Embed Size (px)
Citation preview

t
C0h
R
CM
ORIGINAL ARTICLE: Clinical Endoscopy
Prophylactic temporary 3F pancreatic duct stent to prevent post-ERCPpancreatitis in patients with a difficult biliary cannulation: amulticenter, prospective, randomized study
Tae Hoon Lee, MD,1 Jong Ho Moon, MD,2 Hyun Jong Choi, MD,2 Seung Hyo Han, MD,2
Young Koog Cheon, MD,3 Young Deok Cho, MD,3 Sang-Heum Park, MD,1 Sun-Joo Kim, MD1
Cheonan, Bucheon, Seoul, South Korea
Background: Post-ERCP pancreatitis (PEP) is the most common and serious complication of ERCP. Difficultbiliary cannulation can be a procedure-related risk factor for PEP. Recent studies reported that a prophylacticpancreatic stent (PS) can reduce the frequency and severity of PEP.
Objective: To evaluate the efficacy and usefulness of a temporary 3F PS to prevent PEP in patients with difficultbiliary cannulations.
Design: A multicenter, prospective, randomized study.
Setting: Two tertiary-care academic medical centers.
Patients: In total, 101 patients with a difficult biliary cannulation were randomly divided into the 3F PSplacement group (PS group, n � 50) or the nonstent (NS) group (NS group, n � 51).
Interventions: Endoscopic placement of a 3F unflanged PS.
Main Outcome Measurements: The incidence and severity of PEP in the 2 groups, spontaneous dislodgmentof stents, and procedure-related complications.
Results: The technical success rate of 3F PS placement was 96% (48/50). The lengths of the stents were 4cm (n � 21), 6 cm (n � 15), and 8 cm (n � 12). Spontaneous stent dislodgment within 7 days occurred in94% of patients (45/48). The mean duration until spontaneous dislodgment was 3.5 days. The incidence rateof PEP was 12% (6/50: mild, 5; moderate, 1) in the PS group and 29.4% (15/51: mild, 12; moderate, 2; severe,1) in the NS group. Severe pancreatitis occurred in only 1 patient in the NS group. In a multivariate analysis,prophylactic placement of PS was the only prophylactic factor for PEP (odds ratio, 0.126; 95% CI,0.025-0.632, P � .012).
Limitations: No comparative results for stent size and diameter and a low-risk cohort group.
Conclusions: Prophylactic temporary 3F PS placement in patients with a difficult biliary cannulation duringERCP seems to be a safe and effective method for reducing PEP and results in a high rate of spontaneous passageof stents without complications. (Gastrointest Endosc 2012;76:578-85.)
Abbreviations: NS, nonstent; PD, pancreatic duct; PEP, post-ERCP pan-creatitis; PS, pancreatic stent; SD, standard deviation; SOD, sphincter ofOddi dysfunction.
DISCLOSURE: All authors disclosed no financial relationships relevant tohis publication.
opyright © 2012 by the American Society for Gastrointestinal Endoscopy016-5107/$36.00ttp://dx.doi.org/10.1016/j.gie.2012.05.001
eceived September 30, 2011. Accepted May 1, 2012.
urrent affiliations: Digestive Disease Center (1), Department of Internaledicine, Soon Chun Hyang University School of Medicine, Cheonan, Diges-
tive Disease Center (2), Department of Internal Medicine, Soon Chun HyangUniversity School of Medicine, Bucheon, Digestive Disease Center (3), De-partment of Internal Medicine, Soon Chun Hyang University School of Med-icine, Seoul, South Korea.
Reprint requests: Jong Ho Moon, MD, PhD, Department of Internal Medicine,Soon Chun Hyang University School of Medicine, Digestive Disease Center,Soon Chun Hyang University Bucheon Hospital, 1174 Jung-Dong, Wonmi-Ku, Bucheon 420-767, South Korea.
If you would like to chat with an author of this article, you may contact DrMoon at [email protected].
578 GASTROINTESTINAL ENDOSCOPY Volume 76, No. 3 : 2012 www.giejournal.org

lfiOod
csgetcpVis
paag[afncttppf
E
sJfwa
AscuoaattsTictwTElmpi
Lee et al 3F pancreatic stent to prevent post-ERCP pancreatitis
Post-ERCP pancreatitis (PEP) is the most common andserious complication of ERCP and occurs after 1% to 40%of procedures. Its prevalence depends on several factors,including case mix, thoroughness of the follow-up evalu-ation, definition used, factors related to patient suscepti-bility, types of instrumentations used, and the skill ofthe endoscopist.1-6 Recent studies reported that prophy-actic placement of a pancreatic stent (PS) reduces therequency and severity of PEP in various risk groups,ncluding those with known or suspected sphincter ofddi dysfunction (SOD), papillectomy, precut sphincter-tomy, pancreatic sphincterotomy, history of PEP, or aifficult cannulation.5-23
The overall success rate for selective cannulation duringERCP ranges from 90% to 95%, even when performed byexperts.7 During biliary cannulation, the rate of PEP in-creases when cannulation is difficult and prolonged.3
However, few data are available concerning the effect of aprophylactic pancreatic duct (PD) stent on this technicaldifficulty with respect to cannulation time or frequency ofpapillary contacts. In addition, the sizes and lengths ofstents are variable, and no guideline or consensus yetexists regarding which type or length of PS is optimal.16-18
This prospective, randomized, controlled study was de-signed to evaluate the efficacy and usefulness of a 3F PS toprevent PEP in patients with difficult selective biliarycannulations.
