Embed Size (px)
Citation preview

Radiation Therapy RT 265HISTORY X-rays discovered in 1895Becquerel’s accidental experiment
showed the first radiobiological effects of x-rays
Experimentation of ram testicles revealed radiosensitivity of different tissues
Higher energy units available in 1950s and advent of linear accelerators
Basis of radiation for therapyElectromagnetic radiations release energy
indirectly to cause cellular damageX-rays and Gamma rays are similar in
action; their production is differentX-rays are produced extranuclearlyGamma rays produced intranuclearly

Production of radiation to cause effectDepth of irradiation depends on
radiation beam Lower energy beams affect skin Higher energy beams spares skin Difference between Cobalt-60 and
lower energy linear accelerators involves beam shape
Radiation Dose QuantificationRad has generally been replaced by GrayMeasurement of dose is difficult directlyAbsorbed dose is calculated based on
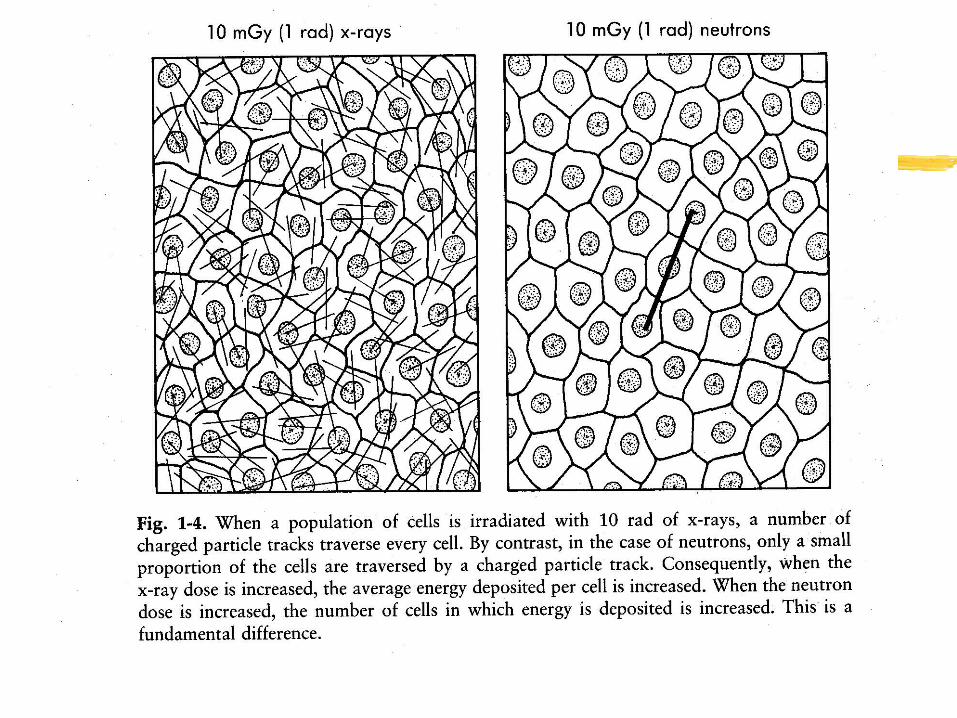
indirect measurements of ionization of airPattern of energy deposition varies with
types of particles causing cellular disruption
Effects on TumorsBoth malignant cells and normal cells
respond similarly to radiationBoth undergo repair of sublethal
damageBoth cell types are more sensitive
during the mitotic phaseOnly malignant cells have areas of
hypoxia - reason for fractionation
Systemic EffectsA value often used is LD50 which is the lethal dose for 50%
of the population sampleDeaths due to total body exposureWhen TBI used before bone marrow transplant interstitial
pneumonitis is the limiting factorEffects on immune reactions varyDepressions generally occur only when large tumors are
irradiated or large surface areasNausea and vomiting secondary to irradiation or disease
processes Nausea that presents later during treatment may be
secondary to underlying disease process

RadiobiologyFractionationReassortment of cellsRepair of sublethal damageAccelerated repopulation
FractionationSingle prolonged dose has profound
effects on normal tissuesStudies on spermatogenesis of ramsReason for fractionation - allows tumor
cells to reassort into the mitotic phaseReduces hypoxia while sparing normal
tissues
ReassortmentCells more radiosensitive in mitosis
or late in G2Survival curve is steep in these
stagesFractionation permits cells to
reassort themselves into more sensitive phases of the cell cycle to allow better killing
Sublethal Damage RepairMolecular basis not understoodDefined as increase in survival when a
dose of radiation is splitThis feature is ubiquitous among cellsBecause of ability to repair damage
quickly, melanomas have been thought of as “relatively radioresistant”
Rationale for fractionationReassortment allows for better cell killingRepair of sublethal damage should be
minimizedReoxygenation allows for better cell
killingHyperfractionation used to minimize the
late effects of irradiation while increasing dose and tumor control

