Embed Size (px)
Citation preview
www.elsevier.com/locate/ajem
American Journal of Emergency Medicine (2012) 30, 1402–1406
Original Contribution
Prospective evaluation of an ED observation unit protocolfor trauma activation patients☆,☆☆
Jessica Holly MD⁎, Joseph Bledsoe MD, Kathryn Black, Riann Robbins, Virgil Davis MD,Philip Bossart MD, Erik Barton MD, MS, MBA, Troy Madsen MD
Department of Surgery, Division of Emergency Medicine, University of Utah School of Medicine, Salt Lake City, UT 84132, USA
Received 27 August 2011; revised 3 October 2011; accepted 8 October 2011
AbstractBackground: The University of Utah emergency department (ED) observation unit (EDOU) cares forover 2500 patients each year, with a significant portion of these patients being trauma activationpatients. We evaluated the safety and efficacy of our EDOU trauma protocol and described patientcharacteristics and outcomes of trauma patients managed in an EDOU.Methods: We performed a prospective observational study of all trauma patients admitted to the EDOUover a 1-year period. Patient disposition, interventions, and adverse events during observation wererecorded. Thirty-day follow-up was performed by telephone and chart review to evaluate for missedinjuries, repeat hospitalizations, or repeat traumatic events.Results: A total of 259 trauma patients were admitted to the EDOU during the study period and werecontacted at least 30 days after discharge. There were no deaths, intubations, or other adverse events. At30-day follow-up, there was 1 missed injury, which did not result in an adverse outcome. Ten patientswere reevaluated in the ED or required hospitalization for events occurring after their initial EDOU staybut related to their initial trauma evaluation. The inpatient admission rate from the EDOU was 10.4%,and 3.1% of patients reported another traumatic event during the 30-day follow-up period.Conclusions: There were no adverse outcomes in trauma patients admitted to the EDOU, and ourinpatient admission rate was within the generally accepted admission rate for patients in observationstatus. The EDOU appears to be a safe alternative to inpatient admission for the evaluation of minimallyinjured trauma activation patients.© 2012 Elsevier Inc. All rights reserved.
1. Introduction
Many trauma activation patients do not have injuriesrequiring hospital admission identified on initial traumaevaluation. However, these patients may have potential
☆ Funding sources/disclosures: Quality improvement grant from theUniversity of Utah Medical Group.
☆☆ Prior presentations: Western Regional Society for AcademicEmergency Medicine Meeting, February 2010.
⁎ Corresponding author. Tel.: +1 530 848 4054.E-mail address: [email protected] (J. Holly).
0735-6757/$ – see front matter © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.ajem.2011.10.012
injuries based on mechanism that require continuedobservation, further diagnostic tests, and serial examinationsrather than discharge. Emergency department (ED) observa-tion units (EDOUs) present an alternative to admission to aninpatient unit. Previous studies have shown that EDOUscan be successful in managing specific patient populations,including low-risk chest pain, pediatric dehydration, andasthma [1-5]. We previously reported that EDOUs areappropriate for minimally injured trauma activation patients[6]. There have been small studies reporting observation unitadmission of specific groups of trauma patients [7-10]. No

1403Observation unit and trauma activation patients
prospective studies have reported on the use of EDOUs forall types of trauma patients.
An appropriate rate of hospital admission from an EDOUsuggests effectiveness. An admission rate that is too highraises concerns about delays in inpatient therapy andincreased resources. Patients who require a more prolongedstay would ideally be admitted to an inpatient unit from theED, rather than placed in an observation unit only to be lateradmitted [2,11,12]. Alternatively, a very low admission rateraises questions about the necessity of observation ratherthan simple discharge from the ED. Generally acceptedadmission rates of 10% to 15% have been reported in theliterature [13-17]. Inpatient admission rates from observationunits are regularly tracked and are used as a marker forappropriate patient selection for the EDOU. In addition,missed injuries or need for readmission in patients dis-charged from an EDOU may indicate incomplete evaluationor too brief a period of observation.
