Embed Size (px)
Citation preview
Primary or Secondary?
Drs. Siu Ngai Lau, A Tangg gRenal unit Department of Medicine & GeriatricsU it d Ch i ti H it lUnited Christian Hospital
Historyy
• Madam MH Chan , F/36, working as a nurse , , gbefore
• NSND
• PMH : – Hepatits B carrier with liver biopsy done in PWH in
19961996– Liver biopsy diagnosis: chronic hepatitis, mild activity
(mild chronic active hepatitis), HBV related– Fu private with blood tests and USG abdomen
Historyy
• December 2006December, 2006
Sh t d t AED ith• She presented to AED with– Acute generalised edema x 3/7– Significant weight gain (18 lb in 1 week)– No skin rash– No joint pain – No systemic symptomsNo systemic symptoms
Physical Examinationy
• Urine : albumin 4+ RBC moderate• Urine : albumin 4+, RBC moderate, WBC –
• Afebrile, No P/J, JVP not elevated• BP 105 / 74 mHg pulse 80 bpmBP 105 / 74 mHg, pulse 80 bpm• No stigmata of chronic liver disease• Facial puffiness, ankle edema 2+, • No lymphoadenopathyNo lymphoadenopathy• Chest, CVS : unremarkable• Abdomen : Ascite +, no organomegaly
Baseline Investigations
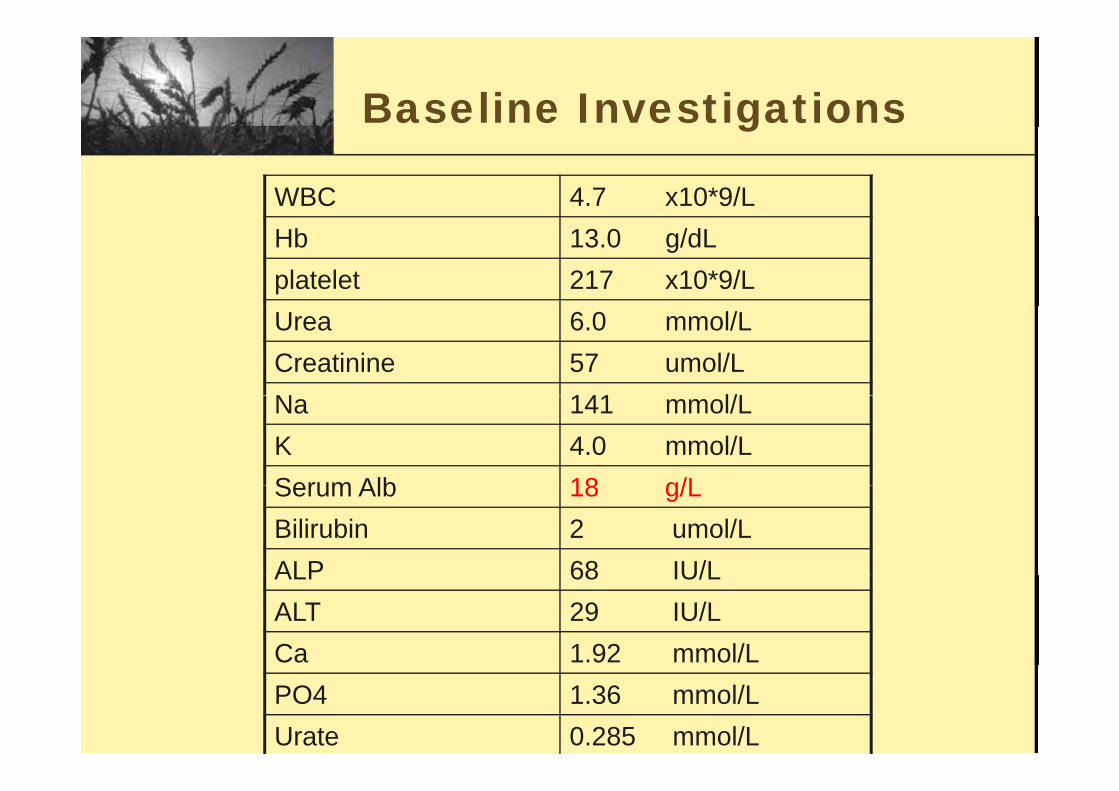
WBC 4.7 x10*9/L
g
Hb 13.0 g/dLplatelet 217 x10*9/LUrea 6.0 mmol/LCreatinine 57 umol/LN 141 l/LNa 141 mmol/LK 4.0 mmol/LSerum Alb 18 g/LSerum Alb 18 g/LBilirubin 2 umol/LALP 68 IU/LALP 68 IU/LALT 29 IU/LCa 1.92 mmol/LPO4 1.36 mmol/LUrate 0.285 mmol/L
Baseline Investigationsg
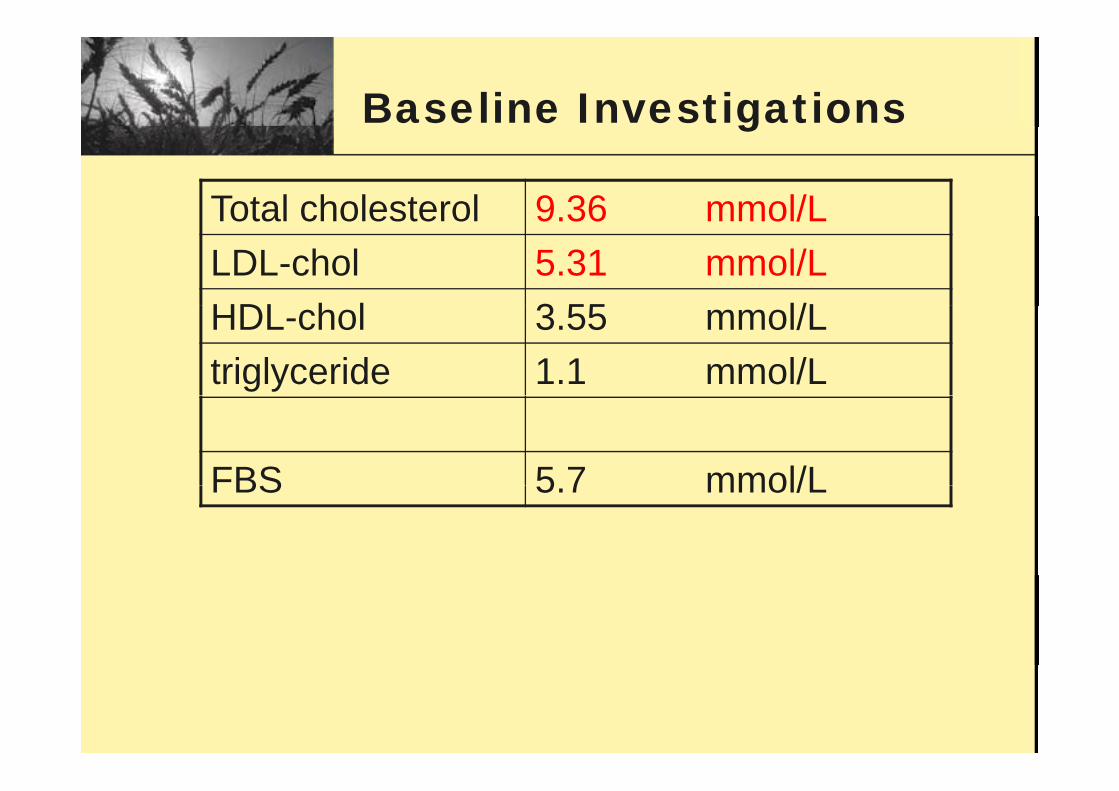
Total cholesterol 9 36 mmol/LTotal cholesterol 9.36 mmol/LLDL-chol 5.31 mmol/LHDL h l 3 55 l/LHDL-chol 3.55 mmol/Ltriglyceride 1.1 mmol/L
FBS 5 7 mmol/LFBS 5.7 mmol/L
Baseline Investigations
• 24hr urine protein 6.69 g/day
g
24hr urine protein 6.69 g/day
• CrCl 122 mL/min• CrCl 122 mL/min
MSU : mod RBC no dysmorphic RBC• MSU : mod RBC, no dysmorphic RBC
USG bd• USG abdomen : – Both kidney size 10cm with normal cortical
echogenicityechogenicity– The echogenicity of liver is within normal limit.
No focal hepatic lesion.No focal hepatic lesion.– Marked ascites
Further Historyy
• Denied taking any herbs / O-T-C drugs• Denied taking any herbs / O-T-C drugs
• No FHx of kidney disease/ neoplasm
Further Investigationsg
• HBsAg: +ve, HBeAg: +ve, Anti-HBe: -veg , g ,
• HBV DNA: > 10^6 copies/ml
• Anti-HCV: - ve
• Streptozyme : < 100 units
• VDRL: Non-reactive
• Anti-HIV : -ve
Further Investigationsg
• ANA : -ve
• Rheumatoid Factor : -ve
• C3/C4 : normal
• CRP: normal
• ESR: 61 mm/hr
• Serum and urine protein electrophoresis: no p pparaprotein
Summary
A hepatitis B carrier lady presented with full blown nephrotic syndromep y
Any Questions?
DDx of Nephrotic dsyndrome
• Glomerulonephritis secondary to InfectionGlomerulonephritis secondary to Infection – hepatitis B
• Primary GlomerulonephritisPrimary Glomerulonephritis • Drugs
– gold penicillamine captopril NSAID mercurygold, penicillamine, captopril, NSAID, mercury, chinese herbs
• Connective tissue disease – SLE
• Diabetes mellitus• Myeloma• AmyloidosisAmyloidosis
Next Step ?