Tumor volume and control by dose of irradiationDifficult to extrapolate dataAssumptions must be made: - number of cells proportional to
volume - hypoxia does not vary with tumor size60 Gy leads to depopulation of
10,000,000,000 or regression of a 2 cm mass in 90% of patients
Sequelae of TreatmentAcute and late effectsMucositisDysphagiaOsteoradionecrosis increases with
irradiated volume and increased dose and proximity of dose to mandible
Lhermitte’s syndrome and transverse myelitis
BrachytherapyRadioactive sources placed close to the
targetTemporary and permanent implantsAdvantagesEntire tumor must be accessibleLymph node metastases preclude sole use
of brachytherapy
Radiotherapy Treatment Planning
PlanningSimulationTreatment
Every treatment using radiotherapy has to be rigorously planned. The planning process consists of three phases:
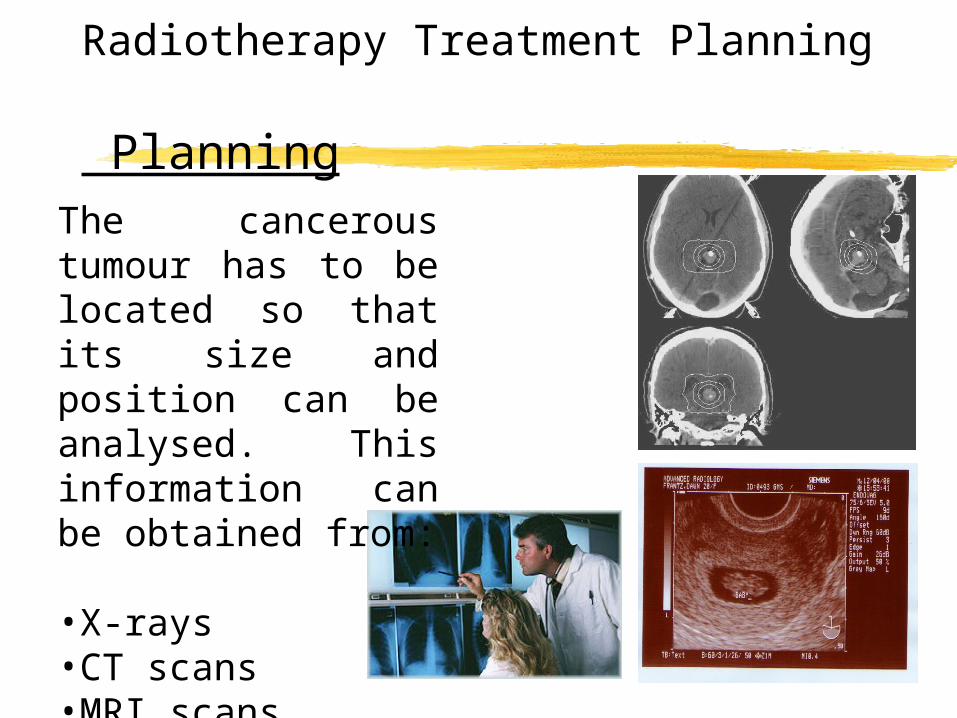
Radiotherapy Treatment Planning Planning
The cancerous tumour has to be located so that its size and position can be analysed. This information can be obtained from:
•X-rays•CT scans•MRI scans•Ultrasound images
Radiotherapy Treatment Planning Simulation
Once the amount of radiation to be given has been accurately calculated, the patient then goes to the simulator to determine what settings are to be selected for the actual treatment using a linear accelerator.
The settings are determined by taking a series of x-rays to make sure that the tumour is in the correct position ready to receive the ionising radiation.
Radiotherapy Treatment Planning Treatment
Irradiation using high energy gamma rays.
Irradiation using high energy x-rays.
Cancerous tumours can be treated using radiotherapy as follows:
