Embed Size (px)
Citation preview

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 1
JeanJean--Jacques Zambrowski Jacques Zambrowski MD, PhDMD, PhD
Health Law & EconomicsHealth Law & EconomicsRenRenéé Descartes University Descartes University -- ParisParis
Department of Internal MedicineDepartment of Internal MedicineBichat University Hospital Bichat University Hospital -- ParisParis
04 May 200704 May 2007
Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical PracticePrinciples and Methods of Health Economics
Their role in the Evaluation of Medical Practice
Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
MARMARA MARMARA ÜÜNIVERSITESI REKTNIVERSITESI REKTÖÖRLRLÜÜĞĞÜÜAkilci Akilci ÍÍlalaçç Kullanimi ve Farmakoekonomi SempozyumuKullanimi ve Farmakoekonomi Sempozyumu
© JJ Zambrowski - May 2007 2Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
and thank you for your effortunderstanding my English !
Beni bağışlama
konuşmamak Türk !
© JJ Zambrowski - May 2007 3Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health has no price…
But it has a cost !Health Care and Health Cost
The Changing Paradigm Health Care and Health Cost
The Changing Paradigm
Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
© JJ Zambrowski - May 2007 5Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health costs rise exceeds GDP growth
In emerging as well as in developed countries, healthcare expenditures are growing faster than the economy.Several reasons
continuous progress in healthcareboth for diagnostic and therapeutic tools and strategies,
aging of the population.All Health Insurance systems, private or public, have to face shortage in resources.This create the need for a better efficiency.
© JJ Zambrowski - May 2007 6Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health costs rise exceeds GDP growth
In emerging as well as in developed countries, healthcare expenditures are growing faster than the economy.Several reasons
continuous progress in healthcareboth for diagnostic and therapeutic tools and strategies,
aging of the population.All Health Insurance systems, private or public, have to face shortage in resources.This create the need for a better efficiency.
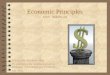
It is estimated that
increase in Health expenditures (%) = increase in GDP (%) + 1,5 points
It is estimated that
increase in Health expenditures (%) = increase in GDP (%) + 1,5 points
100
105
110
115
Year 1 Year 2 Year 3 Year 4 Year 5
GDPHRE

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 2
© JJ Zambrowski - May 2007 7Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Today's challenge : find the good level of spending
(Values : 2000)
© JJ Zambrowski - May 2007 8Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Turkey : x 12 in the last 30 years !Turkey Health Expenditures per capita
0
100
200
300
400
500
600
700
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
US$
OECD - 2006
© JJ Zambrowski - May 2007 9Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Turkey : x 12 in the last 30 years !Turkey Health Expenditures per capita
0
100
200
300
400
500
600
700
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
US$
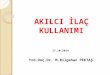
0
2
4
6
8
1996 1997 1998 1999 2000 2001 2002 2003 2004 2005
% of GDP
OECD - 2006
© JJ Zambrowski - May 2007 10Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health related expenses / PIB : Turkey gets closer to OECD mean value
© JJ Zambrowski - May 2007 11Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Pharmaceutical consumptionThe Turkish drug market is witnessing rapid growth
Country's recovery from the 2002 economic crisis picks up pace.
Pharmaceutical sales should reach US$11.1bn in 2010. Recent reforms of the country's social security system are set to have a dramatic impact on drug expenditure. This
will involve the introduction of a basic universal health insurance system, meant to cover 90% of the population. is expected to combine with other key reforms, such as the availability of more cost-effective pharmaceuticals (generics…).
0
1000
2000
3000
4000
5000
6000
1992 1995 1998 2001 2004 2006
Millions US$
© JJ Zambrowski - May 2007 12Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Pharmaceutical consumption
Turkey is in 3rd place for the Middle East & Africa The country's long term political and economic outlook is improving, as the government
toes the International Monetary Fund (IMF) line on economic policy and also looks towards EU accession.
However, the rigorous structural reform initiated by Turkish authorities following the 2001 economic crisis and the IMF advice, along with the reform of the healthcare system in line with the World Bank recommendations
may meanmay mean government health spending as a percentage of GDP is to be reduced.
!

