Embed Size (px)
DESCRIPTION
Examination of the genital tract and the parturient patient and the foetus, and supervision of parturition and the main disorders at parturition in the sheep and goat. Prof. O. Szenci. Reproductive tract. EUB: external uterine bifurcation. Uterine horn. IcE: intercaruncular endometrium. - PowerPoint PPT Presentation
Citation preview
Examination of the genital tract and the parturient patient and the foetus,
and supervision of parturition and the main disorders at parturition in the
sheep and goat
Prof. O. Szenci
Reproductive tract
EUB: external uterine bifurcation
Uterine hornIcE: intercaruncular endometrium
Cervix
Fornix vaginaCranial vagina
Examination of ovariesExamination of ovaries
• by rectal palpation ???• by ultrasonography
• by colour Doppler sonography ???•by laparoscopy ???
• by measurement of plasma P4
Examination of the uterusExamination of the uterus
• Rectal palpation ???
• Ultrasonography
• Laparoscopy ???
• Additional diagnostic methods:– Uterine biopsy ???– Bacteriology ???– Citology ???
Ultrasonography
• Pregnancy diagnosis
• Uterine disorders– uterine inflammation– adhesions ???– abscesses ???– tumors ???– fetal remnants
A. Transabdominal ultrasonography (3.5 or 5 MHz)
Accurate (40 to 90 after AI):
