Embed Size (px)
Citation preview
Pharmacogenetics g
Prof. dr. Henk-Jan GuchelaarClinical Pharmacy & ToxicologyLeiden University Medical Centre
25th A t 200725th August 2007
Variability in drug response
• “more than 90% of the currently used drugs is effective in only 30-50% of the patients”
(Collins – The Independent 8 dec 2003)
2
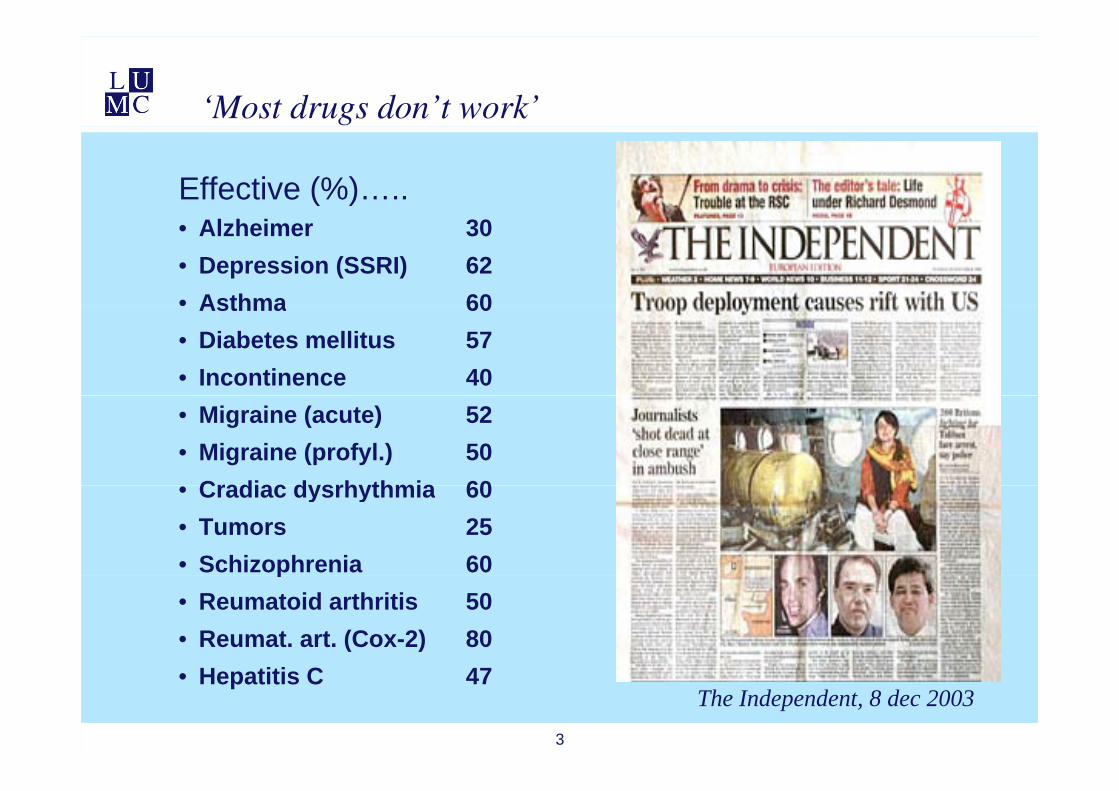
‘Most drugs don’t work’
Effective (%)…..• Alzheimer 30• Depression (SSRI) 62• Asthma 60Asthma 60• Diabetes mellitus 57• Incontinence 40• Migraine (acute) 52• Migraine (profyl.) 50
Cradiac dysrhythmia 60• Cradiac dysrhythmia 60• Tumors 25• Schizophrenia 60p• Reumatoid arthritis 50• Reumat. art. (Cox-2) 80
3
• Hepatitis C 47The Independent, 8 dec 2003
Variability in humans
4
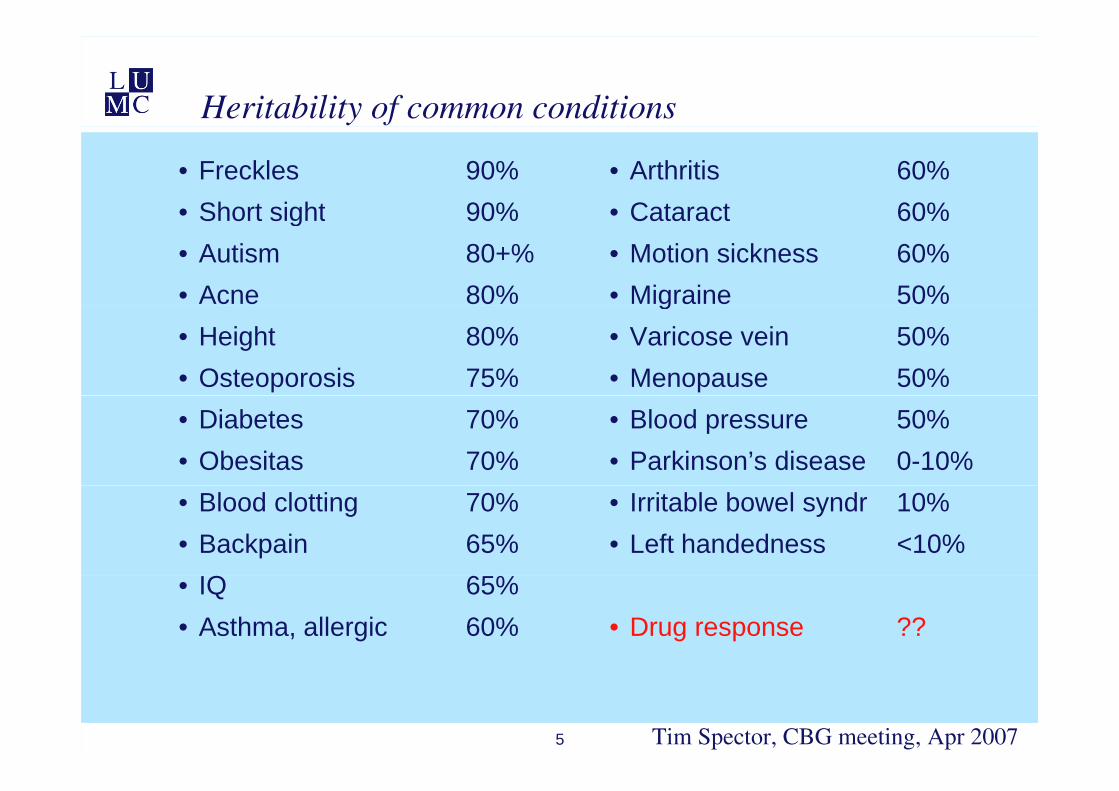
Heritability of common conditions
• Freckles 90%• Short sight 90%
• Arthritis 60%• Cataract 60%Short sight 90%
• Autism 80+%• Acne 80%
Cataract 60%• Motion sickness 60%• Migraine 50%
• Height 80%• Osteoporosis 75%
g• Varicose vein 50%• Menopause 50%
• Diabetes 70%• Obesitas 70%
• Blood pressure 50%• Parkinson’s disease 0-10%
• Blood clotting 70%• Backpain 65%
Q %
• Irritable bowel syndr 10%• Left handedness <10%
• IQ 65%• Asthma, allergic 60% • Drug response ??
5 Tim Spector, CBG meeting, Apr 2007
Gene-Environment interaction
6
Pharmacogenetics
• The heritability of drug response
• Individual pharmacotherapy
• Tailor made pharmacotherapyp py
• “Personal Pills”
7
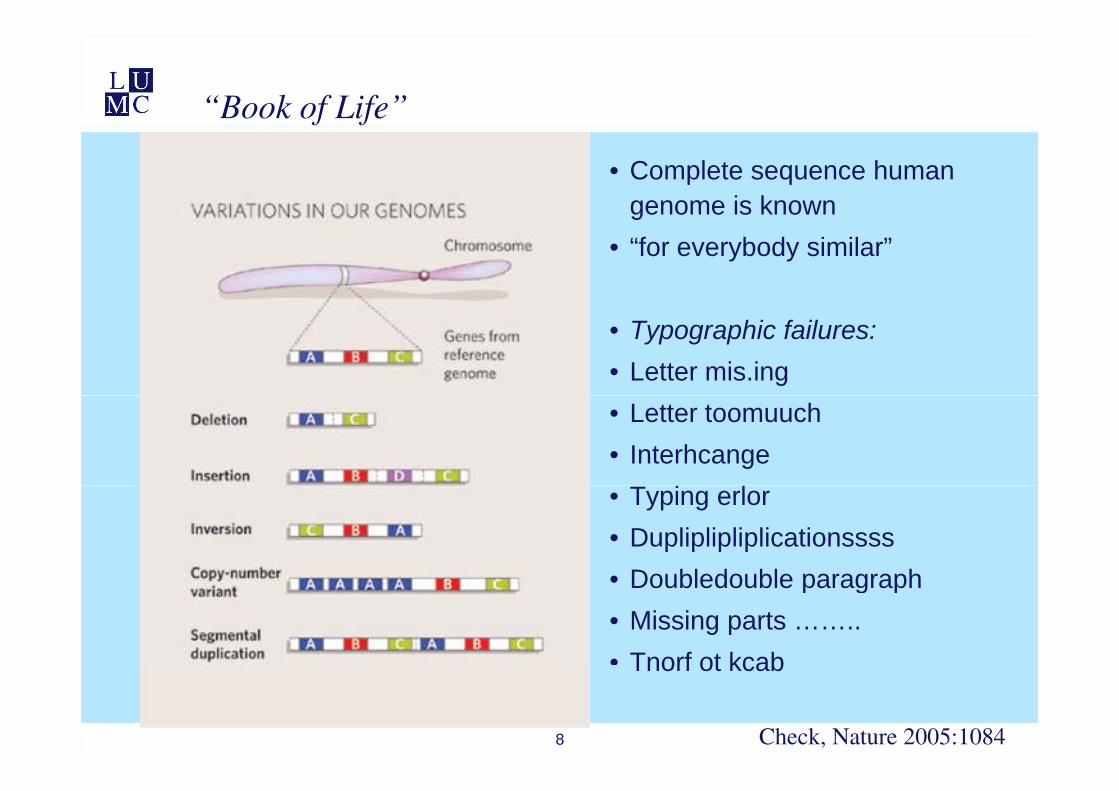
“Book of Life”
• Complete sequence human genome is knowng
• “for everybody similar”
• Typographic failures:• Letter mis.ing• Letter toomuuch • Interhcange• Typing erlor• Dupliplipliplicationssss
