Embed Size (px)
Citation preview

7/27/2019 Psycho-Oncology 2010 Bonnaud_Videotaped Simulated Interviews to Improve Medical Students' Skills in Disclosing a Diagnosis of Cancer
http://slidepdf.com/reader/full/psycho-oncology-2010-bonnaudvideotaped-simulated-interviews-to-improve-medical 1/7
Psycho-Oncology
Psycho-Oncology 19: 975–981 (2010)
Published online 13 November 2009 in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/pon.1649
Videotaped simulated interviews to improve medicalstudents’ skills in disclosing a diagnosis of cancer
Ange lique Bonnaud-Antignac1,2, Loıc Campion3,4, Pierre Pottier 1 and Ste phane Supiot1,5Ã
1University of Nantes, Faculty of Medicine, Nantes, France2CHU Nantes, Department of Medical Oncology, Nantes-St-Herblain, France3Department of Statistics (LC), Nantes-St-Herblain, France4INSERM U892, Centre de Recherche en Cance rologie Nantes-Angers, CHU Nantes, Nantes, France5Centre Rene Gauducheau, Department of Radiation Oncology, Nantes-St-Herblain, France
Abstract
Objective: To assess the performance of the training course on the disclosure of a diagnosis of
cancer intended for fifth year medical students of the University of Nantes.
Methods: The course comprised three sessions: (1) a group discussion that taught a six-point
protocol (SPIKES) for delivering a diagnosis, (2) a videotaped simulated interview to assessprotocol implementation and communication skills, and (3) feedback from a senior physician.
The learning objectives were memorisation and implementation of the protocol, use of
appropriate communication techniques to deal with the patient’s response, and identifying one’s
own reactions in a stressful situation. Two types of assessments were performed before and
after each session: self-assessments by the students and a quantitative and qualitative external
assessment by a psychologist and senior physician. In addition, recall of the six-point protocol
was assessed during the end-of-the-year examination.
Results: Overall, 108 students took part in the course during the 2004–2005 academic year.
They felt that their competence improved after each session in terms of the three learning
objectives. However, recall of the six-point protocol was inadequate. It was best among
students who considered they had progressed most.
Conclusions: Our training course on communication techniques helps students acquire confidence
in their skills in breaking bad news by backing theory with practice and feedback. The students
make progress despite the psychological stress generated by simulated real-life conditions.Copyrightr 2009 John Wiley & Sons, Ltd.
Keywords: cancer; diagnosis; medical students; simulated interviews; feedback; oncology
Introduction
A doctor’s disclosure of a diagnosis of cancershould occur within the context of a good patient-doctor relationship. However, despite the efforts
made by both patients and doctors, the commu-nication process can fall short of expectations(reviewed in [1]). The bearer of the bad news isusually a general practitioner or a consultant‘organ’ physician rather than an oncologist. Forthese doctors who do not often manage cancerpatients, and in particular, for the youngestamongst them, a disclosure of cancer or of acancer-related complication may be a difficultchallenge. A general framework for breaking badnews has been proposed by the World HealthOrganization (WHO). It stipulates that the amountand type of information delivered should meet the
individual patient’s expectations [2]. Both patientsand medical students prefer such a patient-centredapproach to non-disclosure or full disclosure [3,4].
Over the years, however, the part devolved tohumanities (patients’ views and affective compo-nents) and communication techniques in medicalschool curricula has been increasingly overpoweredby biomedical subjects, despite efforts to drawattention to the communication aspects of medicalstudies [5–8]. Available studies show that severalsessions, accompanied by demonstrations, discus-sions, practice, and feedback, are needed to teachskills for delivering bad news (reviewed in [9]). Forthese reasons, the Faculty of Medicine of NantesUniversity (France) decided to offer a course onhow to disclose a diagnosis of cancer to pre-residency medical students in order that they mightacquire the communication skills needed on thewards [10].
A pilot study on a planned training course wasundertaken during the academic year 2003-2004
[11]. Its aims were to teach students the theoryneeded to cope with real-life situations and toenhance their understanding of the psychological
* Correspondence to: Servicede Radiothe rapie, CentreRene Gauducheau, 44800Nantes St-Herblain, France.E-mail: s-supiot@nantes.
fnclcc.fr
Received: 5 January 2009Revised: 14 September 2009
Accepted: 14 September 2009
Copyrightr 2009 John Wiley & Sons, Ltd.