• Simple pregnancy diagnosis
• Determination of fetal numbers
Disadvantage
• Shaving the ventral abdomen (some breeds)
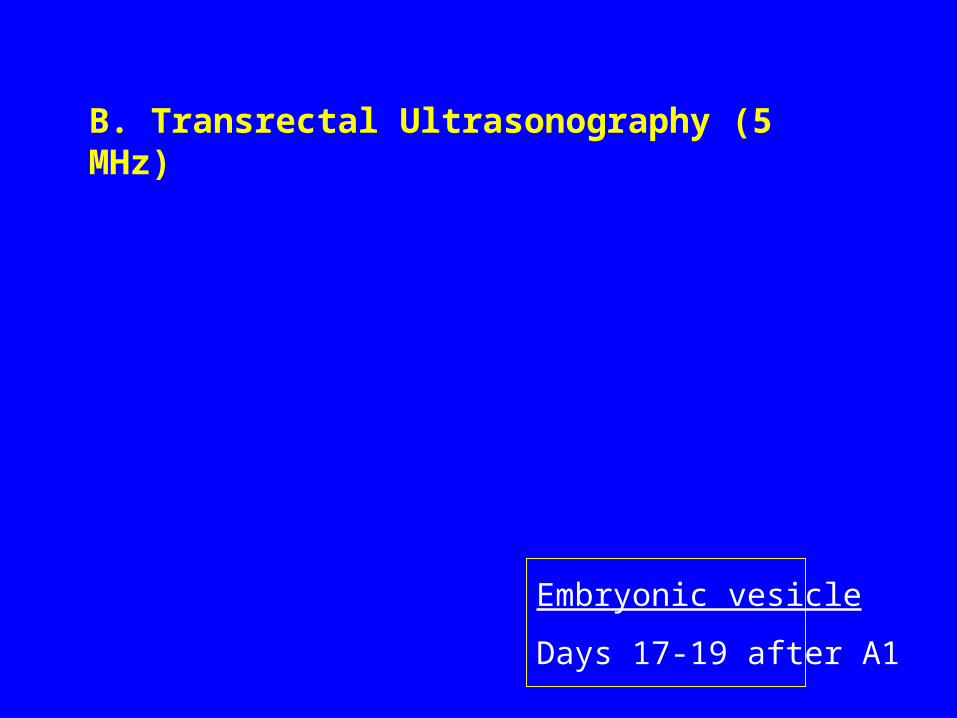
B. Transrectal Ultrasonography (5 MHz)
Embryonic vesicle
Days 17-19 after A1
Examination of the vagina
• by vaginal speculum
• by vaginoscope
Obstetrical examinationObstetrical examination
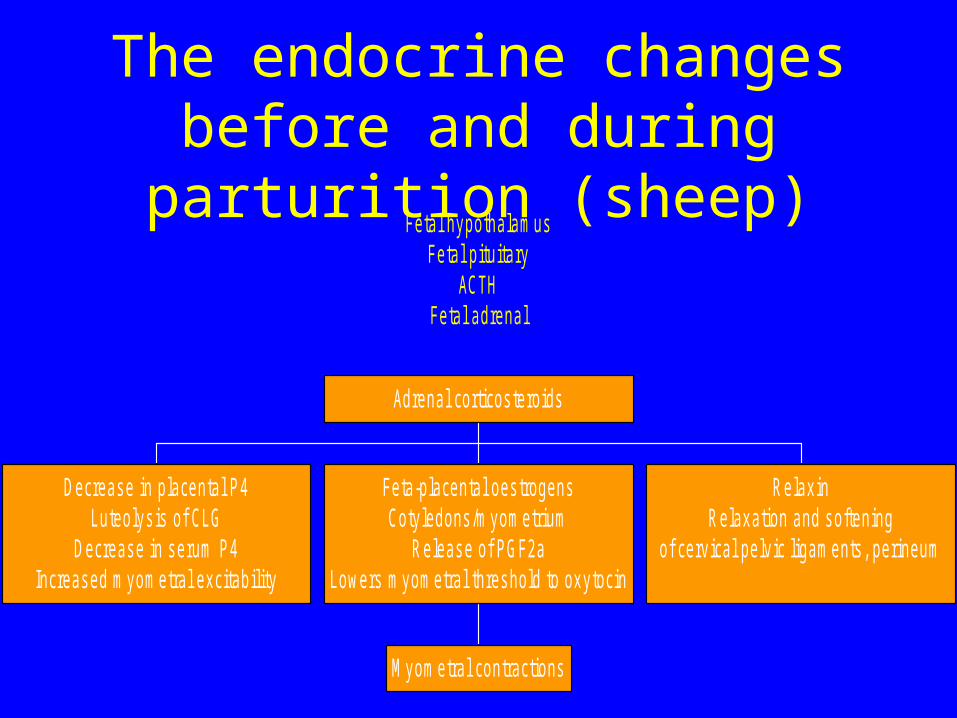
The endocrine changes before and during parturition (sheep)
Fetal hypothalamusFetal pituitary
ACTHFetal adrenal
Decreas e in placental P 4Luteolys is of CLG
Decreas e in s erum P 4Increas ed myometral excitability
M yometral contractions
Feta-placental oes trogensCotyledons /myometrium
R eleas e of P GF2aLowers myometral thres hold to oxytocin
R elaxinR elaxation and s oftening
of cervical pelvic ligaments , perineum
Adrenal corticos teroids
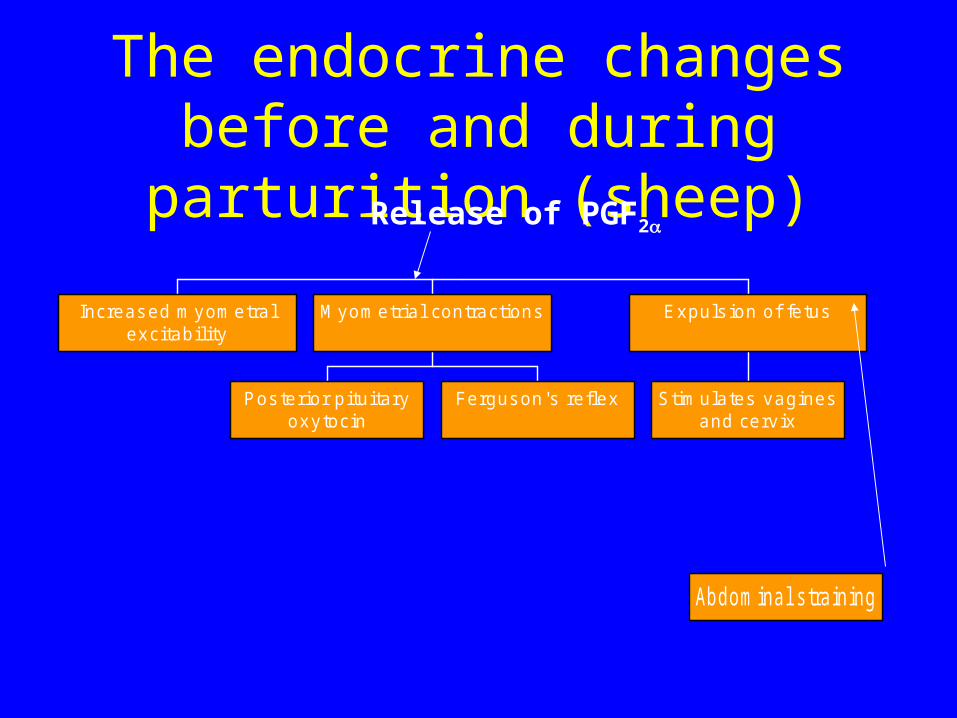
The endocrine changes before and during parturition (sheep)
Increas ed myometralexcitability
P os terior pituitaryoxytocin
Fergus on's reflex
M yometrial contractions
S timulates vaginesand cervix
Expuls ion of fetus
Abdominal s training
Release of PGF2
Premature induction of parturition
• Indications:– fetomaternal disproportion is not common– lambing during daylight with skilled assistance