Doubledouble paragraph• Doubledouble paragraph• Missing parts ……..• Tnorf ot kcab
8
Tnorf ot kcab
Check, Nature 2005:1084
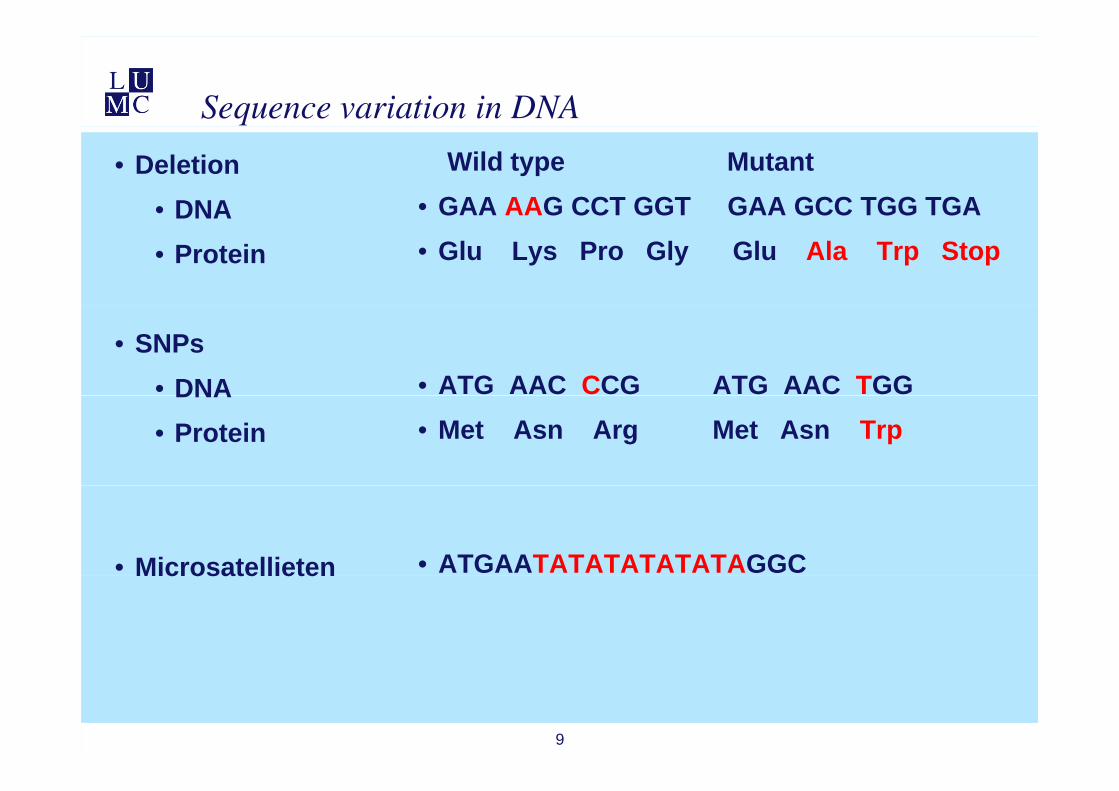
Sequence variation in DNA
• Deletion• DNA
Wild type Mutant• GAA AAG CCT GGT GAA GCC TGG TGADNA
• Protein • Glu Lys Pro Gly Glu Ala Trp Stop
• SNPs• DNA • ATG AAC CCG ATG AAC TGG DNA• Protein • Met Asn Arg Met Asn Trp
• Microsatellieten • ATGAATATATATATATAGGCMicrosatellieten
9
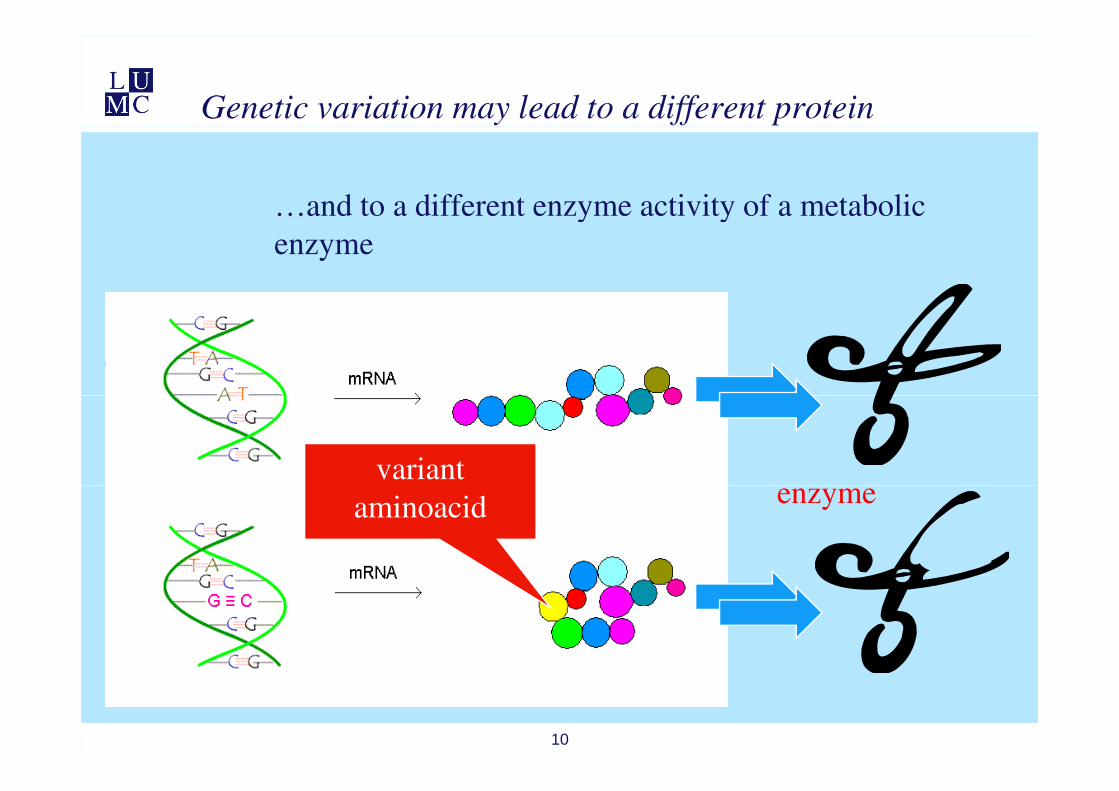
Genetic variation may lead to a different protein
…and to a different enzyme activity of a metabolic … y v y enzyme
variant aminoacid enzyme
10
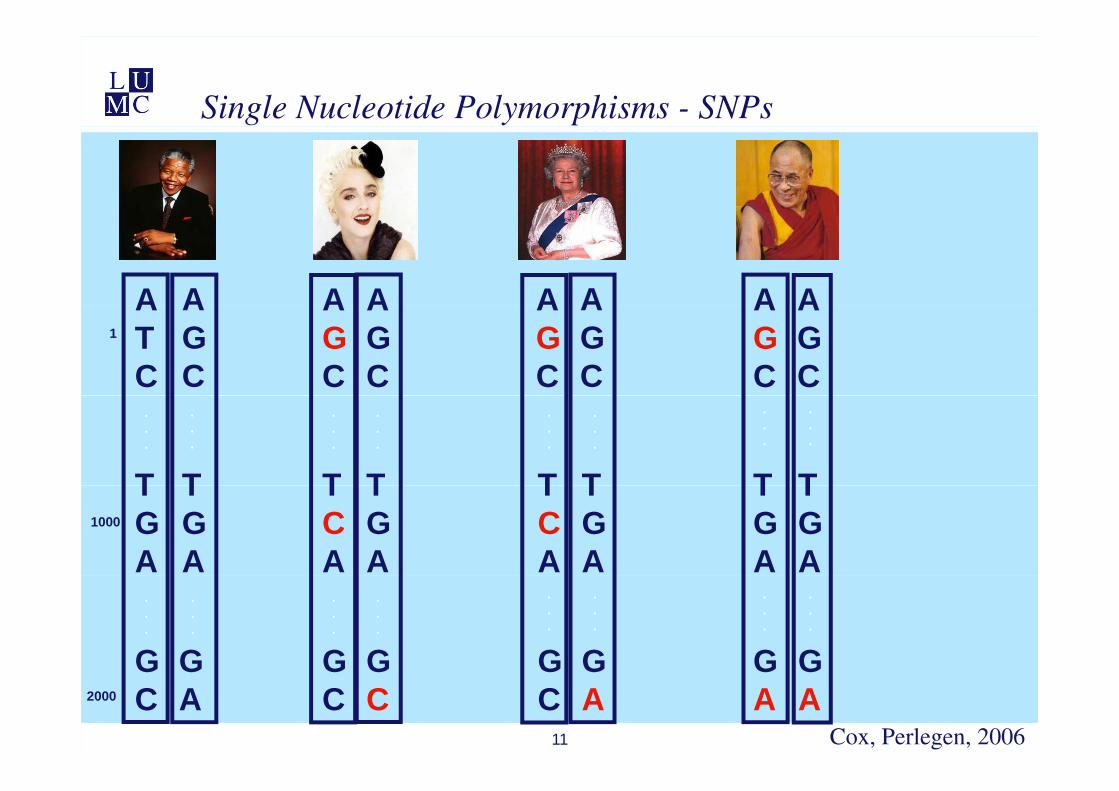
Single Nucleotide Polymorphisms - SNPs
A A A A A A A AATC
AGC
AGC
AGC
AGC
AGC
AGC
AGC
1
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
T T T T T T T TTGA
TGA
TCA
TGA
TCA
TGA
TGA
TGA
1000
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
G G G G G GG G
11
GC
GC
GC
GA
GA
GA
GA
GC2000
Cox, Perlegen, 2006
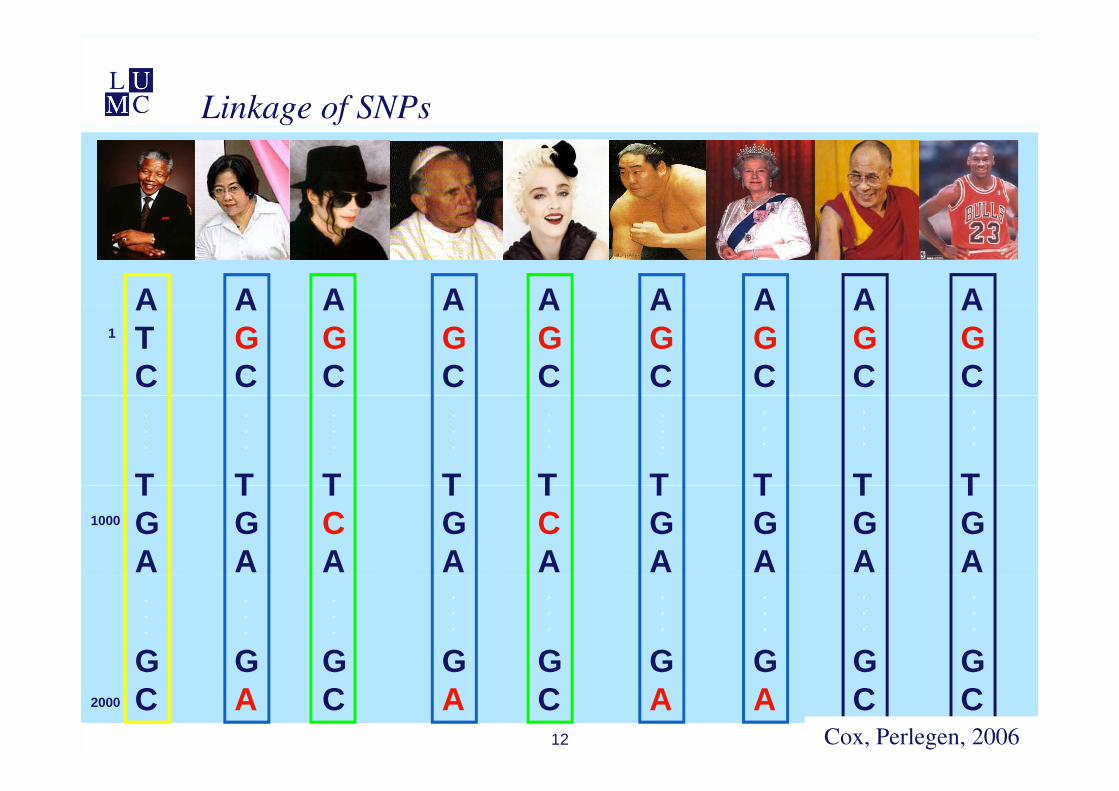
Linkage of SNPs
A A A A A A A A AATC
AGC
AGC
AGC
AGC
AGC
AGC
AGC
AGC
1
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
T T T T T T T T TTGA
TGA
TCA
TGA
TCA
TGA
TGA
TGA
TGA
1000
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
G G G G G G GG G
12
GC
GA
GC
GA
GA
GC
GC
GA
GC2000
Cox, Perlegen, 2006
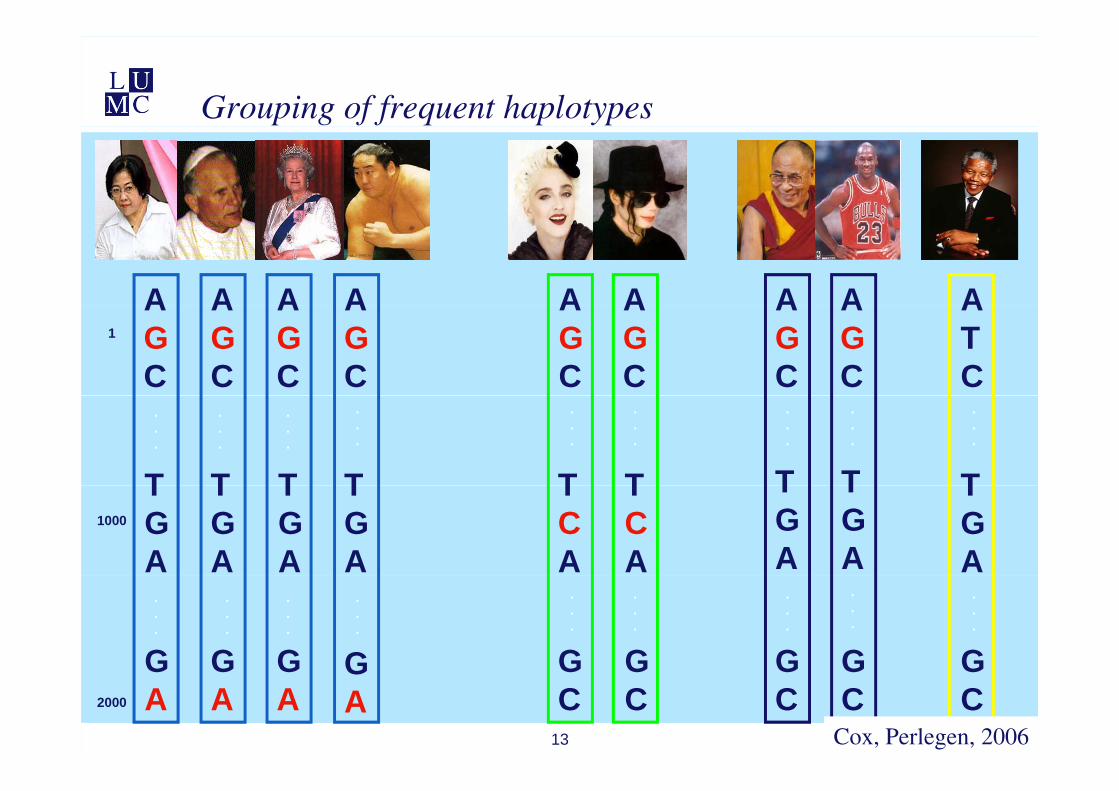
Grouping of frequent haplotypes
A A A A A A A A AAGC
AGC
AGC
AGC
AGC
AGC
AGC
AGC
ATC
1
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
T T T T T T T T TTGA
TGA
TGA
TGA
TCA
TCA
TGA
TGA
TGA
1000
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
.