PATIENTS AND METHODS
Study population and designConsecutive consenting patients referred for therapeu-
tic ERCP between January 2008 and July 2011 were in-cluded from 2 academic tertiary referral centers. Allpatients underwent abdominal US, CT scans, and/or mag-netic resonance cholangiopancreatography before ERCP.Patients who satisfied the following inclusion criteria wereenrolled: difficult biliary cannulation, age 18 years andolder, and agreement to participate in this study. Difficultbiliary cannulation was defined as failure to achieve se-lective biliary access despite 10 minutes of attempted can-nulation, more than 5 attempted unintentional pancreaticcannulations, or frequent papillary contact of more than 10times, whichever occurred first. Papillary contact was de-fined as sustained contact between the catheter and theampulla of Vater for at least 3 to 5 seconds.4,24 Exclusionriteria were the following: age younger than 18 years,uccessful deep biliary cannulation without difficulty, sur-ically altered anatomy (Billroth II gastrectomy or Roux-n-Y anastomosis), previous biliary or pancreatic sphinc-erotomy, uncontrolled coagulopathy, radiological andlinical evidence of acute pancreatitis at the time of therocedure, a tumorous condition invading the ampulla ofater, pancreatic head cancer with main PD obstruction,
ntraductal papillary mucinous neoplasm, pancreatic divi-
um, and refusal to participate in the study. In total, 101 pwww.giejournal.org V
atients with difficult biliary cannulations were enrolled,nd patients who met the eligibility criteria were randomlyssigned by computer-generated randomization to 2roups (PS group [3F plastic stent inserted] vs nonstentNS] group; block randomization with the medical centerss blocks) (Fig. 1). The allocation sequence was concealedrom all patients and endoscopists. A second assistingurse was assigned at the point of difficulty with theannulation. The procedure time, including cannulationime, papillary contacts, and unintentional PD cannula-ion, was recorded by same assisting nurse during therocedures. All institutional review boards involved ap-roved this study. Written informed consent was obtainedrom all enrolled patients.
ndoscopic procedureAll patients underwent ERCP with a standard duodeno-
cope (JF 260 or 260V; Olympus Optical Co, Ltd, Tokyo,apan). The procedure was performed after the patientasted overnight, was placed in the prone position, andas sedated with intravenous midazolam (0.05 mg/kg)nd/or propofol (0.5 mg/kg).
Prophylactic antibiotics and analgesics were permitted.ll procedures started with a standard double-lumenphincterotome or conventional catheter. A wire-guidedannulation technique was not attempted initially, but wassed as a rescue method for difficult biliary cannulationsr selected PD cannulations for stenting. In the PS group,guidewire in the PD for pancreatic stenting was used,
nd then selective biliary cannulation was attempted withhe guidewire in the PD (double wire-guided cannulationechnique). After successful biliary cannulation and/orphincterotomy, patients underwent pancreatic stenting.he endoscopic approach to PS placement involved pass-ng a 0.018- or 0.021-inch/480-cm guidewire (Cook Endos-opy, Winston-Salem, NC) deep into the PD, at least pasthe genu. Before pancreatic stenting, pancreatographyas performed to visualize the correct direction of the PD.hen, an unflanged single pigtail-type PS (Zimmon; Cookndoscopy) with a small-caliber (3F) and 4, 6, or 8 cm inength was placed over the guidewire. Successful PS place-ent was achieved when the stent was appropriatelyositioned within the PD and its distal end was positionedn the duodenal lumen. Prophylactic PS placement was
Take-home Message
● Difficult biliary cannulation can be a risk factor for post-ERCP pancreatitis. Prophylactic temporary placement of a3F pancreatic duct stent was technically feasible andeffectively reduced the rate of post-ERCP pancreatitiswith a high rate of spontaneous dislodgment in patientswith a difficult biliary cannulation.
erformed before biliary therapeutic procedures such as
olume 76, No. 3 : 2012 GASTROINTESTINAL ENDOSCOPY 579

tlmp1wlca
S
Pgb1ttdctyatpbmwi
in th
3F pancreatic stent to prevent post-ERCP pancreatitis Lee et al
stone extraction or stent placement, but not for biliarysphincterotomy. Cannulation was attempted in the NSgroup until successful biliary cannulation was achieved. Ifbiliary cannulation failed within 20 minutes, the procedurewas completed without PD stenting. Precut papillotomy(infundibulotomy) was performed as a rescue method forselective common bile duct cannulation.