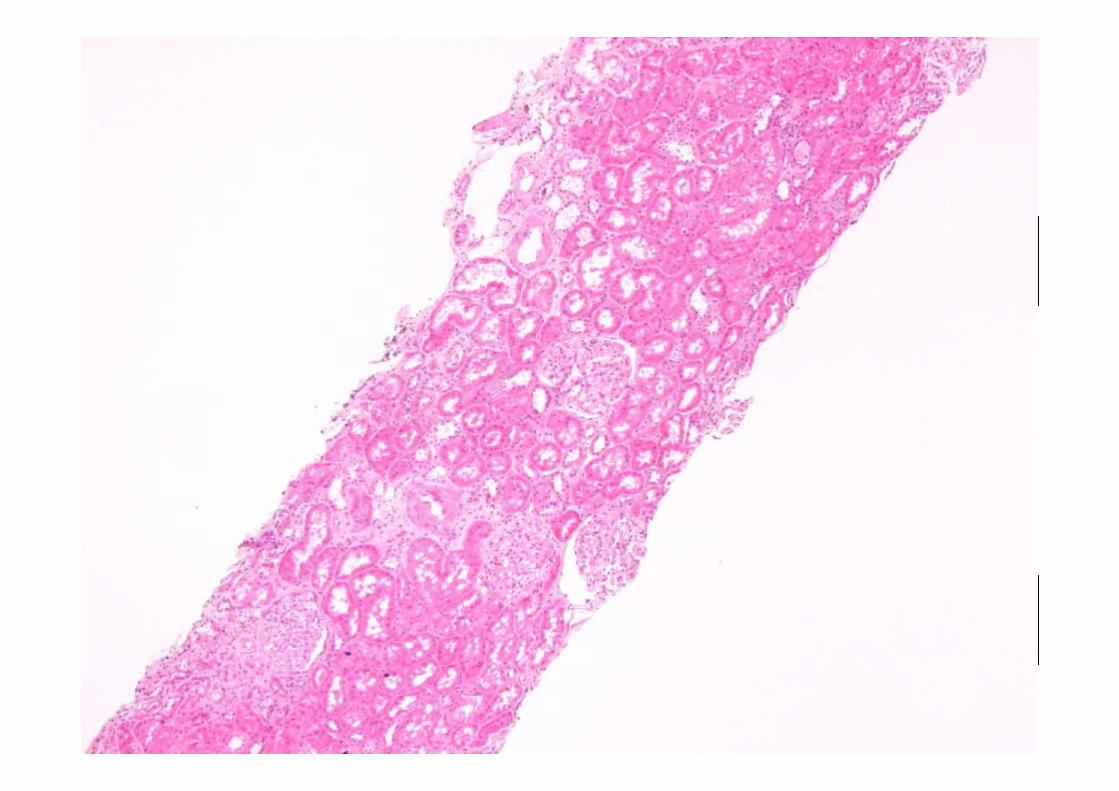
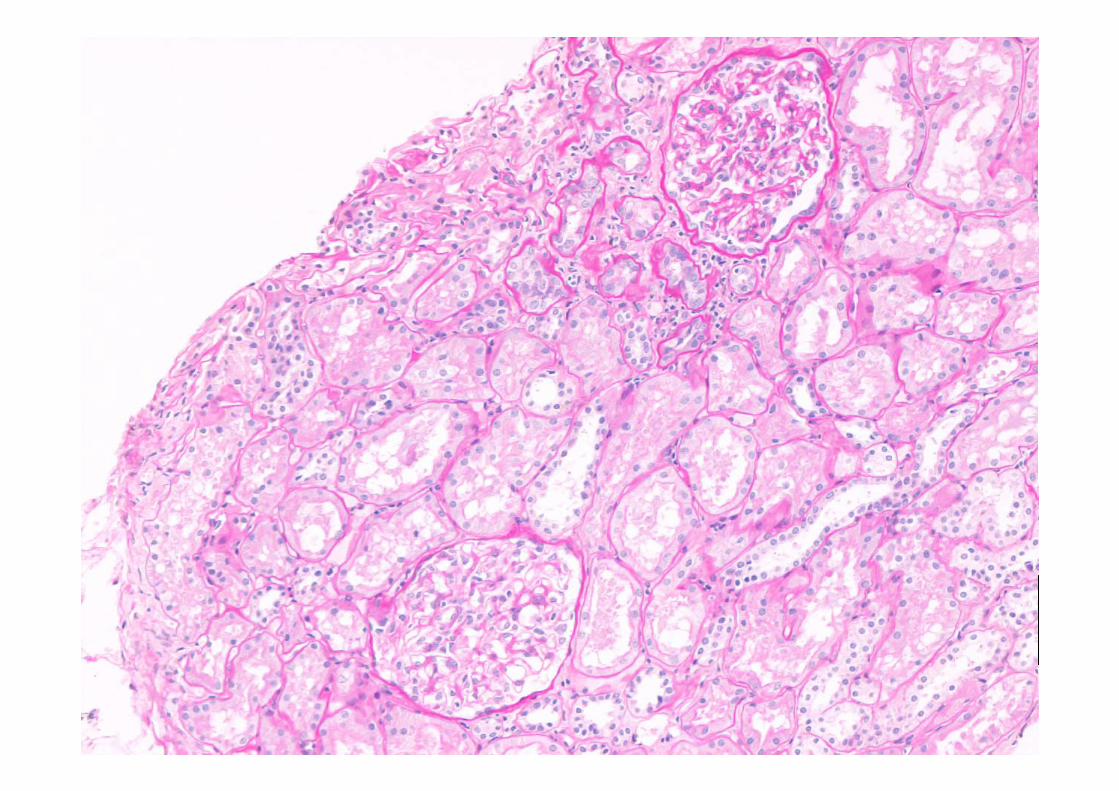
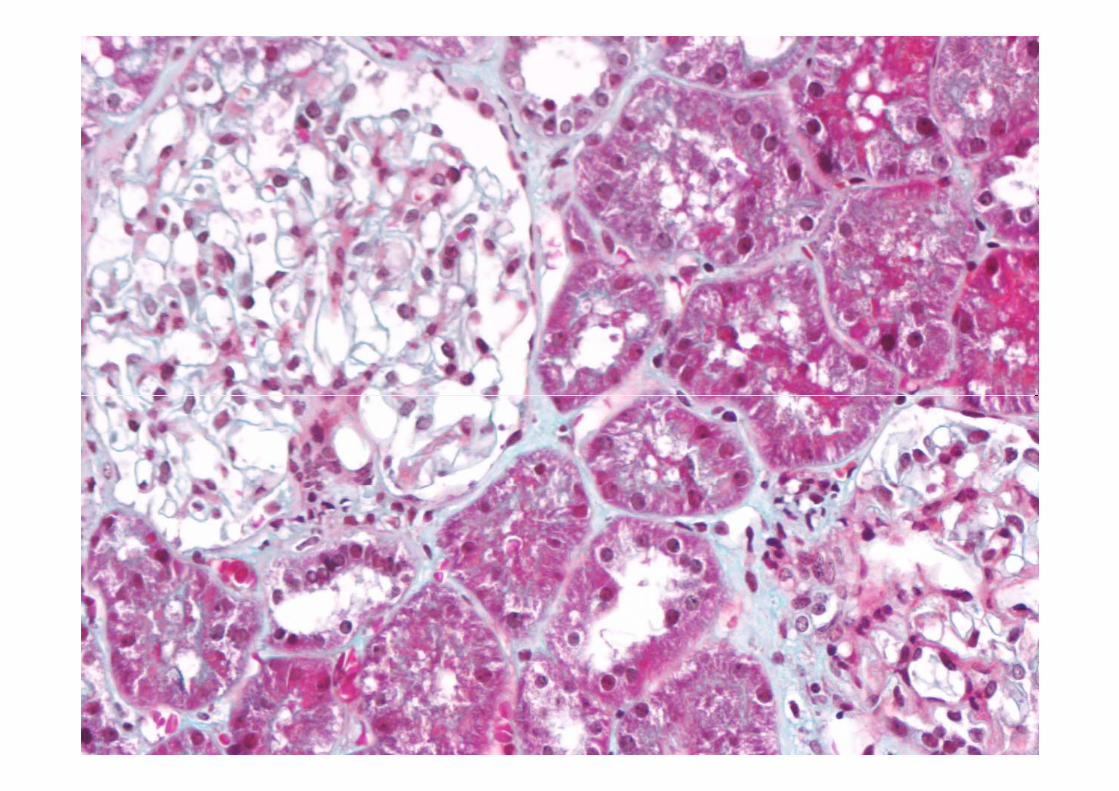
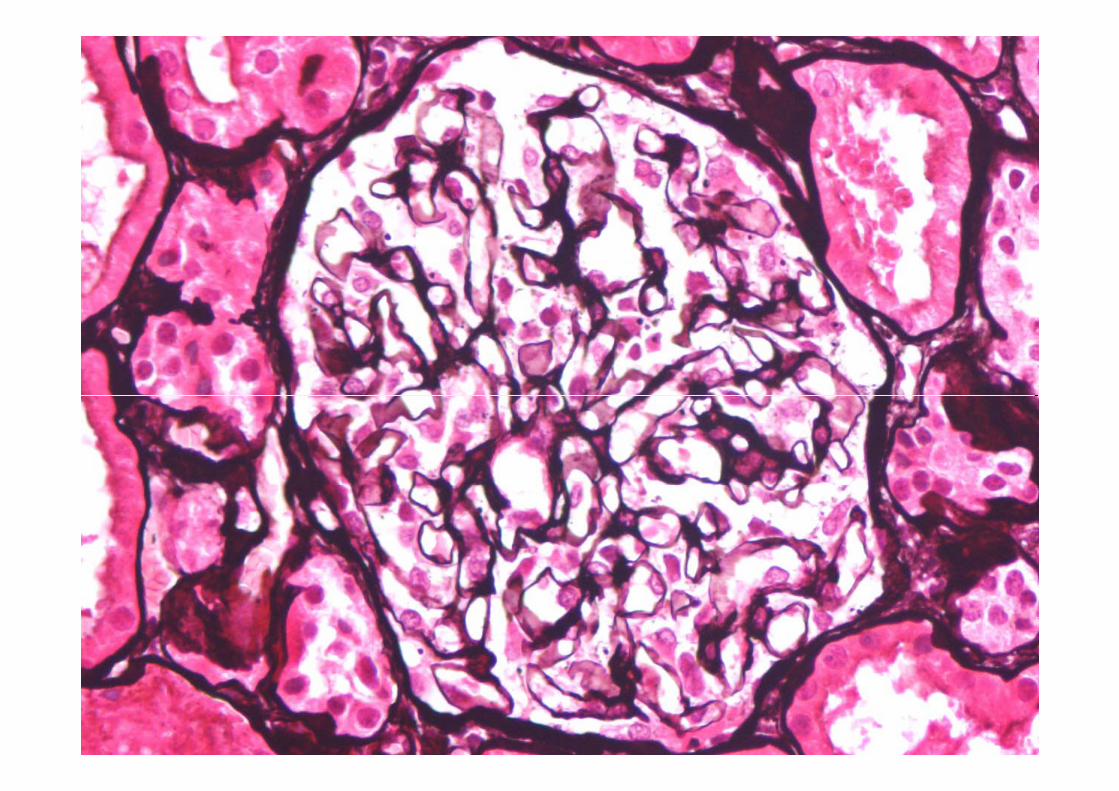
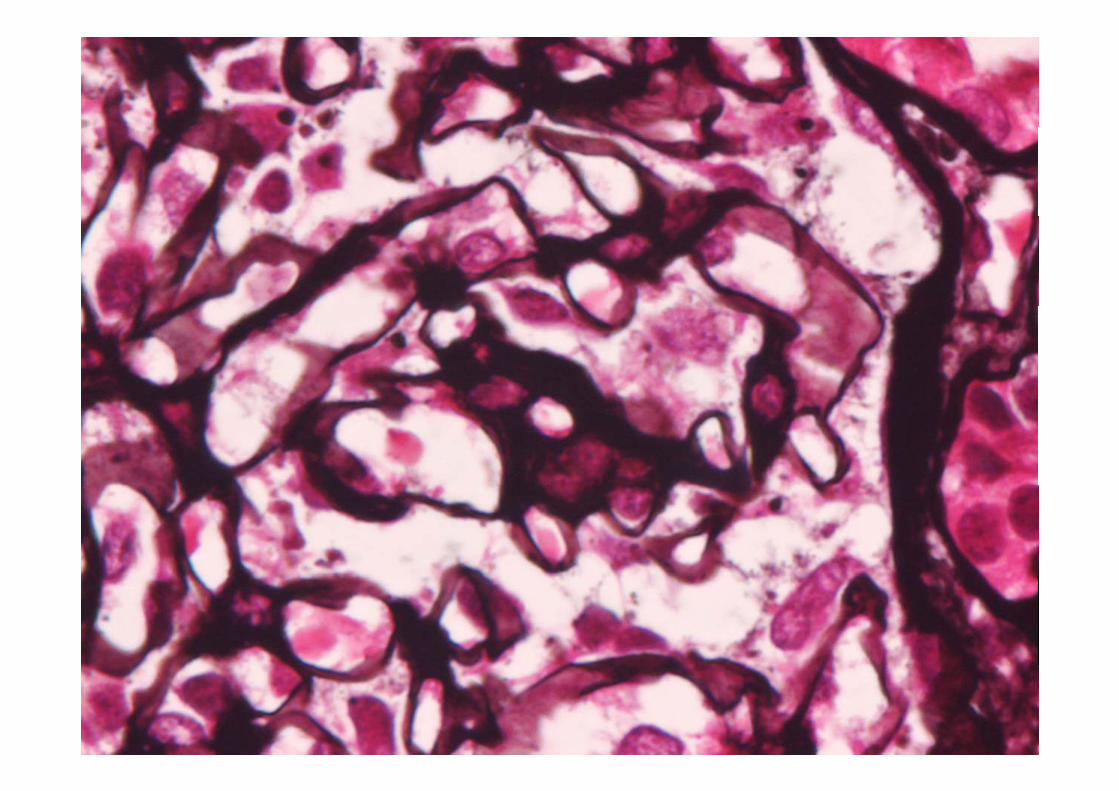
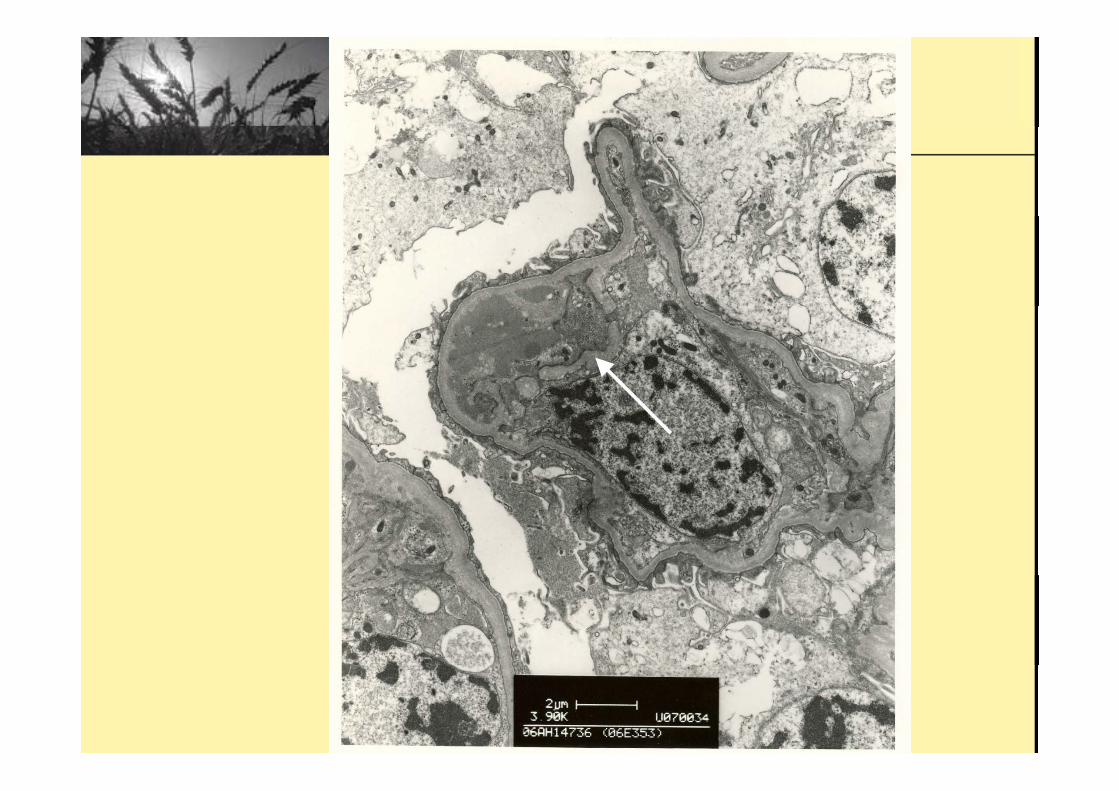
IgA nephropathy?
• IF:• IF: – mild segmental mesangial and
i l d iti f I A (+) d I Mparamesangial deposition of IgA (+), and IgM (++)
• EM: – Definite evidence of membranous GN is notDefinite evidence of membranous GN is not
seen. • Immunostains for HBsAg and HBeAg are• Immunostains for HBsAg and HBeAg are
negative.
IgAN + Hepatitis BIgAN + Hepatitis B
Vs Vs
HBV associated HBV-associated nephropathy
Consult Private N h l i tNephrologist
• Suggest to treat as nephrotic IgAN with• Suggest to treat as nephrotic IgAN with high dose steroid
• 86 patients• 6-month course of steroid treatement• Either supportive therapy or steroid treatment (IV y (
methylprednisolone)• 9/43 patients in steroid group and 14/43 in control group
reached endpoint (50% increase in plasma creatinine) by 5 year
Pozzi C et al. Lancet 1999
Our Treatment
• Started Lamivudine Dec 2006Started Lamivudine Dec., 2006 • Changed to Entecavir (SFI) Jan., 2007
• Rx: Zocor / Telmisartan
• 6 months later:• 6 months later: • Nephrotic syndrome in remission• Seroconversion of HBeAg
Progress (~ 1y later)g ( y )
• Dx: Hepatitis B virus associated• Dx: Hepatitis B virus associated nephropathy
• Plan for life long entecavir
• Patient self stopped Entecavir as desired f b bfor baby
Progress (~ 2 y later)g ( y )
• Nephrotic syndrome in remission• Nephrotic syndrome in remission • Albumin 49 g/L• Proteinuria < 0.06g/d• HBV DNA 1 4x10^4 cp/ml• HBV DNA 1.4x10^4 cp/ml• HBeAg –ve, anti- HBe +ve
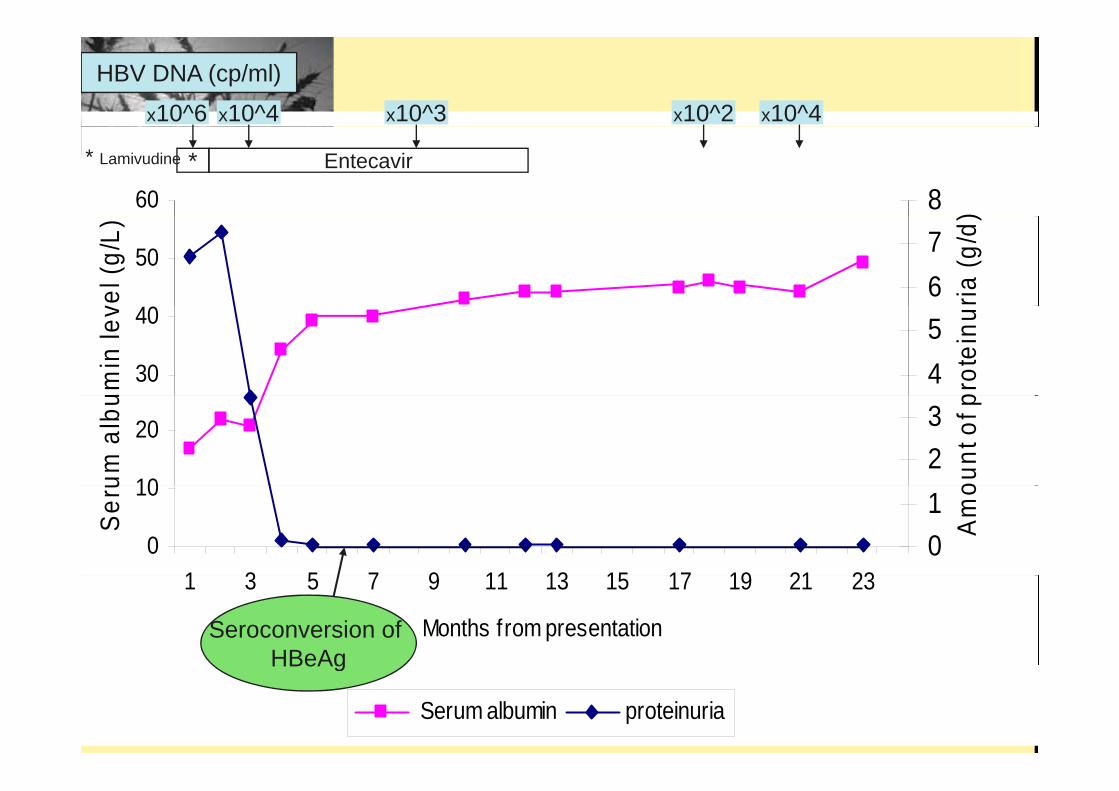
x10^6 x10^4 x10^3 x10^2 x10^4
HBV DNA (cp/ml)
60 8 )
* Entecavir* Lamivudine
50
vel (
g/L)
67
ria (g
/d)
30
40
umin
lev
45
prot
einu
10
20
um a
lbu
23
ount
of p
0
10
1 3 5 7 9 11 13 15 17 19 21 23
Ser
u
01
Am
o
1 3 5 7 9 11 13 15 17 19 21 23
Months from presentationSeroconversion of HBeAg
Serum albumin proteinuria
HBeAg
Summary
Young lady with HBV-associated HBV-associated nephropathy, treated
ith t iwith entecavir
Hepatitis B epat t sVirus-Associated NephropathyNephropathy
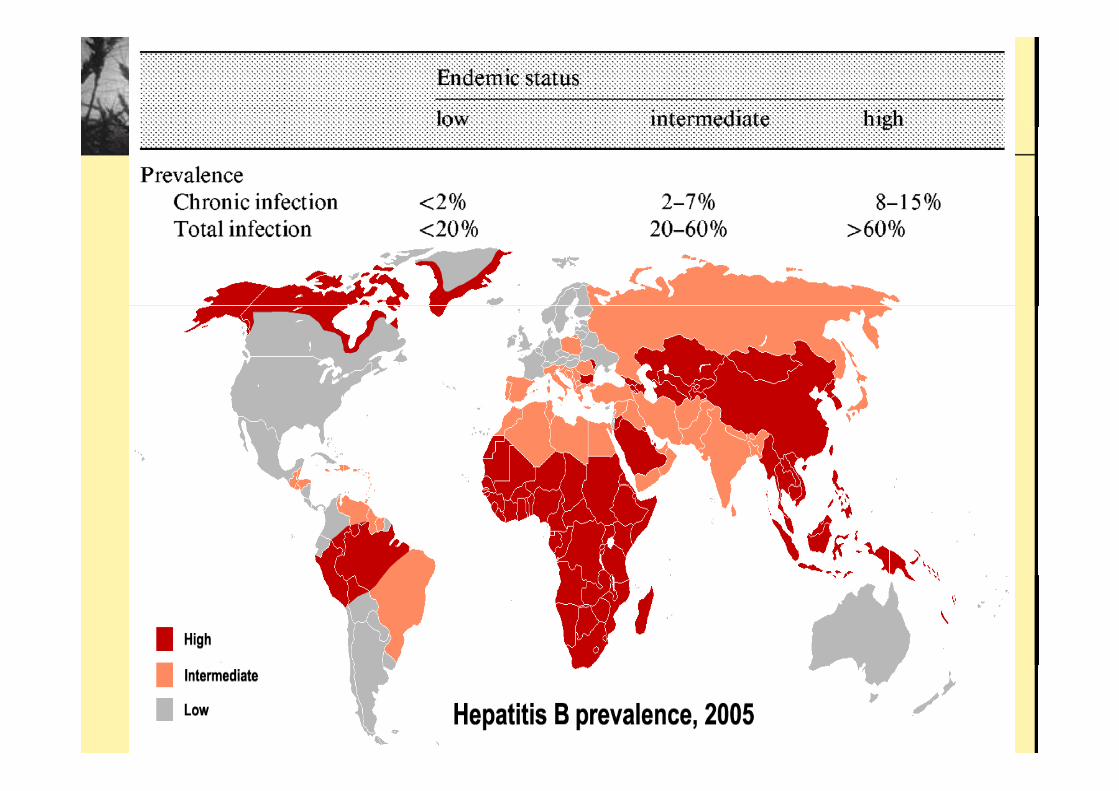
• ~ 350 – 400 million people worldwide are• 350 – 400 million people worldwide are infected with HBV
• The reported prevalence of HBV-The reported prevalence of HBVassociated nephropathy closely parallels to geographic patterns of prevalence ofto geographic patterns of prevalence of HBV
Extrahepatic if t timanifestation
• Prevalence: relatively low, but it can be associated with significant morbidit and e en mortalitsignificant morbidity and even mortality.
• Serum-sickness like "arthritis-dermatitis" prodrome f– is seen in approximately one third of patients acquiring HBV
– consisting of skin eruptions, urticaria and polyarthralgias or arthritis
• Skin rash• Skin rash• Arthritis • Arthralgia
Gl l h iti• Glomerulonephritis • Palpable purpura, papular acrodermatitis• Typical polyarteritis nodosa