G G G G G G GG G
13
GA
GA
GC
GC
GC
GC
GC
GA
GA2000
Cox, Perlegen, 2006
Pharmacogenetics into clinical practice
• FDA approved PGx tests
• Amplichip® – CYP2D6 and CYP2C19
• Invader® – UGT1A1 *28
14
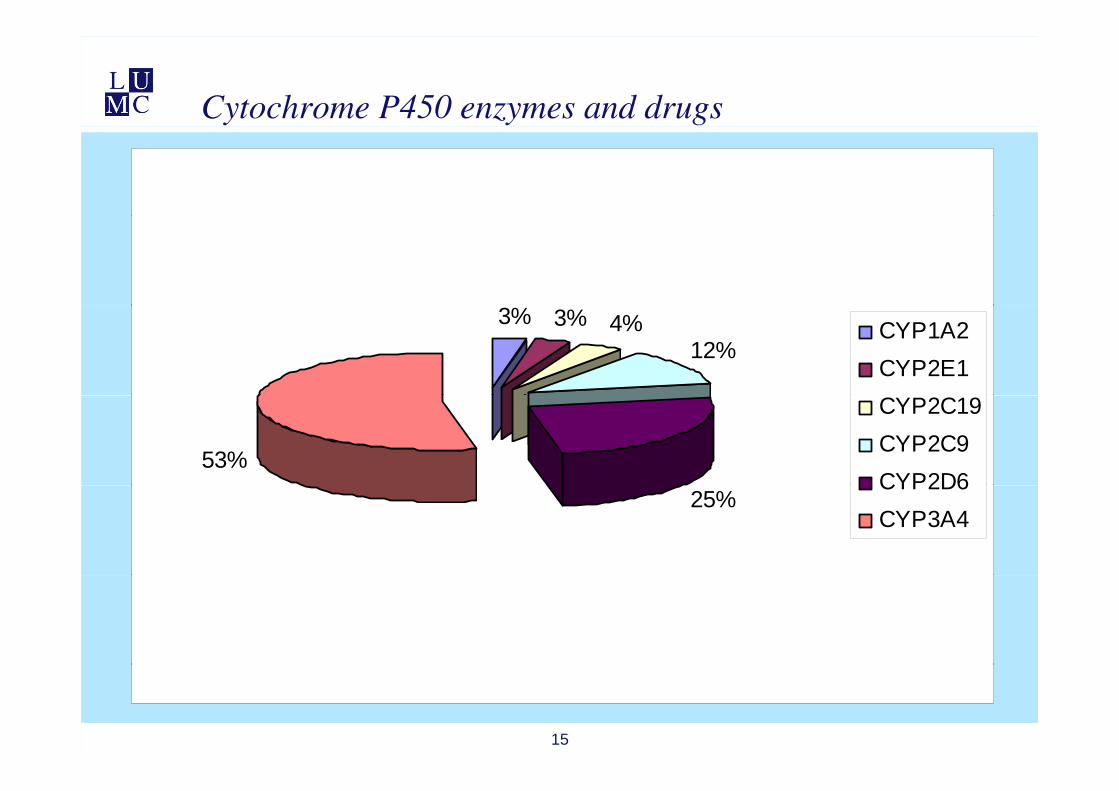
Cytochrome P450 enzymes and drugs
3% 3% 4%12%
CYP1A2CYP2E1
53%
CYP2C19CYP2C9CYP2D6
25%CYP2D6CYP3A4
15
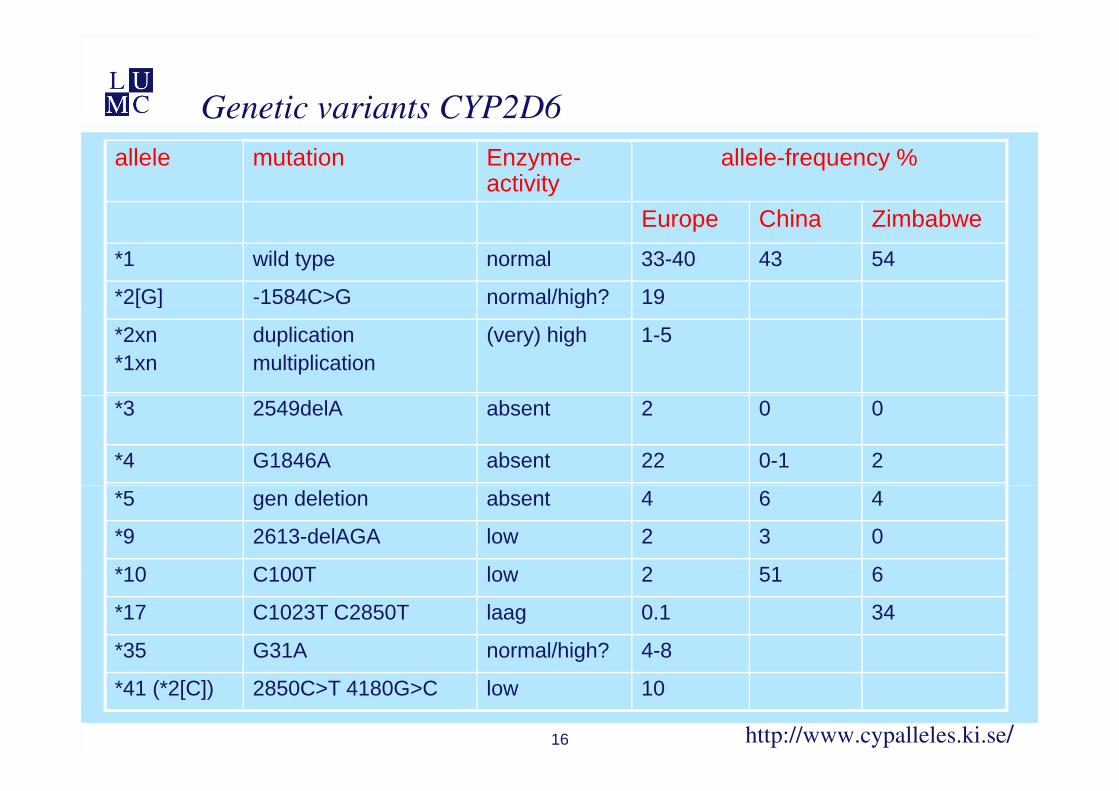
Genetic variants CYP2D6allele mutation Enzyme-
activityallele-frequency %
Europe China ZimbabweEurope China Zimbabwe*1 wild type normal 33-40 43 54
*2[G] -1584C>G normal/high? 19[ ] g
*2xn*1xn
duplicationmultiplication
(very) high 1-5
*3 2549delA absent 2 0 0
*4 G1846A absent 22 0-1 2
*5 gen deletion absent 4 6 4
*9 2613-delAGA low 2 3 0
*10 C100T low 2 51 610 C100T low 2 51 6
*17 C1023T C2850T laag 0.1 34
*35 G31A normal/high? 4-8
16
*41 (*2[C]) 2850C>T 4180G>C low 10
http://www.cypalleles.ki.se/
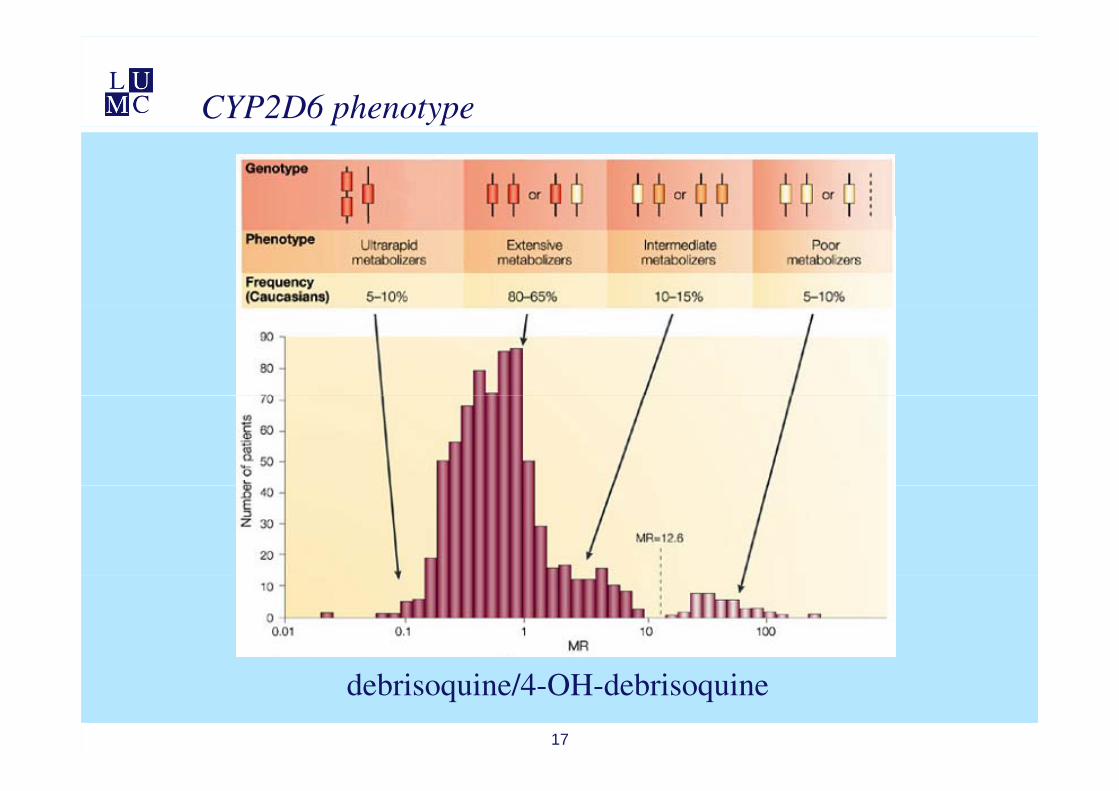
CYP2D6 phenotype
17
debrisoquine/4-OH-debrisoquine
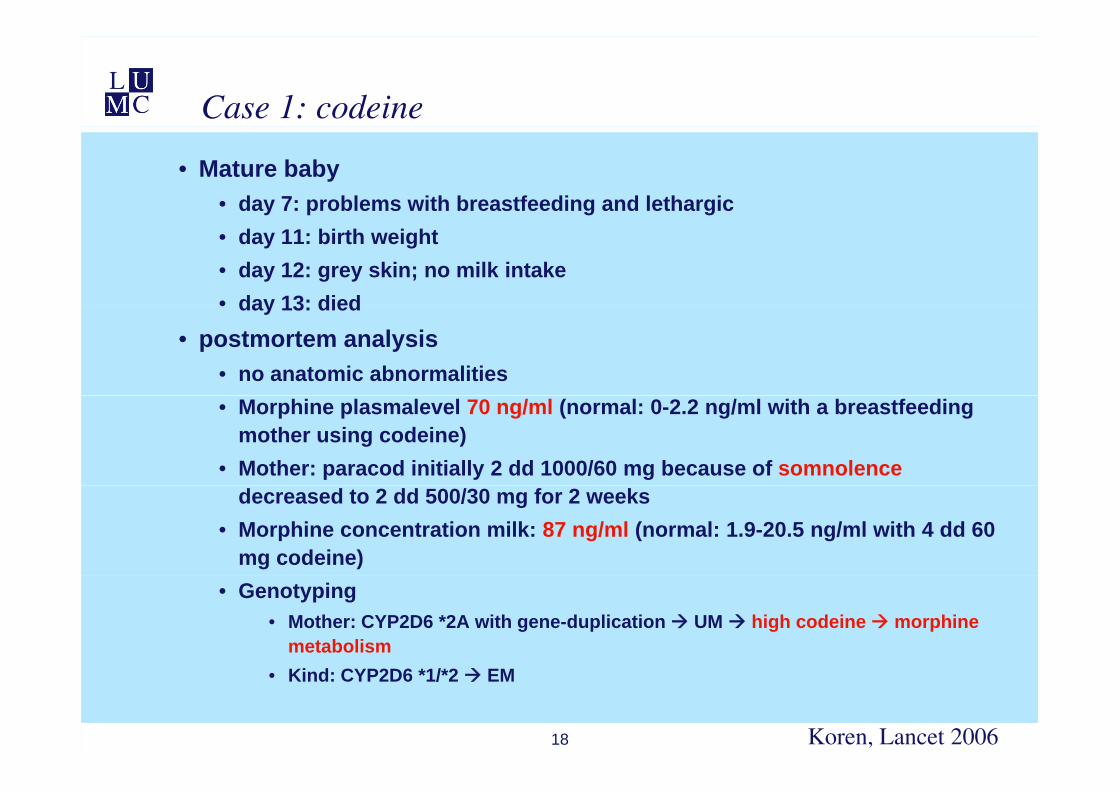
Case 1: codeine
• Mature baby• day 7: problems with breastfeeding and lethargic• day 11: birth weight• day 12: grey skin; no milk intake• day 13: died• day 13: died
• postmortem analysis• no anatomic abnormalities• Morphine plasmalevel 70 ng/ml (normal: 0-2.2 ng/ml with a breastfeeding
mother using codeine)• Mother: paracod initially 2 dd 1000/60 mg because of somnolence
