– Assenza di sintomi e di utilizzo di beta agonisti nei periodi intercorrenti
Bisgaard H. et al. Montelukast reduces asthma exacerbations in 2- to 5- year-old children with intermittent asthma. Am J Respir Crit Care Med, 2005; 171: 315-22.

Disegno dello StudioBisgaard H. et al. Montelukast reduces asthma exacerbations in 2- to 5- year-old children with intermittent asthma.
Am J Respir Crit Care Med, 2005; 171:315-22.
Periodo I Periodo II
Placebo(run-in)
Placebo
Montelukast 4 mg (o 5 mg a seconda dell’età)*
Settimana 48
Visita 7 8
36
1 2 3 4 5 6
241680-2-3
*Se i pazienti compivano il 6° anno di età durante lo studio veniva loro somministrato Montelukast 5 mg (compresse masticabili)

Frequenza delle RiacutizzazioniBisgaard H. et al. Montelukast reduces asthma exacerbations in 2- to 5- year-old children with intermittent asthma.
Am J Respir Crit Care Med, 2005; 171:315-22.
p≤0.0013
2.34
1.60
32%
2Frequenza diriacutizzazioni (numero/anno)
1
0Montelukast 4 mg
(n=265)Placebo (n=257)

Tempo di Comparsa della Prima RiacutizzazioneBisgaard H. et al. Montelukast reduces asthma exacerbations in 2- to 5- year-old children with intermittent asthma.
Am J Respir Crit Care Med, 2005; 171:315-22.
• Tempo medio alla prima riacutizzazione: 206 giorni con Montelukast, 147 giorni con il placebo
0 2 4 6 8 10 120
20
40
60
80
100
12
Montelukast (n=265)Placebo (n=257)
p=0.024
Percentualedi pazienti senzariacutizzazioni
MesiStima di Kaplan-Meier. Analisi Intention-to-Treat

Ricorso ai Corticosteroidi (Inalatori+Orali)Bisgaard H. et al. Montelukast reduces asthma exacerbations in 2- to 5- year-old children with intermittent asthma.
Am J Respir Crit Care Med, 2005; 171:315-22.
1.19
0.660.53
1.74
1.10
0.64
0.0
0.5
1.0
1.5
2.0
2.5 Montelukast 4 mg (n=265)Placebo (n=257)
p=0.024
32% p=0.027Ciclidi trattamentocon corticosteroidi
40%
p=0.368
Totali(via inalatoria e via orale)
Via Inalatoria Via Orale

Stagionalità delle Riacutizzazioni
% Pazienti con riacutizzazione
Inverno Primavera Estate AutunnoMontelukast 4 mg Placebo
Mesi (Emisfero Nord)GEN FEB MAR APR MAG GIU LUG AGO SET OTT NOV DIC
5
10
0
15
Bisgaard H. et al. Montelukast reduces asthma exacerbations in 2- to 5- year-old children with intermittent asthma.Am J Respir Crit Care Med, 2005; 171:315-22.
A Randomized Trial of Montelukast in Respiratory Syncytial Virus Postbronchiolitis
BisgaardBisgaard -- AmAm J J RespirRespir CritCrit Care Care MedMed Vol 2003;167: 379Vol 2003;167: 379––383383
•• I bambini spesso sviluppano I bambini spesso sviluppano iperreattivitàiperreattivitàdelle vie aeree dopo bronchiolite da virus delle vie aeree dopo bronchiolite da virus respiratorio respiratorio sincizialesinciziale (RSV)(RSV)
•• I CysteinylI Cysteinyl--leukotrieni (cysleukotrieni (cys--LT) sonoLT) sonorilasciati durante l’infezione da RSV e rilasciati durante l’infezione da RSV e possono contribuire all’infiammazionepossono contribuire all’infiammazione

A Randomized Trial of Montelukast in Respiratory Syncytial Virus Postbronchiolitis
BisgaardBisgaard -- AmAm J J RespirRespir CritCrit Care Care MedMed Vol 2003;167: 379Vol 2003;167: 379––383383
• 130 bambini tra 3 e 36 mesiospedalizzati con bronchioliteacuta da RSV sono statirandomizzati in uno studio indoppio cieco
• 2 gruppi in terapia per 28 giorni entro una settimana dalla scomparsa deisintomi:
- montelukast 5mg - placebo
Il trattamento con Il trattamento con montelukastmontelukastriduce i sintomi polmonari dovutiriduce i sintomi polmonari dovuti
alla alla bronchiolitebronchiolite da RSVda RSV