Our goals were to prospectively evaluate the utility andsafety of an observation unit protocol for trauma patientswho presented to our level I trauma center and to describepatient characteristics and outcomes of trauma patientsmanaged in an EDOU.
2. Methods
The study design was a prospective observational studyof all trauma patients admitted to our EDOU with 30-dayfollow-up. The study setting was an academic ED in a level Itrauma center, which opened an observation unit in April2006. The University of Utah ED is located in Salt Lake City,Utah, with an annual volume of approximately 39 000patients and is one of 2 level I trauma centers in a regionserving Utah, Nevada, Idaho, Wyoming, and parts ofColorado, Montana, Arizona, and New Mexico. The EDOUis managed by the ED and cares for over 2500 patients peryear with a significant number of the patients being traumaactivation patients, all of whom are managed under a specifictrauma protocol.
Admission to the observation unit was at the discretion ofthe trauma team and the attending emergency physician. Theprotocol was tailored to the individual trauma patient. Patientsgenerally received intravenous fluids, pain medications, vitalsigns monitoring, and serial hematocrit testing. Additionalcomponents of the protocol for selected patients includedregular neurologic examinations, repeat head computedtomography (CT) scan for head injury patients, vas-cular/neurologic examinations for patients with orthopedicinjuries, serial abdominal examinations for patients withabdominal trauma, and repeat chest x-ray for patients withchest trauma. Patients were under the primary oversight of amidlevel provider while in the EDOU, with the supervision ofthe attending ED physician and with the trauma serviceconsulting as needed during the overnight stay and consulting
before patient discharge. Midlevel providers were present inthe ED 21 hours per day, and they performed serial abdominalexaminations, reviewed results of additional testing per-formed in the EDOU, and involved the trauma service andadditional consulting services as needed. Trauma patientswere excluded from observation unit admission if they hadabnormal vital signs, a positive focused assessment withsonography for trauma examination, abnormal electrocardio-graph, abnormal chest radiograph, Glasgow Coma Score(GCS) less than 14, or multiple system injury involvement.
We performed a prospective evaluation of all patientsadmitted to the observation unit under the trauma protocol forthe 13-month period from June 1, 2009, to July 1, 2010. Thestudy received approval from the hospital's institutionalreview board in October 2007, and all participants providedinformed written consent for participation and contact viatelephone at 30 days. Trained research associates staffed theobservation unit 7 days a week to obtain baseline data on allpatients placed in the EDOU under the trauma protocol.Baseline data were recorded at the time of the patient's EDOUadmission. We documented events during the EDOUadmission, including disposition from the EDOU, interven-tions during the EDOU stay, and any adverse outcomes (lossof vital signs, intubation, or death) during the observationperiod. Patient outcomes during 30-day follow-up weredetermined through telephone contact with patients andreview of the electronic medical record at least 30 days afterthe EDOU admission. Outcomes measured at 30-day follow-up included injuries not identified while in observation,repeat ED visits or hospitalizations since observation dis-charge, and repeat trauma. Results are reported using descrip-tive statistics (SPSS v. 17.0. SPSS Inc., Chicago, IL.).
3. Results
During the 13-month study period, 259 trauma activationpatients were admitted to the observation unit under thetrauma protocol. Patient age ranged from 14 to 81 years witha median of 35 years. Of the patients, 19.7% were intoxicatedat the time of arrival, and 73.9% were male; 9.7% of thepatients presented as trauma I activations, 65.6% presentedas trauma II activations, and 24.7% were either trauma IIIactivations or did not meet the initial criteria for traumaactivation. Most of the patients (91.1%) had an initial GCS of15, 7.7% had an initial GCS of 14, and 1.2% had an initialGCS of 13. Although a GCS less than 14 at the time ofEDOU admission was an exclusion criteria, a GCS less than14 at the trauma evaluation was not. Of the patients, 49.6%reported an initial loss of consciousness (Table 1). The mostcommon specific injury mechanisms were motor vehicleaccidents, falls, and skiing/snowboarding injuries (Table 2).