After the ERCP procedure, patients were admitted forobservation and fasted until tests on the following dayconfirmed that no complications had occurred, includingpancreatitis. Follow-up plain abdominal radiographs wereobtained to assess spontaneous stent dislodgment the dayafter ERCP. If the stent had not passed within 48 hours, asimple abdominal radiograph was obtained every day un-til day 7. If the stent had not passed spontaneously by 7days, endoscopic removal was performed. All ERCP pro-cedures were performed by 2 experienced endoscopists(M.J.H. and L.T.H. with an ongoing workload of 500ERCPs annually) in each tertiary referral center.
Definition of outcomesThe primary outcome measurements for both groups
were the frequency and severity of PEP. We also evaluatedthe success rate of PS placement, the duration of sponta-neous stent dislodgment, and complications in bothgroups. All ERCP-related complications were classifiedand graded according to consensus guidelines.25 Serumamylase and lipase levels were measured before ERCP and24 hours thereafter. Asymptomatic hyperamylasemia after
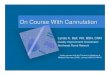
Figure 1. Flow chart showing representative subjects
ERCP was defined by each institution as an elevation of m
580 GASTROINTESTINAL ENDOSCOPY Volume 76, No. 3 : 2012
he serum amylase level within 3 times the upper normalimit without abdominal pain. Pancreatitis was consideredild if hospitalization was extended 2 to 3 days after therocedure, moderate if hospitalization was extended 4 to0 days after the procedure, and severe if hospitalizationas extended for more than 10 days. Spontaneous dis-
odgment of the PS was defined when the entire stentompletely migrated from the PD within 7 days withoutny intervention.
tatistical analysisWe assumed that the proportion of patients with overall
EP would be 25% in the difficult biliary cannulationroup without PS, and 5% in the prophylactic PS groupased on historical data (NS vs PS, 12.5%-33% vs 0%-4%).6,8-12,21 Based on those assumptions, power calcula-ions indicated that 50 patients were needed in each groupo have an 80% chance of rejecting the hypothesis of noifference at the 0.05 level. Exploratory univariate statisti-al analysis was performed to indicate candidate variableso be used in the subsequent, definitive multivariate anal-sis. In the exploratory univariate testing, categorical vari-bles were compared by using the �2 and Fisher exactests, as appropriate, and continuous variables were com-ared with the Student t test. Candidate variables found toe significant on univariate analysis were included in theultivariate model, along with other variables for which itas thought necessary to control for their contributions,
ncluding age (categorized) and suspected SOD. Then a
e prophylactic pancreatic stent and nonstent groups.
ultivariate logistic regression analysis was performed to
www.giejournal.org

Pnrdf1rt
tg(1ornqtdtdN
92sTptesUno4doc
(go(TasgsotPpl
Lee et al 3F pancreatic stent to prevent post-ERCP pancreatitis
determine those factors having an independent associa-tion with PEP after adjusting for the contributions of theother variables. All statistical analyses were performed byusing SPSS version 14.0 software (SPSS Inc, Chicago, Ill),with results considered significant with P � .05. The Pvalues for the univariate statistical tests were not correctedfor multiple testing because those tests were taken asexploratory. The subsequent multivariate logistic regres-sion analysis was considered the main definitive resultbecause it determined those variables independently as-sociated with PEP, after adjusting for the contributions ofthe other variables.
RESULTS
The baseline characteristics and indications for ERCP inboth groups are shown in Table 1. A total of 3625 patientswere prescreened, and 3524 patients were excluded be-cause of age younger than 18 years (n � 19), successfuldeep biliary cannulation without difficulty (n � 1421),surgically altered anatomy (n � 121), previous biliary orpancreatic sphincterotomy or sphincteroplasty (n � 1545),uncontrolled coagulopathy (n � 31), radiological and clin-ical evidence of acute pancreatitis at the time of the pro-cedure (n � 89), a tumorous condition invading the am-
TABLE 1. Baseline characteristics
PS group NS group
No. of patients 50 51
Age, y, mean (range) 57.3 (18-86) 57.9 (24-85)
Sex, M/F 17/33 21/30
Indications for ERCP
Choledocholithiasis 33 34
Malignant CBD obstruction 4 3
Benign CBD stricture 2 1
Bile duct dilation 1 0
Pancreas malignancy* 3 3
Choledochal cyst 0 1
Chronic pancreatitis† 1 1
Ampulla of Vater adenoma 1 0
Cholecystitis 3 7
Abnormal liver chemistry 0 1
Suspected SOD 2 0
PS, 3F plastic stent; NS, nonstent; CBD, common bile duct; SOD,sphincter of Oddi dysfunction.*Pancreas tail cancer with jaundice.†Chronic pancreatitis grade I.
pulla of Vater (n � 24), pancreatic head cancer with main P
www.giejournal.org V
D obstruction (n � 147), intraductal papillary mucinouseoplasm (n � 34), pancreatic divisum (n � 7), andefusal to participate in the study (n � 86). The rate ofifficult cannulation in the patients who provided in-ormed consent and had a naive papilla was 6.6%. In total,01 patients with a difficult biliary cannulation were en-olled and randomly assigned to the PS group (n � 50) orhe NS group (n � 51) (Fig. 1).