MONTELUKAST Riduzione degli eosinofili nell’espettorato indotto
Variazione % degli eosinofili nell’espettorato indotto
-50-40-30-20-100
102030
Placebo
Montelukast
*
% variazionedal
basale
* p=0.026, basato sul modello ANCOVA, confrontato con il placebo
Pizzichini et al. Eur Resp Journal 1999;14:12-18
PREVENZIONE DEL PREVENZIONE DEL WHEEZING WHEEZING
RICORRENTERICORRENTE
Chi è il b. con wheezing ricorrente?Quando iniziare la prevenzione?La prevenzione non farmacologicaLa prevenzione farmacologica
AntistaminiciCorticosteroidiAntileucotrieni
La prevenzione del La prevenzione del wheezingwheezing: quando iniziare?: quando iniziare?

100 –
90 –
80 –
70 –
60 –
50 –
40 –
30 –
20 –
10 –
0
% dei soggetti all’età di 26 anni
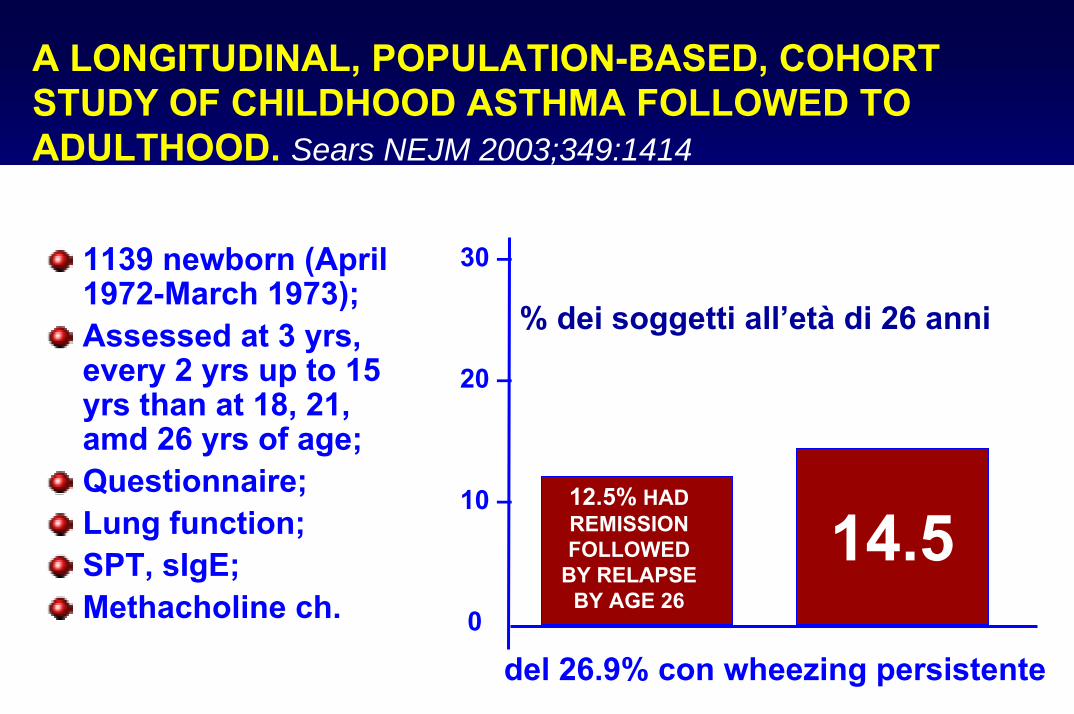
A LONGITUDINAL, POPULATION-BASED, COHORT STUDY OF CHILDHOOD ASTHMA FOLLOWED TO ADULTHOOD.Sears NEJM 2003;349:1414
1139 newborn (April1972-March 1973);Assessed at 3 yrs, every 2 yrs up to 15 yrs than at 18, 21, amd 26 yrs of age;Questionnaire;Lung function;SPT, sIgE;Methacholine ch.
WHEEZING:
72.651.4
26.9Almeno 1 volta
Più di1 volta
persistente
30 –
20 –
10 –
0
A LONGITUDINAL, POPULATION-BASED, COHORT STUDY OF CHILDHOOD ASTHMA FOLLOWED TO ADULTHOOD. Sears NEJM 2003;349:1414
1139 newborn (April1972-March 1973);Assessed at 3 yrs, every 2 yrs up to 15 yrs than at 18, 21, amd 26 yrs of age;Questionnaire;Lung function;SPT, sIgE;Methacholine ch.
del 26.9% con wheezing persistente
14.512.5% HAD REMISSION FOLLOWED
BY RELAPSE BY AGE 26
% dei soggetti all’età di 26 anni