decreased to 2 dd 500/30 mg for 2 weeks• Morphine concentration milk: 87 ng/ml (normal: 1.9-20.5 ng/ml with 4 dd 60
mg codeine)• Genotyping
• Mother: CYP2D6 *2A with gene-duplication UM high codeine morphine metabolism
18
• Kind: CYP2D6 *1/*2 EM
Koren, Lancet 2006

CYP2D6/2C19 variants and Chip technology
• 33 CYP2D6 variants
• 3 CYP2C19 variants
19
Affymetrix fluidic station 450Dx and Scanner 3000Dx
20
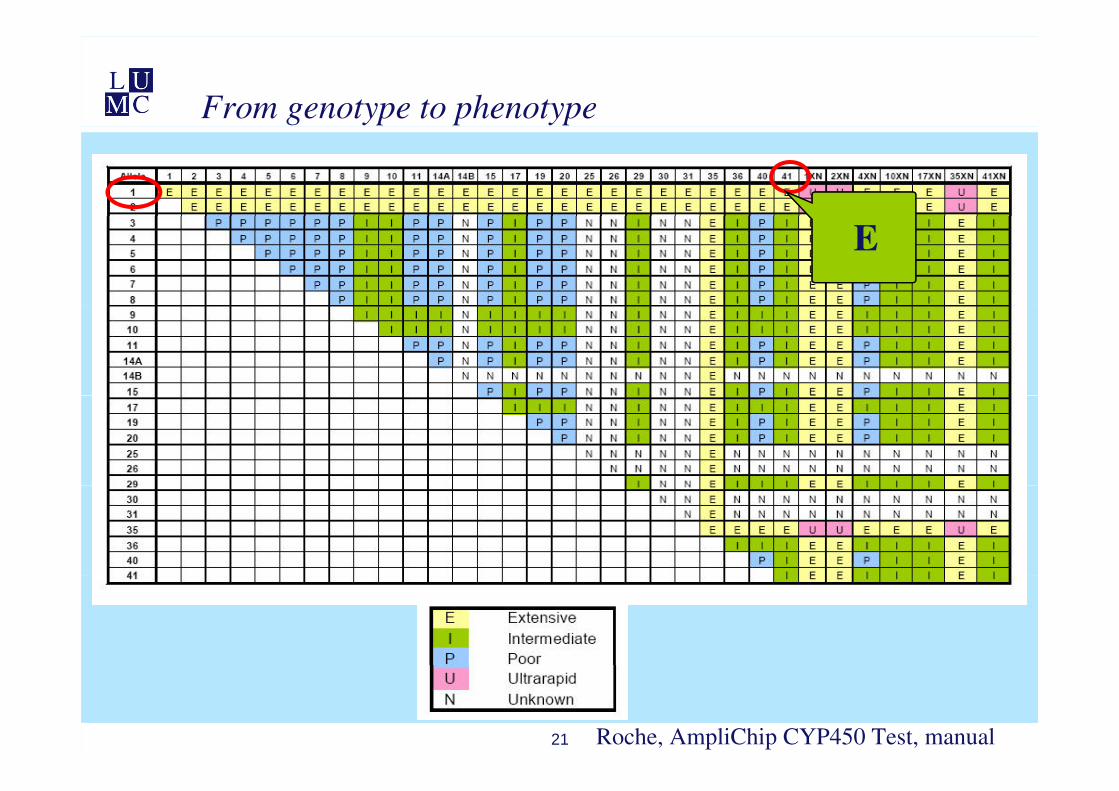
From genotype to phenotype
E
21 Roche, AmpliChip CYP450 Test, manual
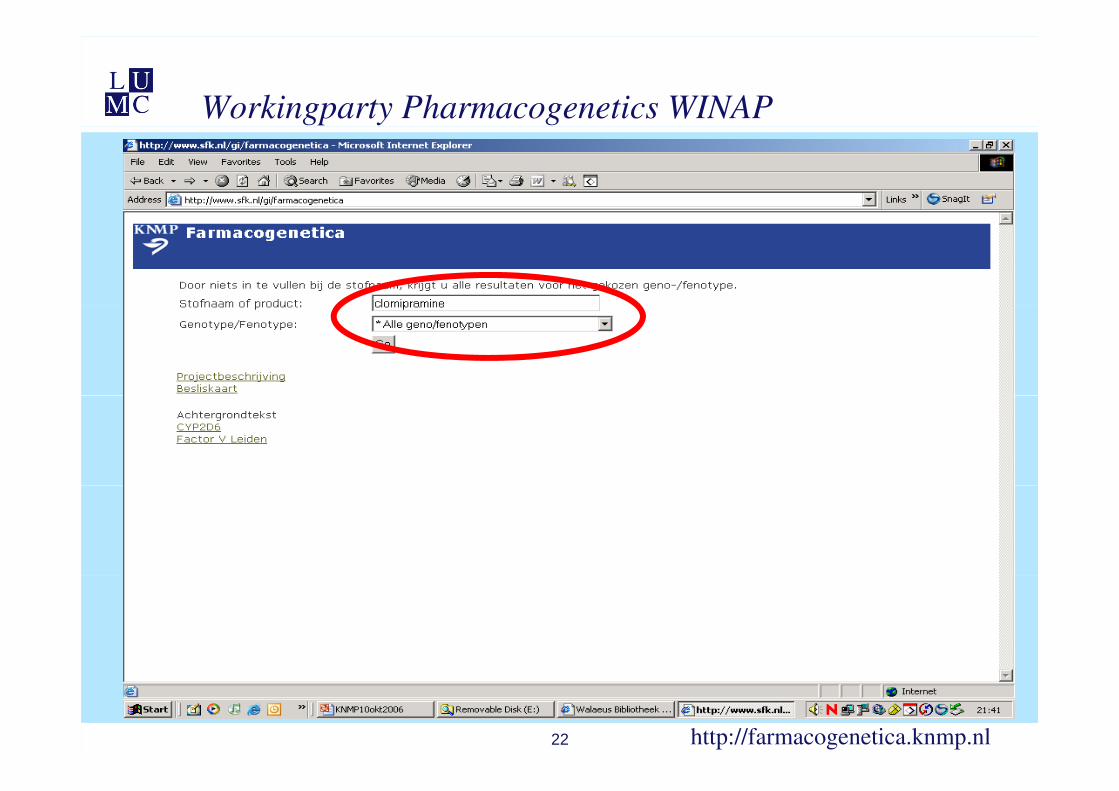
Workingparty Pharmacogenetics WINAP
22 http://farmacogenetica.knmp.nl
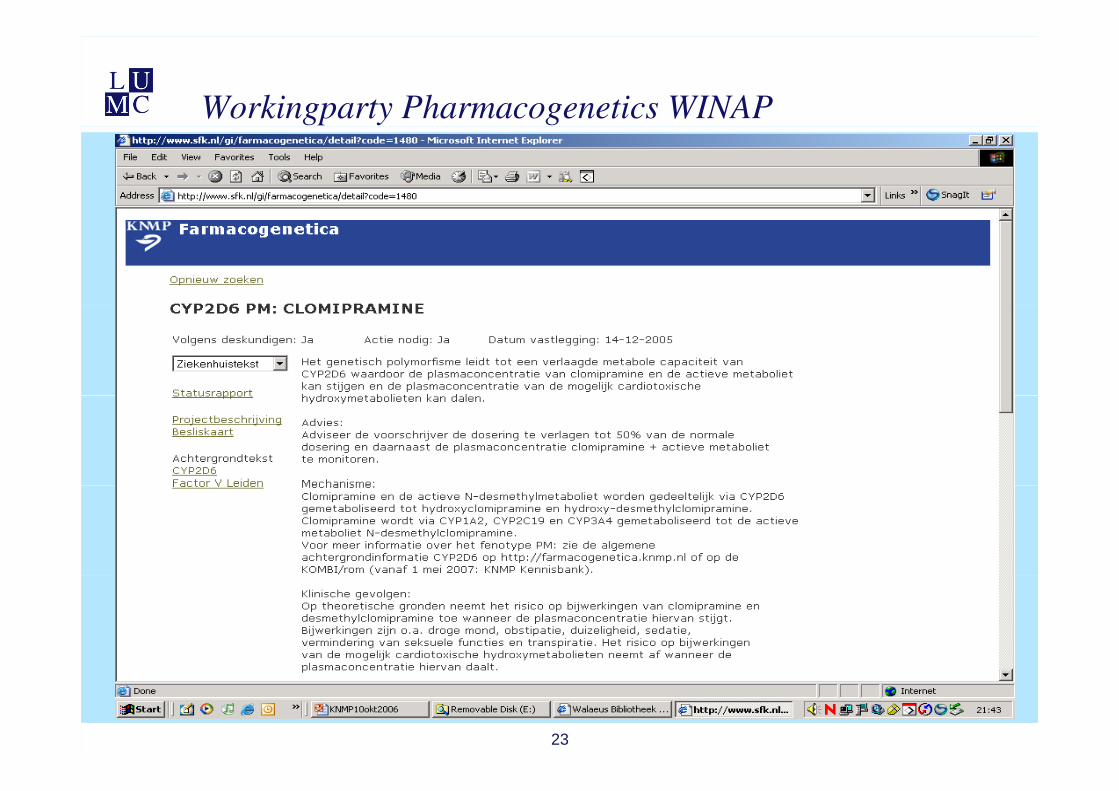
Workingparty Pharmacogenetics WINAP
23
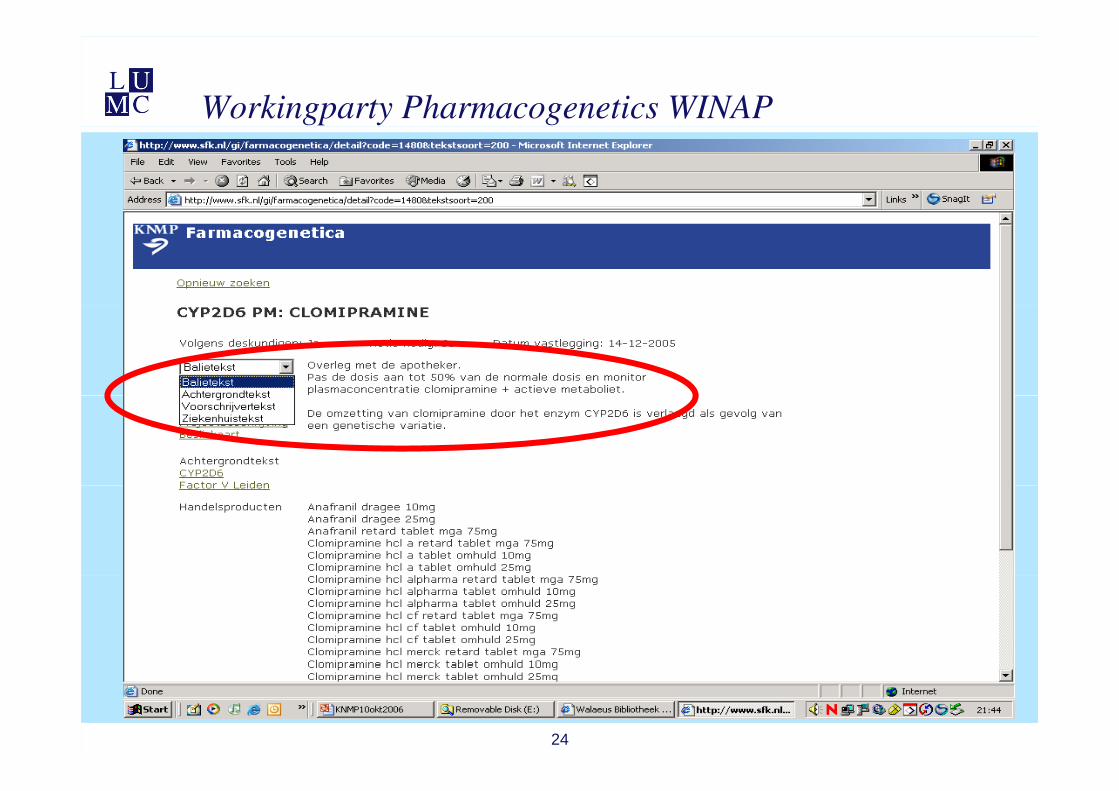
Workingparty Pharmacogenetics WINAP
24
Scientific evidence
• CYP2D6 and nortriptyline• search terms• search terms
• nortriptyline + CYP2D6 (‘only human’)• nortriptyline + debrisoquine• nortriptyline + debrisoquine• nortriptyline + sparteine• nortriptyline + dextromethorphan• nortriptyline + dextromethorphan• nortriptyline + metabolizer• nortriptyline + polymorph*• nortriptyline + polymorph• nortriptyline + IID6
• cross references• cross references
25 Swen, Guchelaar, Plos Med Aug 2007; e209
Scientific evidence
• Quality score:
• 4 controlled study; clinical relevant endpoint