7/27/2019 Psycho-Oncology 2010 Bonnaud_Videotaped Simulated Interviews to Improve Medical Students' Skills in Disclosing a Diagnosis of Cancer
http://slidepdf.com/reader/full/psycho-oncology-2010-bonnaudvideotaped-simulated-interviews-to-improve-medical 2/7
dimensions of these situations. Because medicalstudies are based on both theory and practicaltraining, the course comprised three different typesof session: (1) a group discussion on communica-tion techniques that introduced the well-known six-point Buckman protocol for breaking bad news
[12], (2) a videotaped simulated interview to assessthe student’s ability to implement this protocol aswell as their communication skills, and (3) feed-back on the student’s performance from a psychol-ogist and senior physician. Simulated interviewsare a valid method for judging how a physicianmight perform on the ward and a more ethicalapproach than plunging novices directly into real-life situations [13–17].
As our pilot study had demonstrated thefeasibility of our training course and its utility inhelping students memorise the six-point protocol
[11], we decided the following academic year toextend the course to all medical students duringtheir mandatory clerkship in an oncology depart-ment. We hypothesized that each of the threesessions would improve the students’ confidenceand competence in breaking bad news and helpthem memorise the six-point protocol. We, thus,assessed the performance of each individual sessionand analysed the students’ knowledge of breakingbad news at the end-of-the-year oncology exam-ination.
Method
Description of the course
Medical students in France complete a six-yearcurriculum before becoming residents: the first twoyears (Premier Cycle d’Etudes Me ´ dicales, PCEM1–2) are generally devoted to pre-clinical studies; thenext four years (Deuxie ´ me Cycle d’Etudes Me ´ di-cales, DCEM 1–4) are essentially clinical clerkshipyears. First- to third-year students at our medicalschool attend a programme on communication,
psychology, and medical ethics focusing on thedoctor-patient relationship [5]. Our training courseon breaking bad news took place during thestudents’ clerkship in oncology (fifth year).
We have described the course in detail in ourpilot study [11]. Session 1 was a lecture anddiscussion on suitable communication techniquesderived from French and International references[18–20] during which a well-known six-pointstepwise protocol for delivering bad news (knownas SPIKES) was presented [12,21]. The six pointsare: (1) S for setting (welcome the patient); (2) P for
perception (find out what the patient alreadyknows); (3) I for invitation (ask what the patientwants to know); (4) K for knowledge (inform thepatient about his or her disease); (5) E forexploring/empathy (respond empathically to the
patient’s reaction to the news); and (6) S forstrategy/summary (conclude and propose a treat-ment plan) [12].
Session 2 took place 1–8 weeks later. It was avideotaped simulated patient (actor)-doctor (stu-dent) interview during which students attempted to
implement the six-point protocol and the commu-nication techniques they had just learnt. No medicalknowledge beyond that acquired by a junior medicalstudent was needed. The doctor was considered tohave had no prior contact with the patient, as is thecase during a clerkship. A variety of situations werecovered: breaking the news of a disease for the firsttime, informing the patient of local recurrence ormetastatic spread, or announcing the need forradical ablative surgery. The patients were playedby professional actors. The actors were given thescenario, directions on how to play their part, and
were told of the self-protection mechanisms some-times used by healthcare professionals and patients,such as denial, belittlement, and avoidance [22].During the simulated interview, a psychologistassessed the students’ ability to implement theprotocol and to use appropriate communicationtechniques by completing a form derived from thesix-point protocol [11,12]. He or she analysed thecommunication techniques used by the student(active listening, type of questions asked, rephrasing,silence, etc.) and whether the right technique wasapplied at the right time. At the end of the interview,the problems encountered by the student werediscussed. The psychologist’s assessment form andcomments were handed to the senior physicianbefore session 3.
Session 3 was an individual feedback sessionwith a senior physician and took place 1–2 weekslater. The physician watched the video of theinterview with the student, emphasized the six stepsof the protocol, and described the techniques andskills he or she considered best suited to the fakecase and to similar real-life situations. Twentysenior physicians took part in session 3.
Session 1 was mandatory but student participa-
tion in sessions 2 and 3 was voluntary.
Assessment of learning objectives
The students had to memorise and implement thesix-point protocol for breaking bad news, imple-ment appropriate communication techniques inresponse to the patient’s response, and understandtheir own reactions to a stressful situation. Both self-assessment and external assessment by the psychol-ogist, senior physician, and Faculty were used tofind out whether the objectives had been met.