A LONGITUDINAL, POPULATION-BASED COHORT STUDY OF CHILDHOOD ASTHMA FOLLOWED TO ADULTHOOD Sears NEJM 2003; 349: 1414
Age at assessment (yr)
9 11 13 15 18 2621Classification
Persistent wheezing from 9 yrs of age
Persistent wheezing from onset
Remission
Relapse
Intermittent wheezing
Transient wheezing
No wheezing ever
Patterns of wheezing (shaded bars) in childhood reported by study members or their parents, illustrating definitions of persistent wheezing, remission, relapse, intermittent wheezing, transient wheezing, and no wheezing ever.
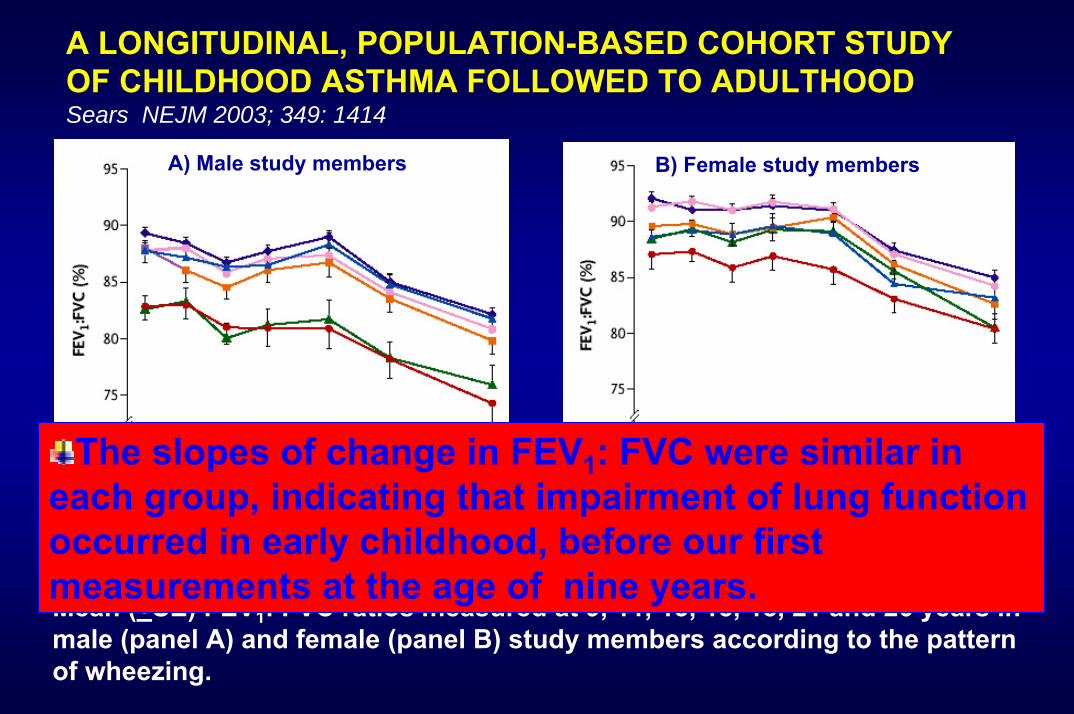
A LONGITUDINAL, POPULATION-BASED COHORT STUDY OF CHILDHOOD ASTHMA FOLLOWED TO ADULTHOOD Sears NEJM 2003; 349: 1414
A) Male study members B) Female study members
Mean (+SE) FEV1: FVC ratios measured at 9, 11, 13, 15, 18, 21 and 26 years in male (panel A) and female (panel B) study members according to the pattern of wheezing.
The slopes of change in FEV1: FVC were similar in each group, indicating that impairment of lung function occurred in early childhood, before our first measurements at the age of nine years.

“Only the paediatrician has the possibility to cure the disease.”
Spahn JD. J All Clin Immunol 2002

Arrivederci alTHESIS 2005
New Europe Hotel15-17 dicembre 2005