Embed Size (px)
Citation preview

December, 1946 PSEUDOCYESIS 395
omentum above the duodenum and the fold isballooned out with IO c.cs. of anaesthetic whichtracks around the common bile duct. The gall-bladder and biliary tract are now "damped off"and the operation can be performed confidentlyand the general anaesthetic can, if it is wished,be discontinued.
3. The Spleen.-The spleen is held forward fromthe splenic bed by the left hand the lienorenal andgastro splenic ligaments are soaked sub-peri-toneally, taking care that the anaesthetic is notinserted into one of the large vessels in the splenichilum by aspirating first.
Local Anaesthesia for Inguinal Herniaor Femoral HerniaLocal Infltration.-The "arrow-head" injection
is made on the side of the operation, using IO c.cs.in each direction and taking care to infiltrate thefull thickness evenly particularly the externaloblique muscle to relax Poupart's ligament,thereby making for a good exposure and accuratework. A taut Poupart's ligament gives pooraccess and stitches tend to cut out. The incisionruns from the anterior superior iliac spine to i inchinternal to the pubic spine, 3 c.cs. are injected sub-cuticularly and 3 c.cs. vertically down along thisline. At the pubic spine 6 c.cs. are injectedtowards the scrotum and perineum to desensitisethe termination of the long perineal nerves. Thedeep side of the neck of the hernial sac requiresinjection when it is exposed; absence of blue,indicates the need.Femoral Hernia.-In addition to the above
*insertion, infiltration is needed about the neck ofthe sac, below Poupart's ligament just externalto the pubic spine and especially around the inferiorside of the neck. If the Lotheisen approach isused then the neck is infiltrated all round, afterincision of the transversalis fascia on the posteriorwall of the inguinal canal above Poupart's ligament.
Local Anaesthesia for Supra Pubic Cys-tostomyThe direct infiltration is of the middle line from
the pubis to the umbilicus. The regional block isthe "arrow-head" injection on both sides.Then 20 c.cs. of anaesthetic are pooled supra
pubically in the perivesical tissues.
Discussion.-A method of Anaesthesia combininglocal and general agents for abdominal procedureshas been detailed. It has been used since May, I937,and is steadily satisfactory. It minimises strain atoperation for the patient and Surgical Team. It isa little slower than other methods. It reduces thepost-operative morbidity and nursing. Last, post-operative chests, headaches, retention of urine orabdominal distension are rare and seldom trouble-some. a
Blood-pressure charts of readings taken duringand after the operation show smaller ranges offall than after procedures under general or spinalanaesthesia.
In my experience no general anaesthetic is con-sistently satisfactory for any abdominal work,neither upper abdominal nor even herniae. Afew patients will not relax, but the local anaestheticmakes this certain.
Balanced anaesthesia is not new, it was firstmentioned by Lundy.
It is now inclined to be "old-fashioned" withthe advent of tubocurarine which is admittedlysuperb in competent hands, but it has its dangers.Expert anaesthetists are not everywhere and atall times available, nor is the drug in full supply.Therefore, for the outpost and emergency surgeon,and there are many such, this scheme of BalancedAnaesthesia is invaluable.
Conclusion.-A combination of local and generalanaesthesia for abdominal operation is describedwhich has proved successful since May, I937.
PSEUDOCYESISBy MARY DOREEN DALEY, M.D., M. R. C . O. G.
(Resident Assistant Obstetric and Gynaecological Surgeon, St. Helier County Hospital, Carshalton, Surrey.)Pseudocyesis is a curious condition in which
symptoms and signs of pregnancy are simulatedsufficiently to convince a woman, her friends andrelations, and in many cases her obstetrician, thatshe is pregnant. The term was first introduced byJohn Mason Good (a) in I823. Till then falsepregnancy was the name most often used, but asPajot (b) said: "II n'y a pas de fausses grossesses,il n'y a que faux diagnositics." Other terms fre-
quently found in the literature are spuriouspregnancy and phantom tumour.The condition has excited attention from very
early times and Hippocrates is said to haveobserved twelve cases in his practice in 300 B.C.Several famous women in history have beenafflicted in this way. Perhaps the most notableexample was Mary Tudor who thought that Godhad not given her a child because she had not
Protected by copyright.
