Embed Size (px)
Citation preview
Prof. dr. Burhanuddin Nasution, SpPK(K)
A. NEONATUS & IBU DIABETESPengendalian DM dengan insulin e ge da a de ga su→ kenaikan wanita DM yang bertahan hidup & melahirkan anakKarakteristik bayi :‐ Besar‐Makrosomia‐Morbiditas tinggi‐Mortalitas tinggi, lebih 5X ibu non DM
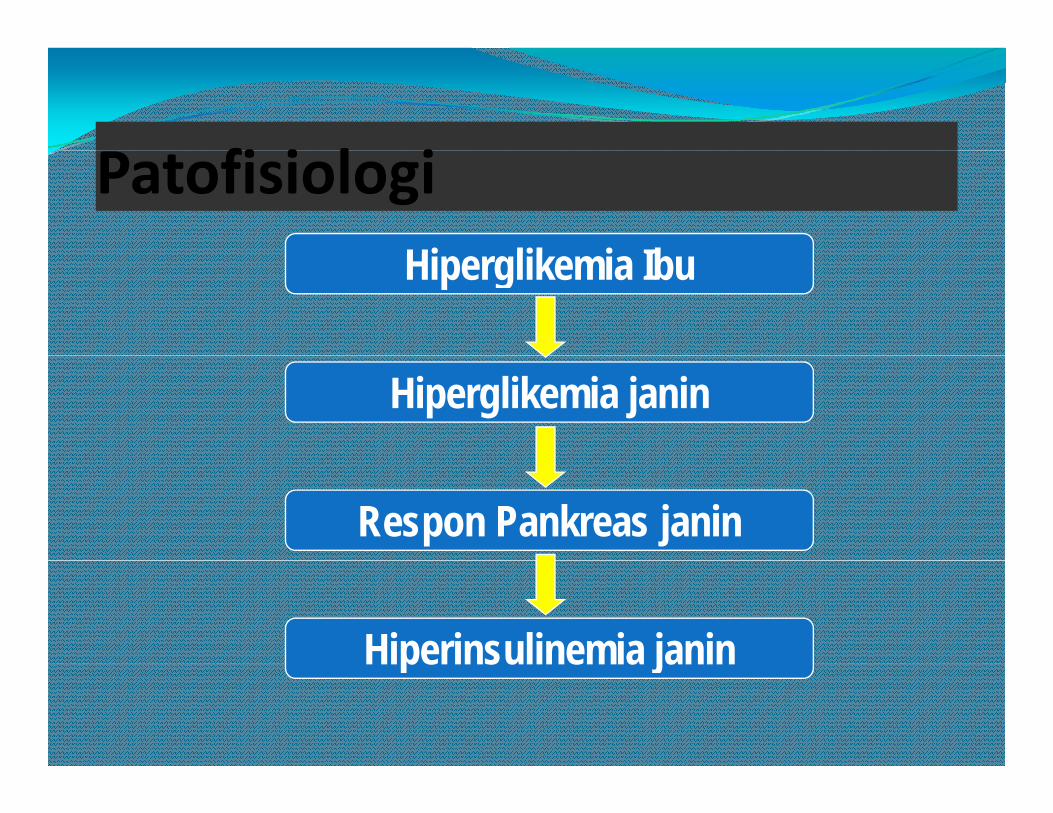
fi i l iPatofisiologiHi lik i IbHiperglikemia Ibu
Hiperglikemia janin
Respon Pankreas janin
Hiperinsulinemia janinHiperinsulinemia janin
Hiperinsulinemia - Hiperglikemiape su e a pe g e a
Ambilan glukose hepatik meningkat, sintesis glikogen meningkat, lipogenesis dan sintesis protein diperbesarHipertropi & hiperplasia P.P langerhansPenambahan berat plasenta & organ bayi kecuali otakHipertropi miokardiumPenambahan jumlah sitoplasma dalam sel hati
Hiperinsulinisme ⇒ Asidosis janin ⇒ angka lahir meninggal meningkatP l l k l k k Pelepasan plasenta ⇒ pemasukan glukose ke neonatus berkurang ⇒ hipoglikemia
75% bayi dari ibu diabetes dan25% bayi dari ibu menderita25% bayi dari ibu menderitadiabetes selama kehamilan Hipoglikemia
Kadar glukose neonatus 40 mg/dl dianggap batas Kadar glukose neonatus 40 mg/dl dianggap batas minimal :Lebih rendah dari 40 mg/dl ⇒ gangguan Lebih rendah dari 40 mg/dl ⇒ gangguan fungsi otakOtak bayi dapat menggunakan glukose padaOtak bayi dapat menggunakan glukose padakecepatan 4‐5 mg/100 gr berat otak/menitOtak neonatus cukup bulan beratnya 420 gr p y 4 gpada bayi 3½ kg, memerlukan glukose dgnkecepatan 20 mg/menitp g
B HIPERBILIRUBINEMIAB. HIPERBILIRUBINEMIA
Ikterus diawali pada usia2 minggu pertama pd 60% bayi cukup bulan & 80% bayi pre‐termIkterus terjadi karena akumulasi pigmen bilirubin yang larut lemak (indirek)Ikt bi l i d k ( /dl)Ikterus biasa mulai pada muka (5 mg/dl)Ikterus tengah abdomen (15 mg/dl)Ikt t l k k ki ( /dl)Ikterus telapak kaki (20 mg/dl)