Self-assessment
To determine the student’s self assessment of learning objectives, we used two methods: (1)
Copyrightr 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 975–981 (2010)
DOI: 10.1002/pon
976 A. Bonnaud-Antignac et al.

7/27/2019 Psycho-Oncology 2010 Bonnaud_Videotaped Simulated Interviews to Improve Medical Students' Skills in Disclosing a Diagnosis of Cancer
http://slidepdf.com/reader/full/psycho-oncology-2010-bonnaudvideotaped-simulated-interviews-to-improve-medical 3/7
appreciation of the value of each session with directquestions and (2) self-assessment before and aftereach session on a ten-point Likert scale.
(1) Students had to complete a three-item ques-tionnaire after each session: Had the sessionhelped them understand the value of the six-point protocol, of communication techniques,and of self-knowledge? Each question had aclosed response (yes, I noticed an improve-ment; no, I did not notice an improvement;I do not know) and an open response (why?).Open responses were analysed using a ‘key-words in context’ method [23], by groupingwords occurring frequently into a limitednumber of categories.
(2) Students also rated their ability to break badnews, implement communication techniques,
and identify their own reactions on a ten-point Likert scale, before the start of thecourse and after each session. Improvementwas defined by an increase in their self-ratedlevels.
External assessment
The psychologist and senior physician assessedwhether the students had implemented the SPIKESprotocol whilst the interview took place and duringthe feedback session. The assessment grid wasderived from the items of the SPIKES protocol(getting the setting right, finding out what thepatient knows already, finding out what the patientwants to know, giving information, responding tothe patient’s reactions, treatment plan, and follow-up) [11]. A further external assessment was doneduring the end-of-the-year oncology examination(June 2005) asking a compulsory question: whatare the steps in breaking the news of a seriousdisease? Students’ answers were analysed bysearching for words or groups of words relatingto the six-point protocol. Recall of the SPIKES
protocol was assessed according to the number of exact items at the end-of-the-year examination.
Statistical analysis
To analyse trends in self-assessed competence levelsafter each session, we used Spearman’s correlationtest between number of sessions and students’ self-assessed competence score. To confirm the trends,we compared self-assessed competence levels beforeand after each step by using paired student T test.To assess for a correlation between self-assessed
competence levels and students characteristics, weused ANOVA tests for repeated measures. We usedFisher Exact test or Pearson’s Chi square test tocompare results at the end-of-the-year examinationand students’ characteristics.
Results
Students’ characteristics
All fifth year medical students in the academic year2004–2005 (n5 108; 69% female, 31% male)
attended the training course during their two-month clerkship in oncology. There were fourconsecutive clerkships during the year, that is, fourgroups of 25–30 students. One student refused toparticipate in session 2 for personal reasons. Theclinical scenarios were classified as either difficult(64%) and related to life-threatening cancer with ashort life expectancy (e.g. metastatic disease orunresectable locally advanced tumours) or lessdifficult (36%), that is, curable cases. Moststudents (77%) were allocated a scenario that theymight encounter on the wards (e.g. diagnosis of leukaemia during a haematology clerkship).
Self-assessment of skills
Assessment of the value of the sessions
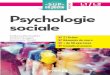
The closed questions on the value of each sessionwere completed by 82, 68, and 83 of the 108students for sessions 1 (theory), 2 (simulatedinterview), and 3 (feedback), respectively. Moststudents reported improved knowledge of how tobreak bad news (i.e. of the six-point protocol) aftersession 1. Half of them experienced no furtherimprovement in knowledge immediately aftersession 2. However, the feedback given in session 3boosted their confidence in having the requiredknowledge (Figure 1(A)). Only half of the studentsfelt that their skills in communication techniqueshad improved after sessions 1 and 2, but 77% feltmore comfortable with these techniques aftersession 3 (feedback) (Figure 1(B)). About 70% of the students felt they understood their ownreactions better after each session (Figure 1(C)).