on 11 October 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.254.395 on 1 D
ecember 1946. D
ownloaded from

POST-GRADUATE MEDICAL -JOURNAL
been sufficiently harsh with the heretics! Manypersecutions followed, after which the Queen feltsure she was pregnant as her abdomen enlargedand she suffered from vomiting. A few seventeenth-century cases are recorded, some of them byWilliam Harvey (c) who, in his Essay on Conception,described similar phenomena in animals. In theeighteenth-century, Mauriceau (d) described thecase of the wife of the French President who waswrongly thought to be pregnant by "many surgeons,physicians, and midwives." A curious case isthat of Joanna Southcott a religious prophetess,aged 64, who in I8I4 thought she was pregnant bythe Holy Spirit, and is said to have disappointedone hundred thousand people when the secondcoming of the Messiah did not eventuate at theexpected time. The poor woman died two monthslater and the post-mortem examination, attendedby fifteen physicians, apparently revea4ed nothingbut intestinal distension and a great increase inomental fat.
Recently, George Bivin', an American psycho-logist, has made an exhaustive inquiry into pseudo-cyesis. He, unfortunately, died before his taskwas finished; but a fellow worker, Pauline Klinger,took it up, and in I937 their book was published.They collected records of 444 cases from all overthe world, including several that Bivin had seenhimself. Apart from this there has been littlerecent literature on the subject and Englishwriters particularly seem to have ignored it.
History of the etiological theories is interestingand though some of them appear to us to besomewhat fantastic, it must be remembered thatwe know today very little of the true nature ofthe condition, in spite of having so many aids toinvestigation at our disposal. The earliest theoriesconcentrate on a physical basis for the condition,while more recently the psychological side hasbeen in greater prominence. It is inevitable thatwith the recent rapid growth in the science ofendocrinology, writers of this century shouldattempt to correlate hormonal dysfunction withpseudocyesis.
Hippocrates thought the abdominal distensionwas due to a combination of excess air in thestomach and retained menstrual fluid. Harveysuggested a similarity in the effect of coitus onthe brain and the uterus. The functions of bothare, as he pointed out, termed "conceptions," andhe adds that it is possible that "the woman shouldbe impregnanted by the conception of a generalimmaterial idea and become the artificer ofgeneration." Mauriceau (d) in I72I regarded theswelling as of uterine origin and caused by "strangematters as wind mixed with waters." La Mottein I746 agreed with him. Chapman (e) in I864,regarded excessive coitus in the newly married,
the menopause and uterine displacements asimportant etiological factors. His displacementtheory was that the abdominal muscles werethereby put on the stretch so that the fibres con-tracted irregularly and spasmodically thus imi-tating foetal movements. Simpson (f) in I87Idisproved the theory of intestinal distension bypassing a rectal tube while the abdominal swellingwas subsiding during induction of anaesthesia.No air escaped. He believed that diaphragmaticspasm pushing the intestine down in the abdominalcavity was the main factor concerned. Hisspeculation on corpus luteum, over-activity simu-lating pregnancy is interesting in the light of morerecent work.
Meantime, many others were doubting the partplayed by gaseous distension. Tichenor (g) inI879 quotes Meigs, who writes: "It is againstphysiology, against pathology, and it flies in theface of common sense to talk of wind distending amaterial like a womb. Air is too subtle to remainquietly locked in a bottle that has no cork in it."In I89I Haultain (h) did an interesting experi-
ment to prove that abdominal distension might bedue to muscular contraction. He passed a faradiccurrent through the abdominal muscles of ananaesthetised woman and reproduced the swellingthat was there before the anaesthetic was adminis-tered. He regarded flatulent distension as asecondary effect of the muscular contraction.The "prime cause" was, he said, purely nervous.A few years later much attention was paid,
especially in France, to hysteria in relation topseudocyesis. Bouchacourt (i) wrote of "deliriousconception.". When he. asked Charcot's opinionon the hysterical basis of the condition, the replywas "Hysterical, no: mental, yes." In I9IIJanet (j) showed that under the influence ofsuggestion respiration could be made of costaltype with depression of the diaphragm andabdominal distension which he ascribed to lossof tone of the abdominal wall. This seems to bea contradiction of Haultain's theory. At aboutthe same time Meynet (k) had no doubt that thecondition was hysterical, and quotes 'Babinsk'sdefinition of hysteria as -"a psychic state whichrenders the subject capable of autosuggestion."