• To reduce problems due to dystocia
• To increase lamb survival rate
Premature induction of parturition
• It is important to accurately known gestational age
• It is not possible to shorten gestation length properly without increasing lamb mortality (the role of the surfactant system)
Premature induction of parturition
• ACTH• Corticosteroids
– Not too successful for induction
– More often used for oestrus synchronisation: lambing in a relatively short period
• Dexamethanose, flumethasone, betamethanose (im.): – within 5 days before expected parturition
– normal parturition within 2 to 3 days
Premature induction of parturition
• Epostane (inhibits the enzyme that is responsible for the catalysis of pregnenolon-progesterone)
• Oestradiol benzoate: – Its use is prohibited in Europe
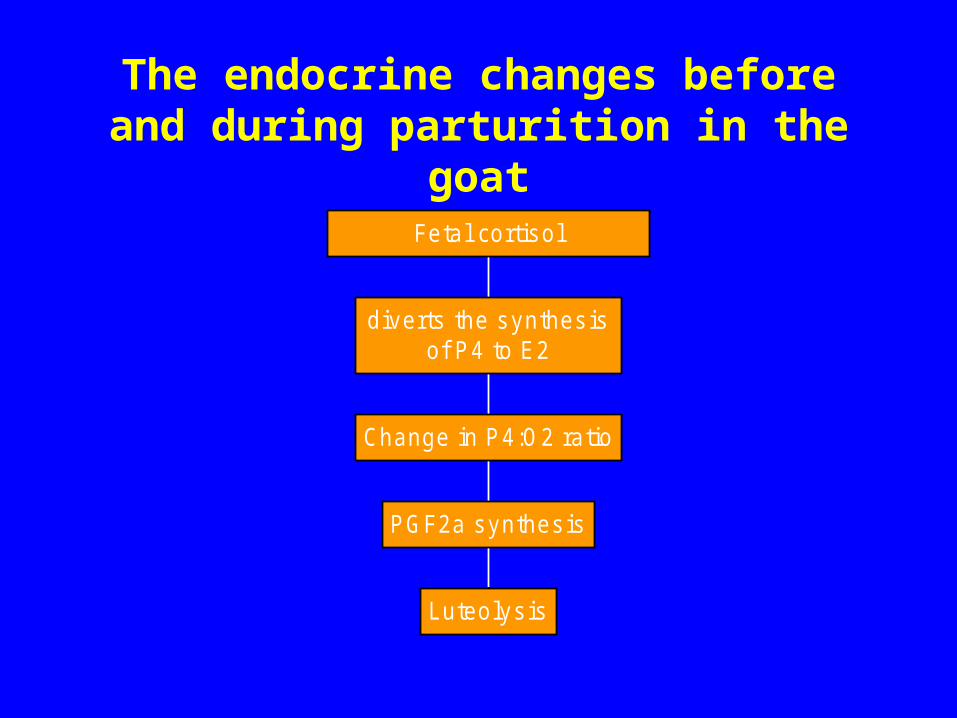
The endocrine changes before and during parturition in the goat
Luteolys is
P GF2a s ynthes is
Change in P 4:O2 ratio
diverts the s ynthes isof P 4 to E2
Fetal cortis ol
Premature induction of parturition (goat)
• Successful induction is possible• PGF2a (2.5-5 mg)• and PG-analogues (cloprostenol,
fenprostalene: 150-500 g)• ACTH• Corticosteroids (D 141.)• Dexamethasone 20-25 mg im.: parturition
within 2 days• (Oestradiol benzoate: 25 mg, but prohibited!)
Care of the parturient ewe
• second stage labour– completion within 1 h: 72%– the majority of ewes drop the placenta within 2
or 3 h after lambing– 95%: anterior presentation
Uterine involution
• Rapid size and weight reduction between 3 and 10 days postpartum
• Involution is completed by 20-25 days
Restoration of the endometrium
• necrosis of the superficial layer of the caruncles: – undergoes autolysis by 4 days pp.– dark reddish, brown or black coloration of the
lochial discharge
Restoration of the endometrium
• necrosis of the whole superficial part of the caruncle: – occurring by Day 16 pp.– separation of the brown necrotic plague:
completed– The necrotized particles are present within in
the uterine cavity– re-epithalisation of the caruncles takes place by
approx. D 28
Restoration of the endometrium
• The quality of the lochia– initially: blood, fetal fluids, placental debris– later: contains sloughed caruncular tissue
Returns of cyclical activity
• follicular growth is common– 2 days to 2 weeks pp.– ovulation is unusual– when it occurs: usually silent heat– inadequate release of LH and GnRH
Elimination of bacterial contamination
• similar like in the cow– however: 1-14 days after lambing (n=10 ewes:
no bacteria)
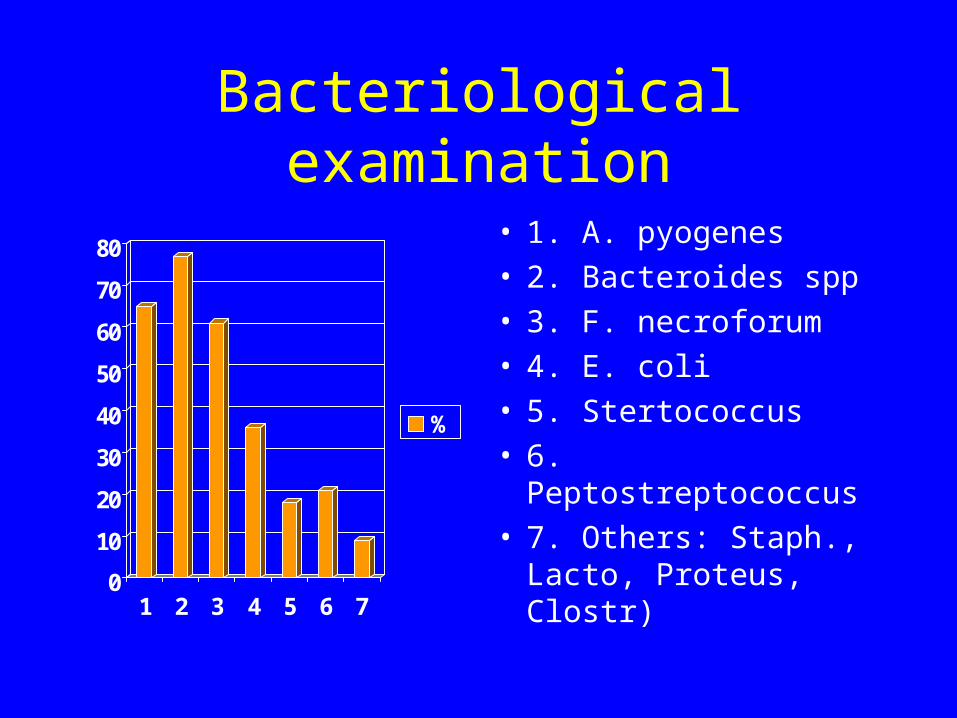
Bacteriological examination
0
10
20
30
40
50
60
70
80
1 2 3 4 5 6 7
%
• 1. A. pyogenes• 2. Bacteroides spp• 3. F. necroforum• 4. E. coli• 5. Stertococcus• 6. Peptostreptococcus• 7. Others: Staph.,
Lacto, Proteus, Clostr)
Classification of ovine births
• Anterior presentation, with head and both forelegs extended: 69,5%
• one foreleg retained: 17.8%
• both forelegs retained: 6.5%
• head retained: 0.7%
• breech presentation (hip flexion): 2.5%
General examination of the animal
• special attention should be paid to the vagina– parts of a foetus may be protruding---- we may
get information about the nature of dystocia
General examination of the animal
• General condition should be described– if recumbent:
• resting
• exhausted
– the importance of body temperature and pulse rate
General examination of the animal
Conditions:– two clean buckets with water – table or bench of straw, sterile cloths– hot water, soap, disinfectant
– restraining the animals– cleaning the external genitals and hands
• the external genitals thoroughly washed (one bucket)
• careful washing the hands (second bucket)
Vaginal examination
• If the vagina is empty:
– checking the cervix– not completely dilated + sticky mucus
covers:» the second stage of parturition has
not yet begun» allow more time
Vaginal examination
• spirally arranged folds– uterine torsion
Vaginal examination
• some parts of the foetus in the vagina– head– fore- or hindlegs
• plantar surfaces of the claws: downwards—usually forelimbs (if position is dorsal)
• checking the direction of the flexion of the joints on the legs
– the joint immediately above the the fetlock flexes in the same direction: foreleg
• if two limbs present: check if they belong to the same foetus
Vaginal examination
• Some cases: repel the foetus in the uterus– to get information about the nature of
displaced fetal parts
Vaginal examination
• moisten foetal parts– fresh cases
• profuse blood– recent injury
• dry foetal parts– protracted case– dark, brown discharge:
• very late case
Vaginal examination
• Solution of abnormal presentations– depending on the operator’s ability to pass a
hand through the pelvic bone into the uterus– possible in most of the ewes– impossible (deliver per vaginam may fail):
• primiparous animals
• smaller breeds
Vaginal examination
• Relative foetal oversize– retropulsion of head or hips– gentle traction with obstetric rope
Vaginal examination
• Abnormal posture of the limbs or head – retropulsion– reposition– lubrication– gentle traction
Vaginal examination
• Abnormal posture of the limbs or head– If a lateral deviation of the head or the
breech presentation cannot be reposited: foetotomy, or caesarean section
Vaginal examination
• Special attention should be payed on the soft birth canal, not to cause laceration
• acute infection
• death
• Prevention: • prophylactic vaccination
• use of antibiotics
Dystocia
• 94,5 anterior presentation
• 3,6% posterior presentation
Dystocia
• based on data from 15 584 parturitions:
• occurrence of dystocia: 3.1%– 3.5% in single lambings– 1.3% in twins
Dystocia
• more frequent: – in primiparous animals– male lambs
Abnormal presentations
– shoulder flexion: (the most common)– unilateral shoulder flexion: often lambing
spontaneously – carpal flexion– breech presentation (two sided hip flexion)– lateral deviation of the head– transverse presentations
Dystocia
• Overview:– lateral deviation of the head: 32%– insufficient cervical dilatation: 15%– shoulder flexion– carpal flexion– twins– breech presentation– foetal oversize
Dystocia
• Other occasional causes:– uterine torsion– monstrosities (schistosoma reflexum, double
monsters, anasarca, perosomus elumbis)
Maternal dystocia
Maternal dystocia
Incidence:
– dry season: less
– estrogenic substances• red clover pasture• contaminated food with Fusarium
graminaerum
– reduced PGF2a production
Maternal dystocia
Treatment:
– digital manipulation
– carbetocin (Depotocin, Hypophysin 0.5-1.0 ml)
– denaverin (Spasmotitrat 2-3 ml)
– Caesarean section
Foetal dystocia
Foetal dystocia
• Foetal component: – foetal oversize– abnormal presentation
Foetal dystocia
• Anterior presentation with flexion of the shoulder and flexion/or less frequently/extension, of the elbows
• Treatment:– Correction of abnormal presentation, standard
obstetric procedures (including fetotomy).
Foetal dystocia
• Gentle traction alone (retention of one forelimb)
• Episiotomy, fetotomy: minimize the need for caesarean section in cases if vaginal and vulval tissues are not dilated enough.
• Suturing the separated tissues after removal of the fetus is optional. Prophylactic antibiotic therapy
Caesarean section
• Indication
• cervical dilatation failure
• relative and absolute foetal oversize
• emphysema, monstrosities, hydrallantois
• vaginal prolapse, pregnancy toxaemia: induction is preferred
Dystocia
• Anaesthesia: administration of local anaesthetics: infiltration, paravertebral block or epidural anaesthesisa
• Sedation: diazepam 0.2 mg/kg
Dystocia
• Operative procedure: left flank or midline laparotomy
• Lamb resuscitation:– Acidotic lamb: administration of sodium
bicarbonate (5 mEq) and glucose (5 ml of a 10% solution)
Dystocia
• Prevention:– Regular exercise of the pregnant ewes– The rearing failure, including dystocia are:
repeatable and heritable– Selection for better rearing ability offers
improved prospect to reducing the prevalence of dystocia and less need for obstetrical aid at lambing.
Dystocia
• ewes with dystocia should be culled from pure-bred flocks because of the repeatable and heritable nature of the rearing failure.
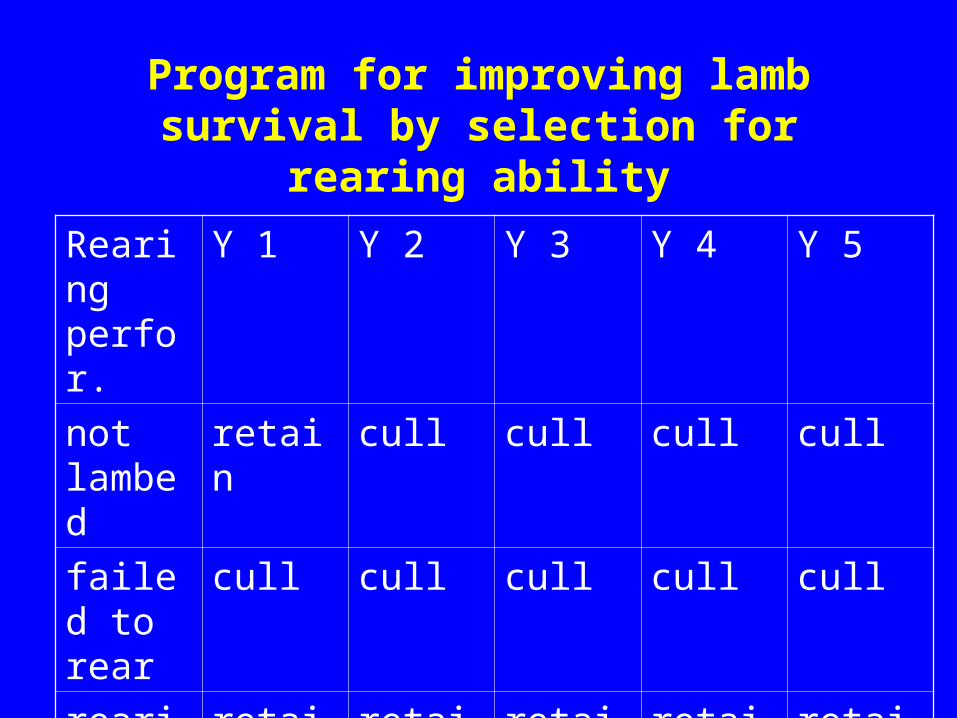
Program for improving lamb survival by selection for rearing ability
Rearing perfor.
Y 1 Y 2 Y 3 Y 4 Y 5
not lambed
retain cull cull cull cull
failed to rear
cull cull cull cull cull
rearing at least 1 lamb
retain retain retain retain retain
The newborn and its care
• Sudden change: – demanding great adaptability
• spontaneous respiratory movements within 60 seconds
• important: upper respiratory tract is cleared of fluid, mucus and attached foetal membranes
• one third: absorbed vial lymphatic systems
The newborn and its care
• Thermoregulation– fall in temperature– recovery within few hours
The newborn and its care
• Thermoregulation controlled in two ways– increase in metabolic rate
• low glycogen and adipose tissue reserves
• immediate and adequate food
– reduce heat loss• little subcutaneous fat and hence insulation is
poor
• wet surface: heat loss due to evaporation
The newborn and its care
• Umbilicus– antiseptic solution
Caprine obstetrics
Periparturient care of the doe
• Goats need a 6 to 8-week dry period.
• Does with a history of mastitis should be dry treated.
• Four weeks before parturition: tetanus, enterotoxaemia vaccinations
• Prophylactic Vitamin E-, Se injections: if white muscle disease occurs.
PARTURITION
PARTURITION
• udder fills: occasionally necessary to milk out
• the vulva also enlarges
• place in a clean, well-bedded and roomy box stall: when parturition is close
PARTURITION
• The preparing doe is restless and may build a nest
• after parturition – she licks the membranes, the kid
• may eat part of the placenta
PARTURITION
• Kids are usually standing within 10 to 30 min.
• Licking for 5 to 10 minutes is usually adequate for acceptance.
• The first 2 hours after birth is critical.
Dystocia
Dystocia
• dystocia: the kidding process > 1 h of active abdominal straining without producing a kid
• usually all kids are born within 3 hours and the placenta is passed within 2 h of the last kid
Dystocia
• correct dystocia early because the cervix will begin to close after 2 – 3 h of non-productive labour– it is not possible to dilate again
Dystocia
• active straining for 1.5 h: no progress
• more than 12 h of restlessness and abdominal discomfort without active labour
Dystocia
• 1. Incomplete cervical dilatation:– Firm rings (usually 2 bands 0.5 to 1 cm wide)
can be felt.– A non-dilatated cervix with cool skin and ears
and muscle weakness, treatment for hypocalcaemia (60 ml) should be initiated.
– Caesarean section is indicated.
Dystocia
• 2. Uterine torsion:– Uncommon– Caesarean section
• 3. Forced extraction:– If the cervix is well dilatated and the foetal
presentation can be corrected, forced extraction may be attempted.
Dystocia
• 4. Foetotomy:– Epidural anaesthesia: 2% 2 to 5 ml Lidocaine
Dystocia
• 5. Caesarean section:– left flank or ventral midline incision.– If the doe is profoundly depressed, she may
require only local anaesthesia (30 ml of 1% Lidocaine) and leg restraint.
– If sedation is required diazepam (0.1 to 0.2 mg/kg IV) or xylazine (0.02 to 0.04 mg/kg IV) may be used.
Dystocia
• 5. Caesarean section (cont.):– Ketamine hydrochloride: 5 mg/kg IV– General anaesthesia: halothane or isoflurane
Dystocia
• Prognosis:– is good if the surgery was performed electively.– In the cases of emphysematous, macerated
foetus or seriously ill dam the prognosis is poor.
Dystocia
• Postoperation treatment:– Oxytocin: 5 IU IV or IM– Systemic antibiotic therapy: Penicillin G 20000
to 40000 units/kg IM– Flunixin meglumine: 1.1 mg/kg: may help to
relieve postoperative pain.
Dystocia
• Postoperation treatment (cont):– susceptible to tetanus:
• vaccinated goat: booster injection of toxoid
• not vaccinated: 1500 IU of tetanus antitoxin
Dystocia
• Postoperation treatment (cont):– contaminated uterus during manipulation
• should be rinsed with warm fluid
• with Betadine
• bolus or fluid antibiotics in the uterus
Newborn kids
• stimulation of respiration– vigorous rubbing or– by placing straw in the nose
• fluids should be drained by gravity
• colostrum: 50 ml/kg by stomach tube – in lethargic case