When the students were asked to defend theresponses they had given to the closed questions onthe value of each session, they gave the following
explanations: They saw session 1 as a preparatorystep to the framework underlying the simulatedinterview. They regretted that only theory and notpractice had been used to teach communicationtechniques. They insisted that practice was requiredin order to be able to grasp the problems of breaking bad news and in order to improve skills.They were rather self-critical about their ownperformance in session 2. They found it difficultto lead up to the question of ‘asking what thepatients wants to know’ and also found it difficultto ‘respond empathically to the patient’s reaction
to the news’, especially if the patient’s reaction wasunexpected. They found it hard to make a consciouseffort to implement the communication techniquesthey had been taught and to master nonverbalcommunication. The simulated interview had
Simulated interviews for learning to break bad news in oncology 977
Copyrightr 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 975–981 (2010)
DOI: 10.1002/pon

7/27/2019 Psycho-Oncology 2010 Bonnaud_Videotaped Simulated Interviews to Improve Medical Students' Skills in Disclosing a Diagnosis of Cancer
http://slidepdf.com/reader/full/psycho-oncology-2010-bonnaudvideotaped-simulated-interviews-to-improve-medical 4/7
unveiled their spontaneous verbal and nonverbalreactions and made them realise the uniqueness of each situation and the need to adapt. The psychol-ogist had helped them gain awareness of how self-protective they were. In their opinion, the simulatedinterview introduced a bias that needed to beremedied by facing a real-life situation. They feltthat the feedback from an experienced physician insession 3 helped them come to terms with their ownself-criticisms, understand how important it is tobreak bad news stepwise, and recognise their ownverbal and nonverbal inadequacies.
Self-rating of skills
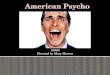
The ten-point Likert scale rating of the value of eachsession was completed by 90, 83, 59, and 76 of the108 students before session 1 and after sessions 1, 2and 3, respectively. Thirty-five students completedall three questionnaires. The students consideredthat their ability had improved on all three counts:
breaking the news (R51
0.558, P Spearma-no0.001), using appropriate communication tech-niques (R510.469, P Spearmano0.001), andunderstanding their own reactions (R510.385, PSpearmano0.001) (Figure 2). The rating for how to
break the news improved two-fold after the course(significant increase— po0.001—following each stepof the course), with the most marked increasesoccurring after sessions 1 and 2. The rating forability to implement communication techniques rose1.7-fold (significant increase—po0.05—followingeach step of the course), with a moderate rise aftereach session. Self-understanding improved 1.4-fold,with no significant increase following session 1, butwith a high increase after the simulated interview( po0.001), and little but significant change aftersession 3 ( p50.003). There was no difference inrating between male and female students, betweendifficult or less difficult scenarios, and according towhether the student had or had not experienced asimilar situation during their clerkship.
External assessment of skills
According to the psychologist’s assessment of thecorrect use of the six-point protocol for breaking
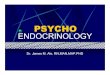
bad news during the simulated interview, moststudents were able to welcome the patient, get toknow what the patient already knew abouttheir disease, provide information, and conclude(Figure 3(A)). However, the psychologist considered
Figure 1. Students’ self-evaluation of curricular objectives by answering to the question ‘Has this session helped you understand the
value of (A) the 6-point protocol, (B) communication techniques, (C) knowing your own reactions? (Step 1: After the theoreticalsession; Step 2: after the simulated interview; and Step 3: after feedback)
978 A. Bonnaud-Antignac et al.
Copyrightr 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 975–981 (2010)
DOI: 10.1002/pon

7/27/2019 Psycho-Oncology 2010 Bonnaud_Videotaped Simulated Interviews to Improve Medical Students' Skills in Disclosing a Diagnosis of Cancer
http://slidepdf.com/reader/full/psycho-oncology-2010-bonnaudvideotaped-simulated-interviews-to-improve-medical 5/7
that only few students were able to take into accountwhat the patient wanted to know and that morethan 30% of the students experienced difficulty inadjusting to the patient’s reactions.
At the end-of-the-year examination, two-thirdsof the students had memorised the following points:(1) welcoming the patient, (4) informing the patientabout their disease, (5) responding empathically tothe patient’s reaction to the news, and (6) conclud-ing and proposing a treatment plan (Figure 3(B)).However, less than half of the students correctlyrecalled the need to (2) find out what the patient
already knows and (3) ask what he or she wants toknow.