We were able to contact 54.4% of the patients via tele-phone and, for all others, reviewed the medical record toevaluate for any return visits for adverse outcomes during the

Table 1 Baseline characteristics
Patient baseline characteristics n (%)
Total 259Age (y), range (median) 14-81 (35)Male 191 (73.9%)GCSGCS 15 236 (91.1%)GCS 14 20 (7.7%)GCS 13 3 (1.2%)Trauma activationTrauma I 25 (9.7%)Trauma II 170 (65.6%)Trauma III or none 64 (24.7%)Loss of consciousness 128 (49.6%)Intoxication 51 (19.7%)
Table 3 Indication for inpatient admission from the EDOU
n Indications for admission
7 Operating room6 Continued observation5 Injury related to trauma5 Pain control or other disposition issue4 Medical condition unrelated to trauma
1404 J. Holly et al.
follow-up period. We also reviewed the electronic medicalrecord (EMR) to confirm the details of any events patientsreported during the telephone contact. Of note, we did notfind that there were any events during the follow-up periodthat patients reported via telephone that were not alsodocumented in the medical record.
There were no deaths, intubations, loss of vital signs, orother adverse outcomes for patients admitted to the obser-vation unit under the trauma protocol. During the initialobservation period, 27 (10.4%) patients required inpatienthospital admission during their EDOU stay. Of thesepatients, 5 were admitted for an injury previously identifiedon their initial trauma evaluation, 6 patients were admittedfor continued observation, 7 patients were taken none-mergently to the operating room from the EDOU, 4 patientswere admitted for a medical condition unrelated to theirtrauma, and 5 patients were admitted for pain control or otherdisposition issue (Table 3). Of the patients who were takento the operating room from the EDOU, 4 patients hadorthopedic injuries (thoracic spine fracture, tibia fracture,finger amputation, and ulna fracture). All of these patients
Table 2 Mechanism of injury
Mechanism n % of total
Motor vehicle accident 79 30.5Fall 54 20.9Skiing/snowboarding 31 12.0Motorcycle accident 22 8.5Bicycle 16 6.2Stab wound 14 5.4Assault 13 5.0Auto vs pedestrian 9 3.5Other 5 1.9All-terrain vehicle 4 1.5Burn 4 1.5Gunshot wound 4 1.5Horse 3 1.2Boat 1 0.4
were initially to be managed with outpatient procedures andwere admitted to the EDOU for observation. The orthopedicservice reevaluated the patients in the morning and decidedto take the patients to the operating room. None of thesepatients had urgent indications for surgery. Two additionalpatients were taken to the operating room for irrigation anddebridement of stab wounds, and 1 patient was taken for thedevelopment of compartment syndrome in an extremity thatdid not have a fracture.
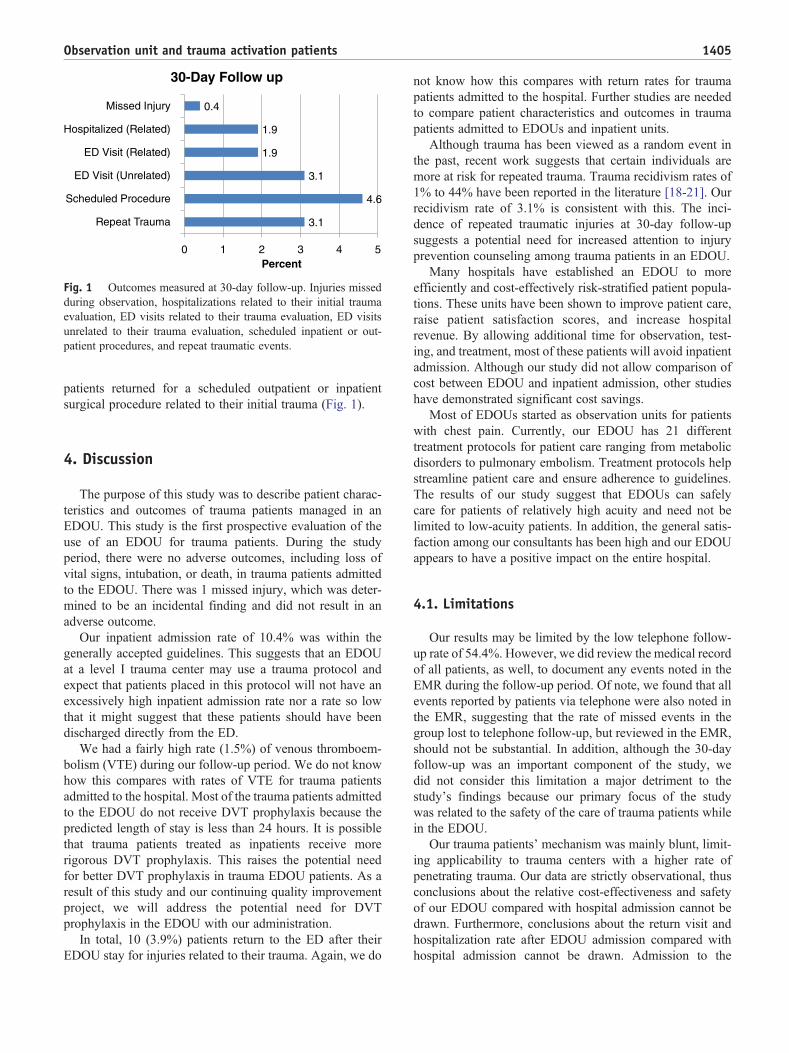
