Embed Size (px)
Citation preview

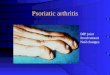
Psoriatic ArthritisBY
EMMANUEL EZRA ABIGROUP 3

Definition
Inflammatory arthritis associated with psoriasisUsually seronegative for Rheumatoid Factor and cyclic citrullinated peptides (CCP)Classified with HLA-B27-associated spondyloarthropathies

Epidemiology
Likely in up to 25-34% of patients with presence of skin diseaseOverall prevalence 0.04-1.2%M=F although it differs in subsetsPeak age of onset between 30-55 years

CASPAR criteriaevidence of psoriasis
current - 2history of - 1family history of - 1
psoriatic nail dystrophy (onycholysis, pitting, hyperkeratosis)negative rheumatoid factordactylitis, either current or history ofradiological evidence of juxta-articular new bone formation

SubtypesDIP joint patternoligoarticular (<5 joints) pattern, usually assymetricpolyarticular (>=5 joints), symmetric in halfarthritis mutilansspondyloarthritis

Other Rheum Findings
enthesitis (inflammation at site of tendon insertion)tenosynovitis (inflammation of tendon and its enveloping sheath)dactylitis or “sausage digit”

Extra-articular findings
skin - psoriasisnails - pits and onycholysispitting edema - often asymmetricalocular inflammation - conjunctivitis, iritis

look for distal joint involvement in asymmetric distributionlook at the nailslook in earsask about family historydactylitis
How to diagnose those without skin
findings

Images

Diagnostic Testingno diagnostic laboratory testingradiologically:
erosive changes and new bone formation in distal jointslysis of terminal phalangesfluffy periostitis and new bone formation at sites of enthesitis“pencil in cup” appearance

Differential
Reactive (Reiter’s) ArthritisRheumatoid Arthritis with concomitant psoriasisankylosing spondylitisgouty arthritis

TreatmentNSAIDs if disease is mild.PT, OT, splinting devicesIf erosive disease, treat aggressively with DMARDs (MTX, Sulfasalazine, CsA).If skin disease is the major issue, should be managed by a dermatologist.Early referral to rheumatology for initiation of DMARDs to prevent progression.

Course and Prognosis20% of patients have a severe an debilitating form of arthritisoriginally thought to be more benign course than RhAprogression of clinical damage occurs in a majority of patientsradiologic changes occur over time despite treatment