Embed Size (px)
Citation preview

Gut, 1968, 9, 569-575
Primary lymphadenopathy complicating idiopathicsteatorrhoeaR. WHITEHEAD
From the Department ofPathology, Radcliffe Infirmary, Oxford
The association of abdominal lymphadenopathyand steatorrhoea has been extensively reviewed(Kent, 1964; Eidelman, Parkins, and Rubin, 1966)and there seems no doubt that a generalized reti-culosarcoma or Hodgkin's disease with involvementof the bowel and/or abdominal nodes can causesteatorrhoea (Sleisenger, Almy, and Barr, 1953).Not only is this steatorrhoea a biochemical entitybut it is also associated with the same histologicaljejunal villous atrophy seen in so-called idiopathicsteatorrhoea. Leaving aside such cases there areundoubtedly others in which a primary lymphadeno-pathy appears as a late complication of idiopathicsteatorrhoea (Best and Cook, 1961; Gough, Read,and Naish, 1962; Tonkin, 1963; Ross, 1965; Harris,Cooke, Thompson, and Waterhouse, 1967; Austad,Comes, Gough, McCarthy, and Read, 1967). Thedevelopment of this pathological entity, however,has not been adequately studied histologically andclearly only when it is more precisely defined willits clinical management be less empirical.
CASES STUDIED
The series includes seven cases in which a necropsywas performed and in four of these material obtainedduring life was also available. In one further casethe only material was obtained at laparotomy.Recent exhaustive clinical reviews of this compli-cation of steatorrhoea have stressed the changesin clinical pattern which herald the onset of thelymphadenopathy, and Harris et al (1967) haveshown that early treatment may help to prevent thecomplication. It is only necessary here, therefore, togive a brief clinical summary, and in Table I thelaparotomy and postmortem findings.
In cases 1, 2, 3, 4, and 7 there was a longstandinghistory and subsequent biochemical proof of stea-torrhoea preceding the onset of lymphadenopathy.In cases 2, 4, and 7 a jejunal biopsy furnished addi-tional evidence. In case 5, before a definite diagnosisof steatorrhoea, presumptive evidence of at leastseven years' previous malabsorption was provided
by a multiple deficiency anaemia responding poorlyto treatment (Whitehead, Carter, and Sharp, 1965)and a hypoproteinaemic oedema. Two years beforethe development of the lymphadenopathy a laparo-tomy showed no gross abnormality of the smallbowel or mesenteric nodes. A similar anaemia,oedema, and osteomalacia were the features shownin case 6 for some 10 years before steatorrhoea wasfinally diagnosed. Although only found to havesteatorrhoea one year before his death, case 8 had along history of mild diarrhoea and was includedbecause of the typical histological features seenin the tissue removed at laparotomy.
Table II summarizes the relevant findings in eachcase and this is accompanied by a more detaileddescription of the cases regarded as a whole.
PROGRESSIVE HYPERPLASIA
THE SMALL BOWEL In all cases the mucosa was inplaces of the flat type as seen with the dissectingmicroscope; elsewhere variations between this anda mucosa showing ridges and stunted, leaf-shapedvilli were seen. Histologically all ranges of villousatrophy up to the subtotal type were present (Fig. 1).The picture was basically that seen in uncomplicatedsteatorrhoea except that the inflammatory infiltratein the lamina propria tended to be denser. This wasmost marked in those cases showing mucosal ulcers,but in sites not ulcerated there was no extension ofthe infiltrate beyond the muscularis mucosa. Inaddition to lymphocytes the infiltrate is composedof large numbers of plasma cells sometimes con-taining Russell bodies and there are eosinophils,occasional histiocytes, and a proportion of cellshaving features of reticulum cells (Fig. 2). These havea blood monocyte-like nucleus, which often appearsfolded or is indented, and has a distinct nuclearmembrane, an open chromatin pattern, and a defi-nite nucleolus.