During the 30 days after patients' discharge from theobservation unit, 27 (10.4%) patients returned to the ED. Inonly 1 (0.4%) of these patients was an injury identified thathad not been noted during the observation visit: an internalcarotid artery dissection. The patient had been involved in aski accident, and her initial trauma evaluation includednegative CT of her head, cervical spine, and facial bones.The patient returned 12 days after her trauma evaluation forpersistent headache and lightheadedness. Computed tomo-graphic angiogram of the neck showed an internal carotidartery dissection. Neurology evaluated the patient and feltthat it was an incidental finding and not the cause of thepatient's symptoms. The patient was not started on heparinand was discharged home from the ED. Two (0.8%) patientswho returned to the ED during the 30-day follow-up periodrequired hospitalization for injuries related to the initial EDtrauma evaluation: 1 patient had recurrence of a knownpleural effusion, and 1 required readmission for pain control.Three (1.2%) additional patients required hospitalizationfor events occurring after their initial EDOU stay but relatedto the trauma: 1 patient developed a pulmonary embolism1 week after a motorcycle collision, 1 patient developed adeep venous thrombosis (DVT) in a leg that had sustained astab wound, and 1 patient developed urosepsis 1 week aftera motor vehicle accident possibly related to Foley catheter-ization during the initial ED trauma evaluation and EDOUstay. Five (1.9%) patients were reevaluated in the ED anddischarged home for findings related to their initial traumaevaluation: 2 of these patients had developed DVTs in the legthat had sustained injury during their initial trauma, 2 morepatients had developed wound infections, and 1 patient haddeveloped seizure-like symptoms and was diagnosed withtraumatic brain injury by neurology. Eight (3.1%) patientspresented to the ED for repeat traumatic events that occurredduring the follow-up period. An additional 8 (3.1%) patientsreturned to the ED for a complaint unrelated to their trauma.During the 30 days after patients' discharge, 12 (4.6%)
3.1
4.6
3.1
1.9
1.9
0.4
0 1 2 3 4 5
Repeat Trauma
Scheduled Procedure
ED Visit (Unrelated)
ED Visit (Related)
Hospitalized (Related)
Missed Injury
Percent
30-Day Follow up
Fig. 1 Outcomes measured at 30-day follow-up. Injuries missedduring observation, hospitalizations related to their initial traumaevaluation, ED visits related to their trauma evaluation, ED visitsunrelated to their trauma evaluation, scheduled inpatient or out-patient procedures, and repeat traumatic events.
1405Observation unit and trauma activation patients
patients returned for a scheduled outpatient or inpatientsurgical procedure related to their initial trauma (Fig. 1).