Female students were more likely to rememberthe six steps of the protocol than male students(mean number of steps 4.6 vs 3.8, p5 0.011)especially step (1) (85.1 vs 67.7%, p5 0.036), step(2) (62.2 vs 41.2%, p5 0.042), and step (5) (75.7vs50%, p5 0.008). Recall was not significantlybetter if the students had to deal with a difficultscenario or a situation already encountered duringtheir clerkship. The students who considered thatthey had made considerable progress during the
Figure 2. Mean Likert scores for self-assessed competence in breaking bad news, using communication techniques, and self-knowledge. (0: baseline; Step 1: after the theoretical session; Step 2: after the simulated interview; and Step 3: after feedback)
Figure 3. (A) Psychologist’s assessment of the implementation of the six-point protocol during the simulated interview. (B) End-of-the-year faculty assessment of knowledge of the six-point protocol
Simulated interviews for learning to break bad news in oncology 979
Copyrightr 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 975–981 (2010)
DOI: 10.1002/pon

7/27/2019 Psycho-Oncology 2010 Bonnaud_Videotaped Simulated Interviews to Improve Medical Students' Skills in Disclosing a Diagnosis of Cancer
http://slidepdf.com/reader/full/psycho-oncology-2010-bonnaudvideotaped-simulated-interviews-to-improve-medical 6/7
course recalled more of the steps of the six-pointprotocol than others ( po0.001).
Discussion
Each of the three sessions of our course improvedthe students’ confidence in their skills with regardto the three objectives we had set: (1) implementingand memorising the six-item protocol for breakingbad news, (2) improving their ability to useappropriate communication techniques, and (3)helping them identify their own reactions whenbreaking bad news.
Several studies have highlighted the advantagesof a course in breaking bad news using videotapepresentations and actors to play patients [24,25].Simulated interviews are now used in many
countries but have not yet been used for initialtraining in France [26,27]. Their ability to improvestudents’ skills in breaking bad news has beeninvestigated [14–17]. However, our study is differ-ent in that it focused on the assessment of each stepof a three-pronged course, and has shown the neednot only for a simulated interview but for a theoryclass and for individual feedback. Each componentof the course was important and tended to developdifferent skills. The theory class provided knowl-edge on how to break bad news. The videotapedsimulated interviews boosted the students’ self-confidence in having the required knowledge.Feedback on attitudes, behaviour, and use of skillsfrom the psychologist [28], and especially from thesenior clinician, increased their understanding of the protocol and their awareness of the importanceof communication techniques. Our study, thus,strongly suggests that formal university training onhow to break bad news should include multiplesessions and opportunities for demonstration,reflection, discussion, practice, and feedback [9].
The six-point protocol proposed by Buckman[12] was not that easy to implement and memoriseby students. Although most managed to ‘find out
what the patient knows’ during the simulatedinterview, many omitted to mention the itemduring the end-of-the-year examination. This wasa rather disappointing result as our pilot study hadindicated that course participants were less likely toforget steps than other students [11]; the students inthis study may have been less motivated than thosein the pilot study. In general, the students with thebest recall were those who felt that they hadprogressed most and were probably the mostmotivated. Female students recalled the six stepsof the protocol better than male students, and may
have a greater aptitude for general learning or agreater interest in communication [29]; a point thatmay have affected the students’ performance is theabsence of a mnemonic for the six-point protocolin French (SPIKES in English).
The students’ understanding of the use of appropriate communication techniques progressedafter each session, although their appreciation of their true value was greatest after feedback fromthe psychologist and physician, once they hadapplied the techniques during the simulated inter-
view. According to the results of the self-assess-ment questionnaire, each session improved thestudents’ understanding of their own reactionswhen breaking bad news. However, according totheir Likert rating, it was the simulated interviewthat helped them most, probably, in part, thanks toearly feedback from the psychologist. Other teamshave also noted improvements in the self-perceivedcommunication skills of medical or nursing stu-dents and oncology fellows after training, inparticular after simulated interviews [30,31].