In the region of the ulcers the most obvioushistological feature is the extension of the infiltratebeyond the lamina propria (Fig. 3). The ulcer base
569
on July 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.9.5.569 on 1 October 1968. D
ownloaded from

R. Whitehead
TABLE ISUMMARY OF CASES STUDIED
Minimum Duration of LaparotomySteatorrhoea (Years)
Principal Postmortem Findings
1 PM 918/60SH 7193/60Hosp. no. 217971
2 PM 821/65Hosp. no. 227818
3 PM 145/61Hosp. no. 8680
4 PM 146/64SH 7414/62
7441/629303/63
Hosp. no. 332292
5 PM 302/62SH 7008/61Hosp. no. 298711
6 PM 836/61Hosp. no. 313623
7 SH 8073/6610624/66
Hosp. no. 4014438 PM 609/67SH 10052/66Hosp. no. 241225
52 Male 5 One month before deathBiopsy of enlargedmesenteric nodes
48 Male 9
58 Male 20
34 Male Since Fifteen months beforechildhood death-resection of
jejunal ulcer, enlargedmesenteric nodes Twomonths before deathfurther jejunal ulcersresected
45 Female 7 Two years before deathsmall bowel adhesionsrelated to chronicsalpingitis
64 Male 10
47 Male 15 Resection of jejunal ulcerand enlarged mesentericnodes
53 Male 1 Six months before deathresection of jejunalulcers and enlargedmesentric lymph nodes
Bronchopneumonia, pulmonary emboli; throm-bosis of inferior vena cava and leg veins;perforated ulcer of jejunum-peritonitis;simple gastric ulcers; enlarged mesenteric, para-aortic, cervical, and inguinal nodesBronchopneumonia; generalized enlargementof lymph nodes; tumour deposits in lungs,liver, spleen, marrow, pericardium; noulceration of bowelBronchopneumonia, bronchiectasis, rightpulmonary mycetoma (aspergillus ?); pul-monary emboli and infarcts, thrombosis ofleg veins; ulcer of ileum; mesenteric lymphnode enlargement; tumour infiltrates of liver,lungs, thoracic duct, and perirenal tissuesPulmonary emboli, thrombosis of leg veins;several jejunal and ileal ulcers; enlargedmesenteric lymph nodes
Pulmonary emboli and infarcts; thrombosisof leg veins; pulmonary and internal genitaltuberculosis; neoplastic ulcers of stomach,small and large bowel; enlarged nmesenteric andparaaortic nodes; tumour infiltrates of skin,breasts, liver, and heartOsteomalacia and multiple fractures; broncho-pneumonia and bronchiectasis; tentorialmeningioma and cholelithiasis; early cirrhosisof liver and splenic enlargement; enlargedmesenteric, paraaortic and peripancreaticlymph nodes; tumour infiltration of marrow
Bronchopneumonia, bronchiectasis, oldmyocardiac infarct; several neoplastic smallbowel ulcers; mesenteric lymph node enlarge-ment
Case No. Small Bowel Mucosa Year
TABLE IISUMMARY OF HISTOLOGICAL FINDINGS
Small Bowel Ulcers Mesenteric Nodes
1 Abnormal'
2 Abnormal3 Abnormal
4 Abnormal
5 Abnormal
1960 Mainly sarcoma with foci ofprogressive hyperplasiaremaining
1965 -
1961 Sarcoma
1962
&1963196419611962
1961
1965
&19661967
6 Abnormal
7 Abnormal
8 Abnormal
Progressive hyperplasiaProgressive hyperplasia withfocal sarcoma
Sarcoma
Progressive hyperplasia withfocal sarcoma
}Progressive hyperplasia
As ulcers Sarcoma
SarcomaMainly progressive hyperplasiawith focal sarcomaProgressive hyperplasiaAs ulcers
{Progressive hyperplasia with{focal sarcoma
Progressive hyperplasia withfocal sarcomaProgressive hyperplasia
{Progressive hyperplasia withfocal sarcoma
Sarcoma SarcomaSarcoma
Paraaortic nodes Sarcomanon-specifichyperplasiaParaaortic nodes Sarcomaas mesenteric
'Varying villous abnormality ranging to subtotal villous atrophy in one or all of biopsy, surgical and postmortem specimens.