– have persistent hepatitis B surface antigenemia (HBs Ag).
Gocke DJ. Am J Med Sci. 1975 Pyrsopoulos NT et al., Curr Gastroenterol Rep. 2001 y p , pHan SH.Clin Liver Dis. 2004.Baig S et al. J Coll Physician Surg Pak. 2008
Renal manifestation of hepatitis B virushepatitis B virus
Rajendra Bhimma et al. Am J of Nephrology 2004
Mechanisms of virus-i d d kid i jinduced kidney injury
• Glomerulonephritis (GN)Glomerulonephritis (GN)– Cytopathic effect of virus
Insitu immune complex formation– Insitu immune complex formation– Circulating immune complexes
• Tubulointerstitial nephritisp– Direct cytopathic effect– Mediated through host inflammatoryMediated through host inflammatory
response and/or viral proteinLai AS et al. Nat Clin Pract Nephrol 2006Faulhaber JR et al. Clin J Soc Nephrol 2007Alpers CE et al. Clin J Am Soc Nephrol 2007
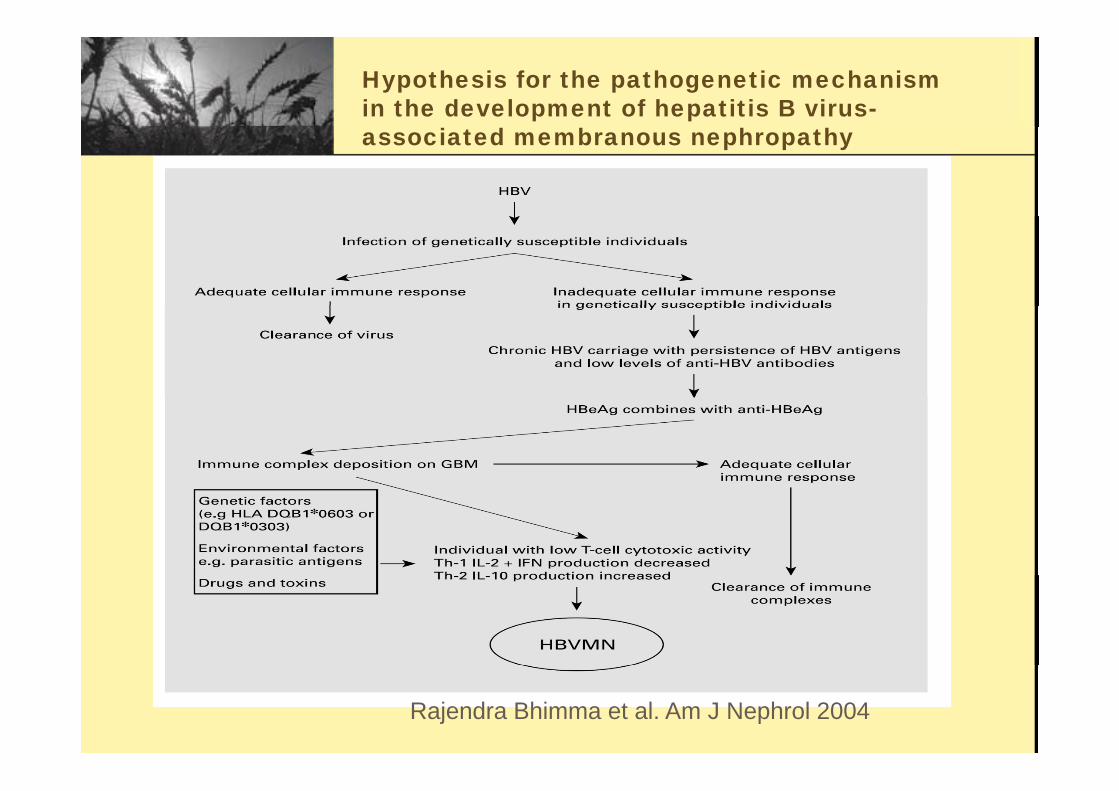
Hypothesis for the pathogenetic mechanism in the development of hepatitis B virus-associated membranous nephropathy
Rajendra Bhimma et al. Am J Nephrol 2004
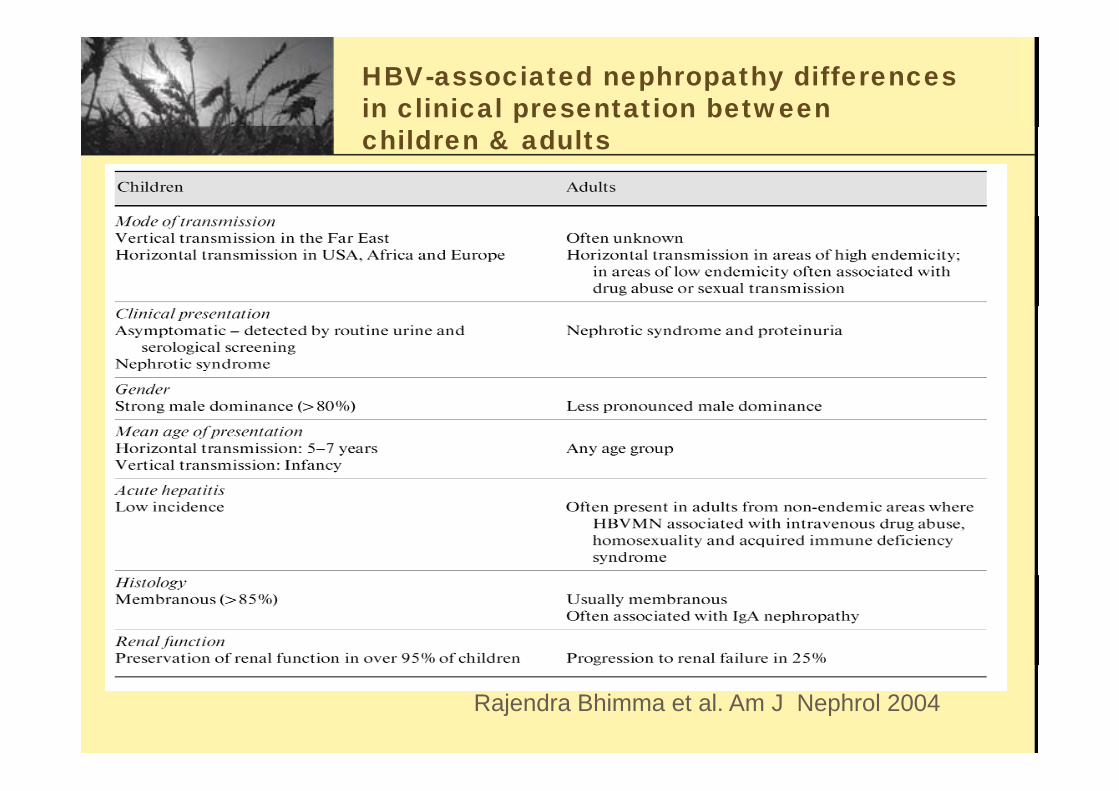
HBV-associated nephropathy differences in clinical presentation between children & adults
Rajendra Bhimma et al. Am J Nephrol 2004
Membranous N h thNephropathy
• Secondary MN was more common than• Secondary MN was more common than idiopathic in Chinese
• MN and most secondary MN diagnosesMN, and most secondary MN diagnoses were secondary to systemic lupus erythematosus and hepatitis B infectionerythematosus and hepatitis B infection.