In more recent times Berkeley2 has comparedthe diaphragmatic spasm of pseudocyesis withhysterical fixation of a joint. Recent Scottishwriters, Johnstone3 and Kerr, et alia4 recognisethe probable cause as hysterical abdominal fixationwith diaphragmatic spasm and an associatedintestinal distension. The group of authors justmentioned discuss disturbed hormonal activity.This aspect of the subject has been studied byHalban5 and Wagner6, who describe cases wherea corpus luteum cyst has caused amenorrhoea,
December, 1946P
rotected by copyright. on 11 O
ctober 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.22.254.395 on 1 Decem
ber 1946. Dow
nloaded from

PSEUDOCYESIS MARY DOREEN DALEY, AI.D., M.R.C.O.G.
/'.... :.j .L\
- K
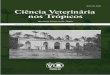
FIG. i i.-Standing up: before operation.
Protected by copyright.
on 11 October 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.254.395 on 1 D
ecember 1946. D
ownloaded from

PSEUDOCYESIS MARY DOREEN DALEY, AI.D., AI.R.C.O.G.
4......
: . :? ::ii0;1MP;: s
of
FIG. I2.-Lying down: after operation.
Protected by copyright.
on 11 October 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.254.395 on 1 D
ecember 1946. D
ownloaded from

PSEUDOCYESIS
breast activity, vulval discoloration, softening ofthe cervix, and erine enlargement. In some ofthese cases a laparotomy was performed for asuspected ectopic gestation. Macomber7 has des-cribed two cases of decidual reaction in womenwhose husbands were sterile. He correlates thiswith pseudopregnancy in animals.
In an effort to classify the confused ideas on theetiology of this condition, Bivin made a detailedanalysis of the 444 case records he had been ableto collect. Some rather unexpected facts as wellas many more obvious ones were brought out. In73 per cent of the cases where age had been notedit was between 15 and 39 years. The figures didnot bear out the usually accepted theory that thecondition is commonest in newly-married women,and in those at the menopause. Nearly three-quarters of the patients were married. Of them2I had re-married and there seemed to be someincrease in the frequency of pseudocyesis at thebeginning of a second marriage. Parity andsocial status did not bear any constant relation tothe condition.The emotional stability of the patients was
studied from the data available. Though aneuropathic tendency was fairly common it wasby no means invariable. The desire to have achild was frequently stressed, but in 3I cases ofthe series there was definite fear of pregnancy. Afew multiparous patients were said to be quiteindifferent to having another child. Hysteria hadbeen diagnosed in 34 cases, but in some thereseemed to be little ground for the diagnosis.Suggestion or auto-suggestion seemed in somepatients to play an important part. This occurredespecially in newly-married women who misseda period or two and were told by a doctor thatpregnancy was probable. Conviction that she waspregnant was shared by all cases.The symptoms and signs of pregnancy have all
been noted on several occasions. In over half ofBivin's series there was complete amenorrhoea.In many cases menstruation was irregular. Whit-ridge Williams8 notes that menstrual irregularityrather than amenorrhoea is more common in theyounger women. In over half of the amenorrhoeicpatients the duration was nine months or more,but many of these were approaching the menopause.Several cases are recorded in which menstruationoccurred within a day or so of the woman beingtold she was not pregnant.Abdominal enlargement was present in all except
three of the cases in which the abdomen wasdescribed. The indefinite outline of the enlarge-ment is stressed. In many cases the swelling wasgradual and corresponded to the time ofamenorrhoea. "Foetal movements" were veryfrequently noted and usually occurred at the
expected time. Whitridge Williams8 describesmovements which the patient feared were visibleto onlookers. The "foetal heart" is said to havebeen counted by doctors on several occasions.
Breast changes are of frequent occurrence andwere described in more than one third of theseries. Though activity of breasts carn be dis-counted in parous women, milk secretion wasrecorded in some of the nulliparous cases.
Nausea, vomiting, constipation, and capriciousappetite are common. Mary Tudor is said tohave had severe nausea.Labour was simulated in a large number of
Bivin's series and in pre-anaesthetic days, Caesareansection was performed for some cases. Apparentlythere was a remarkably realistic "labour" in somenulliparous cases.The duration of the pseudocyesis varies enor-
mously: 43 per cent of Bivin's cases lasted ninemonths. Janas describes a true pregnancy follow-ing pseudocyesis in a woman of i8. Except forfour days bleeding foll6wing "labour" at the280th day there was amenorrhoea for I9 months.Montgomery (1) tells of a lady who consultedDupuytren declaring she was i8 years pregnant.He advised her to swallow a private tutor for herson!The diagnosis has in many cases caused difficulty.