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 3
© JJ Zambrowski - May 2007 13Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health Expenditures : big discrepancies
Total Health Expenditures - US$ - 2003WHO - Health Systems Financing - May 2006
France2500 €/p/y
Turkey500 €/p/y
Mali25 €/p/y
France2500 €/p/y
Turkey500 €/p/y
Mali25 €/p/y
© JJ Zambrowski - May 2007 14Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Spend More does not mean Do Better !
400
500
600
700
800
900
1000
1100
0 1000 2000 3000 4000
GR
A
P GB
E
SI
DUSA
CH
FJ
CANNL
Health Expenditures ( $ PPA)
Mortality (100 000)
Adapted from E. Barral - 1999
© JJ Zambrowski - May 2007 15Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health Economics
Applying economic principles and theories
to health and to the health care sector
source : Prof. Lieven Annemans - Health economist - Ghent University (Belgium)
© JJ Zambrowski - May 2007 16Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
What are Economics ?
EconomyEconomy comes from two Greek wordsΟικοσ : the house, the place where one is livingΝοµια : the rule, the management
EconomyEconomy means""the management of the place the management of the place wherewhere wewe livelive““i.e. the way one makes the best possible use ofthe way one makes the best possible use ofthe available resourcesthe available resources
Human resourcesTechnical resourcesFinancial resources,…
© JJ Zambrowski - May 2007 17Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Spend better, not spend less !
Economics is notnot primarily about saving money
It is about using scarce resources as efficientlyefficiently as possible
© JJ Zambrowski - May 2007 18Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health: costs are skyrocketing…
In all of the developed countries, health -related spending is growing faster than the overall economy.Governments and Health Insurance systems – private and public alike – are trying in vain to control this growing expenditure.The role of medico and pharmaco-economics is to enable healthcare organizations to offer
Better Care at Better CostBetter Care at Better Cost

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 4
© JJ Zambrowski - May 2007 19Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health: costs are skyrocketing…
In all of the developed countries, health -related spending is growing faster than the overall economy.Governments and Health Insurance systems – private and public alike – are trying in vain to control this growing expenditure.The role of medico and pharmaco-economics is to enable healthcare organisations to offer
Better Care at Better CostBetter Care at Better Cost
Medico and Pharmaco-Economics :
Not always spend lessbut always spend better !
Medico and Pharmaco-Economics :
Not always spend lessNot always spend lessbut always spend better !but always spend better !
thinking in terms of overall costsbeing constantly concerned with economic efficiencymaking no concessions regarding
the quality of care (medical outcome)the quality of life (individual and social outcome)
thinking in terms of overall costsbeing constantly concerned with economic efficiencymaking no concessions regarding
the quality of care (medical outcome)the quality of life (individual and social outcome)
© JJ Zambrowski - May 2007 20Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Healthcare Costs…
© JJ Zambrowski - May 2007 21Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health Care as a Percent of GDP
0
5
10
15
1960 1965 1970 1975 1980 1985 1990 1995 2000Adapted from New England Healthcare Institute, 2004
Cost Increases Will Persist
2005 2010
Drugs
AgingMed Tech
© JJ Zambrowski - May 2007 22Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Realistic approach to life’s problemsReliance on quantitative informationOften must make difficult choices in the face of uncertaintyGood decisions require comparing benefits and risks (costs)
Important Similarities Between Physicians and Economists
© JJ Zambrowski - May 2007 23Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Big Difference Between Physicians and Economists
Physicians are usually concerned with an individual patient or small numbers of patientsEconomists are usually concerned with large aggregations:
organizations, industries, governments, society as a whole
© JJ Zambrowski - May 2007 24Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
PatientPatient--Clinical CureClinical Cure--Quality of lifeQuality of life--OutOut--ofof--pocket Costpocket Cost--Satisfaction with Satisfaction with treatment processtreatment process
Hospital / PhysicianHospital / Physician--Clinical CureClinical Cure--Profit from treatmentProfit from treatment--Ethical issuesEthical issues
3rd3rd--Party PayerParty Payer--Clinical CureClinical Cure--CostCost--Customer Customer perception of valueperception of value
Employer / SocietyEmployer / Society--Clinical CureClinical Cure--CostCost--ProductivityProductivity
Which perspective ?