Zeng CH et al. Am J Kidney Dis 2008
History of HBV associated nephropathyassociated nephropathy
• 1974: An immune complex type of1974: An immune complex type of glomerulonephritis may occur following hepatitis B virus infection, usually in association with chronic active hepatitis.
Brzosko WJ et al Lancet 1974
• 1979: Etiology of membranous nephropathy
Brzosko WJ et al. Lancet 1974Gocke DJ. Am J Med Sci. 1975
• 1979: Etiology of membranous nephropathy in children: Association between membranous nephropathy and hepatitis Bmembranous nephropathy and hepatitis B virus infection
Takekoshi. Hokkaido Igaku Zasshi. 1979 C h R t l N h l Di l T l t 1989Cahen R et al. Nephrol Dial Transplant. 1989
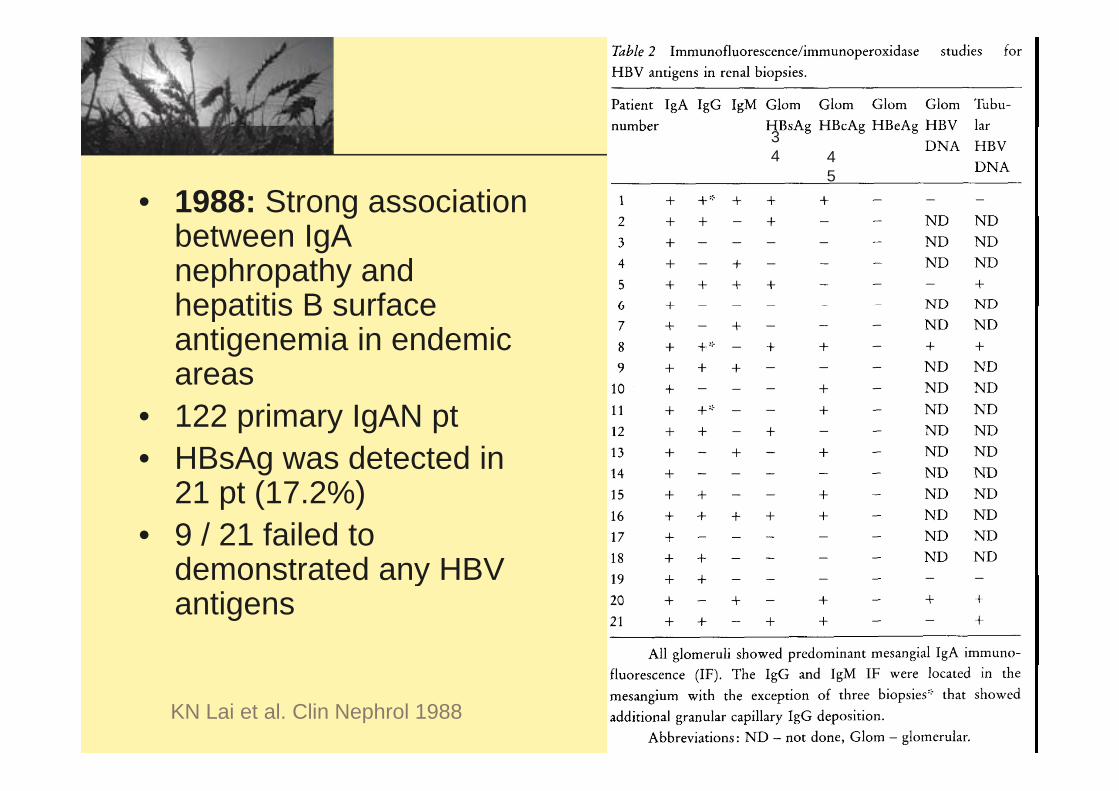
• 1988: Strong association
34 4
5
gbetween IgA nephropathy and hepatitis B surfacehepatitis B surface antigenemia in endemic areas
• 122 primary IgAN pt• HBsAg was detected in
21 t (17 2%)21 pt (17.2%)• 9 / 21 failed to
demonstrated any HBVdemonstrated any HBV antigens
KN Lai et al. Clin Nephrol 1988
• 1990: Membranoproliferative• 1990: Membranoproliferative glomerulonephritis with semilunar f d i d it f I Aforms and massive deposits of IgA associated with HBsAg
Toblli JE et al.,Medicina (B Aires).1990
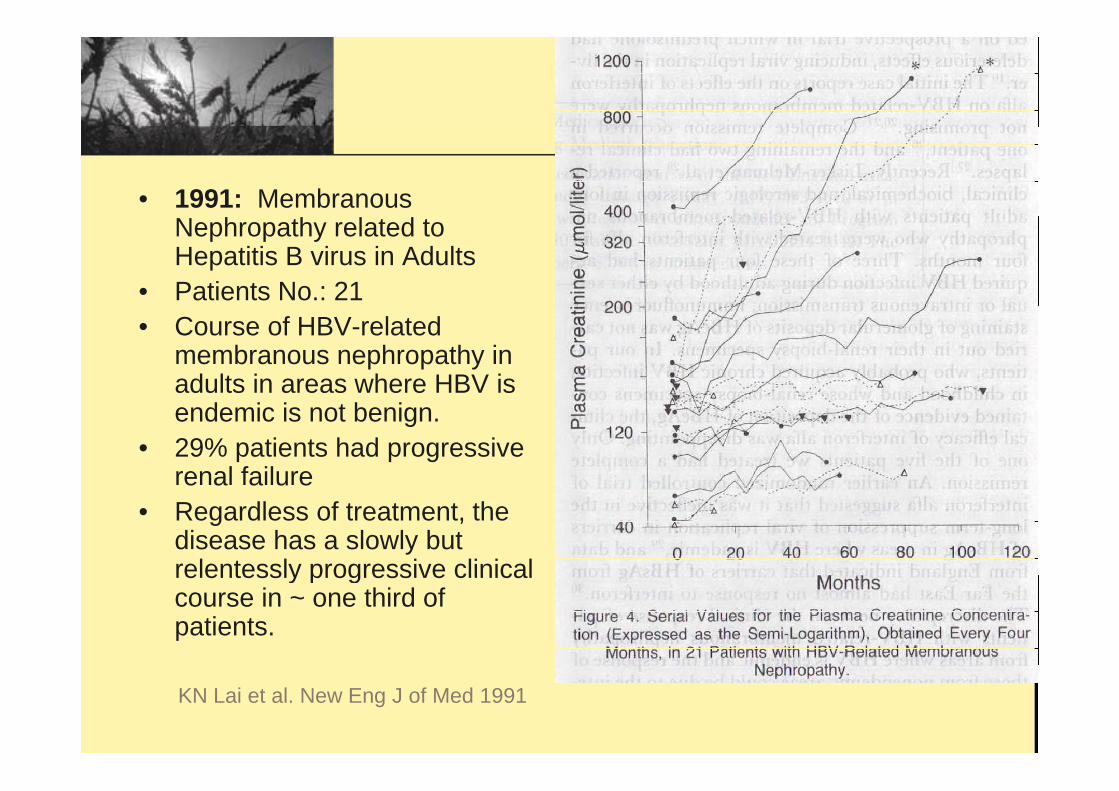
• 1991: Membranous Nephropathy related to Hepatitis B virus in Adults
• Patients No.: 21• Course of HBV-related
membranous nephropathy in adults in areas where HBV is endemic is not benign.
• 29% patients had progressive renal failure e a a u e
• Regardless of treatment, the disease has a slowly but relentessly progressive clinicalrelentessly progressive clinical course in ~ one third of patients.
KN Lai et al. New Eng J of Med 1991
• PAN is seen more frequently in North AmericanPAN is seen more frequently in North American and European patients and rarely in Asian patients.
• Acute renal failure in hepatitis B virus-related cute e a a u e epat t s us e atedmembranous nephropathy with mesangiocapillary transition and crescentic transformation, which partially responded to pulse methylprednisolone therapy, and
b tl d ft l hsubsequently recovered after plasma exchange.
Li PK et al Am J Kidne Dis 1992Li PK et al. Am J Kidney Dis. 1992
• Multiplication of HBV-DNA in the serum, the deposition u t p cat o o t e se u , t e depos t oof HBVAg in glomeruli of kidney increases, and the pathologic lesion aggravates, which have significant correlation.