• 3 controlled study; relevant surrogate endpoint
• 2 well documented case-report
• 1 incomplete case-report
• 0 animal or in vitro study or data on file
26 Swen, Guchelaar, Plos Med Aug 2007; e209
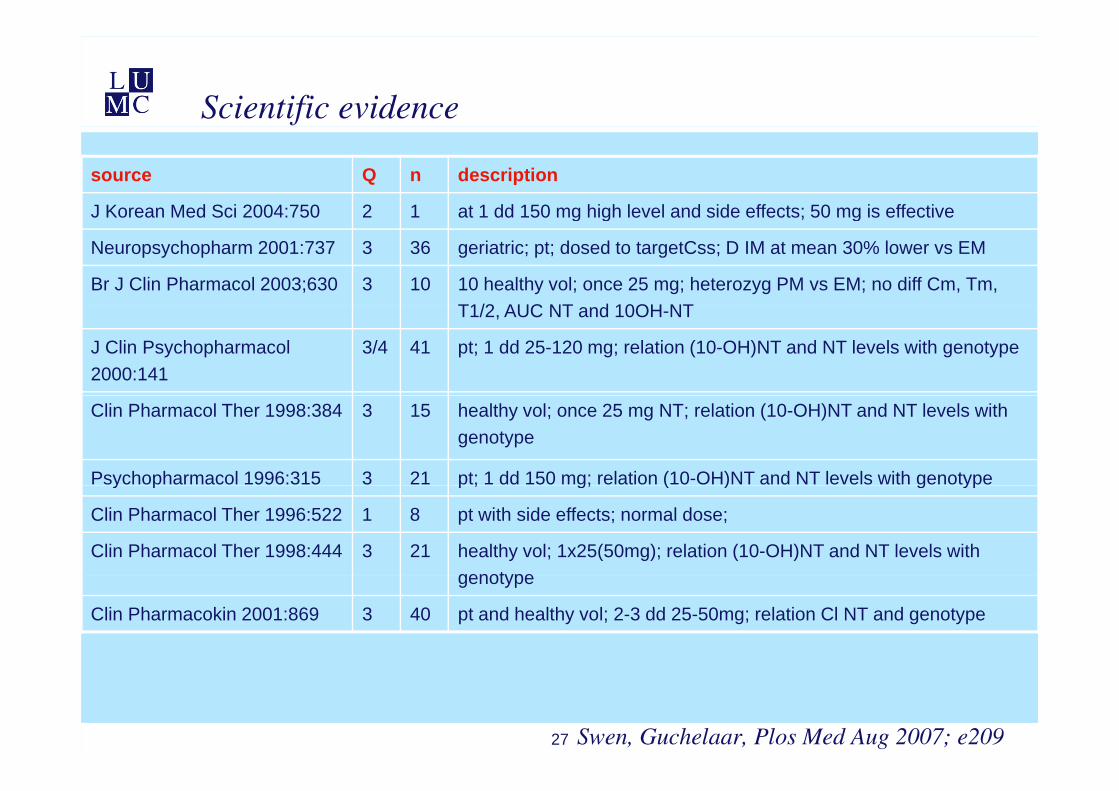
Scientific evidence
source Q n description
J Korean Med Sci 2004:750 2 1 at 1 dd 150 mg high level and side effects; 50 mg is effectiveJ Korean Med Sci 2004:750 2 1 at 1 dd 150 mg high level and side effects; 50 mg is effective
Neuropsychopharm 2001:737 3 36 geriatric; pt; dosed to targetCss; D IM at mean 30% lower vs EM
Br J Clin Pharmacol 2003;630 3 10 10 healthy vol; once 25 mg; heterozyg PM vs EM; no diff Cm, Tm, T1/2 AUC NT d 10OH NTT1/2, AUC NT and 10OH-NT
J Clin Psychopharmacol 2000:141
3/4 41 pt; 1 dd 25-120 mg; relation (10-OH)NT and NT levels with genotype
Clin Pharmacol Ther 1998:384 3 15 healthy vol; once 25 mg NT; relation (10-OH)NT and NT levels with genotype
Psychopharmacol 1996:315 3 21 pt; 1 dd 150 mg; relation (10-OH)NT and NT levels with genotypey p p ; g; ( ) g yp
Clin Pharmacol Ther 1996:522 1 8 pt with side effects; normal dose;
Clin Pharmacol Ther 1998:444 3 21 healthy vol; 1x25(50mg); relation (10-OH)NT and NT levels with genotypegenotype
Clin Pharmacokin 2001:869 3 40 pt and healthy vol; 2-3 dd 25-50mg; relation Cl NT and genotype
27 Swen, Guchelaar, Plos Med Aug 2007; e209
Clinical relevant application?
