Embed Size (px)
Citation preview

Biol Blood Marrow Transplant 20 (2014) 46e52
American Society for BloodASBMTand Marrow Transplantation
Clinical Research
Protective Effect of Cytomegalovirus Reactivation onRelapse after Allogeneic Hematopoietic Cell Transplantationin Acute Myeloid Leukemia Patients Is Influenced byConditioning Regimen
Shivaprasad Manjappa 1, Pavan Kumar Bhamidipati 1,Keith E. Stokerl-Goldstein 2, John F. DiPersio 2, Geoffrey L. Uy 2,Peter Westervelt 2, Jingxia Liu 3, Mark A. Schroeder 2, Ravi Vij 2,Camille N. Abboud 2, Todd A. Fehniger 2, Amanda F. Cashen 2, Iskra Pusic 2,Meagan Jacoby 2, Srinidhi J. Meera 2, Rizwan Romee 2,*
1Division of Hospital Medicine, Department of Medicine, Washington University School of Medicine, St. Louis, Missouri2 Section of Bone Marrow Transplant and Leukemia, Department of Medicine, Washington University School of Medicine, St. Louis,Missouri3Division of Biostatistics, Washington University School of Medicine, St. Louis, Missouri
Article history:
Received 27 August 2013Accepted 2 October 2013Key Words:CMVAcute myeloid leukemiaRelapseAllogeneic hematopoietic celltransplantationMyeloablativeReduced intensity
S.M. and P.K.B. contributed equalFinancial disclosure: See Acknowle* Correspondence and reprint re
Oncology/BMT and Leukemia SecMedicine, Campus Box 8007, 660 S
E-mail address: [email protected]
1083-8791/$ e see front matter �http://dx.doi.org/10.1016/j.bbmt.20
a b s t r a c tCytomegalovirus (CMV) reactivation after allogeneic hematopoietic cell transplant (allo-HCT) has beenassociated with a reduced risk of relapse in patients with acute myeloid leukemia (AML). However, the in-fluence of the conditioning regimen on this protective effect of CMV reactivation after allo-HCT is relativelyunexplored. To address this, we evaluated the risk of relapse in 264 AML patients who received T cellereplete,6/6 HLA matched sibling or 10/10 HLA matched unrelated donor transplantation at a single institution be-tween 2006 and 2011. Of these 264 patients, 206 received myeloablative (MA) and 58 received reduced-intensity conditioning (RIC) regimens. CMV reactivation was observed in 88 patients with MA conditioningand 37 patients with RIC. At a median follow-up of 299 days, CMV reactivation was associated with signif-icantly lower risk of relapse in patients who received MA conditioning both in univariate (P ¼ .01) andmultivariate analyses (hazard ratio, .5246; P ¼ .006); however, CMV reactivation did not significantly affectthe risk of relapse in our RIC cohort. These results confirm the protective effect of CMV reactivation on relapsein AML patients after allo-HCT reported by previous studies but suggest this protective effect of CMV reac-tivation on relapse is influenced by the conditioning regimen used with the transplant.
� 2014 American Society for Blood and Marrow Transplantation.
INTRODUCTION et al. [7] found a modest protection against relapse in AML
Cytomegalovirus (CMV) is a double-stranded DNA b her-pes virus that is generally of no major clinical significance inhealthy immunocompetent hosts but is responsible for sig-nificant morbidity and mortality in immunocompromisedpatients [1,2]. In patients with allogeneic hematopoietic celltransplant (allo-HCT), the incidence of CMV disease has beensignificantly reduced because of early detection of CMVreactivation and use of pre-emptive antiviral therapy. In spiteof this, CMV reactivation remains a significant cause formorbidity and mortality among allo-HCT patients [3-5].Interestingly, in a recent study by Elmaagacli et al. [6], earlyCMV pp65 antigenemia after allo-HCT was associated withreduced risk of relapse in acute myeloid leukemia (AML)patients. This study included a relatively homogeneouspopulation who underwent fully matched allo-HCT withmyeloablative (MA) conditioning. In a large cohort ofpatients, using CMV pp65 antigenemia monitoring, Green
ly to this study.dgments on page 51.quests: Rizwan Romee, MD, Division oftion, Washington University School ofouth Euclid Ave., St. Louis, MO 63110.ustl.edu (R. Romee).
2014 American Society for Blood and Marrow13.10.003
patients after allo-HCT, which included both MA andreduced-intensity conditioning (RIC) patients, but the co-horts were analyzed together with no subgroup analysis.Currently, the influence of conditioning regimen on thisprotective effect of CMV reactivation on the risk of relapse isrelatively unexplored. Quantitative CMV PCR (qPCR) is amore sensitive assay compared with pp65 antigenemia forCMV detection and has been shown to assist in early detec-tion of CMV reactivation after allo-HCT, leading to promptpre-emptive treatment of CMV viremia [3,8,9]. Whetherimplementing CMV qPCR instead of pp65 antigenemia assayalters this association of reduced relapse risk with CMVreactivation after allo-HCT in AML patients is also currentlynot known. To address these questions, we retrospectivelyanalyzed 264 AML patients who received T cellereplete, 6/6HLA matched sibling or 10/10 HLA matched unrelated donortransplantation at a single institution between 2006and 2011.
METHODSStudy Population
The study included a total of 382 consecutive AML patients who un-derwent allo-HCT at Washington University Medical Center at St. Louisbetween January 2006 and December 2011. This study was approved by the
Transplantation.
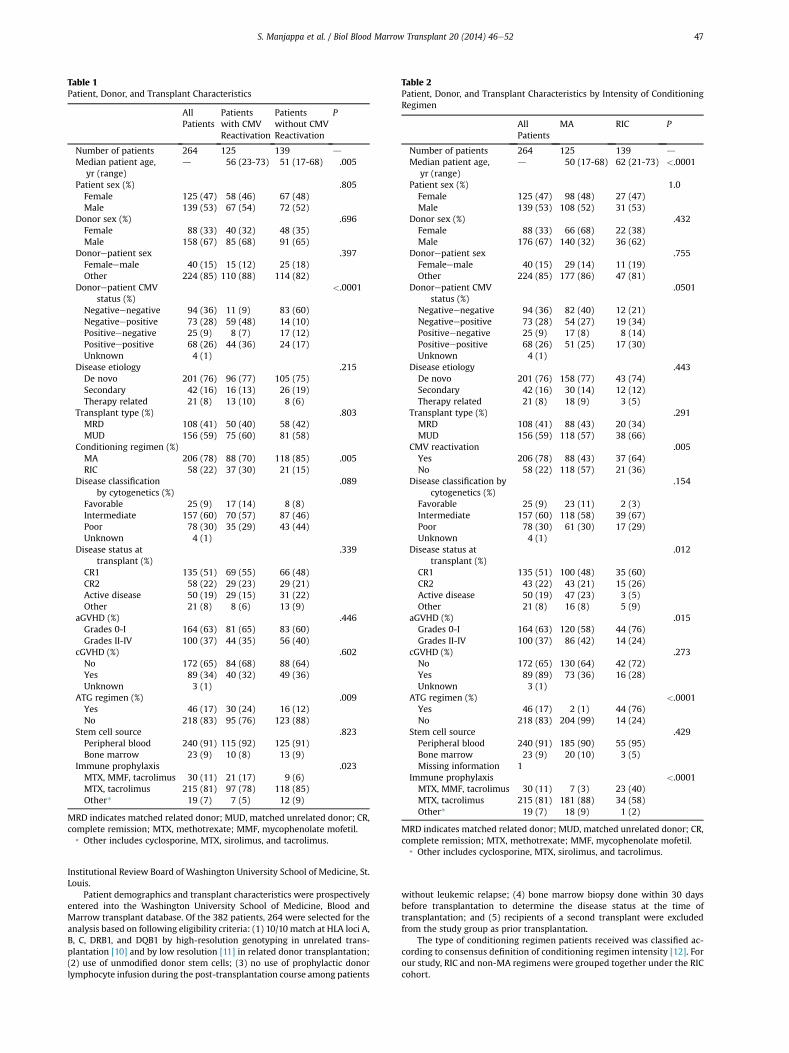
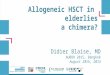
Table 2Patient, Donor, and Transplant Characteristics by Intensity of ConditioningRegimen
AllPatients
MA RIC P
Number of patients 264 125 139 d
Median patient age,yr (range)
d 50 (17-68) 62 (21-73) <.0001
Patient sex (%) 1.0Female 125 (47) 98 (48) 27 (47)Male 139 (53) 108 (52) 31 (53)
Donor sex (%) .432Female 88 (33) 66 (68) 22 (38)Male 176 (67) 140 (32) 36 (62)
Donorepatient sex .755Femaleemale 40 (15) 29 (14) 11 (19)Other 224 (85) 177 (86) 47 (81)
Donorepatient CMVstatus (%)
.0501
Negativeenegative 94 (36) 82 (40) 12 (21)Negativeepositive 73 (28) 54 (27) 19 (34)Positiveenegative 25 (9) 17 (8) 8 (14)Positiveepositive 68 (26) 51 (25) 17 (30)Unknown 4 (1)
Disease etiology .443De novo 201 (76) 158 (77) 43 (74)Secondary 42 (16) 30 (14) 12 (12)Therapy related 21 (8) 18 (9) 3 (5)
Transplant type (%) .291MRD 108 (41) 88 (43) 20 (34)MUD 156 (59) 118 (57) 38 (66)
CMV reactivation .005Yes 206 (78) 88 (43) 37 (64)No 58 (22) 118 (57) 21 (36)
Disease classification bycytogenetics (%)
.154
Favorable 25 (9) 23 (11) 2 (3)Intermediate 157 (60) 118 (58) 39 (67)Poor 78 (30) 61 (30) 17 (29)Unknown 4 (1)
Disease status attransplant (%)
.012
CR1 135 (51) 100 (48) 35 (60)CR2 43 (22) 43 (21) 15 (26)Active disease 50 (19) 47 (23) 3 (5)Other 21 (8) 16 (8) 5 (9)
aGVHD (%) .015Grades 0-I 164 (63) 120 (58) 44 (76)Grades II-IV 100 (37) 86 (42) 14 (24)
cGVHD (%) .273No 172 (65) 130 (64) 42 (72)Yes 89 (89) 73 (36) 16 (28)Unknown 3 (1)
ATG regimen (%) <.0001Yes 46 (17) 2 (1) 44 (76)No 218 (83) 204 (99) 14 (24)
Stem cell source .429Peripheral blood 240 (91) 185 (90) 55 (95)Bone marrow 23 (9) 20 (10) 3 (5)Missing information 1
Immune prophylaxis <.0001MTX, MMF, tacrolimus 30 (11) 7 (3) 23 (40)MTX, tacrolimus 215 (81) 181 (88) 34 (58)Other* 19 (7) 18 (9) 1 (2)
MRD indicates matched related donor; MUD, matched unrelated donor; CR,complete remission; MTX, methotrexate; MMF, mycophenolate mofetil.
* Other includes cyclosporine, MTX, sirolimus, and tacrolimus.
Table 1Patient, Donor, and Transplant Characteristics
AllPatients
Patientswith CMVReactivation
Patientswithout CMVReactivation
P
Number of patients 264 125 139 d
Median patient age,yr (range)
d 56 (23-73) 51 (17-68) .005
Patient sex (%) .805Female 125 (47) 58 (46) 67 (48)Male 139 (53) 67 (54) 72 (52)
Donor sex (%) .696Female 88 (33) 40 (32) 48 (35)Male 158 (67) 85 (68) 91 (65)
Donorepatient sex .397Femaleemale 40 (15) 15 (12) 25 (18)Other 224 (85) 110 (88) 114 (82)
Donorepatient CMVstatus (%)
<.0001
Negativeenegative 94 (36) 11 (9) 83 (60)Negativeepositive 73 (28) 59 (48) 14 (10)Positiveenegative 25 (9) 8 (7) 17 (12)Positiveepositive 68 (26) 44 (36) 24 (17)Unknown 4 (1)
Disease etiology .215De novo 201 (76) 96 (77) 105 (75)Secondary 42 (16) 16 (13) 26 (19)Therapy related 21 (8) 13 (10) 8 (6)
Transplant type (%) .803MRD 108 (41) 50 (40) 58 (42)MUD 156 (59) 75 (60) 81 (58)
Conditioning regimen (%)MA 206 (78) 88 (70) 118 (85) .005RIC 58 (22) 37 (30) 21 (15)
Disease classificationby cytogenetics (%)
.089
Favorable 25 (9) 17 (14) 8 (8)Intermediate 157 (60) 70 (57) 87 (46)Poor 78 (30) 35 (29) 43 (44)Unknown 4 (1)
Disease status attransplant (%)
.339
CR1 135 (51) 69 (55) 66 (48)CR2 58 (22) 29 (23) 29 (21)Active disease 50 (19) 29 (15) 31 (22)Other 21 (8) 8 (6) 13 (9)
aGVHD (%) .446Grades 0-I 164 (63) 81 (65) 83 (60)Grades II-IV 100 (37) 44 (35) 56 (40)
cGVHD (%) .602No 172 (65) 84 (68) 88 (64)Yes 89 (34) 40 (32) 49 (36)Unknown 3 (1)
ATG regimen (%) .009Yes 46 (17) 30 (24) 16 (12)No 218 (83) 95 (76) 123 (88)
Stem cell source .823Peripheral blood 240 (91) 115 (92) 125 (91)Bone marrow 23 (9) 10 (8) 13 (9)
Immune prophylaxis .023MTX, MMF, tacrolimus 30 (11) 21 (17) 9 (6)MTX, tacrolimus 215 (81) 97 (78) 118 (85)Other* 19 (7) 7 (5) 12 (9)
MRD indicates matched related donor; MUD, matched unrelated donor; CR,complete remission; MTX, methotrexate; MMF, mycophenolate mofetil.
* Other includes cyclosporine, MTX, sirolimus, and tacrolimus.
S. Manjappa et al. / Biol Blood Marrow Transplant 20 (2014) 46e52 47
Institutional Review Board of Washington University School of Medicine, St.Louis.
Patient demographics and transplant characteristics were prospectivelyentered into the Washington University School of Medicine, Blood andMarrow transplant database. Of the 382 patients, 264 were selected for theanalysis based on following eligibility criteria: (1) 10/10 match at HLA loci A,B, C, DRB1, and DQB1 by high-resolution genotyping in unrelated trans-plantation [10] and by low resolution [11] in related donor transplantation;(2) use of unmodified donor stem cells; (3) no use of prophylactic donorlymphocyte infusion during the post-transplantation course among patients
without leukemic relapse; (4) bone marrow biopsy done within 30 daysbefore transplantation to determine the disease status at the time oftransplantation; and (5) recipients of a second transplant were excludedfrom the study group as prior transplantation.
The type of conditioning regimen patients received was classified ac-cording to consensus definition of conditioning regimen intensity [12]. Forour study, RIC and non-MA regimens were grouped together under the RICcohort.
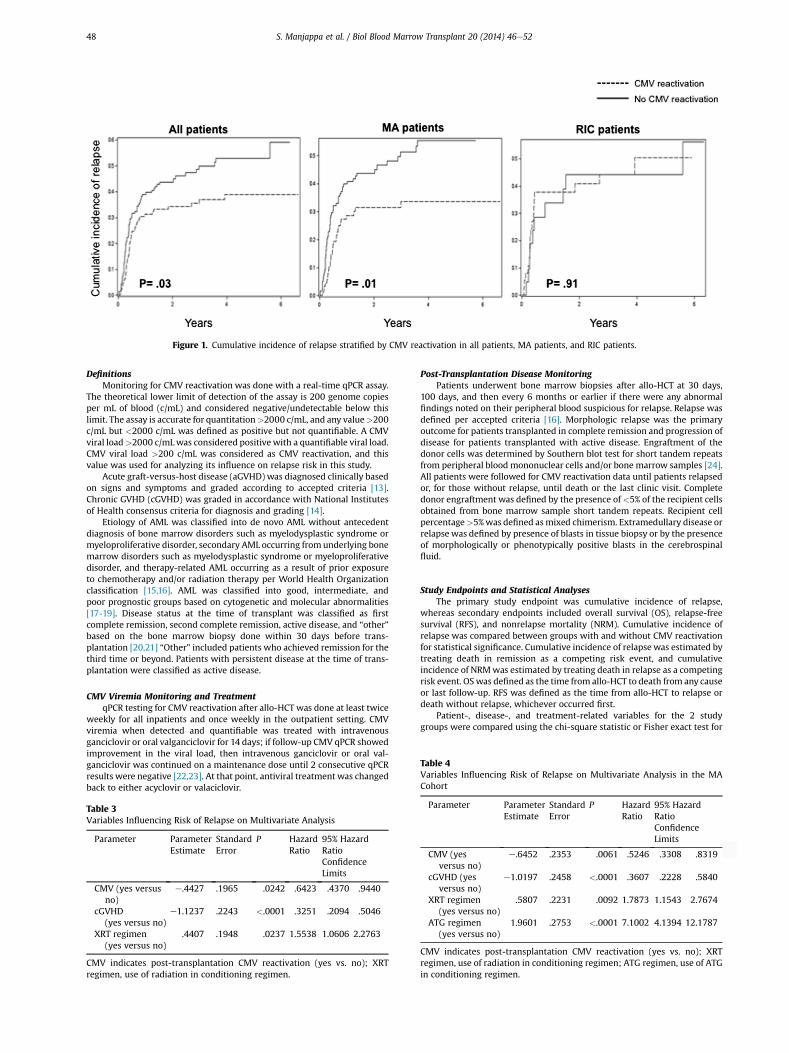
Table 4Variables Influencing Risk of Relapse on Multivariate Analysis in the MACohort
Figure 1. Cumulative incidence of relapse stratified by CMV reactivation in all patients, MA patients, and RIC patients.
S. Manjappa et al. / Biol Blood Marrow Transplant 20 (2014) 46e5248
DefinitionsMonitoring for CMV reactivation was done with a real-time qPCR assay.
The theoretical lower limit of detection of the assay is 200 genome copiesper mL of blood (c/mL) and considered negative/undetectable below thislimit. The assay is accurate for quantitation>2000 c/mL, and any value>200c/mL but <2000 c/mL was defined as positive but not quantifiable. A CMVviral load>2000 c/mLwas considered positivewith a quantifiable viral load.CMV viral load >200 c/mL was considered as CMV reactivation, and thisvalue was used for analyzing its influence on relapse risk in this study.
Acute graft-versus-host disease (aGVHD) was diagnosed clinically basedon signs and symptoms and graded according to accepted criteria [13].Chronic GVHD (cGVHD) was graded in accordance with National Institutesof Health consensus criteria for diagnosis and grading [14].
Etiology of AML was classified into de novo AML without antecedentdiagnosis of bone marrow disorders such as myelodysplastic syndrome ormyeloproliferative disorder, secondary AML occurring from underlying bonemarrow disorders such as myelodysplastic syndrome or myeloproliferativedisorder, and therapy-related AML occurring as a result of prior exposureto chemotherapy and/or radiation therapy per World Health Organizationclassification [15,16]. AML was classified into good, intermediate, andpoor prognostic groups based on cytogenetic and molecular abnormalities[17-19]. Disease status at the time of transplant was classified as firstcomplete remission, second complete remission, active disease, and “other”based on the bone marrow biopsy done within 30 days before trans-plantation [20,21] “Other” included patients who achieved remission for thethird time or beyond. Patients with persistent disease at the time of trans-plantation were classified as active disease.
CMV Viremia Monitoring and TreatmentqPCR testing for CMV reactivation after allo-HCT was done at least twice
weekly for all inpatients and once weekly in the outpatient setting. CMVviremia when detected and quantifiable was treated with intravenousganciclovir or oral valganciclovir for 14 days; if follow-up CMV qPCR showedimprovement in the viral load, then intravenous ganciclovir or oral val-ganciclovir was continued on a maintenance dose until 2 consecutive qPCRresults were negative [22,23]. At that point, antiviral treatment was changedback to either acyclovir or valaciclovir.
Table 3Variables Influencing Risk of Relapse on Multivariate Analysis
Parameter ParameterEstimate
StandardError
P HazardRatio
95% HazardRatioConfidenceLimits
CMV (yes versusno)
e.4427 .1965 .0242 .6423 .4370 .9440
cGVHD(yes versus no)
e1.1237 .2243 <.0001 .3251 .2094 .5046
XRT regimen(yes versus no)
.4407 .1948 .0237 1.5538 1.0606 2.2763
CMV indicates post-transplantation CMV reactivation (yes vs. no); XRTregimen, use of radiation in conditioning regimen.
Post-Transplantation Disease MonitoringPatients underwent bone marrow biopsies after allo-HCT at 30 days,
100 days, and then every 6 months or earlier if there were any abnormalfindings noted on their peripheral blood suspicious for relapse. Relapse wasdefined per accepted criteria [16]. Morphologic relapse was the primaryoutcome for patients transplanted in complete remission and progression ofdisease for patients transplanted with active disease. Engraftment of thedonor cells was determined by Southern blot test for short tandem repeatsfrom peripheral blood mononuclear cells and/or bone marrow samples [24].All patients were followed for CMV reactivation data until patients relapsedor, for those without relapse, until death or the last clinic visit. Completedonor engraftment was defined by the presence of<5% of the recipient cellsobtained from bone marrow sample short tandem repeats. Recipient cellpercentage>5%was defined asmixed chimerism. Extramedullary disease orrelapse was defined by presence of blasts in tissue biopsy or by the presenceof morphologically or phenotypically positive blasts in the cerebrospinalfluid.
Study Endpoints and Statistical AnalysesThe primary study endpoint was cumulative incidence of relapse,
whereas secondary endpoints included overall survival (OS), relapse-freesurvival (RFS), and nonrelapse mortality (NRM). Cumulative incidence ofrelapse was compared between groups with and without CMV reactivationfor statistical significance. Cumulative incidence of relapse was estimated bytreating death in remission as a competing risk event, and cumulativeincidence of NRMwas estimated by treating death in relapse as a competingrisk event. OS was defined as the time from allo-HCT to death from any causeor last follow-up. RFS was defined as the time from allo-HCT to relapse ordeath without relapse, whichever occurred first.
Patient-, disease-, and treatment-related variables for the 2 studygroups were compared using the chi-square statistic or Fisher exact test for
Parameter ParameterEstimate
StandardError
P HazardRatio
95% HazardRatioConfidenceLimits
CMV (yesversus no)
e.6452 .2353 .0061 .5246 .3308 .8319
cGVHD (yesversus no)
e1.0197 .2458 <.0001 .3607 .2228 .5840
XRT regimen(yes versus no)
.5807 .2231 .0092 1.7873 1.1543 2.7674
ATG regimen(yes versus no)
1.9601 .2753 <.0001 7.1002 4.1394 12.1787
CMV indicates post-transplantation CMV reactivation (yes vs. no); XRTregimen, use of radiation in conditioning regimen; ATG regimen, use of ATGin conditioning regimen.
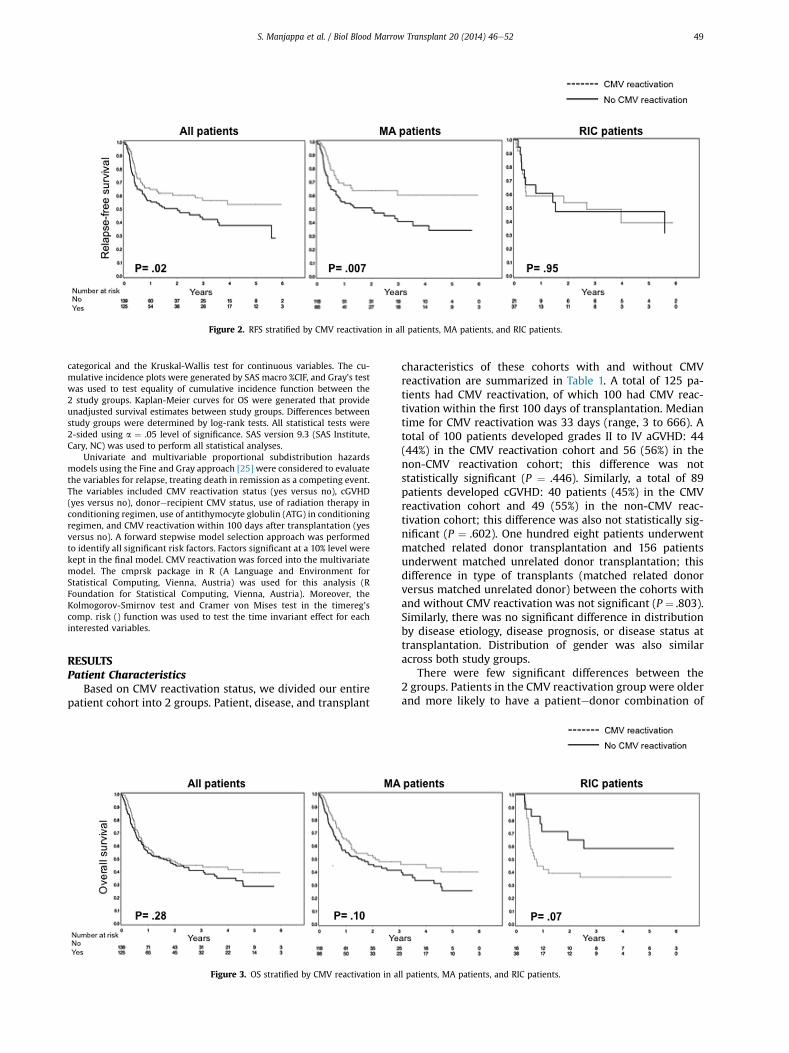
Figure 2. RFS stratified by CMV reactivation in all patients, MA patients, and RIC patients.
S. Manjappa et al. / Biol Blood Marrow Transplant 20 (2014) 46e52 49
categorical and the Kruskal-Wallis test for continuous variables. The cu-mulative incidence plots were generated by SAS macro %CIF, and Gray’s testwas used to test equality of cumulative incidence function between the2 study groups. Kaplan-Meier curves for OS were generated that provideunadjusted survival estimates between study groups. Differences betweenstudy groups were determined by log-rank tests. All statistical tests were2-sided using a ¼ .05 level of significance. SAS version 9.3 (SAS Institute,Cary, NC) was used to perform all statistical analyses.
Univariate and multivariable proportional subdistribution hazardsmodels using the Fine and Gray approach [25] were considered to evaluatethe variables for relapse, treating death in remission as a competing event.The variables included CMV reactivation status (yes versus no), cGVHD(yes versus no), donorerecipient CMV status, use of radiation therapy inconditioning regimen, use of antithymocyte globulin (ATG) in conditioningregimen, and CMV reactivation within 100 days after transplantation (yesversus no). A forward stepwise model selection approach was performedto identify all significant risk factors. Factors significant at a 10% level werekept in the final model. CMV reactivation was forced into the multivariatemodel. The cmprsk package in R (A Language and Environment forStatistical Computing, Vienna, Austria) was used for this analysis (RFoundation for Statistical Computing, Vienna, Austria). Moreover, theKolmogorov-Smirnov test and Cramer von Mises test in the timereg’scomp. risk () function was used to test the time invariant effect for eachinterested variables.
RESULTSPatient Characteristics
Based on CMV reactivation status, we divided our entirepatient cohort into 2 groups. Patient, disease, and transplant
Figure 3. OS stratified by CMV reactivation in a
characteristics of these cohorts with and without CMVreactivation are summarized in Table 1. A total of 125 pa-tients had CMV reactivation, of which 100 had CMV reac-tivation within the first 100 days of transplantation. Mediantime for CMV reactivation was 33 days (range, 3 to 666). Atotal of 100 patients developed grades II to IV aGVHD: 44(44%) in the CMV reactivation cohort and 56 (56%) in thenon-CMV reactivation cohort; this difference was notstatistically significant (P ¼ .446). Similarly, a total of 89patients developed cGVHD: 40 patients (45%) in the CMVreactivation cohort and 49 (55%) in the non-CMV reac-tivation cohort; this difference was also not statistically sig-nificant (P ¼ .602). One hundred eight patients underwentmatched related donor transplantation and 156 patientsunderwent matched unrelated donor transplantation; thisdifference in type of transplants (matched related donorversus matched unrelated donor) between the cohorts withand without CMV reactivation was not significant (P ¼ .803).Similarly, there was no significant difference in distributionby disease etiology, disease prognosis, or disease status attransplantation. Distribution of gender was also similaracross both study groups.
There were few significant differences between the2 groups. Patients in the CMV reactivation group were olderand more likely to have a patientedonor combination of
ll patients, MA patients, and RIC patients.
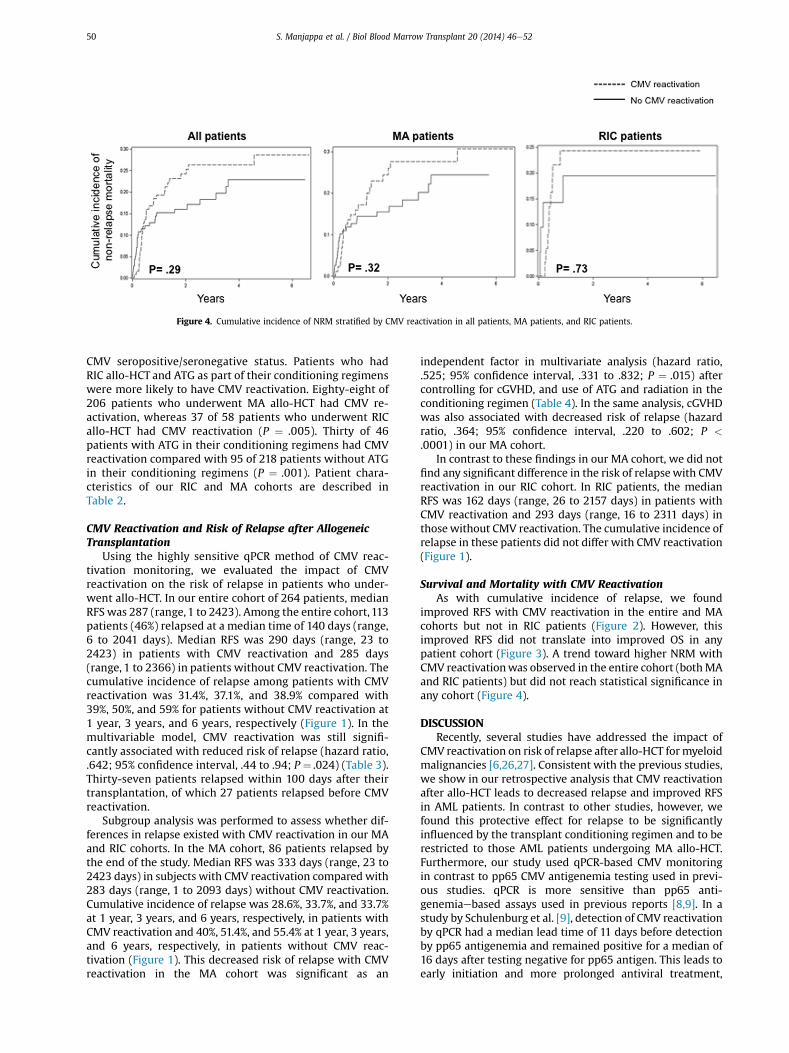
Figure 4. Cumulative incidence of NRM stratified by CMV reactivation in all patients, MA patients, and RIC patients.
S. Manjappa et al. / Biol Blood Marrow Transplant 20 (2014) 46e5250
CMV seropositive/seronegative status. Patients who hadRIC allo-HCT and ATG as part of their conditioning regimenswere more likely to have CMV reactivation. Eighty-eight of206 patients who underwent MA allo-HCT had CMV re-activation, whereas 37 of 58 patients who underwent RICallo-HCT had CMV reactivation (P ¼ .005). Thirty of 46patients with ATG in their conditioning regimens had CMVreactivation compared with 95 of 218 patients without ATGin their conditioning regimens (P ¼ .001). Patient chara-cteristics of our RIC and MA cohorts are described inTable 2.
CMV Reactivation and Risk of Relapse after AllogeneicTransplantation
Using the highly sensitive qPCR method of CMV reac-tivation monitoring, we evaluated the impact of CMVreactivation on the risk of relapse in patients who under-went allo-HCT. In our entire cohort of 264 patients, medianRFS was 287 (range, 1 to 2423). Among the entire cohort,113patients (46%) relapsed at a median time of 140 days (range,6 to 2041 days). Median RFS was 290 days (range, 23 to2423) in patients with CMV reactivation and 285 days(range, 1 to 2366) in patients without CMV reactivation. Thecumulative incidence of relapse among patients with CMVreactivation was 31.4%, 37.1%, and 38.9% compared with39%, 50%, and 59% for patients without CMV reactivation at1 year, 3 years, and 6 years, respectively (Figure 1). In themultivariable model, CMV reactivation was still signifi-cantly associated with reduced risk of relapse (hazard ratio,.642; 95% confidence interval, .44 to .94; P ¼ .024) (Table 3).Thirty-seven patients relapsed within 100 days after theirtransplantation, of which 27 patients relapsed before CMVreactivation.
Subgroup analysis was performed to assess whether dif-ferences in relapse existed with CMV reactivation in our MAand RIC cohorts. In the MA cohort, 86 patients relapsed bythe end of the study. Median RFS was 333 days (range, 23 to2423 days) in subjects with CMV reactivation compared with283 days (range, 1 to 2093 days) without CMV reactivation.Cumulative incidence of relapse was 28.6%, 33.7%, and 33.7%at 1 year, 3 years, and 6 years, respectively, in patients withCMV reactivation and 40%, 51.4%, and 55.4% at 1 year, 3 years,and 6 years, respectively, in patients without CMV reac-tivation (Figure 1). This decreased risk of relapse with CMVreactivation in the MA cohort was significant as an
independent factor in multivariate analysis (hazard ratio,.525; 95% confidence interval, .331 to .832; P ¼ .015) aftercontrolling for cGVHD, and use of ATG and radiation in theconditioning regimen (Table 4). In the same analysis, cGVHDwas also associated with decreased risk of relapse (hazardratio, .364; 95% confidence interval, .220 to .602; P <
.0001) in our MA cohort.In contrast to these findings in our MA cohort, we did not
find any significant difference in the risk of relapsewith CMVreactivation in our RIC cohort. In RIC patients, the medianRFS was 162 days (range, 26 to 2157 days) in patients withCMV reactivation and 293 days (range, 16 to 2311 days) inthosewithout CMV reactivation. The cumulative incidence ofrelapse in these patients did not differ with CMV reactivation(Figure 1).
Survival and Mortality with CMV ReactivationAs with cumulative incidence of relapse, we found
improved RFS with CMV reactivation in the entire and MAcohorts but not in RIC patients (Figure 2). However, thisimproved RFS did not translate into improved OS in anypatient cohort (Figure 3). A trend toward higher NRM withCMV reactivationwas observed in the entire cohort (bothMAand RIC patients) but did not reach statistical significance inany cohort (Figure 4).
DISCUSSIONRecently, several studies have addressed the impact of
CMV reactivation on risk of relapse after allo-HCT formyeloidmalignancies [6,26,27]. Consistent with the previous studies,we show in our retrospective analysis that CMV reactivationafter allo-HCT leads to decreased relapse and improved RFSin AML patients. In contrast to other studies, however, wefound this protective effect for relapse to be significantlyinfluenced by the transplant conditioning regimen and to berestricted to those AML patients undergoing MA allo-HCT.Furthermore, our study used qPCR-based CMV monitoringin contrast to pp65 CMV antigenemia testing used in previ-ous studies. qPCR is more sensitive than pp65 anti-genemiaebased assays used in previous reports [8,9]. In astudy by Schulenburg et al. [9], detection of CMV reactivationby qPCR had a median lead time of 11 days before detectionby pp65 antigenemia and remained positive for a median of16 days after testing negative for pp65 antigen. This leads toearly initiation and more prolonged antiviral treatment,

S. Manjappa et al. / Biol Blood Marrow Transplant 20 (2014) 46e52 51
thereby potentially altering the impact of CMV reactivationon relapse and survival benefit. However, here we showdecreased relapse with CMV reactivation despite this po-tential lead time for CMV treatment when using the highlysensitive qPCR method of CMV monitoring in our allo-HCTpatients.
CMV-positive serostatus of the donor and recipients wasassociated with reduced relapse rates in a pediatric popula-tion who had undergone allo-HCT for acute leukemia [27]. Ina recent report by Elmagacli et al. [6], CMV reactivation inAML patients after allo-HCT was associated with decreasedrelapse and improved OS; however, this study only includedpatients who received MA conditioning. Similarly, Greenet al. [7] observed a decreased risk of relapse with CMVreactivation in a cohort of AML patients, including both MAand RIC patients, that was more pronounced within the first100 days after transplantation and not statistically significantby 1 year. Both these studies used pp65 antigenemiaebasedmonitoring for CMV reactivation.
Using both pp65 antigenemia and qPCR-based assays, Itoet al. [28] found decreased relapse with CMV reactivationafter allo-HCT in CMV patients. Further, in our patients thisbeneficial effect of CMV reactivation on relapse was sus-tained. Despite decreased risk of relapse and improved RFS,we were unable to correlate improved OS with CMV reac-tivation, which may be related to the increased NRM withCMV reactivation because we saw a clear trend towardincreased NRM with CMV reactivation (although it did notreach statistical significance), and this increased NRM withCMV reactivation was also reported by Green et al. [7]. Basedon these results, we hypothesize that decreased relapse risk(and therefore improved RFS) and increased NRM competeto influence OS in patients with CMV reactivation after allo-HCT. This would explain the clear trend of decreased OS seenin our RIC cohort where the lack of this protective effect onrelapse favors the balance toward poor OS (Figure 3).
The mechanism(s) behind decreased relapse with CMVreactivation allo-HCT is currently not known. There hasbeen significant interest in better understanding the impactof natural killer (NK) cell alloreactivity on relapse, especiallyin patients undergoing allo-HCT for myeloid malignancies[29-31]. Foley et al. [32] found selective expansion of theNKG2CþCD57þ NK cells with CMV reactivation, and thesecells have enhanced antileukemia responses in vitro. Theenhanced antileukemia responses by NKG2CþCD57þ NKcells could potentially be responsible for enhanced NKcellemediated “graft-versus-leukemia” (GVL) effect in vivo,translating into less relapse in patients who reactivate CMVafter allo-HCT. Furthermore, CMV reactivation increasesleucocyte fixation antigen-3 expression on blasts carryingCMV, leading to enhanced NK cellemediated lysis of theblasts [26,33]. The NK cellemediated GVL effect in generalseems to be restricted to patients with myeloid malig-nancies and could be the reason why this CMV reac-tivationerelated decreased relapse has been observed inpatients with myeloid malignancies [6,7,28-30]. Donor-derived T cells could also be contributing to this “relapseprotective” effect from CMV reactivation. Leukemic blastscould harbor CMV and, upon reactivation, activated donor-derived T cells specific to CMV could therefore be directlycytotoxic to these blasts expressing CMV antigens [26].Thus, the GVL effect is pronounced in the scenario wherethe recipient is seropositive than in any other combination,and this has been demonstrated in our study as well as inothers [7]. The role of T cells in this enhanced GVL effect is
underscored by the failure to demonstrate decreasedrelapse with CMV reactivation in a study where patientsunderwent T celledepleted grafts with an alemtuzumab-containing conditioning regimen [34].
In our RIC cohort, 44 of 58 patients received ATG as part oftheir conditioning regimens. In vivo T cell depletion by ATGin this cohort may result in mitigating the enhanced GVLeffect induced by CMV reactivation, therefore again under-scoring the importance of graft-derived T cells in mediatingthis effect. Further, host-derived memory T cells can persistfor up to 6 months in RIC patients and contribute towardimmunity against CMV [35,36]. Persistence of these host Tcells could contribute to clearing of CMV upon its reac-tivation, thereby possibly preventing optimal donor T celland NK cell activation. Persistence of the host lymphocytesearly after allo-HCT in RIC patients could also compete forcytokines with donor-derived T and NK cells and thereforeimpair the enhanced GVL effect seen in the context of CMVreactivation. The smaller RIC cohort could also be a factor fornot observing relapse benefit. Further studies in a largercohort of patients with RIC regimens with and without ATGwould be prudent to better understand the role of the con-ditioning regimen in this relapse benefit from CMVreactivation.
Reactivation of CMV after allo-HCT is traditionallyconsidered an adverse event needing aggressive therapy, andmost transplant centers monitor for CMV reactivation veryclosely and institute aggressive pre-emptive therapy uponevidence of CMV reactivation. Here we show that CMVreactivation after allo-HCT, especially in MA conditioningrecipients, is associated with decreased risk of relapse andimproved RFS in AML patients. The mechanisms responsiblefor this enhanced GVL effect with CMV reactivation need tobe further evaluated because a better understanding couldpotentially lead to developing novel CMV antigenebasedvaccination strategies aimed at reducing relapse risk afterallo-HCT in the future.
ACKNOWLEDGMENTSFinancial disclosure: The authors have nothing to disclose.Conflict of interest statement: There are no conflicts of in-
terest to report.Authorship statement: S.M., P.K.B., and R.R. designed the
study and interpreted data. S.M., P.K.B, S.J.M., and K.E.S.-G.prepared the dataset and drafted the manuscript. J.L. didthe statistical analysis. S.M., P.K.B., K.E.S.-G., J.F.D., J.L., T.A.F.,G.U., P.W., A.F.C., M.A.S., R.V., C.N.A., I.P., M.J., and R.R. inter-preted data and critically reviewed the manuscript. All au-thors approved the final manuscript.
REFERENCES1. Rafailidis PI, Mourtzoukou EG, Varbobitis IC, Falagas ME. Severe cyto-
megalovirus infection in apparently immunocompetent patients: Asystematic review. Virol J. 2008;5:47.
2. Boeckh M, Ljungman P. How we treat cytomegalovirus in hematopoi-etic cell transplant recipients. Blood. 2009;113:5711-5719.
3. Ljungman P, Hakki M, Boeckh M. Cytomegalovirus in hematopoieticstem cell transplant recipients. Hematol Oncol Clin North Am. 2011;25:151-169.
4. Ljungman P, Perez-Bercoff L, Jonsson J, et al. Risk factors for thedevelopment of cytomegalovirus disease after allogeneic stem celltransplantation. Haematologica. 2006;91:78-83.
5. Broers AE, van Der Holt R, van Esser JW, et al. Increased transplant-related morbidity and mortality in CMV-seropositive patients despitehighly effective prevention of CMV disease after allogeneic T-cell-depleted stem cell transplantation. Blood. 2000;95:2240-2245.
6. Elmaagacli AH, Steckel NK, Koldehoff M, et al. Early human cytomeg-alovirus replication after transplantation is associated with a decreased
S. Manjappa et al. / Biol Blood Marrow Transplant 20 (2014) 46e5252
relapse risk: Evidence for a putative virus-versus-leukemia effect inacute myeloid leukemia patients. Blood. 2011;118:1402-1412.
7. Green ML, Leisenring WM, Xie H, et al. CMV reactivation after alloge-neic HCT and relapse risk: Evidence for early protection in acutemyeloid leukemia. Blood. 2013;122:1316-1324.
8. Nitsche A, Oswald O, Steuer N, et al. Quantitative real-time PCRcompared with pp65 antigen detection for cytomegalovirus (CMV) in1122 blood specimens from 77 patients after allogeneic stem celltransplantation: Which test better predicts CMV disease development?Clin Chem. 2003;49:1683-1685.
9. Schulenburg A, Rabitsch W, Loidolt H, et al. CMV monitoring afterperipheral blood stem cell and bone marrow transplantation by pp65antigen and quantitative PCR. Bone Marrow Transplant. 2001;28:715-768.
10. Speiser DE, Tiercy JM, Rufer N, et al. High resolution HLA matchingassociated with decreased mortality after unrelated bone marrowtransplantation. Blood. 1996;87:4455-4462.
11. Ottinger HD, Ferencik S, Beelen DW, et al. Hematopoietic stem celltransplantation: contrasting the outcome of transplantations fromHLA-identical siblings, partially HLA-mismatched related donors, andHLA-matched unrelated donors. Blood. 2003;102:1131-1137.
12. Bacigalupo A, Ballen K, Rizzo D, et al. Defining the intensity of condi-tioning regimens: Working definitions. Biol Blood Marrow Transplant.2009;15:1628-1633.
13. Glucksberg H, Storb R, Fefer A, et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation. 1974;18:295-304.
14. Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes ofHealth consensus development project on criteria for clinical trialsin chronic graft-versus-host disease. I. Diagnosis and stagingworking group report. Biol Blood Marrow Transplant. 2005;11:945-956.
15. Vardiman JW, Harris NL, Brunning RD. The World Health Organization(WHO) classification of the myeloid neoplasms. Blood. 2002;100:2292-2302.
16. Cheson BD, Bennett JM, Kopecky KJ, et al. Revised recommendations ofthe International Working Group for diagnosis, standardization ofresponse criteria, treatment outcomes, and reporting standards fortherapeutic trials in acute myeloid leukemia. J Clin Oncol. 2003;21:4642-4649.
17. Mrózek K, Heerema N, Bloomfield CD. Cytogenetics in acute leukemia.Blood Rev. 2004;18:115-136.
18. Slovak ML, Kopecky KJ, Cassileth PA, et al. Karyotypic analysis predictsoutcome of preremission and postremission therapy in adult acutemyeloid leukemia: A Southwest Oncology Group/Eastern CooperativeOncology Group study. Blood. 2000;96:4075-4083.
19. Grimwade D, Walker H, Oliver F, et al. The importance of diagnosticcytogenetics on outcome in AML: Analysis of 1,612 patients enteredinto the MRC AML 10 trial. Blood. 1998;92:2322-2333.
20. Cornelissen JJ, van Putten WLJ, Verdonck LF, et al. Results of a HOVON/SAKK donor versus no-donor analysis of myeloablative HLA-identicalsibling stem cell transplantation in first remission acute myeloid leu-kemia in young and middle-aged adults: Benefits for whom? Blood.2007;109:3658-3666.
21. Kurosawa S, Yamaguchi T, Miyawaki S, et al. Prognostic factors andoutcomes of adult patients with acute myeloid leukemia after firstrelapse. Haematologica. 2010;95:1857-1864.
22. Hebart H, Brugger W, Grigoleit U, et al. Risk for cytomegalovirus dis-ease in patients receiving polymerase chain reaction-based preemptiveantiviral therapy after allogeneic stem cell transplantation depends ontransplantation modality. Blood. 2001;97:2183-2185.
23. Van der Heiden PLJ, Kalpoe JS, Barge RM, et al. Oral valganciclovir aspre-emptive therapy has similar efficacy on cytomegalovirus DNA loadreduction as intravenous ganciclovir in allogeneic stem cell trans-plantation recipients. Bone Marrow Transplant. 2006;37:693-698.
24. Martinelli G, Trabetti E, Farabegoli P, et al. Early detection of bonemarrow engraftment by amplification of hypervariable DNA regions.Haematologica. 1997;82:156-160.
25. Gray JPF, Fine RJ. A proportional hazards model for the subdistributionof a competing risk. J Am Stat Assoc. 1999;94:496-509.
26. Barrett AJ. CMV: When bad viruses turn good. Blood. 2011;118:1193-1194.
27. Behrendt CE, Rosenthal J, Bolotin E, et al. Donor and recipient CMVserostatus and outcome of pediatric allogeneic HSCT for acute leuke-mia in the era of CMV-preemptive therapy. Biol Blood Marrow Trans-plant. 2009;15:54-60.
28. Ito S, Pophali P, Co W, et al. CMV reactivation is associated with a lowerincidence of relapse after allo-SCT for CML. Bone Marrow Transplant.2013;48:1-4.
29. Ruggeri L, Capanni M, Urbani E, et al. Effectiveness of donor naturalkiller cell alloreactivity in mismatched hematopoietic transplants. Sci-ence. 2002;295:2097-2100.
30. Venstrom JM, Pittari G, Gooley T, et al. HLA-C-dependent prevention ofleukemia relapse by donor activating KIR2DS1. N Engl J Med. 2012;367:805-816.
31. Cooley S, Trachtenberg E, Bergemann TL, et al. Donors with group B KIRhaplotypes improve relapse-free survival after unrelated hematopoi-etic cell transplantation for acute myelogenous leukemia. Blood. 2009;113:726-732.
32. Foley B, Cooley S, Verneris MR, et al. Cytomegalovirus reactivation afterallogeneic transplantation promotes a lasting increase in educatedNKG2Cþ natural killer cells with potent function. Blood. 2012;119:2665-2674.
33. Fletcher JM, Prentice HG, Grundy JE. Natural killer cell lysis of cyto-megalovirus (CMV)-infected cells correlates with virally inducedchanges in cell surface lymphocyte function-associated antigen-3(LFA-3) expression and not with the CMV-induced down-regulation ofcell surface class I HLA. J Immunol. 1998;161:2365-2374.
34. Thomson KJ, Mackinnon S, Peggs KS. CMV-specific cellular therapy foracute myeloid leukemia? Blood. 2012;119:1088-1090. author reply1090-1091.
35. Junghanss C. Incidence and outcome of cytomegalovirus infectionsfollowing nonmyeloablative compared with myeloablative allogeneicstem cell transplantation, a matched control study. Blood. 2002;99:1978-1985.
36. Maris M, Boeckh M, Storer B, et al. Immunologic recovery after he-matopoietic cell transplantation with nonmyeloablative conditioning.Exp Hematol. 2003;31:941-952.