– Higher the HBVDNA level, more the deposition of HBV antigens in glomeruli of kidney
Jiang W et al. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2008
Diagnosisg
• Establishing a direct causative relationshipEstablishing a direct causative relationship between a virus and a specific kidney disease often is problematic
• Persistence of circulating HBV or HBV DNAe s ste ce o c cu at g o
• Absence of other causative agentsAbsence of other causative agents
• Presence of HBV specific antigen(s) or viral• Presence of HBV-specific antigen(s) or viral genome in the glomerulus
Dx & Assessment of t t t tresponse to treatment
• LFT• LFT – ALT, GGT, bilirubin levels
• HBV serologiesHBV serologies – HBsAg, HBeAg, Anti-HBe, Anti-HBc
• Serum C3 & C4 levelsSerum C3 & C4 levels – low in 20-50% patients
Treatment
HBV-induced l l diglomerular disease
• Limited data (case series / uncontrolled observations)
IS + steroid / PE
• Little benefitLittle benefit.
I i th• Immunosuppressive therapy may – increase viral replication– possibly lead to exacerbation of chronic
hepatitis p• particularly when it is withdrawn
Lin CY et al. Kidney Int 1991 Lai KN et al. Nephron 1990Sayarlioglu, H et al. Ann Pharmacother 2005y g ,
Anti-viral agentsg
• Interferon alfa• Interferon alfa• Lamivudine• Adefovir• ? Entecavir• ? Entecavir
Adenine arabinoside d th i t tand thymic extract
• Patient No. 24• HBV MN patients who had previously received
corticosteroid treatment and had persistent proteinuria [heavy (22 of 24, 91.6%) or mild (2 of 24, 8.4%)].[heavy (22 of 24, 91.6%) or mild (2 of 24, 8.4%)].
• Treatment: combination therapy with adenine bi id f t k d th i t tarabinoside for two weeks and thymic extract
(Thymostimulin) for six months to decrease urine protein loss and obtain seroconversion.
• Results: only one case (4.2%) had heavy and two cases (8 4%) mild proteinuria;(8.4%) mild proteinuria;
Lin CY et al., Kidney Int. 1991
Antiviral agentg
• 1989:• 1989: • A 9-year-old boy with hepatitis B-
associated glomerulonephritis and nephrotic syndrome p y
• Treatment: antiviral combination therapy including interferon and acyclovirincluding interferon and acyclovir.
• Result: Improvement
De Man RA et al. J Hepatol. 1989
Interferon alfa
• The clinical response to therapy with• The clinical response to therapy with interferon alfa was disappointing;
• Only one of the five patients treated had a complete remission with seroconversion pto antibody to HBeAg.
Lai KN et al.N Engl J Med 1991
Interferon alfate e o a a
• Long-term remission in liver disease in 8• Long-term remission in liver disease in 8 of 15 patients with chronic hepatitis B and l l h itiglomerulonephritis.
• Significant improvement in markers of renal disease in the majority of patientsrenal disease in the majority of patients.
Conjeevaram HS et al. Gastroenterology 1995
Interferon alfate e o a a
• 4 8 months Interferon alfa• 4-8 months Interferon alfa therapy:py–sustained HBeAg clearance:38-80
%%–remission of proteinuria: 25-100%–remission of proteinuria: 25-100%
Lin CY et al Kidney Int 1995Lin CY et al. Kidney Int 1995Conjeevaram HS et al. Gastroenterology 19Chung DR et. Am J Nephrol. 1997Bhimma R et al.Pediatr Nephrol. 2002p
Interferon
• Interferon is less well tolerated but is more• Interferon is less well tolerated but is more likely to induce a prolonged remission.
• In younger patients without renalIn younger patients without renal impairment, a course of interferon, or pegylated interferon may be anpegylated interferon, may be an alternative.
Lamivudine
• 2003:• 2003: • HBV associated nephrotic syndrome:
resolution with oral lamivudine.Connor FL et al., Arch Dis Child. 2003Co o et a , c s C d 003
• Numerous case reports
Lamivudine
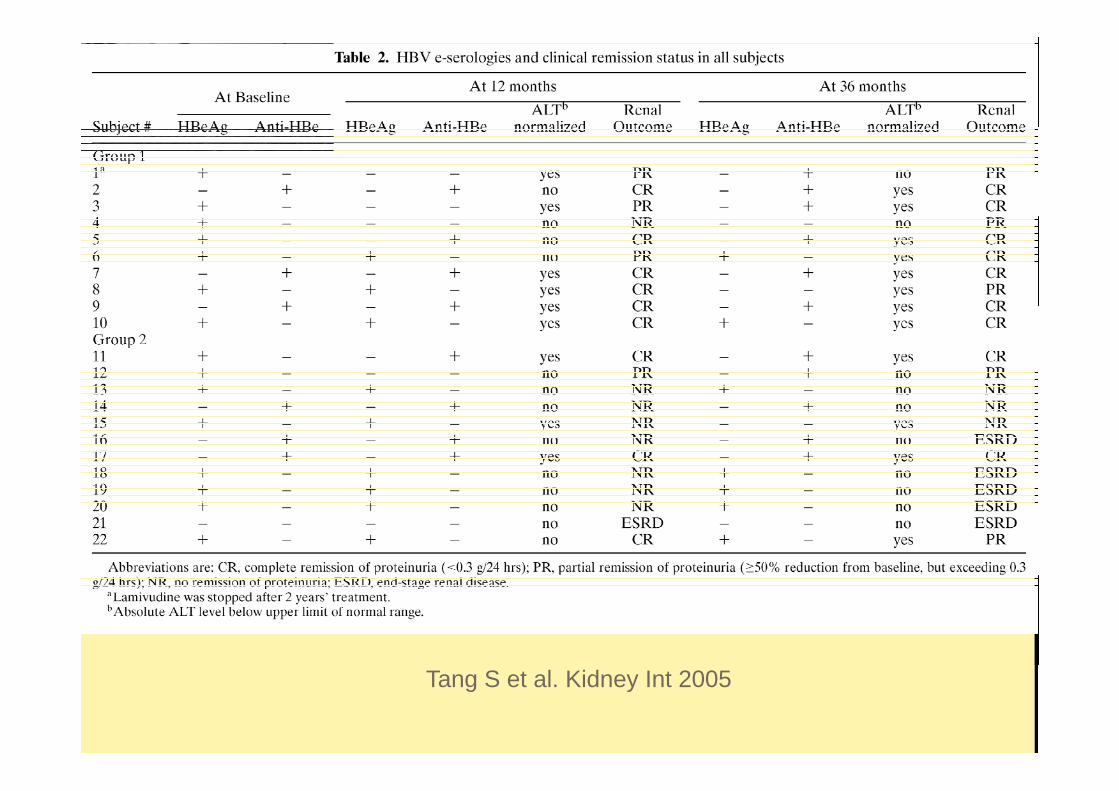
• Biopsy proven membranous nephropathy• Biopsy proven membranous nephropathy associated with HBV patient No. : 10
• Historic controls No: 12• QMH UCHQMH, UCH• Lamivudine was available in Hong Kong in
19981998
Tang S et al Kidney Int 2005Tang S et al. Kidney Int 2005
Tang S et al Kidney Int 2005Tang S et al. Kidney Int 2005
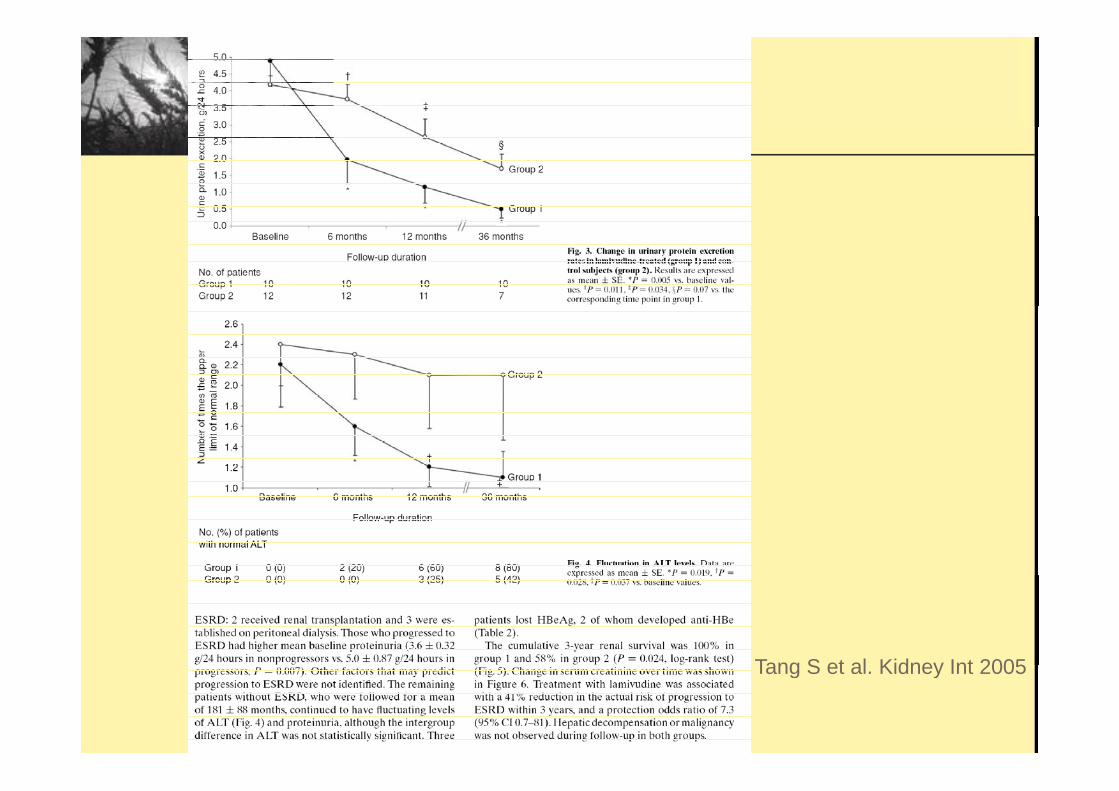
Tang S et al. Kidney Int 2005
Tang S et al. Kidney Int 2005g y
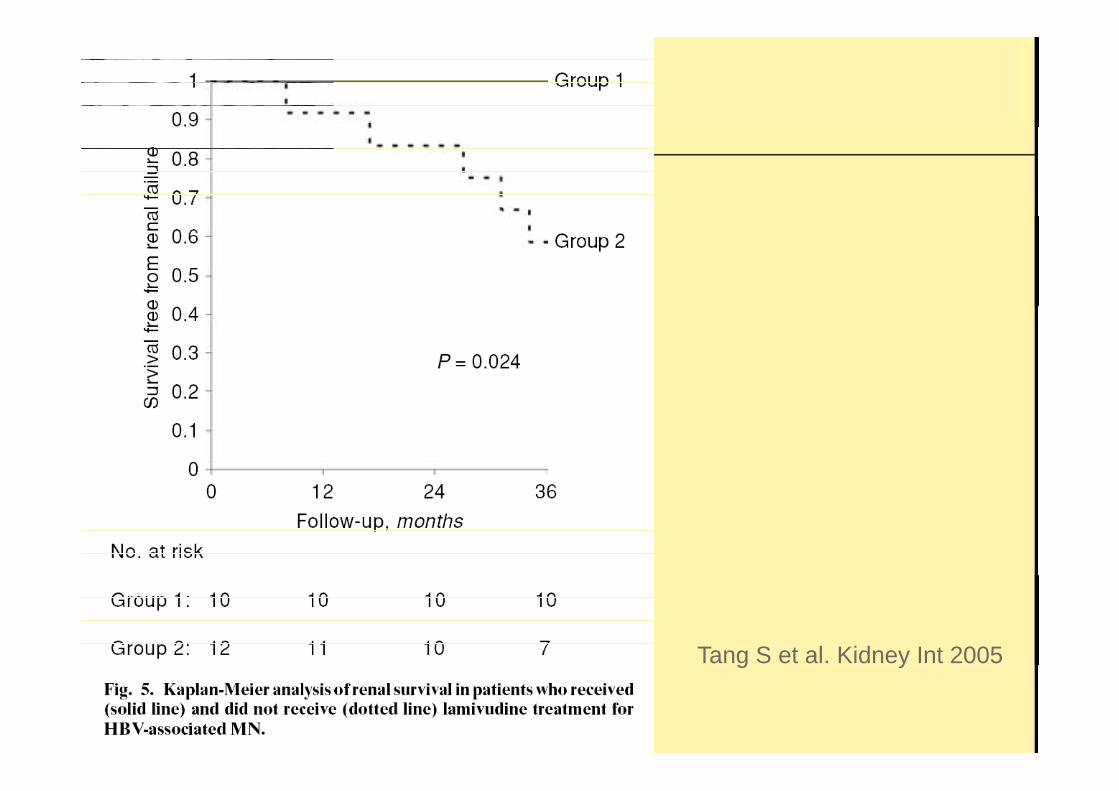
• Treatment with lamivudineTreatment with lamivudine – disappearance of HBV DNA
substantial reduction of proteinuria– substantial reduction of proteinuria – Six of 10 treated and 3 of 12 control patients
had remission of proteinuria to <0 3 g/dhad remission of proteinuria to <0.3 g/d.
• Conclusion: Lamivudine treatment improves renal outcome inHBVcarriers pwith MN and evidence of liver disease.
Tang S et al Kidney Int 2005Tang S et al. Kidney Int 2005
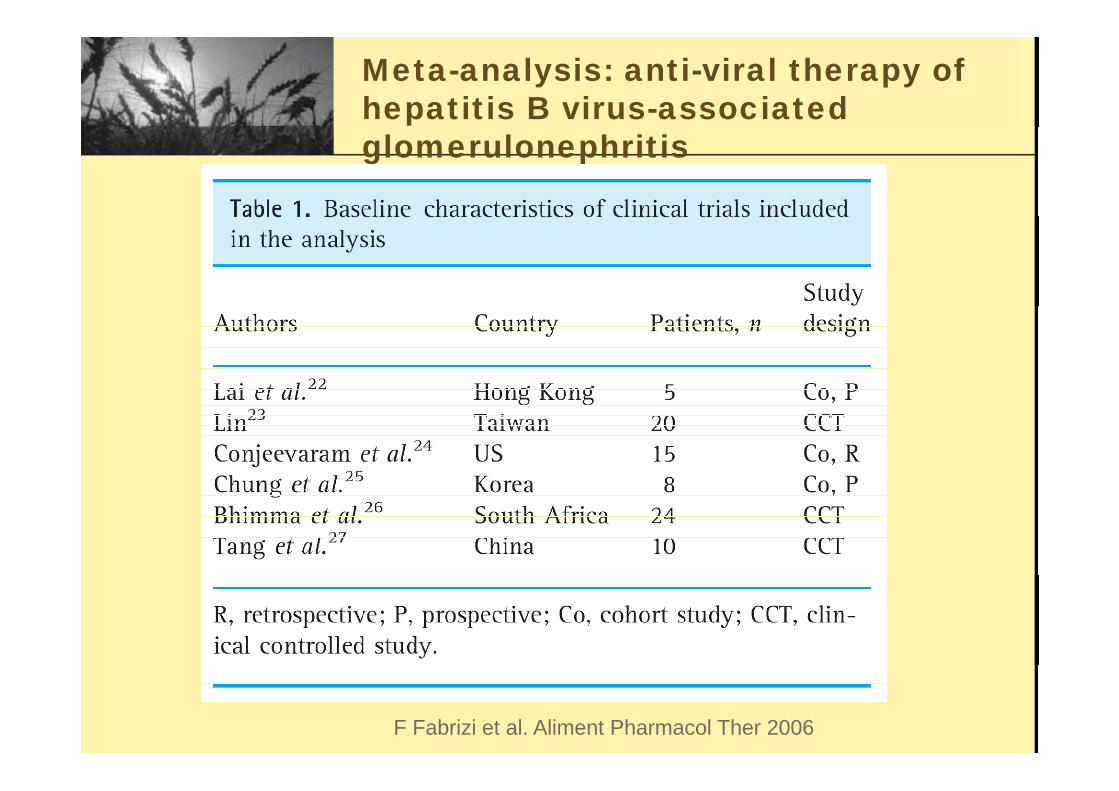
Meta-analysis: anti-viral therapy of hepatitis B virus-associated glomerulonephritis
F Fabrizi et al. Aliment Pharmacol Ther 2006
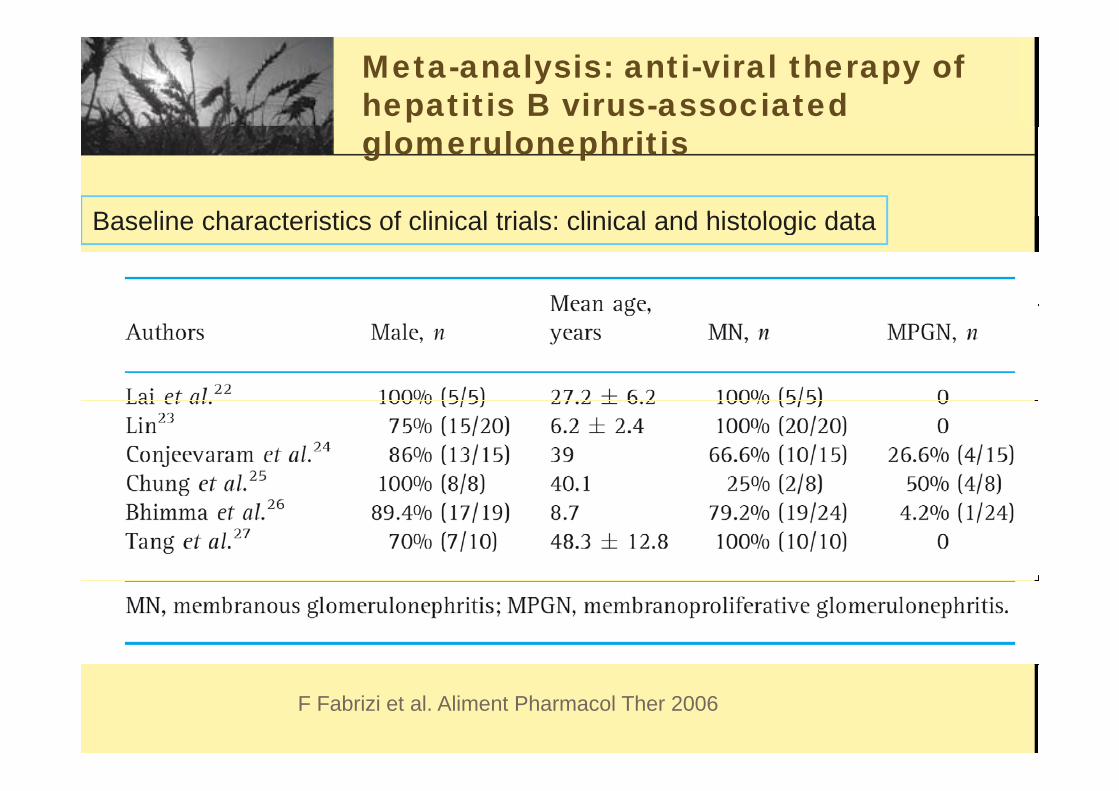
Meta-analysis: anti-viral therapy of hepatitis B virus-associated glomerulonephritis
Baseline characteristics of clinical trials clinical and histologic dataBaseline characteristics of clinical trials: clinical and histologic data
F Fabrizi et al. Aliment Pharmacol Ther 2006
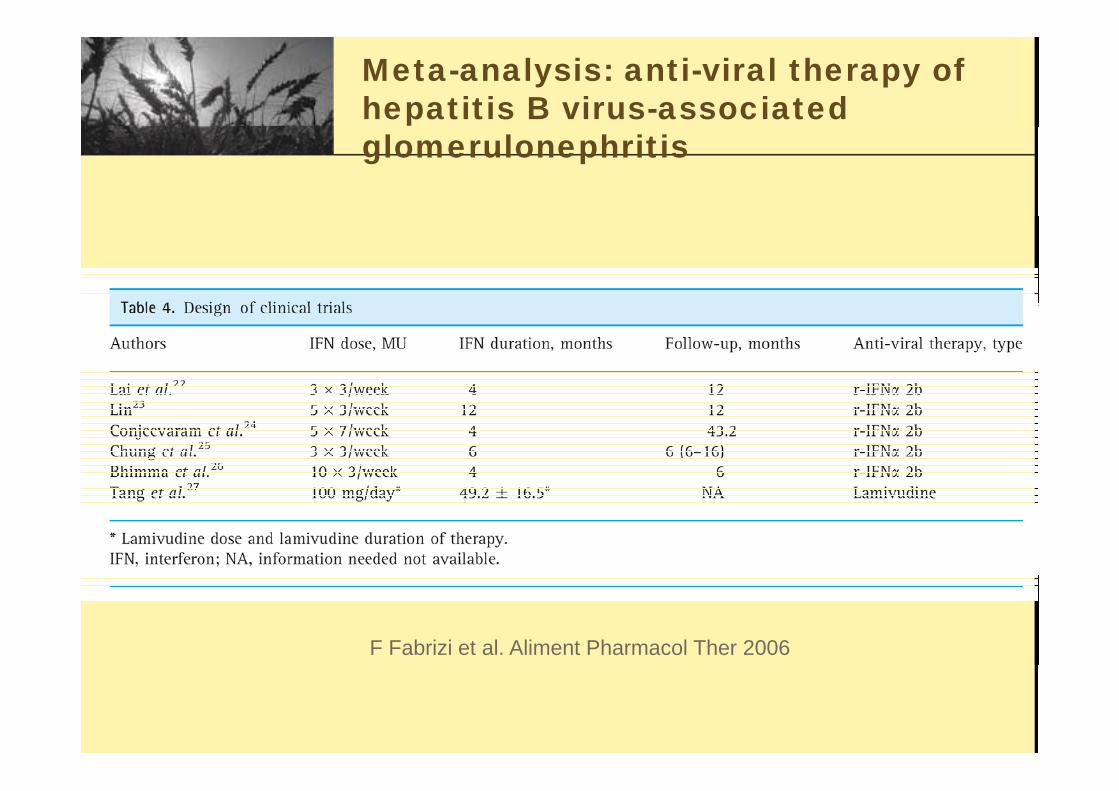
Meta-analysis: anti-viral therapy of hepatitis B virus-associated glomerulonephritis
F Fabrizi et al. Aliment Pharmacol Ther 2006
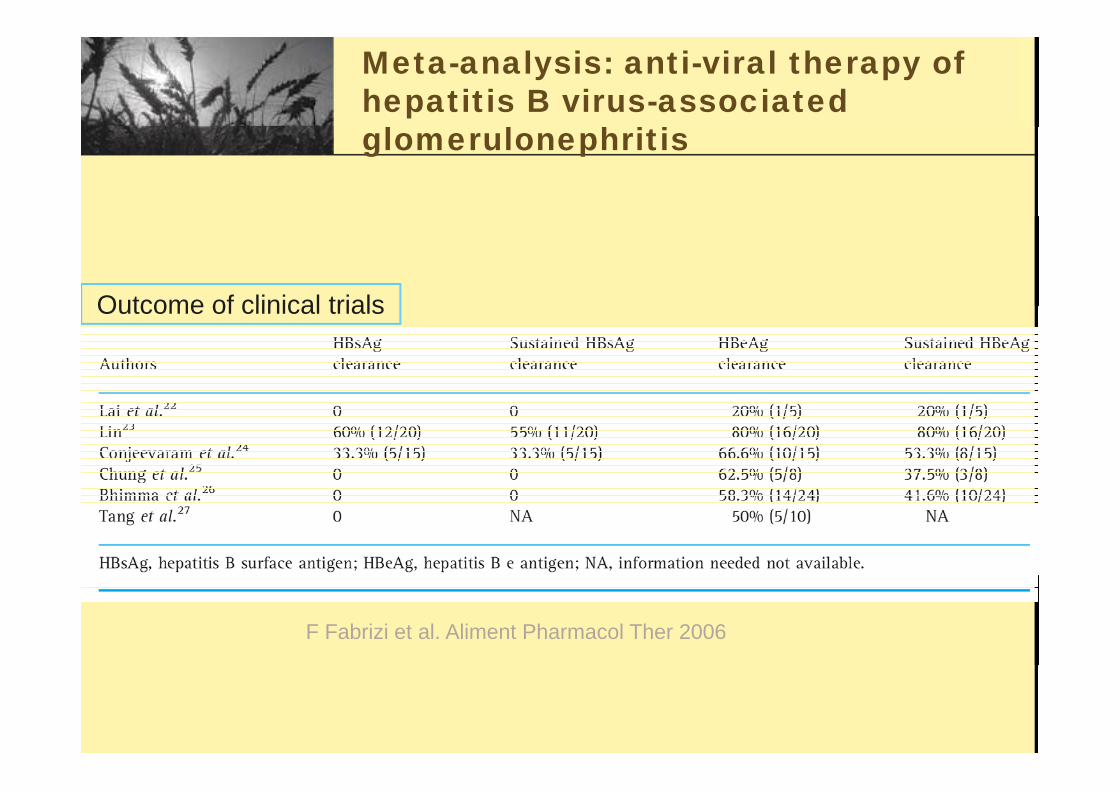
Meta-analysis: anti-viral therapy of hepatitis B virus-associated glomerulonephritis
Outcome of clinical trialsOutcome of clinical trials
F Fabrizi et al. Aliment Pharmacol Ther 2006
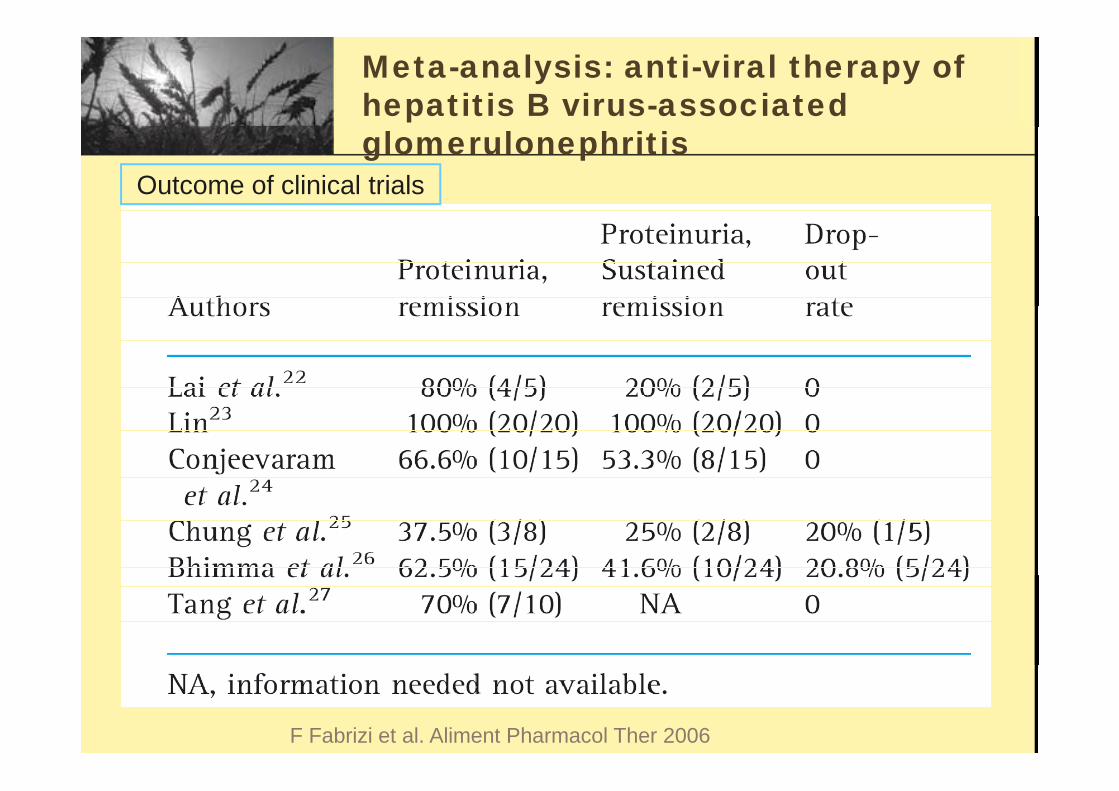
Meta-analysis: anti-viral therapy of hepatitis B virus-associated glomerulonephritis
Outcome of clinical trials
F Fabrizi et al. Aliment Pharmacol Ther 2006
Adefovir dipivoxilp
• OBJECTIVE: To investigate the efficacy and safety of adefovir dipivoxil (ADV) in• OBJECTIVE: To investigate the efficacy and safety of adefovir dipivoxil (ADV) in treating hepatic cirrhosis complicated with hepatitis B virus associated glomerulonephritis.
• Patient No : 6• Patient No.: 6
• RESULTS: • After 3 and 6 months treatment :