Ikterus Fisiologis (Ikterus N t )Neonatorum)Normal kadar bilirubin direk dalam serum tali pusat adalah 1 3 mg/dl Kemudian naik dengan kecepatan kurang dari 5 1‐3 mg/dl. Kemudian naik dengan kecepatan kurang dari 5 mg/dl/24 jamIkterus terlihat :Ikterus terlihat :‐ Pada hari ke 2 s/d 3‐ Puncaknya pd hari ke 2 s/d 4 (kadar 5‐6 mg/dl)u ca ya pd a e s/d 4 ( ada 5 6 g/d )‐ Pada hari ke 5 s/d 7, turun s/d kadar 2 mg/dl
Hal ini terjadi diduga karena :j g‐ Pemecahan sel darah merah‐ Keterbatasan konjugasi oleh hatij g
Secara keseluruhan :
6‐7% bayi cukup bulan kadar bilirubin indireknya > 12 9 mg/dl12,9 mg/dlKurang dari 3% mempunyai kadar > 15 mg/dlKadar menurun s/d kadar normalKadar menurun s/d kadar normal( 1 mg/dl sesudah 10‐14 hari)
Faktor resiko untuk mengalami hiperbilirubinemia indirek adalahhiperbilirubinemia indirek adalah :
Diabetes pada ibuP t it
Trisomi 21S f l h tPrematuritas
Obat‐obatan(Vit. K, Novobiosin)
Sefal hematomInduksi OksitosinPemberian ASI( , )
Tempat yang tinggiPolisitemia
BB menurun (dehidrasi)Pembentukan tinja lambat
Laki‐laki
Hiperbilirubinemia indirek persisten sesudah 2 minggu, memberi kesan :
HemolisisDefisiensi glukuronil tranferase herediterIkterus ASIHipotiroid atauObstruksi usus
Penyebab ikterus diduga patologis bila :p g
Muncul pada usia 24 jam pertamaBilirubin serum naik > 5 mg/24 jamBilirubin serum > 12 mg/dl pada bayi cukup bulanAtau 10‐14 mg/24 jam pada bayi pre‐termBilirubin bereaksi direk lebih besar 1 mg/dl pada setiap saat
li i did kHemolisis diduga kuat
Bila retikukosit > 15%Kern ikterus terjadi pada saudara kandungnyaKern ikterus terjadi pada saudara kandungnyaBilirubin 5 mg/dl atau lebih

14
Newborn screening tests look for:Serious developmental, Genetic, Metabolic disorders
That important action can be taken during the critical time before symptoms develop.
