Embed Size (px)
Citation preview

Psoriasis: Which Drug for Which Patient?
Mark Lebwohl, MD
Sol and Clara Kest Professor And Chairman
Kimberly and Eric J. Waldman Department of Dermatology
Icahn School of Medicine at Mount Sinai

Mark Lebwohl is an employee of Mount Sinai which receives research funds from: Abbvie, Amgen, Boehringer Ingelheim, Celgene, Eli Lilly, Janssen / Johnson & Johnson, Kadmon, Medimmune/Astra Zeneca, Novartis, Pfizer, Valeant and ViDac. Dr. Lebwohl is also a consultant for Allergan, Aqua Leo-pharma,and Promius.
Disclosure

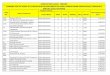
DRUG PsA OBESITY CARDIAC CA +ANA
LUPUS
MS CROHN HEPATITIS C Ab +
HBsAg+ Anti-HBc+
ETANERCEPT
ADALIMUMAB
INFLIXIMAB
CERTOLIZUMAB
USTEKINUMAB
SECUKINUMAB
IXEKIZUMAB
BRODALUMAB
GUSELKUMAB
TILDRAKIZUMAB
RISANKIZUMAB
MIRIKIZUMAB
APREMILAST
METHOTREXATE
CYCLOSPORINE
ACITRETIN

Drug-Induced SLE Associated
with Etanercept Therapy1
• 4 patients.
• Manifestations including fever, arthritis, discoid skin changes, rash, pleuritic pain, ANA, anti-dsDNA, anti-histone, hypocomplementemia, anti-Sm, anti-RNP.
• No baseline serologies.
• All resolved with discontinuation of etanercept and/or addition of corticosteroids.
1 Shakoor N et al. Lancet 2002;359(9306):579-80.

TNF- Inhibitor Induced Lupus Classic DILE1 TNF-α inhibitor
DILE2
ANA >95% 100%
dsDNA <1% 91%
Antihistone >95% 57%
Decreased complement
<1% 59%
Rash 27% 72%
1. Benucci et al Clin Rheumatol 27:91-95
2. Zimmerman et al. Semin Arthritis Rheum: 2008 Jun;37(6):381-7

Regression of subacute cutaneous
lupus erythematosus in a patient with
rheumatoid arthritis treated with a biologic tumor
necrosis factor
alpha-blocking agent: comment
on the article by Pisetsky and
the letter from Aringer et al. Fautrel B, Foltz V, Frances C,
Bourgeois P, Rozenberg S.
Arthritis Rheum. 2002 May;46(5):1408-9.

Safety and efficacy of
tumor necrosis factor
alpha blockade in systemic lupus erythematosus:
an open-label study. Aringer M et al.
Arthritis Rheum.
2004 Oct;50(10):3161-9.
•↓proteinuria, arthritis, C4
•↑autoantibodies

Treatment of coexistent psoriasis and lupus
erythematosus.
Varada S, Gottlieb AB, Merola JF, Saraiya AR, Tintle SJ.
J Am Acad Dermatol. 2015;72:253-60.
“Anti-TNF-α agents, ustekinumab, and abatacept may be valid
treatment options for patients with concomitant LE and
psoriasis. Clinical lupus flares in LE patients treated with
TNF-α inhibitors were infrequent.”

Apremilast for discoid lupus erythematosus: results of
a phase 2, open-label, single-arm, pilot study.
De Souza A, Strober BE, Merola JF, Oliver
S, Franks AG Jr.
J Drugs Dermatol. 2012;11:1224-6.

A 2 year, open ended trial of methotrexate in systemic lupus
erythematosus. Wilson K, Abeles M.
J Rheumatol. 1994;21(9):1674-7.
Discoid lupus erythematosus: successful treatment with oral
methotrexate. Goldstein E, Carey W.
Arch Dermatol. 1994;130(7):938-9.

Hypertrophic lupus erythematosus treated successfully with
acitretin as monotherapy. Al-Mutairi N, Rijhwani M, Nour-Eldin O.
J Dermatol. 2005;32(6):482-6.
Efficiency of acitretin in the treatment of cutaneous lupus
erythematosus. Ruzicka T, Meurer M, Bieber T.
Arch Dermatol. 1988;124(6):897-902.

Low dose cyclosporine A in the treatment of resistant
proliferative lupus nephritis. Sheikholeslami M, et al.
Mod Rheumatol. 2017:1-7 [Epub ahead of print].
Therapeutic drug monitoring of cyclosporine
microemulsion in patients with corticosteroid-resistant
systemic lupus erythematosus. Wada Y, et al.
Mod Rheumatol. 2015;25(5):708-13.