– negative conversion rates of HBV-DNA were 33.3% and 83.3%;– negative conversion rates of HBeAg were 16.7% and 66.7%;– positive conversion rates of HBeAb were both 16.7%;– Recovery rates of ALT were 83.3% and 100.0%; – recovery rates of TBil were 66.7% and 83.3% respectively.– Protein in the urine of two patients was decreased to 0.3 g/d and in three patients it was
50% of the original values.
Aft 1 t t t• After 1 year treatment:– Disease subsided fully in 3 and partially in 2 patients.
• CONCLUSION: Treating hepatic cirrhosis complicated with hepatitis B virus g p p passociated glomerulonephritis using adefovir dipivoxil is effective and safe.
Li DF et al.Zhonghua Gan Zang Bing Za Zhi. 2008
Entecavir
• Mechanism of action: -• Mechanism of action: -– Inhibits reverse transcriptase;– Incorporates into viral DNA (nucleoside
reverse transcriptase inhibitor)
• No data• No data
Tx duration ?
• Optimal duration of antiviral treatment is• Optimal duration of antiviral treatment is unclear
• Many patients will require prolongedMany patients will require prolonged treatment.
• Antiviral medications with low risk of resistance are preferred.
Tx Regime ? g
• Whether combination therapy will be• Whether combination therapy will be better remains to be determined.
Lamivudine Vs Entecavir
• Lamivudine:-– Greatest experience– Anecdotal reports of improvement in proteinuria and
renal outcomesrenal outcomes– Disadvantage: the high rate of resistance developing
with prolonged use (from treatment experience of p g ( pHBV disease in general).
E t i• Entecavir:-– may be preferred if long-term therapy is expected
from experience of recent advance of treatment of– from experience of recent advance of treatment of HBV disease.