Embed Size (px)
Citation preview

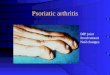
PsoriaticArthritisLAURIE HUGHELL, MSPA-C, MPHIOWA ARTHRITIS & OSTEOPOROSIS CENTER

Seronegative Spondyloarthropathies
uPsoriatic Arthritis
u Ankylosing Spondylitis
u Reactive Arthritis
u Enteropathic ArthritisuCrohn’s DiseaseuUlcerative Colitis

SeronegativeSpondyloarthropathiesu Propensity for axial arthritis
u Sacroiliitis and spondylitis
u Peripheral arthritis
u Enthesitis – inflammation of tendons, ligaments or fascial insertions
u Familial pattern with HLA-B27 associationu Positive result is a 20 fold increased risk of developing
a spondyloarthropathy

Psoriatic Arthritis (PsA)

Psoriatic Arthritis (PsA)u Inflammatory arthritis associated with psoriasis
u Nail changes can be present
u Originally considered a variant of rheumatoid arthritis
u Seronegativity of rheumatoid factor (RF) was an original requirement but no longer
u 10% of patients with psoriasis have a + RF

Pathogenesis of PsAu Genetic factors:
u 40% of patients with psoriasis or PsA have a family history of these disorders
u PsA is 55 times more likely to occur among first-degree relatives
u Paternal transmission bias for psoriasis and PsA has been found

Pathogenesis of PsA
u Environmental factors:u Infections – association with streptococcal infection has been
proposedu One study showed improvement in psoriasis after having
tonsillectomyu Trauma
u Koebner phenomenon – psoriasis forms at sites of traumau Emotional stress
u Obesity – risk factor for psoriasis

Epidemiology of PsA
u Affects men and women equally
u Age of onset usually 30-55 years
u 1-2 per 1000 in the general population

PsA & Psoriasisu PsA prevalence estimates are 4-30% of patients with psoriasis
u Skin involvement precedes joint involvement in the majority of patients
u Study showed psoriasis patients more likely to develop PsA:u Higher skin burdenu nail lesionsu scalp and intergluteal lesions
u Weak relationship between the severity of skin disease and arthritic involvement

Differential Diagnosis
u Rheumatoid Arthritisu Reactive Arthritisu Arthritis of inflammatory bowel disease (enteropathic
arthritis)u Ankylosing Spondylitisu Goutu Osteoarthritis


Psoriasis
Copyright ACR

Psoriasis
Copyright ACR

PsA: Presentation


PsA: Cardinal Findings
} Spinal stiffness, pain or limited range of motion
} Asymmetric peripheral joint stiffness, pain and swelling
} Dactylitis◦ “sausage”-like swelling of the fingers or toes◦ Uniform swelling of the soft tissues between the MCP and interphalangeal
joints such that there is diffuse swelling of the digits◦ Occur in ½ of PsA patients and are associated with an increased risk of
progressive radiographic damage

Dactylitis

Copyright ACR

PsA: Cardinal Findings
} Enthesitis
} Inflammation of the tendons, ligaments and synovium into bone
} Achilles tendon, plantar fascia & the pelvic bones are most common areas
} Tenosynovitis
} May involve flexor tendons of the hands

Achilles tendonitis
Copyright ACR

PsA: Cardinal Findings
} Pitting Edema} Swelling of the hands or feet
} Often asymmetrical and occasionally precedes joint involvement
} Ocular inflammation} Conjunctivitis present in 20% of PsA patients} Uveitis in 7% of PsA patients

PsA: Pitting Edema

PsA: Nail Changes
u Nail lesions occur in 80-90% of patients compared vs. 46% of those with psoriasis
u Pits – depressions in the nail plateu Usually occur in large numbers and involve several nails
u Onycholysisu Separation of the nail from its bed
u Can be difficult to distinguish from Onychomycosis (fungal infection) –should send nail scrapings for fungal culture
u Severity of nail involvement may correlate with the severity of both skin and joint diseaseu Most common in patients with DIP arthritis

Nail pitting

Onycholysis

Onycholysis
Copyright: ACR




PsA: CASPAR Classification Criteriau Skin psoriasis
u Present – 2 points
u Previous history – 1 point
u Family history – 1 point
u Nail lesions – 1 point
u Dactylitis – 1 point
u Negative rheumatoid factor – 1 point
u X-rays changes – 1 point
3+ points makes the diagnosis of PsA

PsA: Comorbidities
u Risk of cardiovascular disease is increased in patients with PsA, especially those not on treatment
u Psoriasis associated with:u Metabolic syndrome
u Hypertension
u Diabetes
u Atherosclerosis
u Malignancy
u Hepatic and pulmonary disorders
u Psychiatric disease (depression & Anxiety)