TNF neutralization in MS: results of a
randomized, placebo-controlled multicenter
study.
The Lenercept Multiple Sclerosis Study
Group and The University of British
Columbia MS/MRI Analysis Group.
Neurology. 1999;53:457-65.
• MS exacerbations ↑ with lenercept.

Demyelination occurring during
anti-tumor necrosis factor alpha
therapy for inflammatory arthritides. Mohan N, et al.
Arthritis Rheum. 2001;44:2862-9.
• 17 – etanercept, 2 – infliximab
• partial or complete resolution on d/c
• 1 positive rechallenge

Repeated subcutaneous injections of IL12/23
p40 neutralising antibody, ustekinumab, in
patients with relapsing-remitting multiple
sclerosis: a phase II, double-blind, placebo-
controlled, randomised, dose-ranging study. Segal BM et al.
Lancet Neurol 2008;7:796-804.
• UST → no effect on MS

Activity of secukinumab, an anti-IL-17A antibody,
on brain lesions in RRMS: results from a randomized,
proof-of-concept study.
Havrdová E, et al
J Neurol. 2016;263:1287-95.

Secukinumab, a human anti-IL-17A monoclonal antibody, for moderate to severe Crohn's disease: unexpected results of a randomised, double-blind placebo-controlled trial.
Hueber W, Sands BE, et al
Gut. 2012;61(12):1693-700.
Secukinumab not effective

No Definitive Role of Secukinumab in Crohn’s Disease Entire treatment period – exposure-adjusted (52 weeks)
• Potential involvement of IL-17 in Crohn’s disease however published trials have not shown clinical benefit or disease exacerbation, consistent with Novartis Phase II in Crohn’s
• Phase III incidence rate as expected with psoriasis – No dose relationship between secukinumab doses
– All cases with Crohn’s disease had prior history
Based on all AEs
AIN457 300 mg (n=1410)
n (IR) [95% CI]
AIN457 150 mg (n=1395)
n (IR) [95% CI]
Placebo (n=793) n (IR)
[95% CI]
Etanercept (n=323) n (IR)
[95% CI]
Inflammatory bowel disease 3 (0.26)
[0.05, 0.75] 4 (0.35)
[0.10, 0.90] 0 (0.00)
[0.0, 1.83] 1 (0.34)
[0.01, 1.90]
Colitis ulcerative 2 (0.17)
[0.02, 0.61] 2 (0.18)
[0.02, 0.63] 0 (0.00)
[0.0, 1.83] 1 (0.34)
[0.01, 1.90]
Crohn’s disease* 0 (0.00)
[0.0, 0.31] 2 (0.18)
[0.02, 0.63] 0 (0.00)
[0.0, 1.83] 0 (0.00)
[0.0, 1.26]
Anal fistula** 1 (0.08)
[0.0, 0.47] 0 (0.00)
[0.0, 0.32] 0 (0.00)
[0.0, 1.83] 0 (0.00)
[0.0, 1.26]
IR=Exposure-adjusted incidence rate per 100 patient-years.
A third case of Crohn’s disease occurred in study A2211E1- 150 mg Start of Relapse arm
** Not associated with inflammatory bowel disease

Does exposure to isotretinoin increase the risk for the
development of inflammatory bowel disease?
A meta-analysis.
Lee SY, Jamal MM, Nguyen ET, Bechtold ML, Nguyen DL.
Eur J Gastroenterol Hepatol. 2016;28:210-6.
NO

Isotretinoin and inflammatory bowel disease: trial lawyer misuse of
science and FDA warnings.
Tenner S.
Am J Gastroenterol. 2014;109:570-1.
Isotretinoin, acne, and Crohn's disease: a convergence of bad skin,
bad science, and bad litigation creates the perfect storm.
Gastroenterol Hepatol (NY). 2013;9:752-5.

Etanercept therapy for patients with psoriatic arthritis and
concurrent hepatitis C virus infection: report of 3 cases. Magliocco MA, Gottlieb AB.
J Am Acad Dermatol. 2004;51(4):580-4.
Etanercept monotherapy for a patient with psoriasis, psoriatic arthritis, and
concomitant hepatitis C infection. Rokhsar C, Rabhan N, Cohen SR.
J Am Acad Dermatol. 2006;54:361-2.
Etanercept therapy in two patients with psoriasis and concomitant hepatitis C. De Simone C, Paradisi A, Capizzi R, Carbone A, Siciliano M, Amerio PL.
J Am Acad Dermatol. 2006;54:1102-4.
Etanercept treatment for three months is safe in patients with rheumatological
manifestations associated with hepatitis C virus.
Marotte H et al.
Rheumatology (Oxford). 2007;46:97-9. Epub 2006 May 23.

Etanercept and Hepatitis C. Pritchard C.
Journal of Clinical Rheumatology.
1999; 5:179-180.
• 1 patient with rheumatoid arthritis & hepatitis C
• etanercept LFT's and viral titers
• d/c etanercept improved liver function

Safety and effectiveness of ustekinumab
and antitumour necrosis factor therapy in
patients with psoriasis and chronic viral
hepatitis B or C: a retrospective,
multicentre study in a clinical setting. Navarro R. et al.
Br J Dermatol. 2013;168(3):609-13.
• ETN (21), ADA (4), UST (4), IFX (2)
• HCV (20), HBV (5)

• ↑LFT’s 2x in one pt (ETN)
• 2 pt’s ↑viral load during followup.
• 2pt’s →hepatocellular ca. (ETN)
Navarro R. et al.
Br J Dermatol. 2013;168(3):609-13.
“Biologic therapy was effective and safe for the
majority of our patients with HCV and HBV
infection”

Etanercept as an adjuvant to interferon and
ribavirin in treatment-naive patients with chronic
hepatitis C virus infection: a phase 2 randomized,
double-blind, placebo-controlled study. Zein NN, for the Etanercept Study Group.
Journal of Hepatology 2005;42:315-322.
• HCV, RNA was absent in 63% (12/19) etanercept
patients, 32% (8/25) placebo patients.
• Patients receiving etanercept had lower frequency of
most adverse events.
• liver bx regression of fibrosis:
6/11(55%) vs 2/6(33%)

Infliximab therapy for Crohn’s disease
in the presence of chronic hepatitis C infection. Campbell S, Ghosh S.
Eur J Gastroenterol Hepatol.
2001;13:191-2.
• Hepatitis C:
Infliximab No worsening of
LFT’s or vital titers by PCR.

Induction of clinical remission with adalimumab-methotrexate combination
therapy in a patient with rheumatoid arthritis and concomitant hepatitis C
virus infection. Noguchi O, Gibo Y
Mod Rheumatol. 2011;21:696-700.
Drug-induced liver injury caused by adalimumab: a case report and
review of the bibliography. Frider B, Bruno A, Ponte M, Amante M.
Case Reports Hepatol. 2013;2013:406901.
Use of tumor necrosis factor-alpha (TNF-alpha) antagonists infliximab,
etanercept, and adalimumab in patients with concurrent rheumatoid arthritis
and hepatitis B or hepatitis C: a retrospective record review of 11 patients. Li S, Kaur PP, Chan V, Berney S.
Clin Rheumatol. 2009;28:787-91.

• Two patients showed a transient elevation in AST and/or
ALT from normal, but in all 11 patients, AST and ALT
levels were within one time the upper range of normal at
the conclusion of the study.
• No significant increase in viral load was seen except one
patient who showed a fourfold increase from baseline.
• “Use of these agents in patients with HBV or HCV may be
associated with a transient transaminitis but appears to be
safe overall. In both groups, frequent monitoring of serum
transaminase levels and viral load is essential.”
Li S, Kaur PP, Chan V, Berney S.Clin Rheumatol. 2009;28:787-91.

The safety profile of ustekinumab in the treatment of
psoriasis patients with concurrent hepatitis B or
hepatitis C. Chiu, H-Y et al.
Br J Dermatol 2013; 169:1295-1303.
• Reactivation of HCV and hepatocellular
ca in 1/4 pts rx’d with UST
•No ↑ in ALT, AST

Psoriasis treated with ustekinumab in a
patient with hepatitis C.
Abuchar A, Vitiello M, Kerdel FA.
Int J Dermatol. 2013 Mar;52(3):381-2.

Safety of Secukinumab in Hepatitis B Virus SL Bevans, TT Mayo, BE Elewski,
in press
• Reports of HBV infection (5patients), HCV infection (3
patients), and HBV and HCV co-infection (1 patient), all
without viral reactivation or significant elevation in liver
enzymes.

Apremilast for a psoriasis patient with HIV and
hepatitis C. Reddy SP, Shah VV, Wu JJ.
J Eur Acad Dermatol Venereol. 2017.
doi:10.1111/jdv.14301.[Epub ahead of print].

Complications in methotrexate treatment of
psoriasis with particular reference to liver
fibrosis. Ashton RE, Millward-Sadler GH, White JE.
J Invest Dermatol 1982;79:229-32
• hepatic fibrosis in 9/38(24%) after 5 years

Does cyclospsorine have a beneficial effect
on the course of chronic hepatitis C infection
after renal transplantation? Kamar N, Selves J, Sandres-Saune K, et al.
Transplant Proc. 2006;38:1329-32.
• “…HCV infection is not harmful to liver histology
in more than 50% of renal transplant patients with
grafts functioning more than 6 years. Cyclosporine
might have beneficial effects on the natural course
of HCV infection”

Successful treatment with cyclosporine A of HCV-driven
chronic liver disease mimicking autoimmune hepatitis in a
patient with common variable immunodeficiency.
Martire B, Gentile A, Francavilla R, et al.
Immunopharmacol Immunotoxicol. 2005;27:535-43.
Evaluation of the anti-hepatitis C virus effects of cyclophilin
inhibitors, cyclosporin A, and NIM811.
Goto K, Watashi K, Murata T, et al.
Biochem Biophys Res Commun. 2006;343:879-84.