28
Tamoxifen label change
29
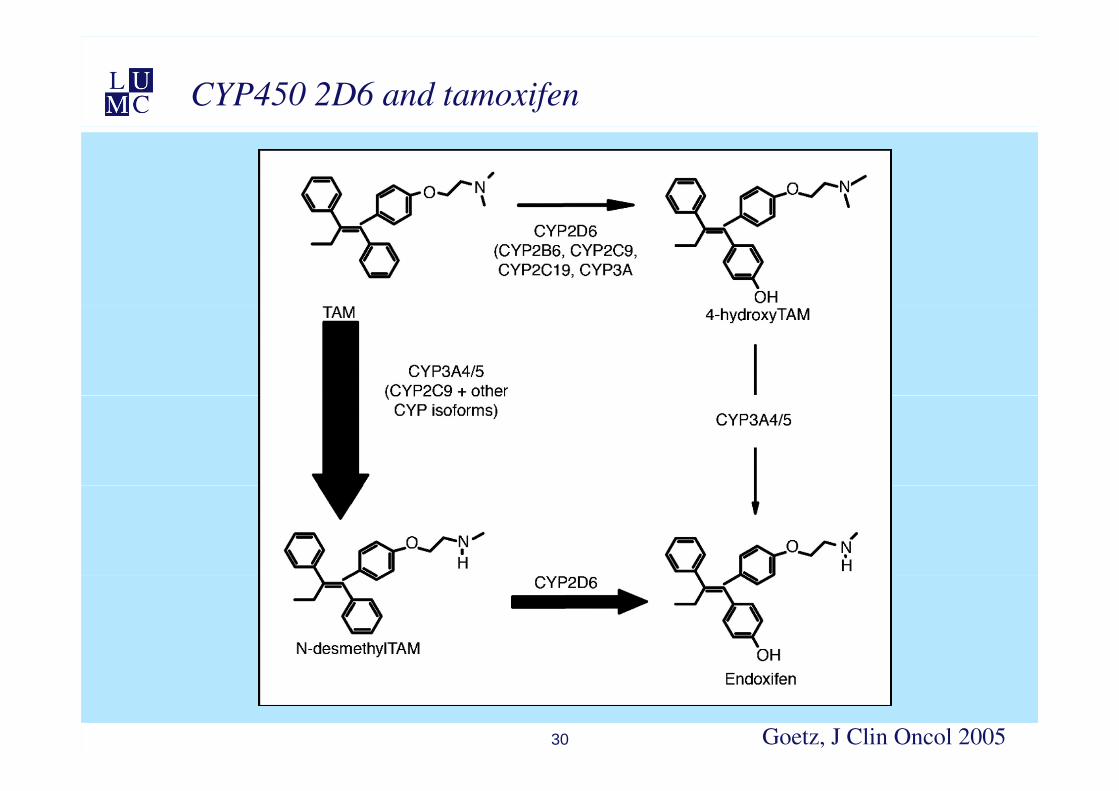
CYP450 2D6 and tamoxifen
30 Goetz, J Clin Oncol 2005
Pharmacogenetics into clinical practice
• FDA approved PGx tests
• Amplichip® – CYP2D6 and CYP2C19
• Invader® – UGT1A1 *28
31
UGT1A1 polymorphism and Irinotecan
32
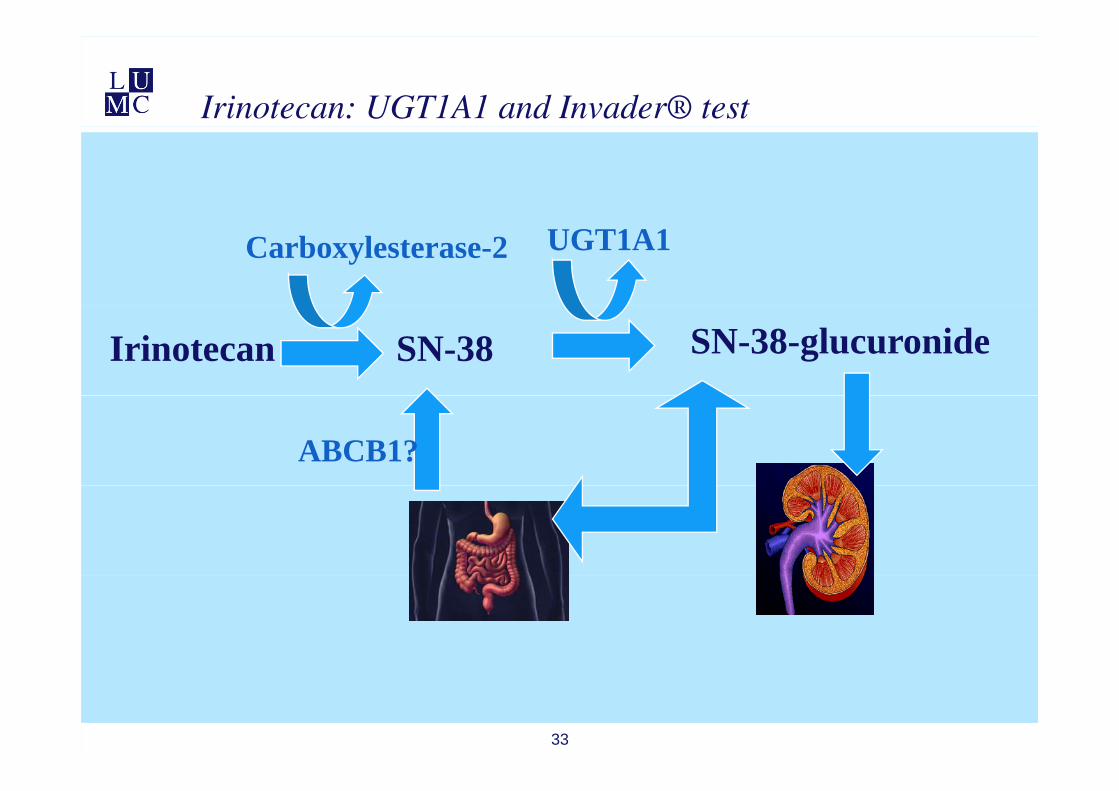
Irinotecan: UGT1A1 and Invader® test
Carboxylesterase-2 UGT1A1
Irinotecan SN-38 SN-38-glucuronide
ABCB1?
33
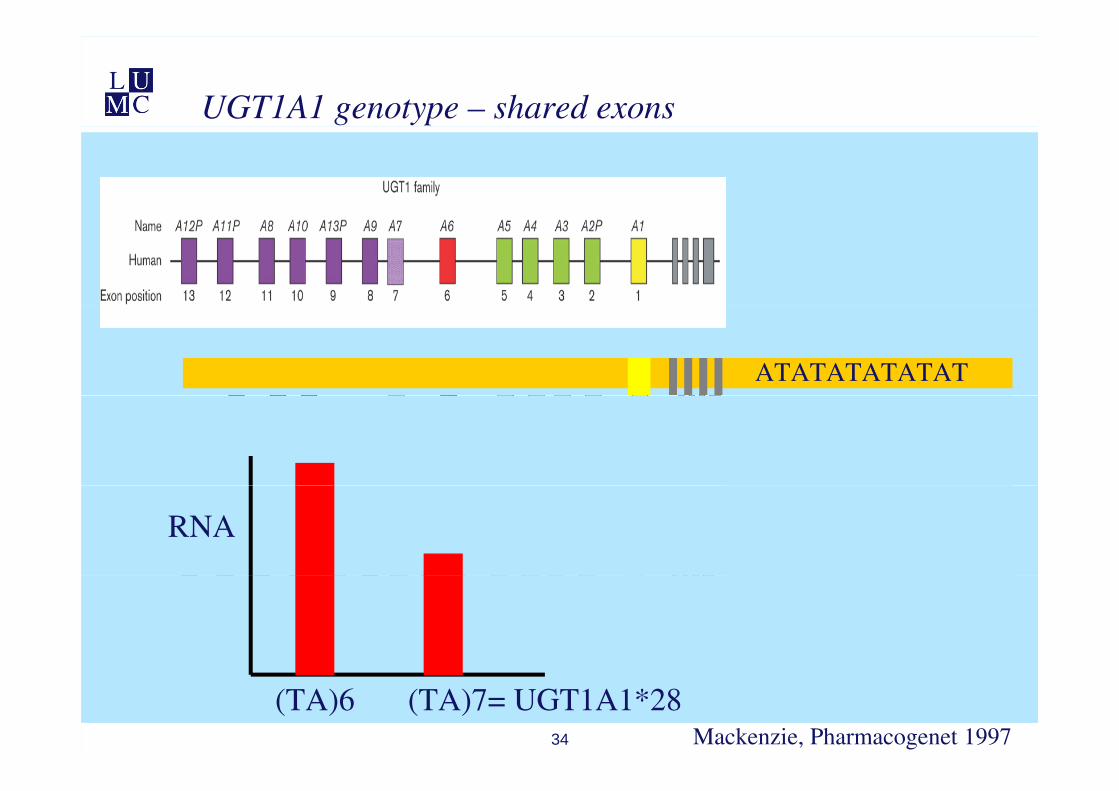
UGT1A1 genotype – shared exons
ATATATATATAT
RNA
34 Mackenzie, Pharmacogenet 1997
(TA)6 (TA)7= UGT1A1*28
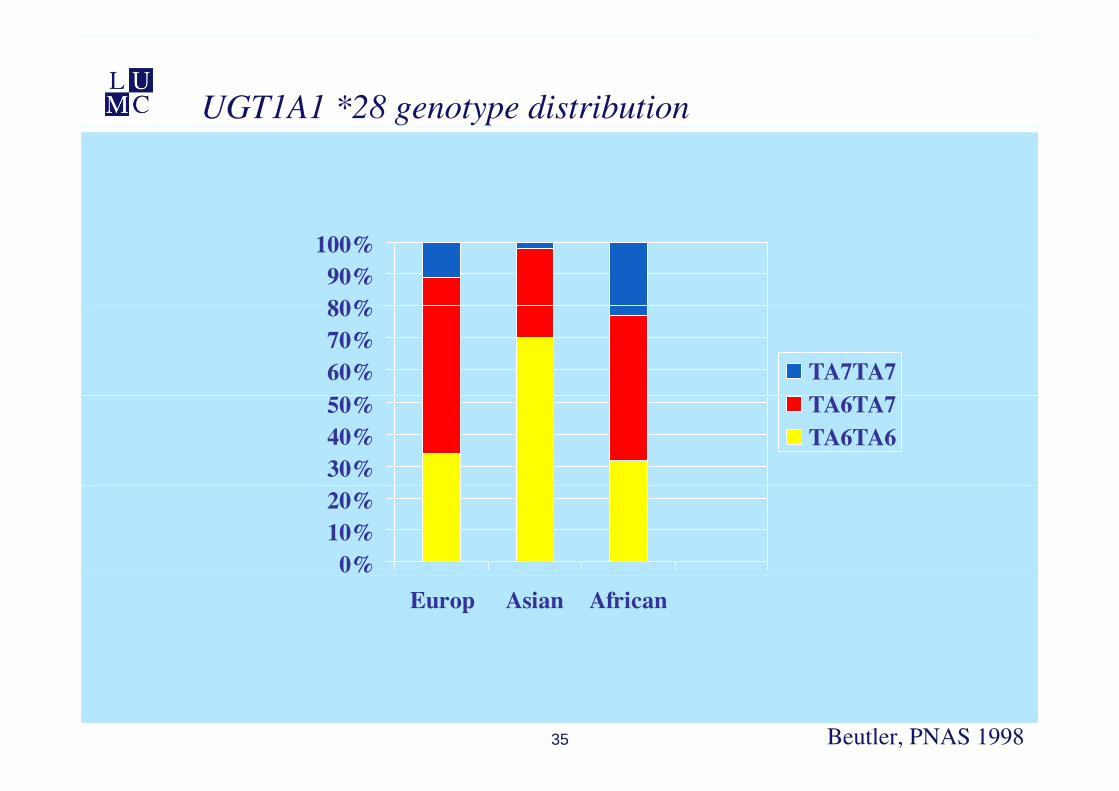
UGT1A1 *28 genotype distribution
80%90%
100%
60%70%80%
TA7TA7
30%40%50% TA6TA7
TA6TA6
0%10%20%
Europ Asian African
35 Beutler, PNAS 1998
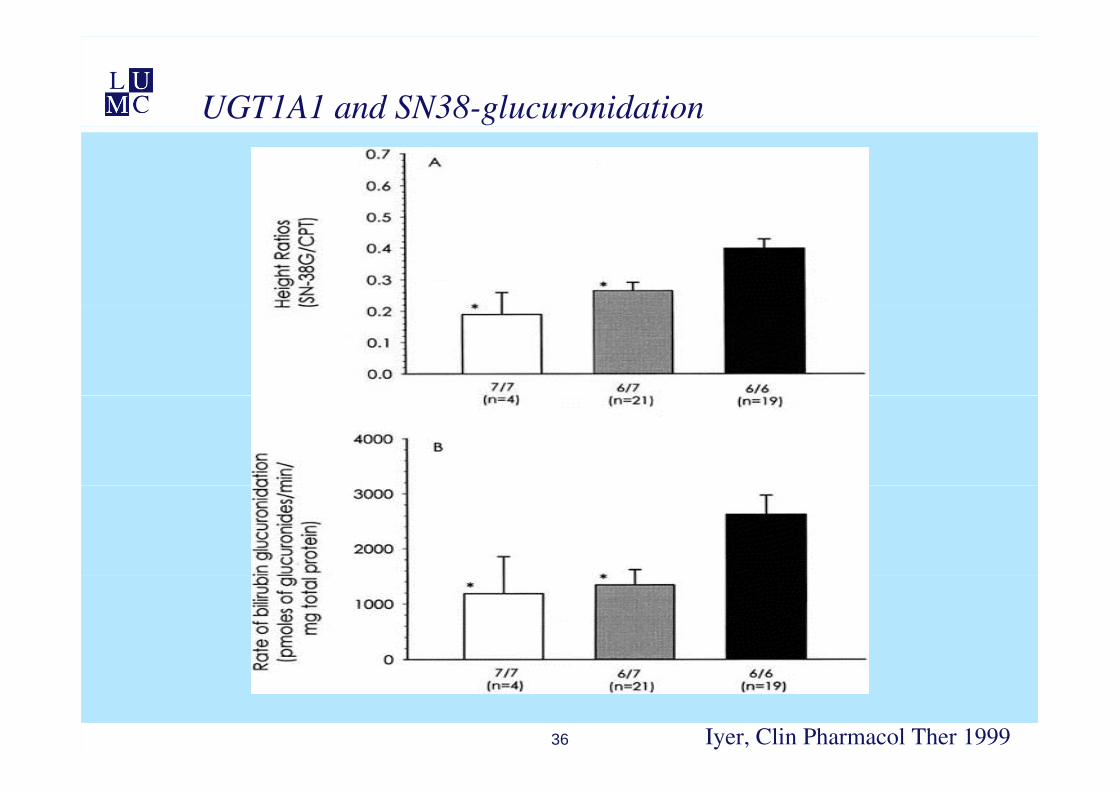
UGT1A1 and SN38-glucuronidation
36 Iyer, Clin Pharmacol Ther 1999
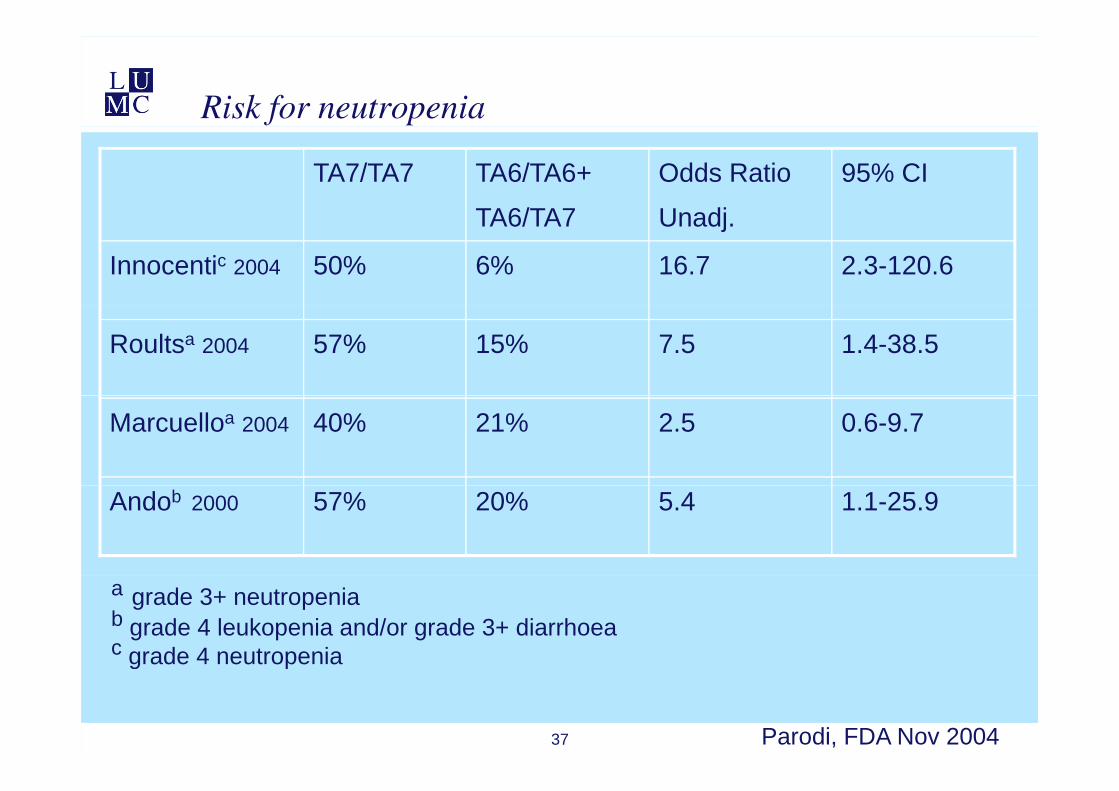
Risk for neutropenia
TA7/TA7 TA6/TA6+
TA6/TA7
Odds Ratio
Unadj
95% CI
TA6/TA7 Unadj.
Innocentic 2004 50% 6% 16.7 2.3-120.6
Roultsa 2004 57% 15% 7.5 1.4-38.5
Marcuelloa 2004 40% 21% 2.5 0.6-9.7
Andob 2000 57% 20% 5.4 1.1-25.9
a grade 3+ neutropeniab grade 4 leukopenia and/or grade 3+ diarrhoeac grade 4 neutropenia
37 Parodi, FDA Nov 2004
g p
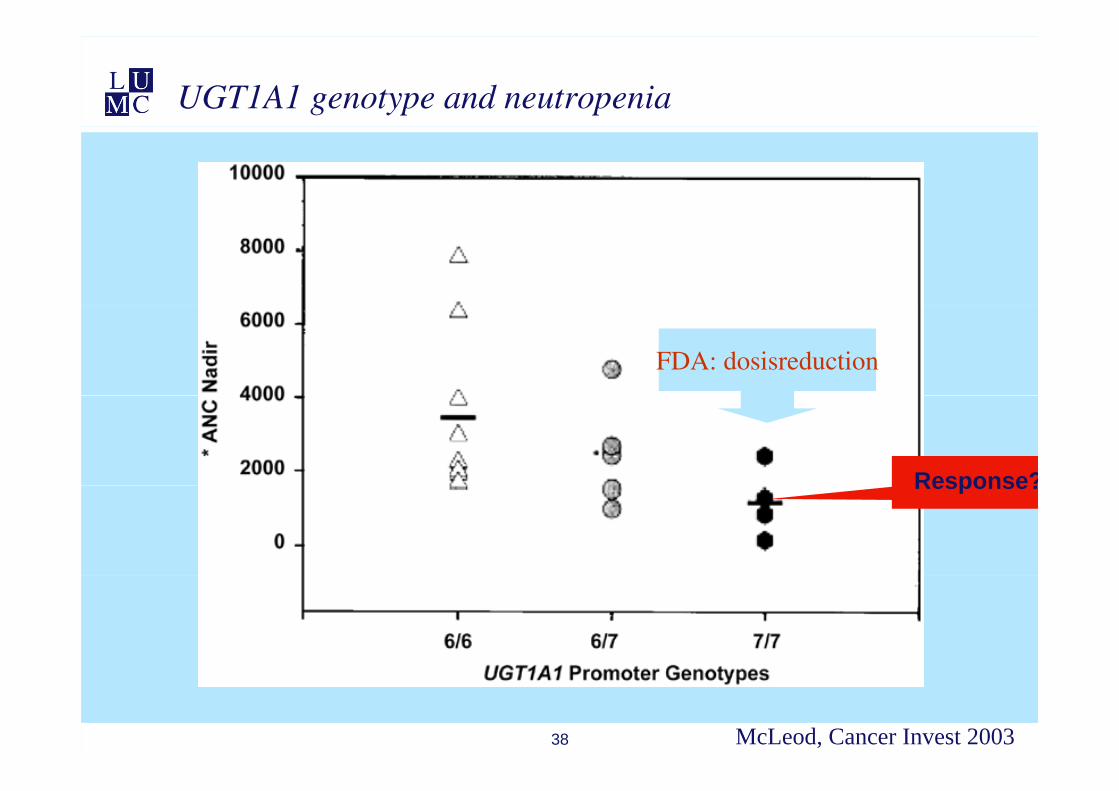
UGT1A1 genotype and neutropenia
FDA: dosisreduction
Response?Response?
38 McLeod, Cancer Invest 2003