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 5
© JJ Zambrowski - May 2007 25Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
ClinicalClinical
• Efficacy• Safety• Impact of therapy
on “natural history”of the disease
EconomicEconomic
• Cost Analysis • Cost-of-Illness• Cost-Minimization• Cost-Benefit• Cost-Effectiveness • Cost-Utility
HumanisticHumanistic
• Health Related Quality of Life
• Patient Satisfaction• Caregiver Impact• Patient Preferences• Functional Status
Health Services ResearchHealth Services Research•Policy Research •Access •Structure of Care
The assessment of technology The assessment of technology (drugs, devices, etc)(drugs, devices, etc)
Outcomes Research
© JJ Zambrowski - May 2007 26Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
DirectDirect
• Doctors, nurses,other personnel involved by case
•Lab, X-Ray, …• Medication• Op. rooms used
IndirectIndirect
• Transport• Time off work• Time of relatives
having to stay withthe patient
• Hospital fixed costs
IntangibleIntangible
• Value of pain anddisabilities
• Pretium doloris• Well-being losses• Morale
Hospital fixed costsHospital fixed costs• Administration • Education • Research
The various types of costs in HealthcareThe various types of costs in Healthcare
Costs : everything counts for !
• Permanence
© JJ Zambrowski - May 2007 27Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Preliminary ConclusionsPreliminary Conclusions
Resources are limited while demand keep Resources are limited while demand keep increasing.increasing.The environment is changing in depth :The environment is changing in depth :
aging populationaging populationexponential scientific progressexponential scientific progresslegal and regulatory constraints increaselegal and regulatory constraints increase
safetysafetycostcost--containmentcontainment
This creates the need for pharmacoeconomicsThis creates the need for pharmacoeconomicsThe goal is to increase efficiencyThe goal is to increase efficiency
costcost--effectiveness effectiveness the best possible efficacy at the best possible the best possible efficacy at the best possible global global cost. cost.
Health Economics As Part Of The Relation Between Physicians and Payers
Health Economics As Part Of The Relation Between Physicians and Payers
Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
© JJ Zambrowski - May 2007 29Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Health Economic EvaluationsAre Just One Part of Health Economics
HealthHealthEconomicsEconomics
HealthEconomicEvaluation
other topics in health economics:optimal size of hospitals, optimal payment for physicians, optimal level of co-payment by patients,….
© JJ Zambrowski - May 2007 30Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Definition of Health Economic Evaluation
The comparativecomparative analysis of alternative courses of action in terms of BOTHBOTH
their costsand health consequences
Pharmaco-economic evaluation=
if at least one drug is involved
Pharmaco-economic evaluation=
if at least one drug is involved

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 6
© JJ Zambrowski - May 2007 31Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Why Health Economic Evaluation?
Budgets are limited, needs are “unlimited”Safety and efficacy do not suffice anymoreIn a world with scarce resources efficiencyefficiency= costcost--effectivenesseffectiveness becomes important
Goal = to allocate the limited budgets to those interventions that offer the most health gain per unit of money
© JJ Zambrowski - May 2007 32Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
What are Policy-makers trying to do ?
Protect and improve the health of the populationAssure access to medical careAchieve efficient use of health care resourcesControl the rate of growth of expenditures for medical care
But also : Avoid bad headlines in the Press…
© JJ Zambrowski - May 2007 33Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
The Different Steps of Evidence
Can it work ? EfficacyEfficacy
Does it work in reality ?EffectivenessEffectiveness
Is it worth doing it, compared to other things we could do with the same money ?
CostCost--effectivenesseffectiveness = EfficiencyEfficiency
© JJ Zambrowski - May 2007 34Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Evaluating a new mode of care
More effective or Less Side-effects or More ConvenientIFIF
Less Physicians Consultations?Less or Shorter Hospitalisation?Less or Cheaper Interventions?
Less Other Drugs?Less Tests and Imaging?
THENTHEN
and only if…and and onlyonly ifif……
© JJ Zambrowski - May 2007 35Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Sometimes little progress has a useless cost
BA
Average AcquisitionAcquisitioncost
New Drug B is more more expensiveexpensive but not a great progressAverage otherother treatment costs• physicians• hospital• surgery• other drugs• tests• ....
+BA
© JJ Zambrowski - May 2007 36Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
If not a real progress, why a useless cost ?
Average otherother treatment costs• physicians• hospital• surgery• other drugs• tests• ....
+ =BA
Average AcquisitionAcquisitioncost
TOTAL COSTCOST
∆ = net cost∆ = net cost
New Drug B is more expensive; is it a REAL progress ?more expensive; is it a REAL progress ?
BA BA