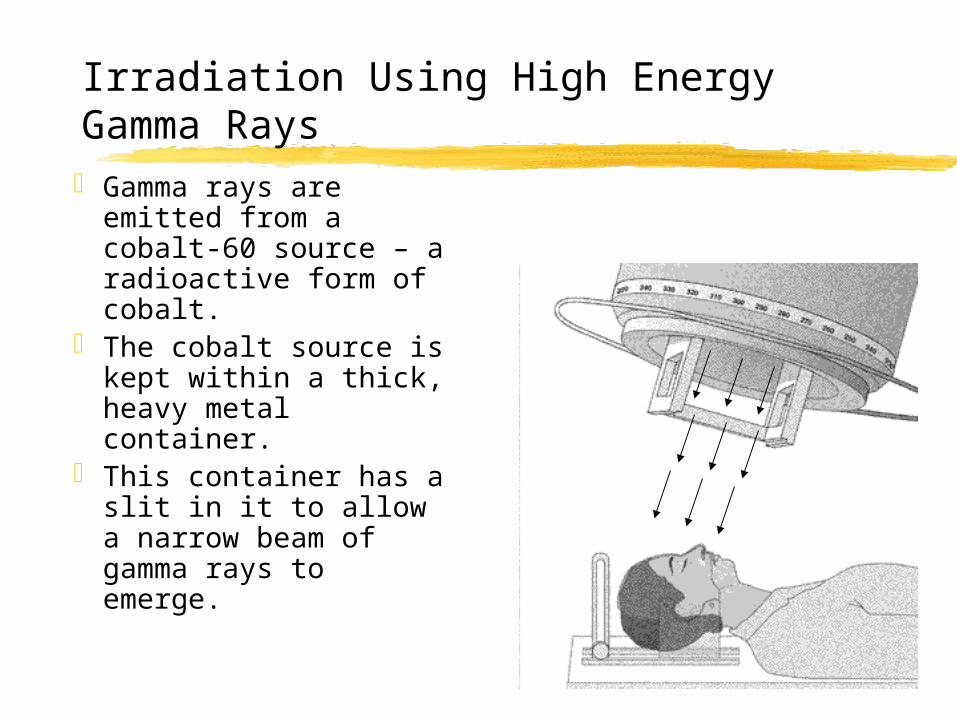
Irradiation Using High Energy Gamma Rays Gamma rays are
emitted from a cobalt-60 source – a radioactive form of cobalt.
The cobalt source is kept within a thick, heavy metal container.
This container has a slit in it to allow a narrow beam of gamma rays to emerge.
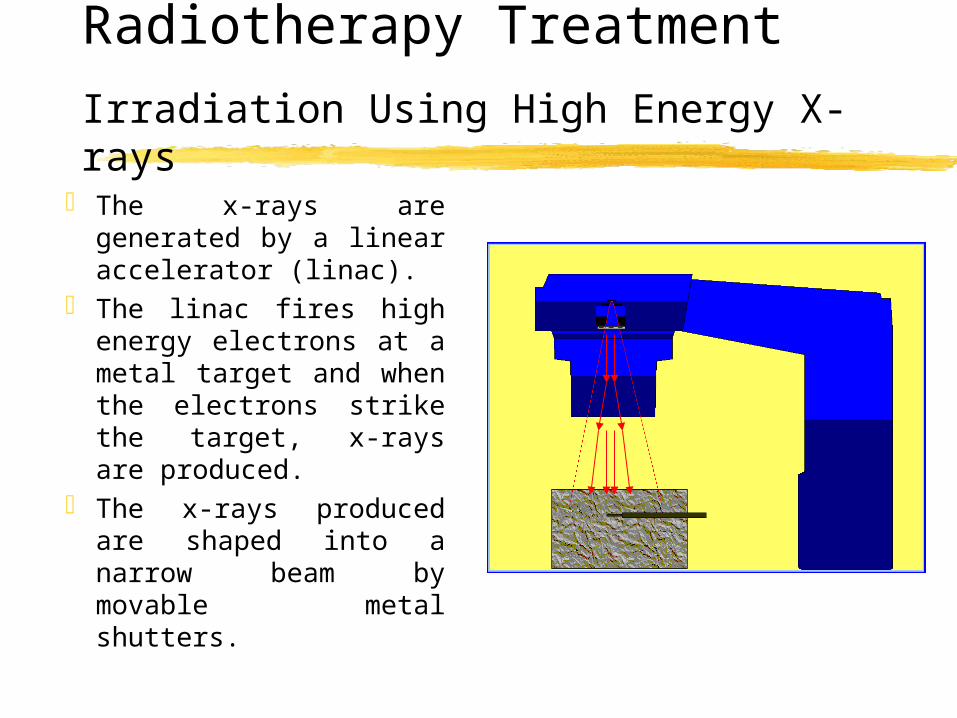
Radiotherapy TreatmentIrradiation Using High Energy X-rays
The x-rays are generated by a linear accelerator (linac).
The linac fires high energy electrons at a metal target and when the electrons strike the target, x-rays are produced.
The x-rays produced are shaped into a narrow beam by movable metal shutters.

Treatment of CancerRadiotherapy
The apparatus is arranged so that it can rotate around the couch on which the patient lies.
This allows the patient to receive radiation from different directions.
The diseased tissue receives radiation all of the time but the healthy tissue receives the minimum amount of radiation possible.
Treatments are given as a series of small doses because cancerous cells are killed more easily when they are dividing, and not all cells divide at the same time – this reduces some of the side effects which come with radiotherapy.
Radiation TherapyBrachytherapy
This involves placing implants in the form of seeds, wires or pellets directly into the tumour.
Such implants may be temporary or permenant depending on the implant and the tumour itself.
The benefit of such a method is that the tumour receives nearly all of the dose whilst healthy tissue hardly receives any.
Radiation TherapyBrachytherapy
UterusCervixProstateIntraocularSkinThyroidBone
Brachytherapy is used to treat the following cancers: