Embed Size (px)
Citation preview

Protein S Deficiency in Men With Long-Term Human Immunodeficiency Virus Infection
By Claire Philipp Stahl, Carol S. Wideman, Thomas J. Spira, Elizabeth C. Haff, Gwendolyn J. Hixon, and Bruce L. Evatt
Decreases in protein S levels have recently been reported in some human immunodeficiency virus (HIV)-infected pa- tients. To examine predisposing factors, 25 men randomly selected from a long-term study of HIV-infected patients were studied. The minimum mean duration of HIV sero- positivity in this group was 106.6 months (range 1 5 to 143 months). No patients were anticoagulated at the time of the study. Three of the 25 randomly selected patients gave a history of thrombosis, in each instance occurring afterthe onset of HIV positivity. Two of the 3 patients with throm- bosis had more than one episode. Coagulation studies showed that 3 of 3 (1 00%) of the patients with thrombosis and 16 of 22 (72.7%) of those without previous thrombosis had decreased free protein S. Mean-free and total protein S levels were statistically lower for HIV-infected patients with and without previous thrombosis compared with healthy male controls. C4b-binding protein was not in-
ROTEIN S IS A vitamin K-dependent plasma protein P that serves as a cofactor for activated protein C.’ Con- genital deficiencies in protein S predispose to thromboembolic complication^.^-^ Hereditary protein S deficiency has been estimated to have a prevalence in the general population of 1 in 29,0005 and to be found in 5% to 8% of individuals with unexplained thrombosis detected at a young age in the ab- sence of known predisposing factors. Normally, approxi- mately 30% to 40% of protein S is free in the plasma and approximately 60% to 70% is bound to C4b-binding protein (C4bBP).6 The latter is functionally inactive as a cofactor for activated protein C . Hereditary reductions in free protein S, caused by either an abnormal distribution between free pro- tein S and inactive protein S bound to C4bBP or caused by reductions in total protein S, increase the risk for thrombosis.’
Acquired decreases in protein S levels occur in pregnancy: with oral contraceptive use: and during warfarin therapy,” and are associated with disseminated intravascular coagula- tion,” liver disease,” nephrotic syndrome,12,13 and systemic lupus erythemato~us.’~ Decreases in protein S levels also have been reported in some human immunodeficiency virus (HIV)-infected patients.” However, whether acquired re- ductions in protein S levels predispose individuals to throm- bosis is currently not known. In congenital protein S defi- ciency the probability of developing thrombosis by age 27 is 50% and increases to 70% by age 35.16 Because of these find- ings, we evaluated retrospectively the clinical implications of the protein S status of a group of men with long-term HIV infection. The results suggest that these individuals may be predisposed to thrombotic complications.
MATERIALS AND METHODS
Twenty-seven men with HIV infection (mean age 38.6 f 5.6 years) and 28 healthy male controls (mean age 40 * 7.9 years) were studied. All subjects gave informed consent. Venous blood was collected in 1/10 vol ofO. 109 mol/L sodium citrate. Platelet- poor plasma was obtained by centrifugation and frozen at -70°C until tested. Twenty-five men with HIV disease were randomly se- lected from a previously established long-term prospective study of HIV-associated lymphadenopathy. An additional two men with HIV
Patient population.
creased in study patients with decreased protein S levels. Decreases in protein S levels did not correlate with CD4+ cell levels, CDC class, p24 antigen positivity, zidovudine (AZT) use, or Pneumocystis carinii prophylaxis. The duration of disease statistically correlated with decreases in protein S levels (r = .37, P < .05). A linear correlation existed between increasing lgG anticardiolipin antibody levels and decreasing free protein S antigen (r = .67, P < .005). This study shows that protein S deficiency is common in long- term HIV-infected patients and is caused by a decrease in the free protein, rather than by changes in the bound com- plex. The data suggest that protein S deficiency is not cor- related with HIV disease severity but may predispose pa- tients to thromboembolic complications. This is a US government work. There are no restrictions on its use.
disease were referred for evaluation of previous thrombosis. Their results are presented separately and are not included in the analysis of data. None of the individuals were on anticoagulants or had active thrombosis at the time of study. None of the patients had laboratory or clinical evidence of liver or kidney disease. All patients were am- bulatory at the time of study and there was no evidence of acute intercurrent infection. A minimum mean duration of HIV seropos- itivity for the 25 randomly selected HIV-infected men was 106.6 months (range 15 to 143). Their mean CD4+ cell level was 226/mm3 (range 29 to 653) (Table 1). Of the 25 men, 13 males with HIV disease were taking zidovudine (AZT) at the time of the study, 4, dideoxycytidine (DDC), and 1, dideoxyinosine (DDI). Twelve patients were on medications for Pneumocystis prophylaxis, including pent- amidine (8), trimethoprim-sulfamethoxazole (4), and dapsone ( I ) . The control population was not on medications.
Protein C antigen and total protein S antigen were measured with the Laurel1 electroimmunoassay as previously
Free protein S antigen was determined by polyethylene- glycol pre~ipitation,~ followed by electroimmunoassay to measure the free protein S. The protein S concentration in plasma was assessed using purified human protein S (American Diagnostica Inc, Green- wich, CT) as a reference standard, and the molarity was calculated using a protein S molecular weight of 75,000.’8 Levels of protein S in the standard were measured by determining its amino acid con- centration following 24-hour 6N HC1 hydrolysis in vacuo. The phenylthiocarbamoyl amino acids were analyzed by high performance liquid chromatography (HPLC) by the Waters Pico-Tag system (Mil-
Coagulation studies.
From the Division of HIV/AIDS, National Center for Infectious Diseases, Centers for Disease Control and Prevention, Public Health Service, US Department ofHealth and Human Services, Atlanta, GA.
Submitted April 16, 1992; accepted November 23, 1992. American Bioproducts Company (Parsippany, NJ/ provided the
C4bBP kits under Grant No. 91ER005. Address reprint requests to Claire Philipp Stahl, MD, Centers for
Disease Control, 1600 Clifton Road, 1-1378 (002). Atlanta, GA 30333. The publication costs of this article were defrayed in part by page
charge payment. This article must therefore be hereby marked “advertisement” in accordance with 18 U.S.C. section 1734 solely to indicate this fact.
This is a USgovernment work. There are no restrictions on its use. 0006-49 71/93/81 0 7-0028$0.00/0
Blood, Vol 81, No 7 (April 1). 1993: pp 1801-1807 1801
For personal use only.on December 30, 2018. by guest www.bloodjournal.orgFrom

1802 STAHL ET AL
Table 1. Immunologic, Clinical, and Coagulation Parameters for Study Patients With HIV
CD4, CD4:CD8 Months Free S Funct. S Total S vWF:AG 656- Ratio 0.7%- Since Thrombotic 5.5-10.2 63%- 18.1-32.0 44%- Fibrinogen
Patient 1801/pL 3.4% CDC Class Onset Events m/mL 144% rg/mL 140% 2.0-4.0 g/L
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 Mean Range
653 29
292 189 41
202 430 377
29 83
600 160 250 228 387 225 383 196 160 29 46
172 242 218
29 226
29-653
0.37 0.05 0.29 0.23 0.07 0.61 0.59 0.38 0.07 0.09 0.32 0.13 0.20 0.32 0.21 0.22 0.23 0.16 0.52 0.13 0.04 0.1 1 0.16 0.40 0.05 0.24
0.04-0.6 1
2 4C 1 4C2 3 3 3 3 3 4D 4C2 2 4C 1 3 3 3 4D 3 3 3 3 3 3 3 3 3
59 121 106 120 107 102 75
122 96
109 19
114 123 102 112 108 107 103 97
107 139 143 123 117 134 106.6
19-143
NONE MI, DVT NONE NONE NONE NONE NONE DVT, PE NONE NONE NONE NONE NONE NONE NONE NONE NONE NONE NONE DVT NONE NONE NONE NONE NONE
5.5 1.3 5.5 5.5 7.7 3.4 5.3 3.4 3.4 3.4 6.6 1.7 4.4 4.0 2.8 6.9 3.3 4.8 2.1 1.8 2.4 3.3 3.6 4.9 2.1 4.0
1.3-7.7
102 44
114 93 92 71 78 51 26 68
128 34 93 65 44 88 61 89 30 33 66 83
118 124 43 74
26-1 28
19.5 20.0 17.6 19.7 32.5 20.8 21.1 16.0 17.9 19.5 30.7 19.2 21.3 16.8 17.9 26.1 17.6 26.1 14.9 17.1 24.8 26.7 29.3 27.7 19.2 21.6
14.9-32.5
175 2.50 20 1 5.30
72 1.90 105 2.20 555 3.30
64 2.30 20 1 3.00 161 2.20 218 2.25 131 3.15 182 2.95 165 4.35 192 3.00 218 2.82
86 2.52 121 4.10 152 3.11 90 2.02 84 2.35
486 2.95 340 2.70 122 2.67 107 2.67 97 2.14
256 2.56 183 2.84
64-555 1.90-5.30
Patients were randomly selected from a previously established cohort of HIV-infected men (see Materials and Methods). Months since onset of
Abbreviations: MI, myocardial infarct; DVT, deep vein thrombosis; PE, pulmonary embolism. HIV positivity and/or onset of first symptoms are reported.
lipore/Water, Milford, MA). The concentration of total protein S in normal-pooled plasma from six men and six women corrected for anticoagulant dilution was determined to be 22.28 f 0.84 pg/mL, and of free protein S, 6.04 f 0.59 &mL. These values are consistent with previously reported concentrations'O.'s-'o when adjusted to the levels for undiluted plasma. Crossed immunoelectrophoresis of pro- tein S was performed using the method of Laurell and McKay as previously described:' with a 1:428 dilution of protein S antiserum (American Diagnostica). Functional protein S was measured with Staclot Protein S kits (Diagnostica Stago, Parsippany, NJ) using the ST4 coagulation instrument (Diagnostica Stago). The test measures the increase in activated partial thromboplastin time (APTT) per- formed on a mixture containing protein Sdeficient plasma, cephalin, test plasma, activated protein C, factor Va, kaolin, and calcium chlo- ride.*' Functional protein C was measured with the Stachrom Protein C kit (Diagnostica Stago). C4bBP antigen was measured with the Laurell electroimmunoassay using C4bBP agarose gel plates (Diag- nostica Stago) and with Liatest C4b-BP (Diagnostica Stago). The von Willebrand factor antigen (vWFAG) was measured by the Laurell electroimmunoassay using rabbit human-factor VIII-related antigen antiserum (Accurate Chemical and Scientific Corp, Westbury, NY). Fibrinogen was measured by the Clauss procedure (Dade, Miami, FL). Antithrombin I11 was determined on the ACA (DuPont, Wil- mington, DE) using bovine thrombin. Plasminogen was also assayed on the ACA. The tissue thromboplastin inhibition test (TTI)23 was modified by testing a 1: 1 mix of patient and normal plasma to correct for possible coagulation factor deficiencies. Factor I1 and X antigens were measured by the Laurell electroimmunoassay using prothrombin
rabbit antiserum (Behring Corp, La Jolla, CA, and Accurate Chemical and Scientific Cow) and factor X rabbit antiserum (Diagnostica Stago).
Discontinuous sodium dodecyl sulfate (SDS) electrophoresis was performed on 7.5%, IO%, or 10% to 15% gradient nondenaturing polyacrylamide gels at 15°C in a Phast System (Pharmacia LKB Biotechnology, Piscataway, NJ). Proteins were im- mediately electrotransferred to nitrocellulose (Hoefer Scientific In- struments, San Francisco, CA) or polyvinylidene difluoride (Millipore, Bedford, MA) in 25 mmol/L Tris, 192 mmol/L glycine, 20% (vol/ vol) methanol, pH 8.3, at 15°C in a PhastTransfer Semi-dry System (Pharmacia LKB Biotechnology) at 25 mA as limiting factor for 3 volt hours.
The membrane was blocked in bovine lacto transfer technique optimizer probed with protein S antisera (American Diagnostica, New York, NY), then incubated with anti-goat IgG horseradish peroxidase conjugate (Chemicon International, Temecula, CA). Molecular weight determinations were performed with pre- stained SDS-polyacrylamide gel electrophoresis (SDS-PAGE) stan- dards (Bio-Rad, Rockville Centre, NY).
IgG and IgM anti- cardiolipin antibodies were measured using a semi-quantitative in- direct enzyme-linked immunosorbent assay (ELISA) test kit (Reaads Medical Products, Inc, Westminster, CO).25 A standard curve was generated using standard sera provided by the Antiphospholipid Standardization Laboratory (University of Louisville, Louisville, KY). The anticardiolipin antibody concentration is expressed in standard units where 1 IgG phospholipid (GPL) and IgM phospholipid (MPL)
Immunoblot procedure.
Anticardiolipin antibodies and P24 antigen.
For personal use only.on December 30, 2018. by guest www.bloodjournal.orgFrom

HIV AND PROTEIN S DEFICIENCY
11 -
10 -
9 -
E8 - a . LI) v
5 7 -
a6 -
E 5 - 2 n
E4 -
LI)
c
v) c
.- c)
.-
al
LL
3 -
2 -
1 -
1803
12 A
H
H
** * H H
*
HIV without Thrombosis
x
* 9
* H
Control Males
m t H
It A -
HIV with Thrombosis
0 ’
35
30
25
z . En 3
Y O cn C al .- 4- e n -15 m 0 F 4-
10
5
0
B
HIV with Thrombosis a
u m t
A i t
* *H r c *
Control Males
-
A
HIV without Thrombosis
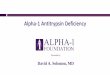
Fig 1. Free protein S antigen levels (A) and total protein S antigen levels (B) in male controls, HIV-infected men with previous thrombosis, and HIV-infected men without thrombosis are shown. Mean values for each group are indicated by a line. Free protein S values for both groups of HIV-infected men were significantly different from those for control men (P < .OOOl). Total protein S levels were significantly lower in both groups of HIV-infected males compared with male controls (HIV with thrombosis, P < .001; HIV without thrombosis, P < .02). Two additional HIV patients referred for thrombosis are shown with (A) but are not included in mean values or statistical analysis.
unit is equivalent to 1 pg/mL of an affinity-purified standard IgG or IgM. Positive values are reported as slightly, moderately, or highly positive. P24 antigens were performed using the Coulter P24 antigen kit (Coulter, Hialeah, FL).