•
39
Irinotecan dose adaptation
• 220 patients CAIRO1 studyM t t ti l t l• Metastatic colorectalcancer
• 1e line• Capecitabine 2 dd 1000 mg/m2 on days 1 14 every 3 weeks• Capecitabine 2 dd 1000 mg/m2 on days 1-14 every 3 weeks• Irinotecan 250 mg/m2 every 3 weeks
• 2e line (following capecitabine)2 line (following capecitabine)• Irinotecan 350 mg/m2 every 3 weeks
• Genotyping UGT1A1 *28 yp g
• Association with grade 3 of 4 febrile neutropenia
• Tumor response for each genotypep g yp
• Irinotecan dose for each genotype
40 Kweekel, submitted
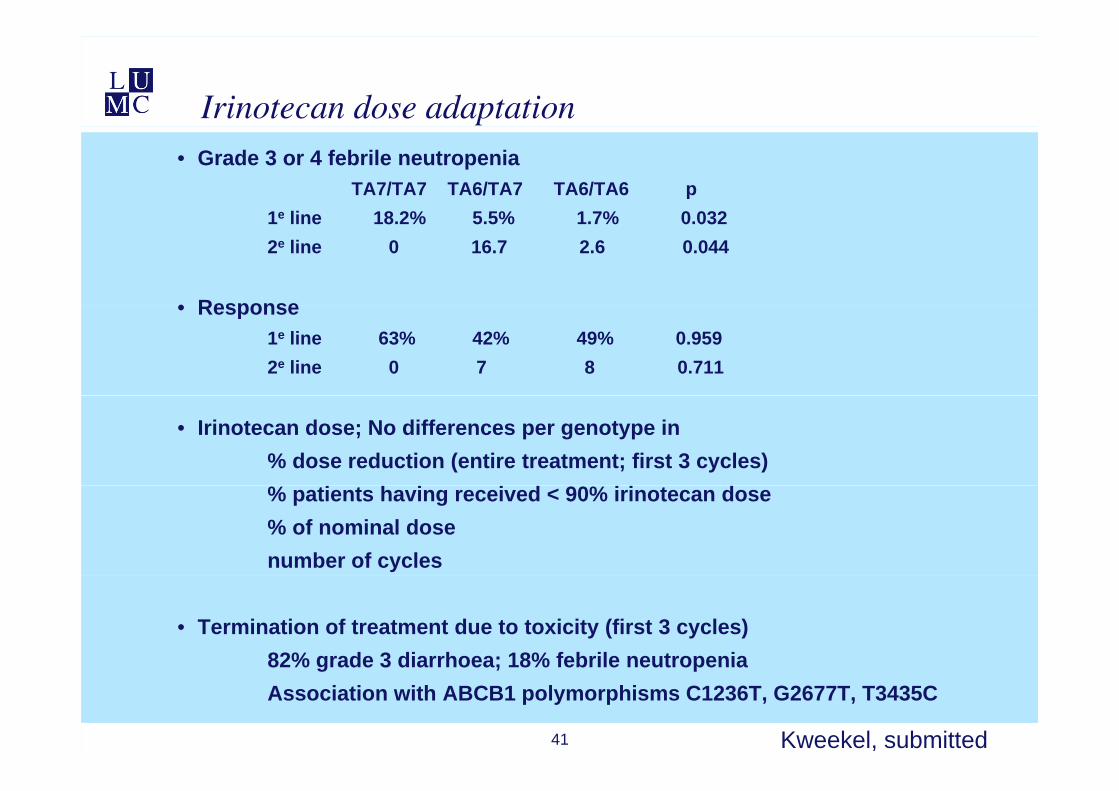
Irinotecan dose adaptation• Grade 3 or 4 febrile neutropenia
TA7/TA7 TA6/TA7 TA6/TA6 p1e line 18 2% 5 5% 1 7% 0 0321e line 18.2% 5.5% 1.7% 0.0322e line 0 16.7 2.6 0.044
• Response• Response1e line 63% 42% 49% 0.9592e line 0 7 8 0.711
• Irinotecan dose; No differences per genotype in% dose reduction (entire treatment; first 3 cycles)% patients having received < 90% irinotecan dose% of nominal dosenumber of cycles
• Termination of treatment due to toxicity (first 3 cycles)82% grade 3 diarrhoea; 18% febrile neutropenia
41
82% grade 3 diarrhoea; 18% febrile neutropeniaAssociation with ABCB1 polymorphisms C1236T, G2677T, T3435C
Kweekel, submitted
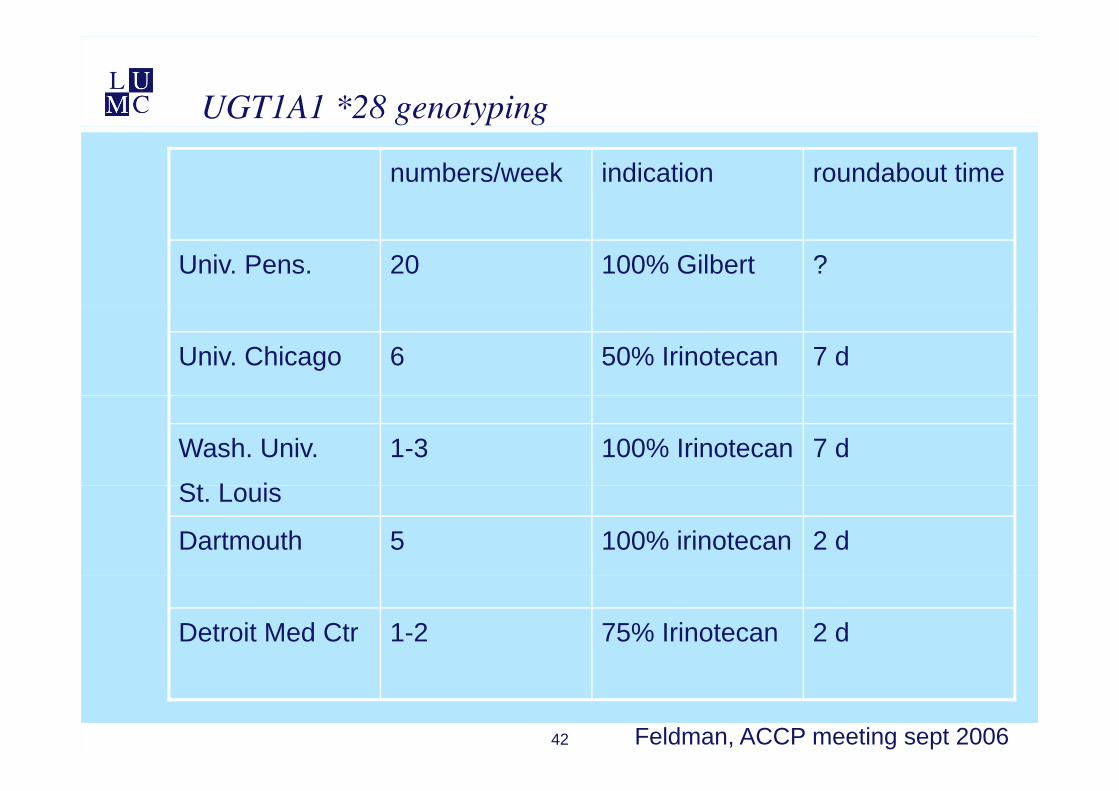
UGT1A1 *28 genotyping
numbers/week indication roundabout time
Univ. Pens. 20 100% Gilbert ?