One hundred and sixty recorded cases havedeceived doctors. In days gone by there wasmuch more excuse for mistakes to be made asantenatal care was so infrequent and many patientsobjected to any examination. Today it is easyto disprove "pregnancy" by anaesthesia, a Fried-man test, or a radiogram. Difficulties arise onlybecause pseudocyesis is not considered. Thedifferential diagnosis is between abnormalities ofpregnancy, abdominal tumours, distended bladderand ascites as well as a straightforward pregnancy.Those who have missed a case of pseudocyesismay take some comfort from De Leelo who says"Pseudocyesis has baffled the diagnostic ability ofthe ablest surgeons and accoucheurs."The treatment is a more difficult problem even
than diagnosis because it is frequently almostimpossible to convince the patient that she is notpregnant, and as Smith (m) says, "All women whoare finally told they are not pregnant hate thephysician and do not believe him." Deceit waspractised by a few of the older physicians one ofwhom, for example, told the woman he hadremoved a stillborn child. Unfortunately shethen became convinced she had twins. Especiallyin France in the early part of this century hypnosisand suggestion were given trial with some goodresults. It was s'aid that suggestion needed an"incubation period" before it became effective.Anaesthesia was first used in these cases by
December, .7946 397P
rotected by copyright. on 11 O
ctober 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.22.254.395 on 1 Decem
ber 1946. Dow
nloaded from

POST-GRADUATE MEDICAL JOURNAL
Simpson (f) in I849 and though the distensionmay return when the patient regains consciousness,a cure is sometimes effected. It is well to haverelatives present so that they may help to convincethe patient she is not pregnant if the swellingreturns. Drugs have been frequently used tostart menstruation, but it seems likely that theirefficacy is due to suggestion. Other treatmentsthat have probably acted in the same way aremassage, replacement of the uterus by a pessaryand curettage.
Mrs. I. B., para o, aged eighteen, first attended ahospital ante-natal clinic on July 3, I940. She gave ahistory of amenorrhoea since January 28, I940. Pre-viously she had had a regular menstrual cycle of 4-5/28days since the menarche at the age of fourteen. Shecomplained of breathlessness on exertion and ankleswelling, and, as she had been in hospital in 1936 as acase of early mitral stenosis, she was admitted for investi-gation. Scrutiny of her previous notes showed that shehad beehi seen by the psychiatrist at that time on accountof emotional instability, but he could find no evidenceof hysteria. One of the clinicians who saw her notedlower abdominal fullness. She had been married sinceNovember I939, and was very anxious to have a baby.Pre-marital intercourse was acknowledged. About twomonths after the last period at the end of January, shehad nausea and occasional vomiting for about a month.When this was improving she noticed an increase in the-size of her breasts and says that clear fluid came fromthem. In the fourth month her abdomen started toenlarge, and continued to do so till after she attended our-clinic. On May I4th she had slight blood-stained dis-charge for a day.
Examination showed a pale, plump girl who was undulymature for her age. The breasts were apparently active.The abdomen was difficult to palpate owing to obesityand poor relaxation, but gave the impression of a 26 weeks'pregnancy, i.e. a little bigger than her dates. The foetalheart was not heard, but the patient said she had feltmovements for the last few weeks. No evidence of cardiacfailure was found, and her dyspnoea and history of oedemawere attributed to anaemia (haemoglobin 68 per cent).
Progress.-After rest, a well-balanced diet (which wasunusual for her), and iron therapy, she was dischargedfrom hospital a fortnight later feeling much better. Aweek later she was readmitted on account of a slight showand backache. Threatened premature labour was diag-nosed and she was treated with progesterone and vita-min E, and after four days bleeding ceased. She waskept in hospital for a fortnight. The notes show that atthat time the uterus appeared to be about the size of a30 weeks' pregnancy, but that the presentation was diffi-cult to make out. The foetal heart is said to have beenheard and the patient was feeling movements.On August 26th, a fortnight later, she was again
admitted, complaining this time of lower abdominal pain.and recent vomiting. Examination showed an abdomenslightly more enlarged than previously. The foetal heartwas not heard, and it was considered that foetal deathmust have occurred recently. Two days later bleedingstarted again, and the patient was told that the chances*of the baby's survival were small. This distressed herconsiderably. On this occasion for the first time thepatient was seen by the Director of the unit.
It was noticed that the abdomen was hyper-resonant,-and the possibility arose that a pregnancy did not existat all. The abdomen was diffusely enlarged, especiallybelow the umbilicus (girth 37 in.), but the "tumour" had
no definite edge. Foetal parts could not be felt. Therewas no thrill nor ascites. Examination of the vulva didnot show suggestive discoloration, but the cervix wasslightly softened. The uterus could not be definitelydefined. The breasts were large and showed Mont-gomery's tubercles, but secretion could not be expressed.Friedman examination was negative and X-rays showedno foetal parts. A barium enema excluded a coloniclesion.A tentative suggestion of pseudocyesis was made, but
we were somewhat unwilling to consider this possibilityseriously in so young a patient. To determine the diag-nosis, she was prepared for examination under anaesthesia.After induction with gas, oxygen and ether, on Septem-ber 20th, the abdomen became soft, distension almostcompletely disappeared, and there was no evidence of anytumour. Girth was then 33 in. Vaginal examinationshowed a uterus normal in size and position. The accom-panying photographs (Fig. i and 2) show the abdominalcontour the day before and a few hours after the anaes-thetic.The next day the girth was increased to 36 in. The
patient was told she was not pregnant, but as she hadreconciled herself to the death of the "foetus" she wasnot unduly distressed. Two days later she was discharged.Follow-up.November 4, I940.-Attended out-patient after a
holiday in the country. She had been well except for anattack of faintness in the previous week. Bleeding hadstarted on the day of discharge and lasted four days. Itrecurred on October i6th and continued for a week.Girth 33 in. Montgomery's follicles still apparent. P. V.Cervix soft. Body of uterus and appendages showed noabnormalities. There was no evidence of pharyngeal or"glove and stocking" anaesthesia.November I5, I940.-Endometrial biopsy taken on the
30th day of the cycle showed a somewhat atrophic endo-metrium but with some evidence of secretory activity.November I9, I940.-Seen by the same psychiatrist who
had seen her in I936. He suggested that "amenorrhoeaoccurring two months after her marriage combined withthe previous tendency to fullness of the abdomen servedto complete the essentials of the picture." He advisedfurther psychological investigation of the causes of herbelief that she was pregnant.
This case illustrates how, even at the present day, casesof pseudocyesis can be missed. The moral is that in everycase of suspected pregnancy where the outline of theuterus cannot be clearly defined, further investigationwith X-ray or biological tests should be carried out.
I would like to thank Professor James Young forpermission to describe this case.
ConclusionsIt is difficult to draw any sati-factory conclusions
with regard to this subject which has baffled themasters of obstetrics, psychology, and medicinefor so many centuries. The etiology is still obscurebut it is hoped that when more is known of theinterrelation between psychology and endocrinologythe position will be clearer.
Macgregor" has shown that 60 per cent of casesof secondary amenorrhoea where no pathology ispresent are due to psychological upsets. Theemotional reactions of sexual intercourse maycause temporary amenorrhoea thus making thewoman believe herself to be pregnant. In somecases, especially if there is a neuropathic tendency
December, I946P
rotected by copyright. on 11 O
ctober 2018 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.22.254.395 on 1 Decem
ber 1946. Dow
nloaded from

December, 1946 TREATMENT OF VINCENT'S INFECTION 399
and when for some reason pregnancy is of especiallygreat importance to the woman, abdominal enlarge-ment and other symptoms follow the amenorrhoea.Diaphragmatic spasm seems to be the mostplausible theory of the cause of the distensionbecause of the rapid effect of anaesthesia. Ifdiagnosis cannot be made clinically with certainty,radiograms and Friedman tests will show con-clusively whether or not the woman is pregnant.It is important to bear in mind the possibility ofpseudocyesis in any atypical "pregnancy" formost mistakes arise at the present day becausethis diagnosis is not considered. Anaesthesia is avaluable combined diagnostic and therapeutic aid.If the patient still believes herself to be pregnantafter the anaesthetic treatment along psychologicallines should be given a trial.
REFERENCESI. BIvIN, G. D., and KLINGER, P. (1937), Pseudocyesis.2. BERKELEY, C. (I922), Midwifery by Ten Teachers.3. JOHNSTONE, R. W. (I932), Textbook of Midwifery.
4. KERR, J. M., et al. (1923), Combined Textbook of Obstetrics and Gynae-cology.
5. HALBAN, J. (I9I5), Zentralb. f. Gynakologie, 39, 409.6. WAGNER (I928), Zentralb. f. Gynakologie, 52, Io.7. MACOMBER, D. (1932), J. Amer. Med. Ass., 98, 4, 304.8. WHITRIDGE WILLIAMS, J. (I923), Textbook of Obstetrics.9. JANA, A. P. "A Case of Pseudocyesis Followed by True Pregnancy.'"