570
Case Age Sex(Years)
Other Nodes Other Areas
on July 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.9.5.569 on 1 October 1968. D
ownloaded from

Primary lymphadenopathy complicating idiopathic steatorrhoea
......$..
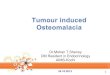
FIG. 1. Jejunal mucosa offlat type (case 7) showing absenceof villi. There is a dense inflammatory infiltrate in thelamina propria (haematoxylin and eosin x 100).
is composed of necrotic debris and necrosis is oftenalso seen in the deeper infiltrate which involves notonly the submucosa but also the muscularis proper.Occasionally the necrosis is associated with thrombiin nearby small vessels. At this stage the infiltrate isconsiderably denser than it is elsewhere and thereticulum cells increase in number at the expenseof the other cell types (Fig. 4). They show anincreasing pleomorphism and hyperchromasia withoccasional mitotic figures and binucleate forms.They correspond to the cell designated as a pro-histiocyte by Robb-Smith (1938). The serosa inrelation to the ulcers is frequently covered by azone of granulation tissue and organizing fibrinand an exact demarcation between this and theouter zone of cellular infiltrate is impossible.
LYMPH NODES In the earliest stages of lymph nodeenlargement (Fig. 5) follicles are increased innumber and are widely spaced, frequently showinggerminal centres. The sinuses are dilated and containoccasional cells of the type found in the medulla,together with a few foamy histiocytes. The sinusendothelial cells are plump and between the sinuses
FIG. 2. Jejunal mucosa (case 7) showing that the infiltratein the lamina propria contains reticulum cells whichare occasionally abnormal (haematoxylin and eosin x 300).
and the follicles the medulla contains a mixture ofcells identical to those seen in the bowel (Fig. 6).As the condition progresses abnormal reticulum
cells increase in number and other cell types decrease.As this occurs the medulla comes to occupy more ofthe node, the sinuses become obliterated, and thefollicles less distinct, often losing their germinalcentres (Fig. 7).
SARCOMA STAGE
THE SMALL BOWEL Between the stage of sarcomaand progressive hyperplasia stages of transitionare seen and some areas of progressive hyperplasiamay persist even when the sarcoma is advanced.The abnormal reticulum cells gradually appear inmore or less homogenous sheets (Fig. 8) and thetumour in each case shows the same type of histo-logical variation as reticulosarcomas arising else-where. Whilst some are well differentiated and pro-duce easily demonstrated fibres (Fig. 9), others aremore anaplastic and form scanty reticulin.
LYMPH NODES As the number of abnormal reti-
571
on July 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.9.5.569 on 1 October 1968. D
ownloaded from

F.I.G,w. .-
FIG. 4.
FIG. 3. Jejunal mucosa (case 8). The infiltrate can be seen penetrating the muscularis mucosa (haematoxylin andeosin x 40).FIG. 4. Jejunal mucosa (case 8). The infiltrate where the muscularis mucosa has been breached. Note the increasednumber and abnormality of reticulum cells and compare with Fig. 2 (haematoxylin and eosin x 300).
FIG. 6.
FIG. 5. Mesenteric lymph node (case 8). The follicles havegerminal centres, there are dilated sinuses, and the medullais cellular (haematoxylin and eosin x 35).
FIG. 6. Same lymph node as in Fig. 5 to show abnormalreticulum cells in the medulla. At upper left and rightthe edges offollicles can be seen (haematoxylin and eosinx 120).FIG. 5.
on July 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.9.5.569 on 1 October 1968. D
ownloaded from

Primary lymphadenopathy complicating idiopathic steatorrhoea
FIG. 7.FIG. 8.
FIG. 7. Mesenteric lymph nodefrom case 4 (necropsy 1964).The follicles have lost their germinal centres and themedulla is extremely cellular with a high abnormalreticulum cell component (haematoxylin and eosin x 35).
FIG. 8. Jejunal mucosa (case 5) showing sarcomatouschange (top) merging with autolysed mucosa (below).The muscularis mucosa runs diagonally top right to bottomleft (haematoxylin and eosin x 100).
FIG. 9. Pericellular reticulin production by sarcoma inlymph node (case 5) (Robb-Smith reticulin x 370).