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 7
© JJ Zambrowski - May 2007 37Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
TOTAL COSTCOST
∆ = net saving∆ = net saving
Sometimes real progress “more expensive”saves money
Average otherother treatment costs• physicians• hospital• surgery• other drugs• tests• ....
+ =BA
Average AcquisitionAcquisitioncost
This happens if B is more more effectiveeffective and/or more convenientmore convenient
BA BA© JJ Zambrowski - May 2007 38Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Only Global Costs make sense
The cost of a given treatment is not only the cost for the drug.One should also consider the cost for
the preparation (pharmacist and technician)the administration (nurse)the monitoring (laboratory tests)
but alsothe side effects (follow-up and delay in cure)…and the failure of the treatment
© JJ Zambrowski - May 2007 39Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
success
70 %
failure
30 %
drug A = 1000
success
90 %
failure
10 %
drug B = 2000
treat disease X
The cost of failure
40004000
30003000
10 0002 0001 000Primary cost
failurefailureBA
Real cost = 1 000 + (0.3 x 10 000 ) 2 000 + (0.1 x 10 000) cost for drug + cost of failure = 4 000 = 3 000
Evaluation of the efficiency of the treatments of Anaemia in Onco-Hematology
Evaluation of the efficiency of the treatments of Anaemia in Onco-Hematology
Example
28©Istanbul Istanbul OncologyOncology MeetingMeeting
© JJ Zambrowski - May 2007 41Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
The economic burden of anaemia in patients with cancer is significant
Patients with anaemia have significantly higher total healthcare expenditures than non-anaemic patients
Mean 6-month total healthcare expenditures (unadjusted):
For any given healthcare status, treating a patient who is anaemic is associated with considerably higher expenditures than non-anaemic patients
Lyman et al. Value in Health 2005;8(2):149–55
70% greater cost
© JJ Zambrowski - May 2007 42Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
The economic burden of anaemia in patients with cancer is significant
Patients with anaemia have significantly higher total healthcare expenditures than non-anaemic patients
Mean 6-month total healthcare expenditures (unadjusted):
For any given healthcare status, treating a patient who is anaemic is associated with considerably higher expenditures than non-anaemic patients
Lyman et al. Value in Health 2005;8(2):149–55
Anaemia
$ 62,499
No anaemia
$ 36,871
70% greater cost
The cost for Non TreatingThe cost for Non Treatingor Non Treating adequatelyor Non Treating adequatelycan be dramatically highercan be dramatically higherthan the cost of treatment !than the cost of treatment !