PsA: Diagnostic Testing

PsA: Laboratory
u Lab findings in PsA are nonspecific
u Rheumatoid factor – in 2-10% of patients with PsA
u ANA – found at low titer (less than 1:40) in ~50% of patients
u Anti-cyclic citrullinated peptide (Anti-CCP) found in 8-16% of patients with PsA
u HLA-B27 –genetic marker that may indicate higher risk of developing PsA
u Acute Phase reactants elevated in 40% of patientsu C-reactive protein and Erythrocyte sedimentation rate

PsA: Imaging
u Unique in inflammatory arthritisu erosive changes & new bone formation occur in the same joint or same
digit
u “pencil and cup” deformity results from erosive changes and formation of hypertrophic bone in the phalanges
u Presence of early radiologic changes in course of PsA suggest aggressive disease
u MRI can be used to look for sacroiliitis u Correlates with decreased spinal mobility and longer duration of
disease



Arthritis Mutilans
Copyright ACR

PsA: Treatment Options

PsA Treatment Options
u Physical Therapyu Occupational Therapyu Weight reductionu Exerciseu Patient Educationu Medications
u DMARDS
u Biologics

PsA Treatment - NSAIDs
} NSAIDs } May be helpful for inflammatory back pain & peripheral joint pain
} OTC vs. Prescription} Ibuprofen, naproxen sodium, etodolac, nabumetone, meloxicam, etc.
} Cox 2 Inhibitor – celecoxib may be better tolerated from GI standpoint
} Side effects:
} Renal insufficiency, GI ulceration, cardiovascular disease

PsA Treatment - Corticosteroids} Corticosteroids◦ Use of oral, low-dose prednisone should be reserved
for severe, peripheral arthritis
◦ Use caution when prescribing high dose steroids◦ Withdrawal of oral steroids may cause worsening of
psoriasis
◦ Corticosteroid joint injections can reduce swelling/pain of single joint◦ Avoid injecting directly into a psoriasis plaque

PsA Treatment - DMARDs
u Disease modifying anti-rheumatic drugs (DMARDs)
u May be used for peripheral arthritis
u May continue NSAIDs as “bridging therapy” until DMARD becomes effective
u Commonly used DMARDs
u Methotrexate
u Leflunomide
u Sulfasalazineu Cyclosporineu Azathioprine

PsA: DMARDsu METHOTREXATE
u 2.5 mg tablets
u 2-10 tablets (5-25 mg) once weekly
u 25 mg/mlu 0.5 – 1.0 cc once weekly
u Side effects: Hepatoxicity, pancytopenia, oral ulcers, GI upset, nausea
u Gold standard treatment
u Patients take folic acid(800-2,000 mcg) daily
u LEFLUNOMIDEu Dosing 10-20 mg once daily
u Side effects: Hepatoxicity, pancytopenia, GI upset, nausea
u Loading dose is 100 mg daily x 5 days
u Can cause vomiting and diarrhea

Otezla (Apremilast)
u 30 mg twice dailyu Starter titration pack
u Has not been shown to stop radiographic changes of erosionu Excellent safety profile so good for those with comorbiditiesu Potential side effects: Unexplained weight loss, depression

Biologics: TNF Inhibitors
TNF Inhibitors:} Have shown excellent
efficacy in treating skin disease as well as joint disease and preventing x-ray erosions
} FDA Black Box Warnings:} Opportunistic
infections including tuberculosis, histoplasmosis, etc.
} Malignancy risk is slightly increased for lung cancer, skin cancer, lymphoma

Biologics: TNF Inhibitors
u Enbrel (etanercept)u 50 mg SC once weekly
u Cimzia (certolizumab)u 400 mg SC once monthly
u Simponi (golimumab)u 50 mg SC monthly
u Humira (adalimumab)u 40 mg SC every other week
u Remicade (infliximab)
u 5 mg/kg at weeks 0, 2 and 8 weeks then 5 mg/kg every 8 weeks
u Biosimilar TNF Inhibitors for Infliximab:u Inflectrau Renflexis

Other Biologicsu Stelara (ustekinumab)
u Human interleukin 12 and 23 antagonist
u Initial is week 0 and 4 thenu Injectable q 3 months
u Abatacept (Orencia)u T-cell modulatoru FDA approved for PsA in
2017u IV or Injectable q month
u Cosentyx (secukinumab)u Human interleukin-17A
antagonist u Injectable q monthu Titration dose at weeks 0,
1, 2, 3 & 4
u Taltz (ixekizumab)u Human Interleukin-17
antagonistu Injectable q month

Oral Biologic
u Tofacitinib (Xeljanz, Xeljanz XR)
u Oral inhibitor or Janus Kinase (JAK)u FDA approved for PsA in patients with inadequate
response or intolerance to Methotrexate

PsA: Prognosisu Risk factors for progressive joint damage/ poor prognosis:
u Increased numbers of actively inflamed joints
u Elevated CRP or ESR (sed rate)
u Failure of previous medication trials
u Presence of joint damage (clinically or radiographically)
u Loss of function (by Health Assessment Questionnaire)
u Diminished quality of life

Health Assessment Questionnaire