Suppression of hepatitis C virus replication by cyclosporin a
is mediated by blockade of cyclophilins.
Nakagawa M, Sakamoto N, Tanabe Y, et al.
Gastroenterology. 2005;129:1031-41.
Specific inhibition of hepatitis C virus replication by
cyclosporin A.
Nakagawa M, Sakamoto N, Enomoto N, et al.
Biochem Biophys Res Commun. 2004;313:42-7.

Cyclosporin A in chronic active hepatitis.
Results of a pilot study of 20 patients. Friedrich K, Henning H.
Z Gastroenterol 1988;26:265-70.
• Only 3 improved
• 1 case of hepatotoxicity of CsA

The role of different immunosuppression in the long-term histological outcome of HCV reinfection after liver transplantation for HCV cirrhosis.
Papatheodoridis GV, Davies S, Dhillon AP, Teixeira R, Goulis J, Davidson B,Rolles K, Dusheiko G, Burroughs AK.Transplantation. 2001 Aug 15;72(3):412-8.
-cyclosporine associated with recurrence & progression of hepatitis C
-need for retransplantation in 10-25% of patients within 5 years

Reactivation of chronic hepatitis C after withdrawal of
immunosuppressive therapy.
Gruber A, Lundberg LG, Bjorkholm M.
J Intern Med 1993;234:223-5.
Activation of hepatitis C virus following
immunosuppressive treatment.
Yoshiba M, Sekiyama K, Sugata F, et al.
Dig Dis Sci. 1992;37:478.

Effects of acitretin on the liver Roenigk HH Jr, Callen JP, Guzzo CA,
Katz HI, Lowe N, Madison K, Nigra T,
FiedlerVC, Armstrong RB. J Am Acad
Dermatol 1999 Oct;41(4):584-8
-No hepatotoxicity on liver bx
after 2 yrs

DRUG PsA OBESITY CARDIAC CA +ANA
LUPUS
MS CROHN HEPATITIS C Ab +
HBsAg+ Anti-HBc+
ETANERCEPT + + + - + +/- X + +* - +/-*
ADALIMUMAB + + + - + +/- X + +* - +/-*
INFLIXIMAB + + + - + +/- X + +* - +/-*
CERTOLIZUMAB + + + - + +/- X + +* - +/-*
USTEKINUMAB + + + - + + + + - ?+/-* ?/+*
SECUKINUMAB + + ? +/- + + + X ?/+* ?+* ?/+*
IXEKIZUMAB + + ? +/- + + + X ?/+* ?+* ?/+*
BRODALUMAB + + ? +/- + + + X ?/+* ?+* ?/+*
GUSELKUMAB + + ? +/- + + + + ? ? ?
TILDRAKIZUMAB ? ?/+ ? +/- + + + + ? ? ?
RISANKIZUMAB ? ?/+ ? +/- + + + + ? ? ?
MIRIKIZUMAB ? ?/+ ? +/- + + + + ? ? ?
APREMILAST ? + ? +/- + + + + ?/+* ? ?
METHOTREXATE + X + - + + + + X X X
CYCLOSPORINE +/- + ?/- X + +/- + + +/-* X X
ACITRETIN +/- + ?/- +
+ + + ? X + + +

Which of the following treatments would be
ideal for a patient with severe psoriasis,
multiple sclerosis and Crohn disease?
A) Certolizumab
B) Brodalumab
C) Acitretin
D) Infliximab
E) Ustekinumab

Reasons to Become a Registry Investigator
• Contribute to education/clinical knowledge of the psoriasis
community
• Opportunity to establish a database of your patient population
• Academic recognition and publication opportunities
• Supplement existing insurance fee schedules
– Site compensation is $525 (including $25 for patient) per Enrollment
visit and $350 (including $25 for patient) per biannual Follow Up visit

If you are interested in participating in the Psoriasis
Registry as a research investigator, please email
or visit www.corrona.org
or call 508.408.5432
Become a Registry Research Investigator






![S026 表2・3 [更新済み]kksanko.com/merchandice_info/up_pdf/1406032449-120356.pdfTitle S026 表2・3 [更新済み] Author M'sクリエイト 倉重 Created Date 4/22/2014 12:19:25](https://img.pdfslide.net/doc/110x75/60ca59b48d4016427603fba7/s026-e2f3-title-s026-e2f3-author-msff.jpg)