4. Discussion
The purpose of this study was to describe patient charac-teristics and outcomes of trauma patients managed in anEDOU. This study is the first prospective evaluation of theuse of an EDOU for trauma patients. During the studyperiod, there were no adverse outcomes, including loss ofvital signs, intubation, or death, in trauma patients admittedto the EDOU. There was 1 missed injury, which was deter-mined to be an incidental finding and did not result in anadverse outcome.
Our inpatient admission rate of 10.4% was within thegenerally accepted guidelines. This suggests that an EDOUat a level I trauma center may use a trauma protocol andexpect that patients placed in this protocol will not have anexcessively high inpatient admission rate nor a rate so lowthat it might suggest that these patients should have beendischarged directly from the ED.
We had a fairly high rate (1.5%) of venous thromboem-bolism (VTE) during our follow-up period. We do not knowhow this compares with rates of VTE for trauma patientsadmitted to the hospital. Most of the trauma patients admittedto the EDOU do not receive DVT prophylaxis because thepredicted length of stay is less than 24 hours. It is possiblethat trauma patients treated as inpatients receive morerigorous DVT prophylaxis. This raises the potential needfor better DVT prophylaxis in trauma EDOU patients. As aresult of this study and our continuing quality improvementproject, we will address the potential need for DVTprophylaxis in the EDOU with our administration.
In total, 10 (3.9%) patients return to the ED after theirEDOU stay for injuries related to their trauma. Again, we do
not know how this compares with return rates for traumapatients admitted to the hospital. Further studies are neededto compare patient characteristics and outcomes in traumapatients admitted to EDOUs and inpatient units.
Although trauma has been viewed as a random event inthe past, recent work suggests that certain individuals aremore at risk for repeated trauma. Trauma recidivism rates of1% to 44% have been reported in the literature [18-21]. Ourrecidivism rate of 3.1% is consistent with this. The inci-dence of repeated traumatic injuries at 30-day follow-upsuggests a potential need for increased attention to injuryprevention counseling among trauma patients in an EDOU.
Many hospitals have established an EDOU to moreefficiently and cost-effectively risk-stratified patient popula-tions. These units have been shown to improve patient care,raise patient satisfaction scores, and increase hospitalrevenue. By allowing additional time for observation, test-ing, and treatment, most of these patients will avoid inpatientadmission. Although our study did not allow comparison ofcost between EDOU and inpatient admission, other studieshave demonstrated significant cost savings.
Most of EDOUs started as observation units for patientswith chest pain. Currently, our EDOU has 21 differenttreatment protocols for patient care ranging from metabolicdisorders to pulmonary embolism. Treatment protocols helpstreamline patient care and ensure adherence to guidelines.The results of our study suggest that EDOUs can safelycare for patients of relatively high acuity and need not belimited to low-acuity patients. In addition, the general satis-faction among our consultants has been high and our EDOUappears to have a positive impact on the entire hospital.
4.1. Limitations
Our results may be limited by the low telephone follow-up rate of 54.4%. However, we did review the medical recordof all patients, as well, to document any events noted in theEMR during the follow-up period. Of note, we found that allevents reported by patients via telephone were also noted inthe EMR, suggesting that the rate of missed events in thegroup lost to telephone follow-up, but reviewed in the EMR,should not be substantial. In addition, although the 30-dayfollow-up was an important component of the study, wedid not consider this limitation a major detriment to thestudy's findings because our primary focus of the studywas related to the safety of the care of trauma patients whilein the EDOU.
Our trauma patients' mechanism was mainly blunt, limit-ing applicability to trauma centers with a higher rate ofpenetrating trauma. Our data are strictly observational, thusconclusions about the relative cost-effectiveness and safetyof our EDOU compared with hospital admission cannot bedrawn. Furthermore, conclusions about the return visit andhospitalization rate after EDOU admission compared withhospital admission cannot be drawn. Admission to the

1406 J. Holly et al.
EDOU was at physician discretion; thus, the generalizabilityto other settings and practice patterns cannot be predicted.