15
How to Prepare for the TestHow to Prepare for the Test
Between 24 hours and 7 days old, Typically before the baby goes home from Typically before the baby goes home from the hospital.
16
Screening tests are used to detect aScreening tests are used to detect a number of disorders, including:
Amino acid metabolism disorders: Arginosuccinic acidemia Citrullinemia Homocystinuria Maple syrup urine disease Maple syrup urine disease Phenylketonuria (PKU) Tyrosinemia type ITyrosinemia type I
Congenital adrenal hyperplasia
17
Cystic fibrosis Galactosemia Glucose‐6‐phosphate dehydrogenase deficiency (G6PD)C i l h h idiCongenital hypothyroidism
18
The most common disordersThe most common disorders tested for are:
1. Cystic fibrosis2 Galactosaemia2. Galactosaemia3. Congenital hypothyroidism4 Phenylketonuria4. Phenylketonuria
19
Cystic fibrosisCystic fibrosis
Cystic fibrosis (CF) is a genetic disorder known to be an inherited disease of the secretory glands, including the glands that make mucus and sweatthe glands that make mucus and sweat.Cystic fibrosis affects males and females equally. (1:2500)(1:2500)
20
Signs and symptomsSigns and symptoms
Lung and sinus illnessGastrointestinal, liver and pancreatic diseaseEndocrine disease and growthInfertility
21
CauseCause
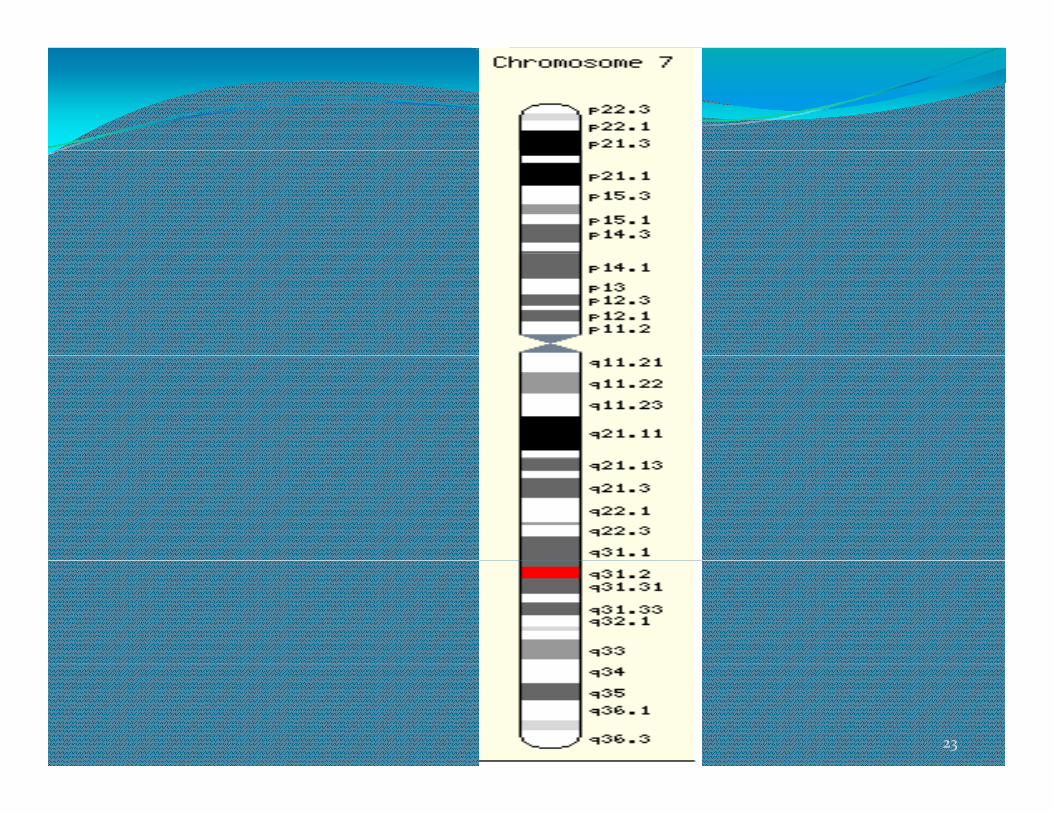
CF is caused by a mutation in the gene cystic fibrosis transmembrane conductance regulator (CFTR)Th CFTR i f d h l f The CFTR gene is found at the q31.2 locus of chromosome 7The product of this gene is a chloride ion channel The product of this gene is a chloride ion channel important in creating sweat, digestive juices and mucus.
22
23
DiagnosisDiagnosis
Newborn screening Sweat testing Genetic testing
Trypsinogen levels can be increasedP l i h C h i d f di d People with CF have increased amounts of sodium and chloride in their sweat. > 60 mmol/L ( < 40 mmol/L )Identification of mutations in the CFTR geneIdentification of mutations in the CFTR gene
24
GalactosaemiaGalactosemia is a rare genetic metabolic disorder that affects an individual's ability to metabolize the sugar galactose properlygalactose properly1 per 60,000 births
25
CauseCause
Lactose in food (such as dairy products) is broken down by the enzyme lactase into glucose and galactose In individuals with galactosemia the galactose. In individuals with galactosemia, the enzymes needed for further metabolism of galactose are severely diminished or missing entirely, leading to y g y, gtoxic levels of galactose in the blood, resulting in hepatomegaly (an enlarged liver), cirrhosis, renal f il t t b i d d i f il failure, cataracts, brain damage, and ovarian failure. Without treatment, mortality in infants with galactosemia is about 75%.g 75
26
DiagnosisA galactosemia test is a blood test (from the heel of the infant) or urine test that checks for three enzymes that are needed to change galactose a sugar that is found in are needed to change galactose‐a sugar that is found in milk and milk products‐into glucose, a sugar that your body uses for energyy gy
UDP galactose epimeraseGalactokinasegalactose‐1‐phosphate uridyl transferase
27
Congenital hypothyroidismCongenital hypothyroidism (CH) is a condition of thyroid hormone deficiency present at birth.A i l i b i fApproximately 1 in 4000 newborn infantssevere congenital hypothyroidism can lead to growth failure and permanent mental retardationfailure and permanent mental retardation.
28
Etiologyiodine deficiencyCongenital hypothyroidism can also occur due to
i d f f h i ii d h i genetic defects of thyroxine or triiodothyronine synthesis within a structurally normal glandAmong specific defects are thyrotropin (TSH) Among specific defects are thyrotropin (TSH) resistance, iodine trapping defect, organification defect, thyroglobulin, and iodotyrosine deiodinase y g ydeficiency.
29
Diagnostic Measurement of TSH or thyroxine (T4) on the second or third day of life. Th TSH i hi h h T lThe TSH is high, or the T4 low,
30
PhenylketonuriaPhenylketonuria
Phenylketonuria (PKU) is an autosomal recessive genetic disorder characterized by a deficiency in the hepatic enzyme phenylalanine hydroxylase(PAH)hepatic enzyme phenylalanine hydroxylase(PAH)This enzyme is necessary to metabolize the amino acid phenylalanine ('Phe') to the amino acid tyrosinephenylalanine ( Phe ) to the amino acid tyrosine.When PAH is deficient, phenylalanine accumulates and is converted into phenylpyruvate (also known as p y pyphenylketone), which is detected in the urine.
31
It can cause problems with brain development, leading to progressive mental retardation, brain damage, and seizuresseizures.Eliminating foods high in phenylalanine, such as meat, chicken fish nuts cheese legumeschicken, fish, nuts, cheese, legumes
32
PKU is normally detected using the HPLC test, but some clinics still use the Guthrie test,
i l d b N l h l i k)using samples drawn by Neonatal heel prick)musty odor" to the baby's sweat and urine (due to phenylacetate one of the ketones produced)phenylacetate, one of the ketones produced)
33





