Our study has several limitations that need to be
addressed in future studies. First, we used a non-validated questionnaire comprising a restrictednumber of items based on the SPIKES protocol[11] for the psychologist’s assessment of studentperformance during the simulated interview. How-ever, a validated questionnaire needs to be devel-oped. Second, because of the large number of students doing their clerkship in different hospitals,we were unable to obtain all students’ ten-pointLikert rating. This may affect the statisticalsignificance of our results. Third, we have nolong-term follow-up data. Medical students whounderstand ethical issues, gain self-knowledgeabout relationships, and feel more confident inbreaking bad news may not necessarily use appro-priate communication techniques once they havequalified. Further studies on our cohort will helpdetermine the impact of simulated interviews onresidents’ competencies. Fourth, a bias in our studyis the nature of the assessor. Communication skillswere assessed by the psychologist, the studentsthemselves, and by the physician, but not by theone person truly concerned, the patient. In future,cancer patients could be called upon to rate theinterpersonal and communication skills of medical
students [32].Interestingly, students who considered they had
made progress during the course recalled more of the steps of the six-point protocol at the end-of-the-year examination. One possible explanation is thatstudents who make progress may believe thatcommunication with patients may be controlledby physicians themselves and, therefore, benefitmore from educational interventions. These para-meters will have to be analysed using validatedquestionnaires in further studies of our cohort. Thechallenge is now to improve the competencies of
less motivated students.In conclusion, although each session improvedthe students’ feeling of competence, the studentsdid not actually develop perfect recall of the sixsteps of the protocol even though this protocol was
980 A. Bonnaud-Antignac et al.
Copyrightr 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 975–981 (2010)
DOI: 10.1002/pon

7/27/2019 Psycho-Oncology 2010 Bonnaud_Videotaped Simulated Interviews to Improve Medical Students' Skills in Disclosing a Diagnosis of Cancer
http://slidepdf.com/reader/full/psycho-oncology-2010-bonnaudvideotaped-simulated-interviews-to-improve-medical 7/7
taught using a highly practical approach. Thepractical approach was welcomed by the studentsdespite the stress generated by a situation simulat-ing real life. This three-steps training course on thedisclosure of a diagnosis of cancer is still ongoingat the University of Nantes.
Acknowledgements
The authors wish to thank all who took part in the trainingsessions: psychologists (Elisabeth Jegaden, Jean-Charles LeDrezen, Myriam Auger), physicians (Ve ´ ronique Barbarot,Emmanuelle Bourbouloux, He ´ le ` ne Se ´ nellart, Ste ´ phanieBordenave, Christine Digabel, Jaafar Bennouna, DominiqueBerton-Rigaud, Gaelle Quereux, Sonia Marques, Jean-MarcClasse, Vale ´ rie Delecroix, Isabelle Doutriaux, Magali Le-blanc, Gaelle Brocard, Tyffen L’Haridon, Thierry Chatellier,Maud Aumont-Le Guilcher, Franc-ois Thillays, Fre ´ de ´ ricRolland), and actors (Ligue d’Improvisation de Nantes-Atlantique), as well as all those who provided support (Dr J-
Y Ge ´ not, Centre Franc-
ois Baclesse, Caen, Professors AlainMouzard and Jean-Michel Rogez, Faculte ´ de Me ´ decine deNantes).Sponsors:
Fonds de Recherche du Centre Rene ´ Gauducheau(Professor Franc-ois-Re ´ gis Bataille), Ligue De ´ partementaleContre le Cancer de Loire-Atlantique, and the FrenchMinistry of Health (Fonds National de Pre ´ vention, d’Edu-cation et d’Information Sanitaires)
References
1. Hack TF, Degner LF, Parker PA. The communication
goals and needs of cancer patients: a review. Psycho-Oncology 2005;14(10):831–845; discussion 46–47.
2. Donovan K. Communicating bad news. Division of Mental Health, World Health Organization. 1993;http://whqlibdoc.who.int/hq/1993/WHO_MNH_PSF_ 93.2.B.pdf.
3. De Valck C, Bensing J, Bruynooghe R. Medicalstudents’ attitudes towards breaking bad news: anempirical test of the World Health Organization model.Psycho-Oncology 2001;10(5):398–409.
4. Dowsett SM, Saul JL, Butow PN et al . Communicationstyles in the cancer consultation: preferences for apatient-centred approach. Psycho-Oncology 2000;9(2):147–156.
5. Bonnaud A, Pottier P, Barrier JH et al . E ´ valuation del’enseignement de la relation me ´ decin-patient aupre ` s dese ´ tudiants de deuxie ` me et troisie ` me anne ´ e de me ´ decine a `la faculte ´ de me ´ decine de Nantes. Pe dagogie Me dicale2004;5(3):159–166.
6. Rosenthal F, Ogden F. Changes in medical education:the beliefs of medical students. Med Educ 1998;32(2):127–132.
7. Powell A, Boakes J, Slater P. What motivates medicalstudents: how they see themselves and their profession.Med Educ 1987;21(3):176–182.