Comparisons between groups were performed using the Wilcoxon rank sum test. Spearman’s rank correlation coef- ficient was used to assess correlations between two parameters. Results were considered statistically significant for P < .05.26
Statistical analysis.
RESULTS
Of the 25 HIV-infected men, 3 had a history of one or more previous episodes of thromboembolism (Table 1). Two out of 3 of the men with thrombosis had more than one episode. In addition to one myocardial infarct, there were four episodes of venous thrombosis, including one episode of pulmonary embolism documented by angiography and three episodes of deep vein thrombosis (DVT) documented by venogram ( 2 ) and Doppler studies (1). All episodes oc- curred after infection with HIV. Two patients had thrombosis within the first year after the diagnosis of HIV-associated lymphadenopathy. Of the 2 additional HIV-positive patients referred with a previous diagnosis of thrombosis, 1 patient
had two episodes of pulmonary emboli and an episode of DVT, and I patient had a pulmonary embolus and a DVT. All of these episodes were documented by lung scans or venograms.
In this study, various coagulation parameters associated with hypercoagulable states were examined. None of the 25 HIV-infected men had decreased protein C, antithrom- bin 111, plasminogen levels, or evidence of a lupus inhibitor as measured by tissue thromboplastin inhibition test. Fi- brinogen was increased in two HIV-infected men. Anti- cardiolipin antibodies, which have been associated with an increased frequency of thrombosis in patients with sys- temic lupus erythematosus*’ but not with H I V - d i s e a ~ e , ~ ~ - ~ ~ were also measured in this study. IgM anticardiolipin antibodies were strongly positive in 1 of 18 HIV-infected men, whereas IgG anticardiolipin antibodies were strongly positive in 3 of 24 and moderately positive in 14 of 24. vWF:AG was increased in 3 of 3 study patients with pre- vious thrombosis and 12 of 29 patients with no previous history. Factor I1 and X antigen levels were normal in all study patients.
For personal use only.on December 30, 2018. by guest www.bloodjournal.orgFrom

1804
130
120
STAHL ET AL
-
12 L
10
l1 1 11 - 10 -
- 9 :
a*: E
.E 6 - w .
Q .
I e 5 -
0 ' 1 1 " " " " ' 1
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140
Functional Protein S ("A normal) 0 10 20 30 40 50 60 70 80 90 100 110 120 130 140
Functional Protein S ("A normal)
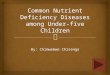
Fig 2. Correlation between functional protein S determinations and free protein S antigen levels in 25 study patients. A linear regression line is drawn. A significant correlation is seen between functional and free protein S determinations (r = .78, P < .005).
Protein S deficiency was common in the randomly selected group of HIV-infected men. Free protein S antigen was de- creased in 3 of 3 (100%) randomly selected men with previous thrombosis and in 16 of 22 (72.7%) of those men without a history of thromboembolism. The HIV-infected men with a prior episode of thrombosis had a mean (? 1 SD) free protein S level of 2.2 f 1.1 pg/mL (range 1.3 to 3.4 pg/mL, n = 3) compared with a mean free protein S level of 4.2 ? 1.6 pg/ mL (range 1.7 to 7.7 pg/mL, n = 22) in HIV-infected men without a previous history of thrombosis. Male controls had a mean free protein S level of 7.9 f 1.2 pg/mL (range 5.0 to 10.7 pg/mL, n = 27). Mean values for both groups of HIV- infected men were significantly different from those for un- infected men (P < .0001) (Fig 1). Total protein S, which includes both bound and unbound protein S, was also sig- nificantly decreased in both groups of HIV-infected men, with mean levels of 17.7 f 2.1 pg/mL (range 16.0 to 20.0 pg/mL) in the three men with previous thrombosis ( P < .OO l), and 22.1 f 4.9 pg/mL (range 14.9 to 32.5 pg/mL, n = 22) in HIV-infected men without previous thrombosis (P < .02) compared with a mean level of 25.0 +. 3.2 pg/mL (range 18.1 to 32.0 pg/mL) in male controls (Fig I ) . Functional protein S determinations correlated with free protein S antigen levels ( r = 0.78, P < .005) (Fig 2). HIV-infected men with a prior history of thrombosis had a mean (+-SD) functional protein S value of 42.7% ? 9.1% (range 33 to 51%, n = 3) compared with a mean of 77.7% f 30.1% (range 27% to 128%, n = 22) in HIV-infected men without a previous thrombotic episode. Control men had a mean functional protein S level of 103.4% +- 20% (range 63% to 144%, n = 20). Functional protein S values were significantly different in HIV-infected men with (P < .0001) and without ( P < .003) previous thrombosis compared with control men. Free and total protein S antigen levels were also evaluated 3 to 6 months after the initial low- free protein S determination in 13 HIV-infected males. No significant differences between initial and follow-up protein S determinations for the group were seen.
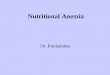
To determine whether the decreases in free protein S could be attributed to shifts in protein S to the complexed form, C4bBP was measured. C4bBP levels did not correlate with free protein S levels ( r = .12, NS). None of the group of HIV- infected men with decreased free protein S had increases in C4bBP. Two HIV-infected men who had normal levels of free protein S had increased C4bBP (Fig 3). Similar results were obtained with both the Laurell electroimmunoassay and the Liatest C4bBP. To obtain a qualitative estimate of the distribution of bound and free protein S, crossed immuno- electrophoresis was performed. A reduction in the height of the lower, more rapidly migrating free protein S peak was observed in 18 of 25 study patients examined (Fig 4), con- firming the decreased levels of free protein S obtained on the Laurell procedure. However, no changes were seen in the pattern of distribution of free and bound protein S. Variant protein S molecules have been shown in familial protein S deficiency.21 Immunoblot studies were performed on the 25 study patients to exclude the presence of a variant protein S molecule. Twenty-four patients had normal protein S im- munoblots. One patient (patient 9, Table l), without a pre- vious history of thrombosis, showed both a variant and nor- mal protein S molecule, with the variant protein S antigen migrating abnormally fast at approximately 66,000 molecular weight (mol wt) compared with the normal protein S at ap- proximately 7 1,000 mol wt.
The protein S status ofthe study group was compared with HIV disease seventy, degree of immunodeficiency, and med- ications. No correlation was seen between protein S deficiency and CDC classification, CD4+ cell levels, p24 antigen status, AZT use, or Pneumocystis carinii prophylaxis. There was a statistically significant correlation between decreases in pro- tein S and duration of HIV disease ( r = .37, P < .05).
IgG and IgM anticardiolipin antibodies were correlated with the free protein S levels (Fig 5). A significant linear re-
- - m 110
2 8 100
C W
Q m
U C
._ c 2 90
.E 80
n 70 4 J
60
t 0
t
4 ., u.
u 5
c .i. --
HIV with S Def HIV with nl S Control Males
Fig 3. C4b binding protein (C4bBP) in 25 HIV-study patients compared with 21 controls (Nl). HIV study patients were further divided by protein S status. The three patients with previous throm- bosis are indicated by (0). Two HIV patients with normal protein S levels had increased C4bBP. No statistically significant differences existed between the groups. Data shown here were performed by the Laurell assay.
For personal use only.on December 30, 2018. by guest www.bloodjournal.orgFrom

HIV AND PROTEIN S DEFICIENCY 1805
Fig 4. Crossed immunoelec- trophoresis of protein S in nor- mal plasma (A) and in two HI;' study patients (B and C). The two immunoprecipitation peaks associated with protein S are shown. The taller, slower-mi- gratingpeakrepresentsthebound protein S, while the lower, faster- migrating peak represents free protein S. Eighteen of 25 HIV- infected patients had a pattern similar to (C) with lower free protein S peaks than those ob- served in normal plasma. A
lationship existed between increasing IgG anticardiolipin an- tibody levels and decreasing free protein S levels (r = .67, P < .005). vWFAG, in contrast, did not correlate with free protein S levels (r = .I3, NS).
DISCUSSION
Protein S deficiency was commonly found in HIV-infected men. In our study, the incidence of decreased free protein S below the lower level established for the control male pop- ulation was higher (76%) than that reported by others (31%).15 One possible explanation for this discrepancy may be the longer mean duration of HIV infection in our study group compared with others. Although stage of disease, CD4 counts, and p24 antigen positivity did not correlate with decreased levels of free protein S, the duration of disease did statistically correlate with decreases in protein S. A similar lack of cor- relation with more advanced disease has been noted in one study,I5 but not in another."
C 8 0)
c q 6 rn
g7
1
t " 00 I
0 ' ' ' ' ' ' ' ' 1 1 ' ' 1 '11 10 20 30 40 50 W 70 80 90 103 110 120 130 " 560
IgG Anticardiolipin Antibody (GPL units)
Fig 5. Correlation between free protein S antigen levels and lgG anticardiolipin antibody levels in 24 study patients. A linear regres- sion line is drawn. A significant correlation is seen between in- creasing IgG-anticardiolipin-antibody levels and decreasing free protein S antigen levels (r = .67. P < .005). lgG anticardiolipin antibody levels are expressed in standard GPL units where 1 unit is equivalent to 1 rg/mL of an affinity-purified lgG standard sample (see Materials and Methods).
=-+ B C
+
The occurrence of thromboembolic events in 3 of 25 ran- domly selected long-term HIV-infected men, as well as the associated findings of free protein S deficiency, elevated vWF AG, and increased IgG-anticardiolipin antibodies in all 3 pa- tients with a history of thromboembolic disease, appears sig- nificant. Elevations in vWFAG have been associated with a large number of chronic diseases3* including HIV disease.33." Although it has been associated with conditions in which change or injury to the endothelium occurs, including ex- perimental'venous occl~sion.'~ it has not been shown to pre- dispose to clinical thrombosis. Increases in anticardiolipin antibodies, although associated with thrombosis in systemic lupus erythematosus?' have not been linked with thrombosis in HIV di~ease.~'-~" Based on these data, reduced protein S levels appear the most likely to contribute to the risk for thrombotic disease in HIV-infected men. It remains unclear whether increasing longevity in this population poses a con- stant increase in thrombotic risk. Of note, in contradistinction to this hypothesis, is the occurrence of thrombosis within I year of the onset of HIV symptomatology in two of the in- dividuals in this study. Cross-sectional or longitudinal studies are needed to clarify this.
Because C4bBP is an acute-phase reactant protein, ele- vations of C4bBP at times of inflammation can shift the pro- tein S from the free to the bound form. This shift results in a decrease in free protein S antigen and in protein S functional activity. However, protein S deficiency secondary to HIV disease results in decreased free and total protein S antigen levels, but normal C4bBP levels, suggesting these changes may be different than occur in an inflammatory response. Similar findings of normal C4bBP associated with reduced total protein S and quantitatively greater reduced free protein S levels have been associated with oral contraceptive use? pregnancy: and liver disease." This relatively greater decrease in free protein S is as expected when the relationship between free protein S level, total protein S antigen, and C4bBP is calculated from the dissociation constant of the protein S/ C4bBP complex.' In systemic lupus erythematosus, reduced free and normal total protein S have been rep~r ted , '~ sug- gesting a shift in distribution to the bound form caused by an increase in C4bBP levels.
The pathogenesis of the decrease in protein S levels asso- ciated with HIV disease remains to be elucidated. Protein S
For personal use only.on December 30, 2018. by guest www.bloodjournal.orgFrom

1806 STAHL ET AL
is synthesized by e n d ~ t h e l i u m , ~ ~ . ~ ’ hepatocyte^,'^ and mega- k a r y o c y t e ~ . ~ ~ In view of the lack of decrease in protein C, fibrinogen, and factors I1 and X, the current study does not implicate impaired hepatic synthesis of protein S as a possible cause for the HIV-associated decrease in free protein S. Be- cause abnormalities in several other substances secreted by the endothelium and involved in coagulation have been as- sociated with HIV infection,34 disturbances in endothelial function may play a role in the etiology of the reduced protein S. As has been observed by others,33 the present study showed that vWF was increased in association with HIV disease, al- though no correlation was found between increases in vWF and decreases in protein S. Other mechanisms besides altered production or secretion may occur with HIV infection, re- sulting in the observed findings. The linear correlation be- tween increased IgG-anticardiolipin antibodies and reduced free protein S levels seems relevant in this regard. Antiphos- pholipid antibodies have been postulated to interfere with the activated protein C/protein S complex at the phospholipid surface4’ and inhibition of the activated protein C complex has been ~hown.~’ .~ ’ A n abnormal interaction of protein S with the phospholipid membrane has also been postulated in association with antiphospholipid antibodies and func- tional protein S def i c i en~y .~ ’ ,~~ Other reports have also linked antigenic protein S deficiency with the presence of lupus an- t i c o a g u l a n t ~ , ~ ~ . ~ ~ suggesting the possibility that protein S, in addition to its affinity for phospholipid membranes, binds to antiphospholipid antibodies. In fact, anticardiolipin anti- bodies have been shown to be polyspecific and to strongly cross-react with other anionic phospholipid^.^^
Taken together, the results suggest that HIV-associated protein S deficiency may predispose infected individuals to thrombosis. The full clinical implications of these findings remain to be ascertained as the average life-span of HIV- infected patients increases with more effective antiviral agents and treatment of opportunistic infections. This study provides a strong rationale for further studies at the cellular level to elucidate the etiology of the decrease in protein S and the data strongly suggest that the presence of anticardiolipin or related antibodies may play a role in its pathogenesis.
ACKNOWLEDGMENT
The authors thank Tim Green for statistical assistance and Martha Byrd, Tamara Hine, and Danny Jue for technical assistance with anticardiolipin-antibody levels and amino acid determinations. Moreover, the authors thank Dr John Griffin for helpful discussions.
REFERENCES
1. Walker FJ: Regulation of activated protein C by a new protein. A possible function for bovine protein S. J Biol Chem 255:5521, 1980
2. Comp PC, Nixon RR, Cooper MR, Esmon C T Familial protein S deficiency is associated with recurrent thrombosis. J Clin Invest 74:2082, 1984
3. Comp PC, Esmon C T Recurrent venous thromboembolism in patients with a partial deficiency of protein S. N Engl J Med 3 1 1: 1525, 1984
4. Schwartz HP, Fischer M, Hopmeier P, Batard MA, Griffin JH: Plasma protein S deficiency in familial thrombotic disease. Blood 64:1297, 1984
5. Gladson CL, Scharrer I, Hack V, Beck KH, Griffin JH: The frequency of type I heterozygous protein S and protein C deficiency in 141 unrelated young patients with venous thrombosis. Thromb Haemost 59:18, 1988
6. Dahlback B: Purification of human C4b-binding protein and formation of its complex with vitamin K-dependent protein S. Biochem J 209:847, 1983
7. Comp PC, Doray D, Patton D, Esmon CT: An abnormal plasma distribution of protein S occurs in functional protein S deficiency. Blood 67504, 1986
8. Comp PC, Thurnau GR, Welsh J, Esmon C T Functional and immunologic protein S levels are decreased during pregnancy. Blood 685381, 1986
9. Boerger LM, Moms PC, Thurnau GR, Esmon CT, Comp PC: Oral contraceptives and gender affect protein S status. Blood 69:692, 1987
IO. Fair DS, Revak DJ: Quantitation of human protein S in the plasma of normal and warfarin-treated individuals by radioimmu- noassay. Thromb Res 36527, 1984
11. DAngelo AD, Vigano-DAngelo S, Esmon CT, Comp PC: Acquired deficiencies of protein S. Protein S activity during oral an- ticoagulation, in liver disease, and in disseminated intravascular co- agulation. J Clin Invest 81:1445, 1988
12. Vigano-D’Angelo S, D’Angelo A, Kaufman CE, Scholer C, Esmon CT, Comp PC: Protein S deficiency occurs in the nephrotic syndrome. Ann Intern Med 107:42, 1987
13. Allon M, Soffer 0, Evatt BL, Hixon G, Wideman CS: Protein S and C antigen levels in proteinuric patients: Dependence on type of glomerular pathology. Am J Hematol 31:96, 1989
14. Keeling DM, Campbell SJ, Mackie IJ, Machin SJ, Isenberg DA: Total and free protein S in Fystemic lupus erythematosus. Thromb Res 60:237, 1990
15. Lafeuillade A, Alessi MC, Poizot-Martin I, Dhiver C, Quilichini R, Aubert L, Gastaut JA, Juhan-Vague I: Protein S deficiency and HIV infection. N Engl J Med 324:1220, 1991 (letter)
16. Comp PC: Hereditary disorders predisposing to thrombosis, in Coller B (ed): Progress in Hemostasis and Thrombosis, vol 8. Or- lando, FL, Grune & Stratton, 1986, p 71
17. Seligsohn U, Berger A, Abend M, Rubin L, Attias D, Zivelin A, Rapaport SI: Homozygous protein C deficiency manifested by massive venous thrombosis in the newborn. N Engl J Med 310:559, 1984
18. Griffin JH, Gruber A, Fernandez JA: Reevaluation of total, free and bound protein S and C4b-binding protein levels in plasma anticoagulated with citrate or hirudin. Blood 79:3203, 1992
19. Comp PC, Forristall J, West CD, Trapp R G Free protein S levels are elevated in familial C4b-binding protein deficiency. Blood 76:2527, 1990
20. Schwarz HP, Heeb MJ, Lammle B, Berrettini M, Griffin JH: Quantitative immunoblotting of plasma and platelet protein S. Thromh Haemost 56:382, 1986
2 1. Schwarz HP, Heeb MJ, Lottenberg R, Roberts H, Griffin JH: Familial protein S deficiency with a variant protein S molecule in plasma and platelets. Blood 74:213, 1989
22. Wolf M, Boyer-Newmann C, Martinoli J-L, Leroy-Matheron C, Amiral J, Meyer D, Larrieu MJ: A new functional assay for human protein S activity using activated factor V as substrate. Thromb Hae- most 62:1144, 1989
23. Schleider MA, Nachman RL, Jaffe EA, Coleman M: A clinical study of the lupus anticoagulant. Blood 48:499, 1976
24. Johnson DA, Gautsch JW, Sportsman JR, Elder JH: Improved technique utilizing nonfat dry milk for analysis of proteins and nucleic acids transferred to nitrocellulose. Gene Anal Techn 1.3, 1984
For personal use only.on December 30, 2018. by guest www.bloodjournal.orgFrom

HIV AND PROTEIN S DEFICIENCY 1 a07
25. Hams EN, Gharavi AE, Patel SP, Hughes GRV: Evaluation of the anticardiolipin antibody test: Report of an international work- shop held 4 April 1986. Clin Exp Immunol68:215, 1987
26. Hollander M, Wolfe DA: Nonparametric Statistical Methods. New York, NY, Wiley, 1973
27. McNeil HP, Chesterman CN, Krilis SA: Immunology and clinical importance of antiphospholipid antibodies. Adv Immunol 49:193, 1991
28. Stimmler MM, Quismorio FP, McGehee WG, Boylen T, Sharma O P Anticardiolipin antibodies in acquired immunodeficiency syndrome. Arch Intern Med 149:1833, 1989
29. Mulhall BP, Naselli G, Whittingham S: Anticardiolipin an- tibodies in homosexual men: Prevalence and lack of association with human immunodeficiency virus (HIV) infection. J Clin Immunol9: 208, 1989
30. Taillan B, Roul C, Fuyibet J-G, Vinti H, Pesce A, Bayle J, Cassuto P, Dujardin P Antiphospholipid antibodies associated with human immunodeficiency virus infection. Arch Intem Med 150: 175, 1990
3 1. Francois B, Berruyer M, Causse X, DeChavame M, Trepo C: Acquired protein S deficiency: Correlation with advanced disease in HIV-1-infected patients. J Acquir Immune Defic Syndr 5:484, 1992
32. Sadler JE, Davie DW. Hemophilia A, Hemophilia B, and von Willebrand's Disease, in Stamatoyannopoulos G, Nienhuis AW, Leder P, Majurus DW (eds): The Molecular Basis of Blood Diseases. Phil- adelphia, PA, Saunders, 1987, p 608
33. Janier M, Flageul B, Drouet L, Scrobohaci ML, Villette JM, Palangie A, Cottenot F: Cutaneous and plasma values of von Wil- lebrand factor in AIDS A marker of endothelial stimulation? J Invest Dermatol 90:703, 1988
34. Lafeuillade A, Alessi MC, Poizot-Martin I, Boyer-Neumann C, Zandotti C, Quilichini R, Aubert L, Tamalet C, Juhan-Vague I, Gastaut JA: Endothelial cell dysfunction in HIV infection. J Acquire Immune Defic Syndr 5:127, 1992
35. Blann A: Changes in von Willebrand factor antigen levels in venous occlusions. Thromb Haemost 67:383, 199 I
36. Stern D, Brett J, Harris K, Nawroth P Participation of en- dothelial cells in the protein C-protein S anticoagulant pathway: The synthesis and release of protein S. J Cell Biol 102:1971, 1986
37. Fair DS, Marlar RA, Levin EG: Human endothelial cells syn- thesize protein S. Blood 67:1168, 1986
38. Fair DS, Marlar RA: Biosynthesis and secretion of factor VII, protein C, protein S, and the protein C inhibitor from a human hepatoma cell line. Blood 67:64, 1986
39. Ogura M, Tanabe N, Nishioka J, Suzuki K, Saito H: Biosyn- thesis and secretion of functional protein S by a human megakaryo- blastic cell line (Meg-01). Blood 70:301, 1987
40. Malia RG, Kitchen S, Greaves M, Preston FE: Inhibition of activated protein C and its cofactor protein S by antiphospholipid antibodies. B J Haematol 76:101, 1990
41. Lo SCL, Salem HH, Howard MA, Oldmeadow MJ, Firkin BG. Studies of natural anticoagulant proteins and anticardiolipin antibodies in patients with the lupus anticoagulant. B J Haematol 76:380, 1990
42. Rossi E, Gatti L, Guarneri D, Finotto E, Lombardi A, Preda L: Functional protein S in women with lupus anticoagulant inhibitor. Thromb Res 65:253, 1992
43. Moreb J, Kitchens CS: Acquired functional protein S defi- ciency, cerebral venous thrombosis, and coumarin skin necrosis in association with antiphospholipid syndrome: Report of two cases. Am J Med 87:207, 1989
44. Greaves M, Malia RG, Cooper P, Preston FE: Reduced free protein S in patients with the lupus anticoagulant. Br J Haematol 69:81, 1988 (suppl)
45. Friedman KD, Marlar RA, Gill JC, Endres-Brooks J, Mont- gomery RR: Protein S deficiency in patients with lupus anticoagulant. Blood 68:333, 1986 (abstr, suppl)
46. Hams EN, Gharavi AE, Loizou S, Derue G, Chan JK, Patel BM, Macworth-Young CG, Bunn CC, Hughes GRV: Crossreactivity of antiphospholipid antibodies. J Clin Lab Immunol l6:1, 1985
For personal use only.on December 30, 2018. by guest www.bloodjournal.orgFrom

1993 81: 1801-1807
CP Stahl, CS Wideman, TJ Spira, EC Haff, GJ Hixon and BL Evatt virus infection [see comments]Protein S deficiency in men with long-term human immunodeficiency
http://www.bloodjournal.org/content/81/7/1801.full.htmlUpdated information and services can be found at:
Articles on similar topics can be found in the following Blood collections
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requestsInformation about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprintsInformation about ordering reprints may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtmlInformation about subscriptions and ASH membership may be found online at:
Copyright 2011 by The American Society of Hematology; all rights reserved.Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American
For personal use only.on December 30, 2018. by guest www.bloodjournal.orgFrom