FIG. .....:....;..:
FIG. 9.
573
A.
M.M
on July 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.9.5.569 on 1 October 1968. D
ownloaded from

574~ R. Whtehea
_ .*. * v s. a* '~
FIG. 10. FIG. 11.
FIG. 10. Mesenteric lymph node (case 2). The abnormal reticulum cells have all but filled the node, small groups oflymphocytes remain. Note capsular invasion (haematoxylin and eosin x 100).FIG. 1 1. Mesenteric lymph node (case 5). Diffuse abnormal reticulum cell proliferation (haematoxylin and eosin x 100).
culum cells increases in the medulla, reticulin isproduced concomitantly and produces abnormalskeins of fibres in the interfollicular areas and gra-dually as diffuse sarcoma supervenes the normalpattern of reticulin is replaced by a diffuse network.Other types of cells gradually disappear (Fig. 10)and the sarcoma begins to penetrate the capsule.Areas of progressive hyperplasia persist for a timeas in the bowel but gradually a uniform picture ofreticulum cell sarcoma is produced (Fig. 11).Sarcoma of mesenteric nodes can develop inde-
pendently of that in the bowel and vice versa. Oncethis stage is reached in either site sarcoma maybe found in other nodes and in other organs.Whether other nodes are involved by metastases orgo through a stage of hyperplasia is not known.Progressive hyperplasia with focal sarcoma wasseen with regularity only in the mesenteric nodesand only in one case (case 6) in other abdominalnodes (the paraaortic nodes). On the evidence, aswith other generalized lymph node malignancies,both metastases and a multifocal origin areprobable.
DISCUSSION
In previously published cases of a lymphadenopathycomplicating steatorrhoea it has been describedvariously as Hodgkin's disease, lymphosarcoma, orreticulosarcoma. In this study the course of pro-gressive hyperplasia turning into malignancy isshown to be a characteristic and definite entityending as it does in a reticulum cell sarcoma. Inthe stage of progressive hyperplasia it is easy tosee its superficial resemblance to Hodgkin's disease.Apart from the fact that Hodgkin's disease seldominvolves the gastrointestinal tract, the intimatemorphology of the lymphadenopathy associatedwith steatorrhoea is quite distinct from Hodgkin'sdisease. Even in the cellular phase of Hodgkin'sdisease the normal architecture of the node isobscured by the cellular proliferation in whichreticulum cells, including Sternberg-Reed cells,lymphoid cells, fibroblasts and eosinophils predo-minate whereas cells of the histiocyte series areinconspicuous; in the steatorrhoea lymphadenopathythe architectural landmarks of the node are main-
R. Whitcehead574
on July 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.9.5.569 on 1 October 1968. D
ownloaded from

Primary lymphadenopathy complicating idiopathic steatorrhoea 575
tained until sarcomatous change develops, the pre-dominant cell is of the histiocyte or prohistiocytetype, and fibrosis does not occur although thereusually is an increase in reticulin. Robb-Smith(1938) described this type of progressive hyperplasiaas 'prohistiocytic fibrillary reticulosis' and in 1964emphasized its association with steatorrhoea. How-ever it would seem simpler to designate this form oflymphoreticular proliferation as the steatorrhoealymphadenopathy.
It is equally clear how in some of these cases ahistological diagnosis of lymphosarcoma could bereached. This is true especially when the cells are offairly uniform type and fibre production is notmarked. In our material fibre production has alwaysbeen a feature even in the more pleomorphic andanaplastic tumours.Why this complication occurs is not known but it
may be in the nature of an autoimmune responsewhich goes on to irreversible malignancy. In thisrespect the condition may be compared with thereticuloses which complicate a percentage of casesof Hashimoto's disease (Cox, 1964). There is infact some serological evidence (Malik, Watson,Murray, and Cruickshank, 1964) that the lesion ofidiopathic steatorrhoea is autoimmune in originand the glandular atrophy with a lymphocytic andplasma cell infiltrate are typical of the lesions seenin other autoimmune diseases. The change canaffect the small bowel, lymph nodes, or both, andonce sarcoma has supervened infiltration of otherorgans may appear. It is obvious, therefore, thatrepeated small bowel biopsies will not necessarilyhelp in the early diagnosis of the condition but ifabnormal reticulum cells and numerous eosinophilsare seen in an otherwise typical small bowel biopsyin steatorrhoea then the condition should be sus-pected.