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 8
© JJ Zambrowski - May 2007 43Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Anaemia has an immense cost
To healthcare systemsCost of management
And also to the patientImpaired QoL
© JJ Zambrowski - May 2007 44Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
What does blood cost per unit?
Blood transfusion costs: a multicenter study.Forbes JM, et al. Transfusion. 1991 May; 31(4):318–23
Global mean costs per unit transfused in oncology patients: 469 $ (360 €) Mean costs for 2 units transfused per session = 938 $ (720 €)
Cost of Outpatient Blood Transfusion in CancerPatients. J Clin Oncol 18;(14)2000:2755–61
Cost of blood37%
Blood bank13% Laboratory tests
43%
Administration7%
© JJ Zambrowski - May 2007 45Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Blood is getting more expensive to transfuse safely
Donor supply is declining — each unit takes more effort to collectScreening tests needed — each new test costs more and rejects more donors
Patient screening:■ Reduces risk of exposure to infection (e.g.
variant CJD*)Blood screening:■ Blood groups — minor compatibility antigens■ Diseases — new variants of hepatitis and HIV
Screening for variant CJD* becoming necessary*Creutzfeldt–Jakob disease
© JJ Zambrowski - May 2007 46Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
The overall cost of treatment with rHuEPO is less than for transfusion
Costs of the moral consequences linked to iatrogenic complicationsCost of disturbance, loss of time
Costs of the moral consequences linked to iatrogenic complications
Intangible
Possible costs of carers and other professionalsPost of loss of productivity (patient and accompanying parties)Cost of donor’s time
Possible costs of carers and other professionals
Indirect
Preparation, treatment, tests, administration, premedication, iron supplementation, adverse events and possible complications, patient transport
Acquisition, administration,tests, iron supplementation, transfusion (if response is insufficient)
DirectTransfusionTransfusionEPOEPOCOSTSCOSTS
© JJ Zambrowski - May 2007 47Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
The cost of treatment with rHuEPO is less than that for transfusion
Coiffier et al.1 showed that for a comparable increase in QoL (FACT-F points gained)
treatment with rHuEPO cost 5–7 times less than transfusion
1. Coiffier et al. Blood 2000;96(11): Abstract 5440
0
0,2
0,4
0,6
0,8
1
Epoetin beta Transfusion
Relative cost for a similar gain in QoL
"€0.15–0.19 spent onepoetin beta are neededto reach the same improvements in qualityof life as €1 spent onstandard therapy."
© JJ Zambrowski - May 2007 48Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
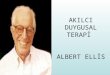
A weekly rHuEPO regimen is cost-effective vs blood transfusion
Cost-effectiveness of EPO (Markov analysis)Two patient cohorts treated for lung cancerSecond cohort received EPO weekly if Hb <11 g/dlSignificant reduction in transfusions required (33.6% to 19.1%)
Decreased number of units transfused (2.97 to 2.11)
Cost-effectiveness ratio favourable for EPO : 7.02 vs 9.04This sensitive analysis confirms the advantage of EPO in the majority of situations.
EPO is more costEPO is more cost--effective than transfusion foreffective than transfusion forlung cancerlung cancer
Borget et al. Lung Cancer 2006;51(3):369–76

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 9
© JJ Zambrowski - May 2007 49Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
EPO therapy accounts for <2% of total expenditures in cancer patients with anaemia
Proportion of total cost for treating with rHuEPO
Based on a dosage of 30 000 IU/week and an average treatment length of 12 weeks per year, EPO therapy costs approximately €2500–3000/patient/year
Lyman et al. Value in Health 2005;8(2):149–55
How to Evaluate Costsand Benefits in Healthcare
issues ?
© JJ Zambrowski - May 2007 51Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
COST AND EFFECTS: the key graph
Tota
l cos
t (va
lue
per p
atie
nt)
Effect (LY, QALY, SFD, QoL …)
A
0
∆ effect
∆C
ost
LY = Life Years, QALY = Quality Adjusted LY, SFD = symptom free days, QoL = quality of life
ValueValue 2N2N / LY/ LYValueValue 5N / 5N / LYLY
Value N / LYValue N / LYB
© JJ Zambrowski - May 2007 52Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Effectiveness /Outcomes
IV
Treatment Cost
C
: New Drug
C : Control
: New Drug
C : ControlII
I III
Adopt
RejectEvaluate
Evaluate
Value : Ratio Acceptability
LOW
LOW
HIGH
HIGH
© JJ Zambrowski - May 2007 53Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
The cost-effectiveness plane
adapted from Alastair Gray - Oxford Healtrh Economics Research Center
© JJ Zambrowski - May 2007 54Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Cost myopia