The mean (standard deviation [SD]) duration for selec-ive biliary cannulation was 15.9 (6.7) minutes in the PSroup and 15 (4.1) minutes in the NS group. The meanSD) frequency of papillary contacts was 10.8 (4.2) and0.9 (5.1), respectively. More than 15 papillary contactsccurred in 9 of 50 cases (18%), and 7 of 51 cases (13.7%),espectively. When the 2 groups were compared, no sig-ificant differences were found for cannulation time, fre-uency of papillary contacts, unintentional PD cannula-ion, or total procedure time (Table 2). No significantifference was found for therapeutic procedures betweenhe 2 groups except for the rate of endoscopic nasobiliaryrainage, which was higher for the PS group than for theS group (16.2% vs 6.1%, P � .01).The technical success rate of 3F PS placement was
6% (48/50). The lengths of the stents were 4 cm (n �1), 6 cm (n � 15), and 8 cm (n � 12). The rate ofpontaneous dislodgment by day 7 was 94% (45/48).he stents had to be removed endoscopically in only 3atients (6%) 7 days later. The mean duration to spon-aneous dislodgment was 3.5 days. No significant differ-nce in the rate of spontaneous dislodgment was ob-erved among the stent lengths (P � .168) (Table 3).nsuccessful PS placement occurred in 2 patients, buto serious complications developed, except for 1 casef mild pancreatitis. Pancreatography was performed in1 patients (85.4%) without pancreatic acinarizationuring stent placement. Intramural contrast injectionccurred in 2 patients. No major complications wereaused by the PS.
Mean (SD) serum amylase levels after ERCP were 254.1228.5) U/L in the PS group and 401.4 (395.7) U/L in the NSroup (P � .024). Asymptomatic hyperamylasemia devel-ped in 8 patients (16%) in the PS group and 6 patients11.8%) in the NS group, without a significant difference.he incidence rate of PEP was 12% (6/50) in the PS groupnd 29.4% (15/51) in the NS group (P � .031). Pancreatitiseverity was mild (n � 5) or moderate (n � 1) in the PSroup, whereas it was mild (n � 12), moderate (n � 2), orevere (n � 1) in the NS group (Table 4). No severe PEPccurred in the PS group. Multivariate analysis indicatedhat 15 or more cannulation attempts were a risk factor forEP (odds ratio 4.301; 95% CI, 1.203-15.380; P � .025), androphylactic placement of a 3F PS was the only prophy-actic factor for PEP (odds ratio 0.126; 95% CI, 0.025-0.632;
� .012) (Table 5).
olume 76, No. 3 : 2012 GASTROINTESTINAL ENDOSCOPY 581

ppoefmaditoi
tintpmuatucrww
admptAPsAgdsia
3F pancreatic stent to prevent post-ERCP pancreatitis Lee et al
DISCUSSION
Risk factors for PEP include papillectomy, sphincterot-omy including precut, SOD, young age, female sex, bal-loon dilation of an intact biliary sphincter, history of PEP,difficult or prolonged attempts at cannulation, and injec-tion of contrast into the PD (including the number of PDinjections and degree of PD filling).1-5,25,26 The underlyingathogenesis of PEP is thought to be multifactorial. Theresumed PEP mechanisms are believed to be pancreaticutflow obstruction as a result of papillary spasm ordema and local injury as a result of manipulation ororceful/repetitive contrast injections causing local inflam-ation. These factors may lead to premature intracellular
ctivation of proteolytic enzymes, which results in furtheramage and enhanced local inflammation, as indicated byncreased levels of cytokines (interleukins 1, 6, and 8). Ifhe inflammation is severe, this also leads to activationf a systemic inflammatory response with multiorgan
TABLE 2. Therapeutic outcomes
PS group,no.
NS group,no.
Pvalue
EST 32 25 .129
EPST 1 0 .485
ENBD, 5F 16 6 .014
ERBD, plastic/metal 12/2 7/1 .134
Manometry 2 0 .243
IDUS 9 6 .378
Intraductal biopsy/cytology
2 6 .269
Precut papillotomy 7 5 .515
Papilla contact, frequency(SD)
10.8 (4.2) 10.9 (5.1) .912
1-9 21 22
10-14 20 22
�15 9 7
Cannulation time, min,mean (SD)
15.9 (6.7) 15 (4.1) .397
Unintentional PDcannulation, no.
6 3 .318
Total procedure time,min, mean (SD)
39.5 (15.8) 35.5 (13.8) .177
PS, 3F plastic stent; NS, nonstent; EST, endoscopic sphincterotomy;EPST, endoscopic pancreatic sphincterotomy; ENBD, endoscopicnasobiliary drainage; ERBD, endoscopic retrograde biliary drainage;IDUS, intraductal US; SD, standard deviation; PD, pancreatic duct.
nvolvement.2,8,9,27-29 r
582 GASTROINTESTINAL ENDOSCOPY Volume 76, No. 3 : 2012
Multiple clinical trials and a meta-analysis demonstratedhat placing PS in high-risk patients effectively reduces thencidence of PEP.8-15,29 Prophylactic placement of PS isow being increasingly adopted as an approach to reducehe risk of PEP. PS was originally introduced to treat PDathology such as strictures and duct leaks. The exactechanism by which PS might reduce PEP risk is not wellnderstood. The stents probably preserve pancreatic drain-ge that otherwise might be impaired by mechanical injury tohe pancreatic sphincter from catheter and guidewire manip-lations and from thermal injury caused by biliary and pan-reatic sphincterotomy or snare ampullectomy. PS placementeduces the frequency of severe PEP.8-15,27-30 Among patientsho had pancreatic drainage in this study, most cases of PEPere mild in severity except 1 case (moderate in severity).At present, the routine use of PS in high-risk cases at
dvanced centers has changed ERCP, reducing the inci-ence and severity of PEP to a more acceptable level. Thisay relax some of the fear factor surrounding a previouslyrohibitively high-risk patient population. However, con-roversy exists regarding which type or length of PS is best.n ideal PS should completely prevent the occurrence ofEP, dislodge spontaneously, deploy easily, and not causetent-induced ductal or parenchymal pancreatic changes.large retrospective study suggested that unflanged, lon-
er length (8-10 cm) 3F polyethylene stents with a singleuodenal pigtail are associated with significantly higherpontaneous dislodgment rates compared with larger cal-ber, shorter length unflanged 4F and 5F stents. That studylso reported a lower incidence of PEP in patients who
TABLE 3. Results of successful 3F pancreatic duct stentplacement
No. of patients (PS group) 50
Technical success, % 48/50 (96)
Pancreatography 41 (85.4)
Acinarization 0
Intramural contrast injection 2 (4.2)
Spontaneous stent dislodgment, % 45/48 (94)
4-cm stent 21/21 (100)
6-cm stent 14/15 (93.3)
8-cm stent 10/12 (83.3)
Stenting duration, d, mean (SD) 3.5 (1.8)
1-3, % 28 (58.3)
4-7, % 17 (35.4)
Endoscopic removal, �7 d 3 (6.3)*
PS, 3F plastic stent; SD, standard deviation.*6 cm (n � 1) and 8 cm (n � 2) in length.
eceived a 3F stent compared with patients who received
www.giejournal.org

l
tPlheag3ples7
cTahbsbwpmh0tsndrwPrd(Wwu
Lee et al 3F pancreatic stent to prevent post-ERCP pancreatitis
a 5F stent, although the difference was not statisticallysignificant.16 Another study by Chahal et al17 comparing
TABLE 4. Post-ERCP pancreatitis in 3F stent group and nonsten
PS group
Pre-/post-ERCP amylase, mean (SD) 103.1 (58.6)/2
Asymptomatic hyperamylasemia, no. (%) 8 (1
Post-ERCP pancreatitis, no. (%) 6 (1
Mild 5 (1
Moderate 1 (2
Severe 0
PS, 3F plastic stent; NS, nonstent; SD, standard deviation.
TABLE 5. Univariate and multivariate analyses of riskfactors
FactorsP
valueOddsratio 95% CI
Univariate analysis
Female .649 1.265 0.460-3.483
Age �40 y .648 1.324 0.397-4.416
Prophylactic pancreaticstent
.031 .327 0.115-0.930
Suspected SOD .339 3.950 0.237-65.931
Periampullarydiverticulum
.975 1.020 0.299-3.472
Cannulation attempts�15
.019 3.944 1.259-12.358
Precut papillotomy .708 .737 0.149-3.652
Endoscopicsphincterotomy
.941 1.037 0.393-2.737
Unintentional PDcannulation
.999
Pancreatography .577 1.500 0.361-6.230
Intramural injection .999
Multivariate analysis
Age �40 y .910 1.084 0.268-4.390
Prophylacticpancreatic stent
.012 0.126 0.025-0.632
Cannulation attempt�15
.025 4.301 1.203-15.380
Suspected SOD .139 11.963 0.448-319.667
CI, Confidence interval; SOD, sphincter of Oddi dysfunction; PD,pancreatic duct.
ong 3F stents with short 5F stents showed that the spon- t
www.giejournal.org V
aneous dislodgment rate of unflanged, short-length, 5FSs (98%) was significantly higher than that for unflanged,ong length, 3F stents (88%) after 14 days in patients atigh-risk of PEP (P � .0001). This decreased the need forndoscopic removal. A higher rate of PS placement failurend PEP, but without statistical difference (14% in 3Froup and 9% in 5F group), was observed in patients withF stents. Recently, Zolotarevsky et al18 reported thatlacement of a 5F compared with a 3F PS for PEP prophy-axis is easier and faster and requires fewer wires. How-ver, there was no statistically significant difference inpontaneous passage rates (5F group, 68.4%; 3F group,5.0 %; P � .617) and PEP rates (P � .519).
However, to date, the use of smaller 3F stents for diffi-ult biliary cannulations has undergone little evaluation.echnically, the failure rate in previous studies for placing3F PD stent after therapeutic ERCP has been significantlyigh (9%–10%).9,17 Deployment of long-length 3F PS maye technically more difficult because of the need for amaller-caliber 0.018- or 0.021-inch guidewire, which cane difficult to maneuver around tortuous PDs comparedith a hydrophilic-tip 0.035-inch guidewire. Long stentlacement also requires deeper guidewire access into theain PD, which may not be possible in patients withighly angulated or tortuous PDs. Thus, a 5F PS with a.035-inch guidewire may be beneficial for easy negotia-ion of the PD and for stent deployment. Accordingly, ourtudy was designed to evaluate the feasibility and useful-ess of the smaller and shorter 3F stents to focus onifficult biliary cannulation as a risk factor for PEP. Thisandomized, controlled trial showed that placing a 3F PSas technically feasible, significantly reduced the rate ofEP during difficult biliary cannulations, and had a higherate of spontaneous dislodgment distally (94%) within 7ays. The technical failure rate for experts was very low4%), and no complications resulted from PS placement.e used a relatively short stent length, such as 4 to 8 cm,ithout an internal flange. A too short duration and these of smaller and shorter stent lengths may not be pro-
up in a difficult cannulation
50) NS group (n � 51) P value
(228.5) 121.3 (87.6)/401.4 (395.7) .224/.024
6 (11.8) .538
15 (29.4) .031
12 (23.5)
2 (3.9)
1 (2)
t gro
(n �
54.1
6)
2)
0)
)
ective against PEP, but our results showed that unflanged
olume 76, No. 3 : 2012 GASTROINTESTINAL ENDOSCOPY 583

dohtirttCssnssqnrstwrs
sdTbsr
R
3F pancreatic stent to prevent post-ERCP pancreatitis Lee et al
small-caliber stents could minimize PD injury and alsofacilitate spontaneous dislodgment.
With regard to procedure-related factors, we focusedon difficult biliary cannulations as a risk factor for PEP.Few data are available on the prophylactic effect of PS ina difficult biliary cannulation. Increasing papillary contactand long duration are known risk factors for PEP, but thedefinition varies in different studies.4,24 Our resultsshowed associations between an increasing risk of PEPand cannulation time, papilla contacts, or unintentionalPD cannulation as a difficult cannulation. With these def-initions, placement of a prophylactic stent significantlyreduced PEP. To date, a consensus holds that prophylacticPS placement is beneficial for preventing PEP in high-riskindividuals.20-23 Patients with difficult cannulations, suchas a longer duration cannulation and frequent papillarycontacts, should be considered a risky group for PEP.Furthermore, whether the stents should be placed after orbefore the therapeutic procedure such as sphincterotomy,stone extraction, and stent placement is unclear, but earlyplacement of a PS may be beneficial because variousprocedure-related factors could contribute to PEP occur-rence. In our study, prophylactic PS placement was per-formed before other biliary therapeutic procedures, ex-cept for biliary sphincterotomy. Removal of difficultcommon bile duct stones (�2 cm or multiple stones)needing mechanical lithotripsy or advanced techniqueswas attempted in a second session of ERCP after place-ment of PS and biliary drainage. In addition, completepancreatography without acinarization was performed in85.4% of the PS group. Others in the PS group and somepatients in the NS group underwent incidental injection ofsmall amounts of contrast without acinarization or com-plete pancreatography. Complete PD opacification or aci-narization is a known risk factor for PEP. However, in ourstudy, we injected contrast to correct the direction of thePD after guidewire cannulation without acinarization.Then, we subsequently inserted the PS for prophylaxis.
The limitations of this study include the following. Ourstudy population was a relatively low-risk cohort. In amulticenter study, the complication rate was highest whenthe indication for ERCP was suspected SOD (21.7%).3 Inour study population, SOD was suspected in only 2 pa-tients (2%) in both groups because of the low incidence ofSOD and because patients who had a history of PEP wereexcluded. However, although the procedure was per-formed by experts in a low-risk cohort, a relatively highrate of PEP might have occurred. Other confounding fac-tors (ie, endoscopic sphincterotomy, endoscopic nasobili-ary drainage, endoscopic retrograde biliary drainage, in-traductal US, and manometry) might have had roles in thedevelopment of complications, and conventional contrastmethods also have an increased risk for complications.31-33
Second, in our study, we did not use a wire-guided can-nulation method at the initiation of cannulation. We used
a wire-guided cannulation method as a rescue method or584 GASTROINTESTINAL ENDOSCOPY Volume 76, No. 3 : 2012
uring pancreatic stenting. Wire-guided cannulation is rec-gnized as an effective method for reducing PEP.31-33 If wead used this method as a primary cannulation method,he rate of PEP may have been further reduced, especiallyn the NS group. Third, the actual stent diameter thatesulted in a lower incidence of PEP was not clear, nor washe most effective duration for retention of the stent withinhe duct for reducing PEP and avoiding ductal changes.onsequently, further follow-up studies using variableizes and lengths of PSs and a second pancreatographytudy to observe stent-related ductal changes may beeeded in selected cases in future studies to distinguishtent-induced ductal changes. Fourth, no definite consen-us criteria exist for difficult biliary cannulations. The fre-uency and time of papillary contact or duration of can-ulation varies in different studies. The technical successate of 3F PS placement also may be different based on thekill and experience of the endoscopist. In our study, all ofhe endoscopic procedures were performed by expertsithout involvement of trainees, so the technical success
ate was relatively higher than that reported in previoustudies and the rate of difficult cannulation was only 6.6%.
In conclusion, prophylactic temporary placement of amall 3F PS was technically feasible and effectively re-uced the rate of PEP during difficult biliary cannulation.he rate of spontaneous dislodgment of the 3F PS was 94%y day 7. Additional large-scale comparative studies oftent length and size should be conducted to confirm ouresults.
EFERENCES
1. Elton E, Howell DA, Parsons WG, et al. Endoscopic pancreatic sphincter-otomy: indications, outcome, and a safe stentless technique. Gastroin-test Endosc 1998;47:240-9.
2. Freeman ML. Adverse outcomes of ERCP. Gastrointest Endosc 2002;56:273-82.
3. Freeman ML, Nelson DB, Sherman S, et al. Complication of biliary endo-scopic sphincterotomy. N Engl J Med 1996;335:909-18.
4. Freeman ML, DiSario JA, Nelson DB, et al. Risk factors for post-ERCPpancreatitis: a prospective, multicenter study. Gastrointest Endosc2001;54:425-34.
5. Freeman ML. Pancreatic stents for prevention of post– endoscopic ret-rograde cholangiopancreatography pancreatitis. Clin GastroenterolHepatol 2007;5:1354-65.
6. Sofuni A, Maguchi H, Itoi T, et al. Prophylaxis of post-endoscopic retro-grade cholangiopancreatography pancreatitis by an endoscopic pan-creatic spontaneous dislodgement stent. Clin Gastroenterol Hepatol2007;5:1339-46.
7. Huibregtse K, Kimmey MB. Endoscopic retrograde cholangiopancre-atography, endoscopic sphincterotomy and endoscopic biliary andpancreatic drainage. In: Yamada T, editor. Textbook of gastroenterol-ogy. Philadelphia (Pa): JB Lippincott; 1995. p. 2590-617.
8. Tarnasky P, Palech Y, Cunningham J, et al. Pancreatic stenting preventspancreatitis after biliary sphincterotomy in patients with sphincter ofOddi dysfunction. Gastroenterology 1998;115:1518-24.
9. Smithline A, Silverman W, Rogers D, et al. Effect of prophylactic mainpancreatic duct stenting on the incidence of biliary endoscopicsphincterotomy-induced pancreatitis in high risk patients. Gastrointest
Endosc 1993;39:652-7.www.giejournal.org

2
2
2
2
2
2
2
2
3
3
3
3
Lee et al 3F pancreatic stent to prevent post-ERCP pancreatitis
10. Harewood GC, Pochron NL, Gostout CJ. Prospective, randomized, controlledtrial of prophylactic pancreatic stent placement for endoscopic snare excisionof the duodenal ampulla. Gastrointest Endosc 2005;62:367-70.
11. Fazel A, Quadri A, Catalano MF, et al. Does a pancreatic duct stent pre-vent post-ERCP pancreatitis? A prospective randomized study. Gastro-intest Endosc 2003;57:291-4.
12. Tsuchiya T, Itoi T, Sofuni A, et al. Temporary pancreatic stent to preventpost endoscopic retrograde cholangiopancreatography pancreatitis: apreliminary, single-center, randomized controlled trial. J HepatobiliaryPancreat Surg 2007;14:302-7.