If the complication is suspected due to a changein the clinical picture of the steatorrhoea patient,and if radiographic investigation is negative, adiagnostic laparotomy is probably indicated. Be-cause the whole small intestine is potentially in-volved it would seem that surgical resection of thelocal lesions and lymph nodes which has beenadvocated (Lancet, 1964) is not a rational procedure.Whether radiotherapy and/or cytotoxic drugs shouldbe recommended, and at what stage they should beused, are problems which will only be solved when the
entity as a specific complication of steatorrhoea isbetter recognized and experienced.
SUMMARY
Idiopathic steatorrhoea is sometimes complicatedby a lymphadenopathy. The development of thislymphadenopathy as a progressive hyperplasia whichbecomes reticulosarcoma has been studied and des-cribed in eight cases. It is concluded that the lympha-denopathy of steatorrhoea is a specific histologicalentity which could be called 'steatorrhoea lympha-denopathy'.
During the preparation of this paper I have been fortu-nate to have the advice and helpful criticism of Dr A.H. T. Robb-Smith to whom I am indebted. For allowingaccess to the case records I would also like to expressmy thanks to those physicians and surgeons of theRadcliffe Infirmary who were responsible for the patients'care.
REFERENCES
Austad, W. I., Cornes, J. S., Gough, K. R., McCarthy, C. F., andRead, A. E. (1967). Steatorrhea and malignant lymphoma.Amer. J. dig. Dis., 12, 475-490.
Best, C. N., and Cook, P. B. (1961). Cases of mesenteric reticulo-sarcoma associated with gluten-sensitive steatorrhoea. Brit.med. J., 2, 496-498.
Cox, M. T. (1964). Malignant lymphoma of the thyroid. J. clin.Path., 17, 591-601.
Eidelman, S., Parkins, R. A., and Rubin, C. E. (1966). Abdominallymphoma presenting as malabsorption. Medicine (Baltimore).45, 111-137.
Gough, K. R., Read, A. E., and Naish, J. M. (1962). Intestinalreticulosis as a complication of idiopathic steatorrhoea. Gut,3, 232-239.
Harris, 0. D., Cooke, W. T., Thompson, H., and Waterhouse, J. A.H. (1967). Malignancy in adult coeliac disease and idiopathicsteatorrhoea. Amer. J. Med., 42, 899-912.
Kent, T. H. (1964). Malabsorption syndrome with malignant lym-phoma. Arch. Path., 78, 97-103.
Lancet (1964). Coeliac disease and malignant change. 1, 544.Malik, G. B., Watson, W. C., Murray, D., and Cruickshank, B.
(1964). Immunofluorescent antibody studies in idiopathicsteatorrhoea. Lancet, 1, 1127-1129.
Robb-Smith, A. H. T. (1938). Reticulosis and reticulosarcoma: ahistological classification. J. Path. Bact., 47, 457-480.
-(1964). The classification and natural history of the lympha-denopathies. In Lymphomas and Related Diseases, p. 24,edited by S. J. Park and I. M. Ariel Hoeber Medical Division,New York.
Ross, J. R. (1965). The gastrointestinal biopsy capsule as a diagnosticaid. Amer. J. Gastroent., 43, 285-302.
Sleisenger, M. H., Almy, T. P., and Barr, D. P. (1953). The spruesyndrome secondary to lymphoma of the small bowel. Amer. J.Med., 15, 666-674.
Tonkin, R. D. (1963). Reticulosis of the small bowel as a late compli-cation of idiopathic steatorrhoea. Proc. roy. Soc. Med., 56,167-168.
Whitehead, R., Carter, R. L., and Sharp, A. A. (1965). Anaemia inoccult intestinal malabsorption. J. clin. Path., 18. 110-113.
on July 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.9.5.569 on 1 October 1968. D
ownloaded from