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 10
© JJ Zambrowski - May 2007 55Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
How to Express Effectiveness ?
clinical parameters (efficacy)symptom free daysN of cured patientsevent free survivalavoided eventscured patients saved livessaved life yearsimproved QoLdays in good QoLquality adjusted life years
© JJ Zambrowski - May 2007 56Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
clinical parameters (efficacy)symptom free daysN of cured patientsevent free survivalavoided eventscured patients saved livessaved life yearsimproved QoLdays in good QoLquality adjusted life years
How to Express Effectiveness ?
QUANTITYOF LIFE
QUALITYOF LIFE
© JJ Zambrowski - May 2007 57Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
QALY = Quality Adjusted Life Years
No Drug
Drug B
death
INDEX (“utility level”)
TIME
1
0Drug A
Adding Life to Years….Adding Life to Years….© JJ Zambrowski - May 2007 58Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
QALY = Quality Adjusted Life Years1
adapted from Alastair Gray - Oxford Healtrh Economics Research Center
© JJ Zambrowski - May 2007 59Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
How to Interpret Results of cost-effectiveness studies?
WhatWhat is is costcost--effectiveeffective??
© JJ Zambrowski - May 2007 60Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
The Decision Maker’s View on PE Evaluation
1.1. SScepticismcepticism: : “Economic evaluation is a tool for obtaining higher prices, increased sales and hiding lack of effectiveness data. Anything can be proven with it.”
2.2. Keep on working in Keep on working in isolated budgetsisolated budgets ::““hospitalhospital savingssavings are are notnot interestinginteresting forfor meme””
3.3. DDilemmailemma of evaluating a drug when not yet all of evaluating a drug when not yet all knowledge is availableknowledge is available
4.4. IfIf allall the the aboveabove is is solvedsolved: : whatwhat is is costcost--effectiveeffectiveand and whatwhat is is notnot ??

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 11
© JJ Zambrowski - May 2007 61Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Apply thresholds
NL: 20,000 €/LYUK: 25,000 £/QALYCanada: 25,000-75,000 Can$/QALYUS: 50,000 $/QALY….
Other way: compare with other interventions in same area
The hard reality
Health care budgets are limited
© JJ Zambrowski - May 2007 63Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
How to Spend the same amount of money ?
A* to G*: Different treatments in different disease areaAll compared to “next best alternative” in their own area (A to G).
23,8106,30021.00100%150 M300500,000G*
20,00010,0000.1050%200 M200,0001,000F*
16,66712,0000.60100%200 M20,00010,000E*
15,62516,0003.201%250 M500,000500D*
20,46817,10019.0090%350 M1,000350,000C*
22,22218,0009.002%400 M100,0004,000B*
28,57121,0001.4025%600 M60,00010,000A*
C/EQALYQALY/patpat. imprimpactpatcost
source : Prof. Lieven Annemans - Health economist - Ghent University (Belgium)
1 extra Billion, 7 different treatments and diseases1 extra Billion, 7 different treatments and diseases
© JJ Zambrowski - May 2007 64Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
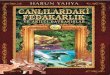
Where to Draw the Line ? Choice 1Choice 1Rank from most costRank from most cost--effective to least costeffective to least cost--effectiveeffective
23,8106,30021.00100%150 M300500,000G*
20,46817,10019.0090%350 M1,000350,000C*
22,22218,0009.002%400 M100,0004,000B*
28,57121,0001.4025%600 M60,00010,000A*
20,00010,0000.1050%200 M200,0001,000F*
16,66712,0000.60100%200 M20,00010,000E*
15,62516,0003.201%250 M500,000500D*
C/EQALYQALY/patpat. imprimpactpatcost
source : Prof. Lieven Annemans - Health economist - Ghent University (Belgium)
D+E+F+C=
1 Billion
D+E+F+CD+E+F+C==
1 Billion1 Billion
© JJ Zambrowski - May 2007 65Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Where to Draw the Line ? Choice 2Choice 2Rank from most costRank from most cost--effective to least costeffective to least cost--effectiveeffective
But : number of patients ! budget impact !
23,8106,30021.00100%150 M300500,000G*
20,46817,10019.0090%350 M1,000350,000C*
22,22218,0009.002%400 M100,0004,000B*
28,57121,0001.4025%600 M60,00010,000A*
20,00010,0000.1050%200 M200,0001,000F*
16,66715,0000.60100%250 M25,00010,000E*
15,62548,0003.201%750 M1,500,000500D*
C/EQALYQALY/patpat. imprimpactpatcost
source : Prof. Lieven Annemans - Health economist - Ghent University (Belgium)
Solutions: societal willingness to pay = constant ? Budget increase ? price reduction ?; Better selection of patients ?…
Solutions: societal willingness to pay = constant ? Budget increase ? price reduction ?; Better selection of patients ?…
D+E=
1 Billion
D+ED+E==
1 Billion1 Billion
© JJ Zambrowski - May 2007 66Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Discussion
There is more than just cost-effectivenessHealth economic evaluations do not replace decision making, they are just an extra element.Not only drugs, but also medical management can be assessed this way.In countries with a state-controlled health insurance, decisions will often still remain driven by political choices, even if they are based on technical issues .