13. Fogel EL, Eversman D, Jamidar P, et al. Sphincter of Oddi dysfunction:pancreaticobiliary sphincterotomy with pancreatic stent placement hasa lower rate of pancreatitis than biliary sphincterotomy alone. Endos-copy 2002;34:280-5.
14. Aizawa T, Ueno N. Stent placement in the pancreatic duct prevents pan-creatitis after endoscopic sphincter dilation for removal of bile ductstones. Gastrointest Endosc 2001;54:209-13.
15. Singh P, Das A, Isenberg G, et al. Does prophylactic pancreatic stentplacement reduce the risk of post-ERCP acute pancreatitis? A meta-analysis of controlled trials. Gastrointest Endosc 2004;60:544-50.
16. Rashdan A, Fogel EL, McHenry L Jr, et al. Improved stent characteristicsfor prophylaxis of post-ERCP pancreatitis. Clin Gastroenterol Hepatol2004;2:322-9.
17. Chahal P, Tarnasky PR, Petersen BT, et al. Short 5Fr vs long 3Fr pancreaticstents in patients at risk for post-endoscopic retrograde cholangiopan-creatography pancreatitis. Clin Gastroenterol Hepatol 2009;7:834-9.
18. Zolotarevsky E, Fehmi SM, Anderson MA, et al. Prophylactic 5-Fr pancre-atic duct stents are superior to 3-Fr stents: a randomized controlled trial.Endoscopy 2011;43:325-30.
19. Saad AM, Fogel EL, McHenry L, et al. Pancreatic duct stent placementprevents post-ERCP pancreatitis in patients with suspected sphincter ofOddi dysfunction but normal manometry results. Gastrointest Endosc2008;67:255-61.
20. Moffatt DC, Pradermchai K, Avula H, et al. Moderate and severe posten-doscopic retrograde cholangiopancreatography pancreatitis despiteprophylactic pancreatic stent placement: the effect of early prophylac-tic pancreatic stent dislodgement. Can J Gastroenterol 2011;25:215-9.
21. Sherman S, Earle DT, Bucksot L, et al. Does leaving a main pancreatic
duct stent in place reduce the incidence of precut biliary sphincterot-www.giejournal.org V
omy (ES)-induced pancreatitis? A final analysis of a randomizedprospective study. Gastrointest Endosc 1996;43:A489.
2. Choudhary A, Bechtold ML, Arif M, et al. Pancreatic stents for prophy-laxis against post-ERCP pancreatitis: a meta-analysis and systematic re-view. Gastrointest Endosc 2011;73:275-82.
3. Moffatt DC, Coté GA, Fogel EL, et al. Acute pancreatitis after removal ofretained prophylactic pancreatic stents. Gastrointest Endosc 2011;73:980-6.
4. Kaffes AJ, Sriram PV, Rao GV, et al. Early institution of pre-cutting fordifficult biliary cannulation: a prospective study comparing conven-tional vs. a modified technique. Gastrointest Endosc 2005;62:669-74.
5. Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy com-plications and their management: an attempt at consensus. Gastroin-test Endosc 1991;37:383-93.
6. Chen YK, Foliente RL, Santoro MJ, et al. Endoscopic sphincterotomy-induced pancreatitis: increased risk associated with nondilated bileducts and sphincter of Oddi dysfunction. Am J Gastroenterol 1994;89:327-33.
7. Jacob L, Geenen JE, Catalano MF, et al. Prevention of pancreatitis inpatients with idiopathic recurrent pancreatitis: a prospective non-blinded randomized study using endoscopic stents. Endoscopy 2001;33:559-62.
8. Ohshio G, Saluja A, Steer ML. Effects of short-term pancreatic duct ob-struction in rats. Gastroenterology 1991;100:196-202.
9. Lerch MM, Saluja AK, Runzi M, et al. Pancreatic duct obstruction triggersacute necrotizing pancreatitis in the opossum. Gastroenterology 1993;104:853-61.
0. Tarnasky PR, Cunningham JT, Cotton PB, et al. Pancreatic sphincter hy-pertension increases the risk of post-ERCP pancreatitis. Endoscopy1997;29:252-7.
1. Lee TH, Park do H, Park JY, et al. Can wire-guided cannulation preventpost-ERCP pancreatitis? A prospective randomized trial. GastrointestEndosc 2009;69:444-9.
2. Artifon EL, Sakai P, Cunha JE, et al. Guidewire cannulation reduces risk ofpost-ERCP pancreatitis and facilitates bile duct cannulation. Am J Gas-troenterol 2007;102:2147-53.
3. Lella F, Bagnolo F, Colombo E, et al. A simple way of avoiding post-ERCP
pancreatitis. Gastrointest Endosc 2004;59:830-4.olume 76, No. 3 : 2012 GASTROINTESTINAL ENDOSCOPY 585