8. Wolf TM, Balson PM, Faucett JM, Randall HM.A retrospective study of attitude change during medicaleducation. Med Educ 1989;23(1):19–23.
9. Rosenbaum ME, Ferguson KJ, Lobas JG. Teachingmedical students and residents skills for delivering badnews: a review of strategies. Acad Med 2004;79(2):107–117.
10. Bonnaud-Antignac A. L’enseignement de la psychologieen me decine. Les Belles Lettres: 2007.
11. Supiot S, Bonnaud-Antignac A. Using simulated inter-views to teach junior medical students to disclose thediagnosis of cancer. J Cancer Educ 2008;23(2):102–107.
12. Buckman R. How to Break Bad News, a Guide forHealth Care Professional . Universiy of Toronto Press:
Toronto, 1992.13. Yedidia MJ, Gillespie CC, Kachur E et al . Effect of
communications training on medical student perfor-mance. Jama 2003;290(9):1157–1165.
14. Maguire P, Booth K, Elliott C, Jones B. Helping healthprofessionals involved in cancer care acquire keyinterviewing skills—the impact of workshops. Eur J Cancer 1996;32A(9):1486–1489.
15. Gordon J, Sanson-Fisher R, Saunders NA. Identifica-tion of simulated patients by interns in a casualtysetting. Med Educ 1988;22(6):533–538.
16. Ainsworth MA, Rogers LP, Markus JF et al . Standar-dized patient encounters. A method for teaching andevaluation. JAMA 1991;266(10):1390–1396.
17. Razavi D, Delvaux N, Marchal S et al . Testing health
care professionals’ communication skills: the usefulnessof highly emotional standardized role-playing sessionswith simulators. Psycho-Oncology 2000;9(4):293–302.
18. Iandolo C. Guide pratique de la communication avec lepatient. Techniques, arts et erreurs de la communica-tion: MMI Editions, Masson, 2002.
19. Tate P. Soigner (Aussi) Sa Communication: La RelationMe ´ decin-Patient. De Boeck: Paris, 2005.
20. Kurtz S, Silverman J, Draper J. Teaching and LearningCommunciation Skills in Medicine. Radcliffe MedicalPress; Oxford, 1998.
21. Baile WF, Buckman R, Lenzi R et al . SPIKES—A six-step protocol for delivering bad news: application to thepatient with cancer. Oncologist 2000;5(4):302–311.
22. Ruszniewski M. Face a ` La Maladie Grave. Dunod:
Paris, 2004.23. Bardin L. L’analyse De Contenu (10th edn), Presses
Universitaires de France: France, 2000.24. Whitehouse C, Morris P, Marks B. The role of actors in
teaching communication. Med Educ 1984;18(4):262–268.25. Cushing AM, Jones A. Evaluation of a breaking bad
news course for medical students. Med Educ 1995;29(6):430–435.
26. Fortin AH, Haeseler FD, Angoff N et al . Teaching pre-clinical medical students an integrated approach tomedical interviewing: half-day workshops using actors.J Gen Intern Med 2002;17(9):704–708.
27. Betson CL, Fielding R, Wong G et al . Evaluation of twovideotape instruction programmes on how to break badnews—for Cantonese-speaking medical students inHong Kong. J Audiov Media Med 1997;20(4):172–177.
28. Wakefield A, Cooke S, Boggis C. Learning together: useof simulated patients with nursing and medical studentsfor breaking bad news. Int J Palliat Nurs 2003;9(1):32–38.
29. Kimura D. Sex and Cognition. Mit Press: London, 1999.30. Lenzi R, Baile WF, Berek J et al . Design, conduct and
evaluation of a communication course for oncologyfellows. J Cancer Educ 2005;20(3):143–149.
31. Butow P, Cockburn J, Girgis A et al . Increasingoncologists’ skills in eliciting and responding to emo-tional cues: evaluation of a communication skillstraining program. Psycho-Oncology 2008;17(3):209–218.
32. Lown BA, Sasson JP, Hinrichs P. Patients as partners inradiology education: an innovative approach to teach-ing and assessing patient-centered communication. Acad Radiol 2008;15(4):425–432.
Simulated interviews for learning to break bad news in oncology 981
Copyrightr 2009 John Wiley & Sons, Ltd. Psycho-Oncology 19: 975–981 (2010)
DOI: 10.1002/pon