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 12
How to Conduct Economic Evaluation Studies?
© JJ Zambrowski - May 2007 68Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Economic Evaluation Design
Models (decision trees, Markov models)Prospective: alongside clinical trial
Phase IIIa = “Superposed*”: artificial environmentPhase IIIb, IV: “Observational”: real environment
Retrospective: real costsRetrolective: physician estimatesCombining different sources
E.g. a model, based on input from clinical trials, retrospective data, expert opinion.
* : "Piggy-back" evaluations
© JJ Zambrowski - May 2007 69Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Prospective research for economic evaluation: different aspects
Environment, protocol requirementsEnvironment, protocol requirementsResultsResultsComparatorComparatorTime horizonTime horizonPatientsPatientsDropDrop--outsoutsStatistical analysisStatistical analysisValidityValidity
© JJ Zambrowski - May 2007 70Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Major differences clinical vs economic trial
ControlledControlledRegistrationRegistrationStrict protocol ordersStrict protocol ordersProtocol induced Protocol induced resource useresource useCompared to placebo or Compared to placebo or to to ““golden standardgolden standard””Avoid coAvoid co--morbiditiesmorbiditiesLimited timeLimited timeDropDrop--outs not outs not analysedanalysedHigh internal validity, low High internal validity, low external validityexternal validity
Real lifeReimbursement“Do what you normally do”Real resource use
Compared to relevant practiceInclude co-morbiditiesDrop-outs crucialTime should include all relevant costs and effectsHigh external validity, low High external validity, low internal validityinternal validity
© JJ Zambrowski - May 2007 71Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Pharmaco-economy today and tomorrow
Pharmaco- economic models are easy to conduct, fast, and relatively cheap.
Challenge: Make them Transparent, Make them as Credible as Clinical evidence.
© JJ Zambrowski - May 2007 72Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Pharmaco-economy today and tomorrow
Pharmaco- economic models are easy to conduct, fast, and relatively cheap.
Challenge: Make them Transparent, Make them as Credible as Clinical evidence.
WHO BMJ series - 2005
Follow the policy suggested by WHOFollow the policy suggested by WHOCHOICECHOICE
CHOoCHOosese IInterventions that are nterventions that are CCost ost EEffectiveffective

Principles and Methods of Health EconomicsTheir role in the Evaluation of Medical Practice
Jean-Jacques Zambrowski MD, PhD
Istanbul – May 2007 © Jean-Jacques Zambrowski 13
© JJ Zambrowski - May 2007 73Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
ConclusionsConclusions
Medical Care should be based on evidences.Medical Care should be based on evidences.Evidence Based Medicine should also include Evidence Based Medicine should also include an economic constituent.an economic constituent.Choices in daily practice should be based Choices in daily practice should be based
first, on relevant clinical evidencefirst, on relevant clinical evidencethen, if efficacy, safety and quality of care are equal, then, if efficacy, safety and quality of care are equal,
on theon the globalglobal cost cost from the patient's perspectivefrom the patient's perspectivefrom the health insurance perspectivefrom the health insurance perspectivefrom the community's perspectivefrom the community's perspective
© JJ Zambrowski - May 2007 74Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
ConclusionsConclusions
Finally, the issue is simple :Finally, the issue is simple :Since there is a shortage in resources Since there is a shortage in resources when compared to a fast increasing demand,when compared to a fast increasing demand,the choice is limited between 2 options :the choice is limited between 2 options :
To To rationalizerationalize healthcare offer and practiceshealthcare offer and practicesToTo rationration access to healthcareaccess to healthcare
Medical ethics dictate the choice for health Medical ethics dictate the choice for health professionals :professionals :
Offer and practices should be rationalized, Offer and practices should be rationalized, i.e. managed so as to ensure i.e. managed so as to ensure
better care better care at better cost. at better cost.
© JJ Zambrowski - May 2007 75Istanbul Istanbul PharmacoEconomyPharmacoEconomy MeetingMeeting
Merci de Merci de votrevotre attention !attention !
[email protected]@univ-paris5.fr
Teşekkür ederim dikatiniz için !