Ind. Med. Gaz., Aug. 1934, 445.Io. DE LEE, J.I I. MACGREGOR.
Quoted from BIVIN, G. D. and KLINGER, P.:(a) GOOD, J. M. (i823), A Physiological System of Nosology with a
Corrected and Simplified Nomenclature, 443.(b) PAJOT, C. (i882), Travaux d'obstetrique et de gynecologie; precedes
d'elements de pratique obstetricale, 679.(c) HARVEY, W. (i847), Works of William Harvey. Translation by Willis,
624.(d) MAURICEAU, F. (I72i-8), Traitd des maladies des femmes grossesses et
de celles qui sont accouchees. 6th ed. 555.(e) CHAPMAN, E. M. (i864), "Spurious Pregnancy, its Symptoms,
Diagnosis, and Treatment, with a Record of Cases," Amer. Med.Times, 9, 50, 62.
(f) SIMPSON, J. Y. (I87I), Clinical Lectures on the Diseases of Women.Edit. A. L. Simpson, Vol. III.
(g) TICHENOR, E. J. (I879), "Phantom Turmour or What Is It." Obst.Gaz. 2, 7-I3.
(h) HALTAIN, F. W. (I89I), "Spurious Pregnancy," Amer. J. Med. Sci.101, 342-5.
(i) BOUCHACOURT, A. (I892), "Sur la grossesse nerveus au imaginaire,'"Lyon Med., 69,192I.
(j) JANET, P. (IgII), L' tat mental des hysteriques. 2nd ed. 708.(k) MEYNET, J. (I907), "Du diagnostic de la grossesse reveuse," Marseilles.
Med., 44, 4I7-529.(1) MONTGOMERY, F. W. (i857), Signs and Symptoms of Pregnancy, 568.(m) SMITH, W. S. (g902), "Pseudopregnancy," Am. J. Obst. ,46, 79-85.
MODERN TREATMENT OF VINCENT'S INFECTIONBy F. W. E. WAGNER, M.A., Sc.D.
Fellow of the Royal Academy of Medicine in Ireland. Fellow of the Royal Society of Trojpical Medicine.
It is a true estimate to say that the incidence ofVincent's Infection has increased to an alarmingextent during recent years. We must recognisethis disease as a grave menace to the health of thenation, and that at a time when health, strengthand vigour are more than ever necessary for thework of restoration and reconstruction. Neverbefore was the national need so great for healthybodies and healthy minds. As a nation we aresuffering from under-nourishment, unhygienic andinadequate housing conditions and war-strain. Itis apparent in the poor physique and the lack ofstamina so painfully evident in modern life.Capacity for resisting infection is today at a lowebb.The incidence of Vincent's Infection is particu-
larly heavy amongst industrial workers; and thisis probably due to transmission of infection byimperfectly cleansed spoons, forks and drinkingvessels in Works Canteens. This fruitful sourceof infection should be first on the list for attack inany organised and effective campaign. Stepsshould be taken to bring home to workers thegravity of the disease, the importance of avoidinginfection and of obtaining skilled treatment inthe early stages. It is unfortunate that thegeneral public does not at all appreciate the
gravity of Vincent's Infection, or its far-reachingsystemic consequences. The mere matter of aninflamed condition of the gums seems to most laypersons a comparatively trivial thing, with theunhappy result that they do not seek advice andtreatment until the disease is in its advancedstages with most of its evil sequelae in full play.This may be explained by the fact that in theearlier stages the two factors which usually impelpeople to seek medical or dental treatment-painand impairment of function-are absent. Theindividual is not the only sufferer by reason ofthis procrastination; the community suffers too,for the infected person is a source of potentialdanger, since he infects every drinking-vessel,spoon or fork that he uses. Early diagnosis andearly treatment are of the utmost importance forthe patient's own sake, to prevent the develop-ment of remote systemic consequences, and alsoto check the spread of the disease. May I repeatthat Vincent's Infection is today a grave menaceto the public health? I base that consideredopinion on the experience of a large and busydental practice which deals with a considerablenumber of industrial workers in an importantcentre of industry. The number of those who
Protected by copyright.
on 11 October 2018 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.22.254.395 on 1 D
ecember 1946. D
ownloaded from