Univ. Chicago 6 50% Irinotecan 7 d
Wash. Univ.
St L i
1-3 100% Irinotecan 7 d
St. Louis
Dartmouth 5 100% irinotecan 2 d
Detroit Med Ctr 1-2 75% Irinotecan 2 d
42 Feldman, ACCP meeting sept 2006
Pharmacogenetic research
• Aimed at solving importantAimed at solving important clinical problems
• Providing scientific evidence for added value of PGt testing
• Aimed at providing clinically applicable and clear cutapplicable and clear cut guideline following a test result
• Combine PGt and non-genetic determinants for drug response
43
Predictive model MTX response in RA patients
• 205 RA patients• Best-cohort (rheumatology LUMC)
• MTX monotherapy• 15 mg/wk + folic acid 1 mg/dag• Increased to 25 mg/wk if DAS>2.4
• Response: 47% • Adverse drug events: 30%Adverse drug events: 30%
• 17 polymorphisms in 13 candidate genes• folate and adenosine
• Non-genetic factors
44
Non-genetic factors
Wessels, A&R 2005, 2006, 2007
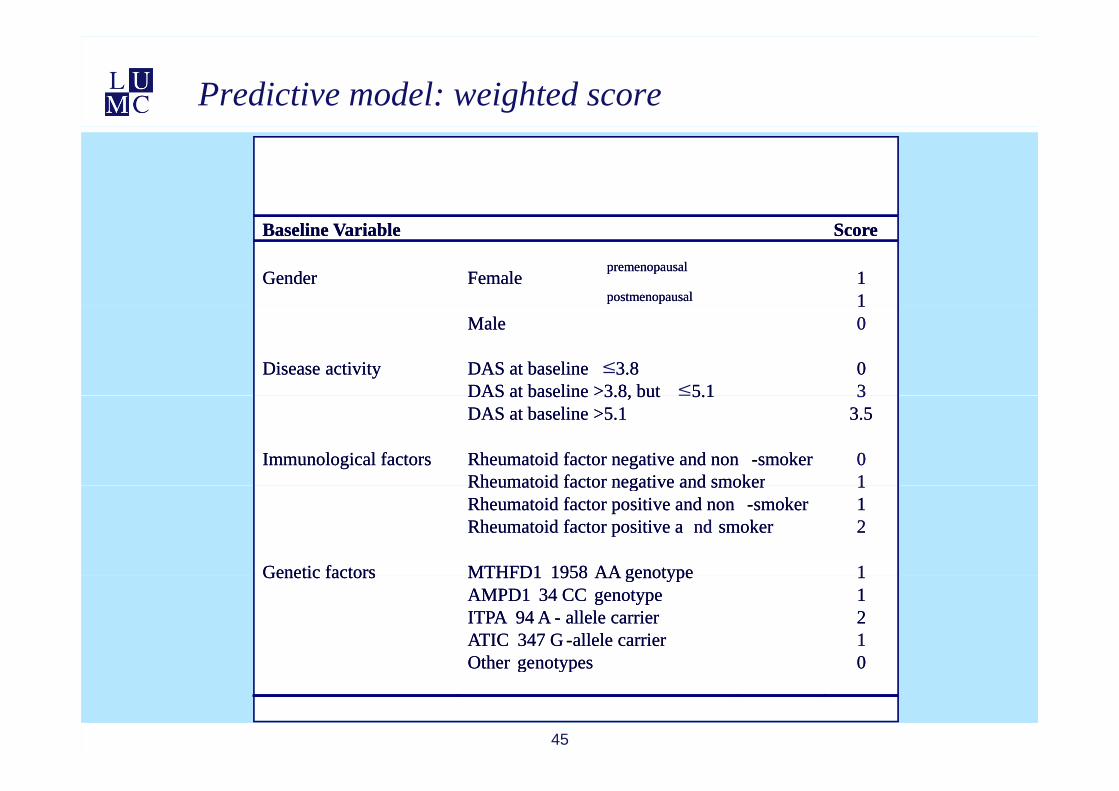
Predictive model: weighted score
Baseline Variable Score
premenopausal1Gender Female
postmenopausal 1
Baseline Variable Score
premenopausal1Gender Female
postmenopausal 11Male 0
Disease activity DAS at baseline 3.8 0DAS at baseline >3.8, but 5.1 3
1Male 0
Disease activity DAS at baseline 3.8 0DAS at baseline >3.8, but 5.1 3
≤≤DAS at baseline 3.8, but 5.1 3
DAS at baseline >5.1 3.5
Immunological factors Rheumatoid factor negative and non -smoker 0Rheumatoid factor negative and smoker 1
DAS at baseline 3.8, but 5.1 3DAS at baseline >5.1 3.5
Immunological factors Rheumatoid factor negative and non -smoker 0Rheumatoid factor negative and smoker 1
≤
Rheumatoid factor negative and smoker 1Rheumatoid factor positive and non -smoker 1Rheumatoid factor positive a nd smoker 2
Genetic factors MTHFD1 1958 AA genotype 1
Rheumatoid factor negative and smoker 1Rheumatoid factor positive and non -smoker 1Rheumatoid factor positive a nd smoker 2
Genetic factors MTHFD1 1958 AA genotype 1Genetic factors MTHFD1 1958 AA genotype 1AMPD1 34 CC genotype 1ITPA 94 A - allele carrier 2ATIC 347 G -allele carrier 1Other genotypes 0
Genetic factors MTHFD1 1958 AA genotype 1AMPD1 34 CC genotype 1ITPA 94 A - allele carrier 2ATIC 347 G -allele carrier 1Other genotypes 0
45
Other genotypes 0Other genotypes 0
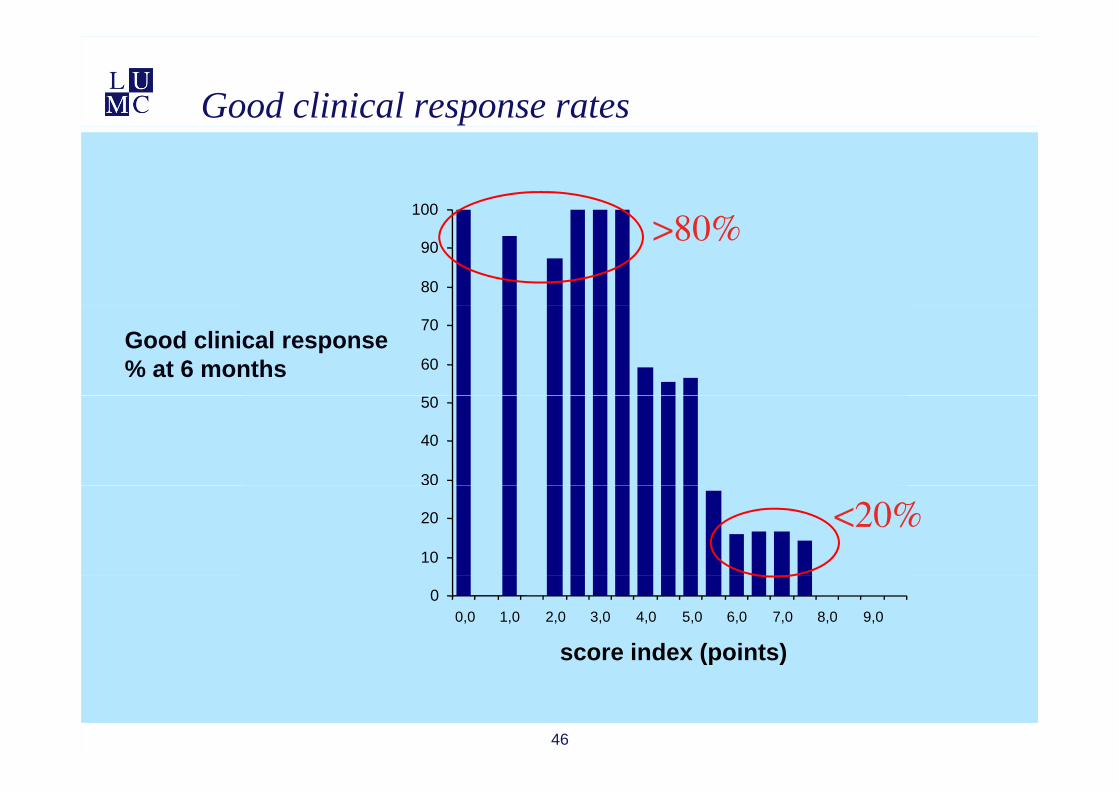
Good clinical response rates
>80%10080%>80%
80
90>80%
good response % 60
70Good clinical response % at 6 months
<20%30
40
50
10
20 <20%
00,0 1,0 2,0 3,0 4,0 5,0 6,0 7,0 8,0 9,0
score index (points)
46
( )
Conclusions
• Drug response is –at least in part- a heritable trait (‘proof of principle’)heritable trait ( proof of principle )
• PGt has the potential to solvePGt has the potential to solve important clinical problems and to improve pharmacotherapy
• The (added) value of PGt tests needs to be proven
• The approval of two PGt tests has introduced PGt into the clinic
47





