5. Conclusions
There were no adverse outcomes in trauma patientsadmitted to the observation unit. There was 1 missed injury,which was determined to be an incidental finding and did notresult in an adverse outcome. Our inpatient admission rate iswithin the generally accepted admission rate for patients inobservation status. The observed rate of VTE after EDOUadmission raises the potential need for better DVT pro-phylaxis in trauma EDOU patients. The incidence of repeattraumatic injuries in 30-day follow-up suggests a potentialneed for increased attention to injury prevention counselingamong trauma patients in an EDOU. The observation unitappears to be a safe alternative to inpatient admission for theevaluation of minimally injured trauma activation patients.Further studies are needed to compare patient characteristicsand outcomes in trauma patients admitted to EDOUs andinpatient units.
References
[1] Amsterdam EA, et al. Exercise testing in chest pain units: rationale,implementation, and results. Cardiol Clin 2005;23(4):503-16 vii.
[2] Brillman J, et al. Management of observation units. American Collegeof Emergency Physicians. Ann Emerg Med 1995;25(6):823-30.
[3] Cross E, How S, Goodacre S. Development of acute chest painservices in the UK. Emerg Med J 2007;24(2):100-2.
[4] Mallory MD, et al. Use of a pediatric observation unit for treatment ofchildren with dehydration caused by gastroenteritis. Pediatr EmergCare 2006;22(1):1-6.
[5] Miescier MJ, et al. Children with asthma admitted to a pediatricobservation unit. Pediatr Emerg Care 2005;21(10):645-9.
[6] Madsen TE, Bledsoe JR, Bossart PJ. Observation unit admission as analternative to inpatient admission for trauma activation patients. EmergMed J 2009;26(6):421-3.
[7] Henneman PL, et al. The use of an emergency department observationunit in the management of abdominal trauma. Ann Emerg Med 1989;18(6):647-50.
[8] Ammons MA, Moore EE, Rosen P. Role of the observation unit in themanagement of thoracic trauma. J Emerg Med 1986;4(4):279-82.
[9] Holsti M, et al. Pediatric closed head injuries treated in an observationunit. Pediatr Emerg Care 2005;21(10):639-44.
[10] Ochoa-Gomez J, et al. Attendance of patients with minor head injury inan emergency department observation ward. Eur J Emerg Med2000;7(4):267-70.
[11] Daly S, Campbell DA, Cameron PA. Short-stay units and observationmedicine: a systematic review. Med J Aust 2003;178(11):559-63.
[12] Martinez E, et al. The observation unit: a new interface betweeninpatient and outpatient care. Am J Med 2001;110(4):274-7.
[13] Roberts R, Graff LGt. Economic issues in observation unit medicine.Emerg Med Clin North Am 2001;19(1):19-33.
[14] Goodacre SW. Should we establish chest pain observation units in theUK? A systematic review and critical appraisal of the literature.J Accid Emerg Med 2000;17(1):1-6.
[15] Farkouh ME, et al. A clinical trial of a chest-pain observation unit forpatients with unstable angina. Chest Pain Evaluation in the EmergencyRoom (CHEER) Investigators. N Engl J Med 1998;339(26):1882-8.
[16] Crenshaw LA, et al. An evaluation of emergency physician selectionof observation unit patients. Am J Emerg Med 2006;24(3):271-9.
[17] Wilkinson K, Severance H. Identification of chest pain patientsappropriate for an emergency department observation unit. Emerg MedClin North Am 2001;19(1):35-66.
[18] Hedges BE, et al. Characteristics of repeat trauma patients, San DiegoCounty. Am J Public Health 1995;85(7):1008-10.
[19] Sims DW, et al. Urban trauma: a chronic recurrent disease. J Trauma1989;29(7):940-6 [discussion 946-7].
[20] Morrissey TB, Byrd CR, Deitch EA. The incidence of recurrentpenetrating trauma in an urban trauma center. J Trauma 1991;31(11):1536-8.
[21] Cesare J, et al. Characteristics of blunt and personal violent injuries.J Trauma 1990;30(2):176-82.