Embed Size (px)
Citation preview
Puberty and Adolescence
PUBERTY:IS THE PROCESS OF PHYSICAL CHANGES BY WHICH A CHILD'S BODY BECOMES AN ADULT BODY CAPABLE OF REPRODUCTION
ADOLESCENCE: IS THE AGE BETWEEN 10 -19 YEARSE TRANSITIONAL STAGE OF PHYSICAL AND MENTAL HUMAN DEVELOPMENT GENERALLY OCCURRING BETWEEN PUBERTY AND LEGAL ADULTHOOD
PHYSIOLOGY• Puberty is initiated by hormone signals from the
brain to the gonads (the ovaries and testes).
• the gonads produce a variety of hormones that stimulate the growth, function, or transformation.
THE NORMAL PUBERTY
• Physical changes.Physical changes.
• Hormonal changes.Hormonal changes.
Physical Physical changeschanges..
Hair distribution
Menstruation+ fertility
Reproductive Reproductive system system
maturationmaturation
Body Body compositioncomposition BMD
PHYSICAL CHANGESPHYSICAL CHANGES..
• Puberty proceeds through five stages from childhood to full maturity (P1 to P5) as described by Marshall and Tanner.
• In both sexes, these stages reflect the progressive modifications of the external genitalia and of sexual hair.
PHYSICAL CHANGES FOR MALES
1-testicular enlargement is the first physical manifestation of puberty
2-pubic hair often appears on a boy shortly after the genitalia begin to grow
3- voice change and Adams apple
4-Male musculature and body shape and Body odor and acne
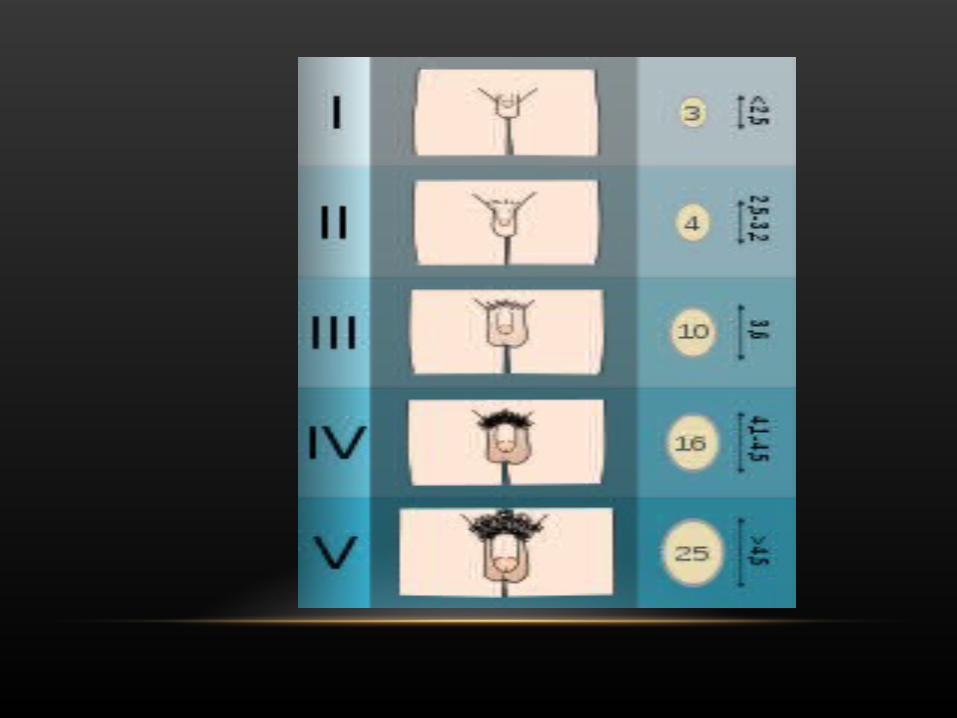
TANNER STAGING OF PUBERTY IN MALESTanner I
prepubertal (testicular volume less than 3.5 ml; small penis of 3 cm or less)[
Tanner II testicular volume 6 ml; skin on scrotum thins, reddenss and enlarges; penis length unchanged
Tanner III testicular volume between 6 and 12 ml; scrotum enlarges further; penis begins to lengthen to about 6 cm
Tanner IV testicular volume between 12 and 20 ml; scrotum enlarges further and darkens; penis increases in length to 10 cm and circumference
Tanner V testicular volume greater than 20 ml; adult scrotum and penis of 15 cm in length
BREAST DEVELOPMENT
The first physical sign of puberty in girls
occurring on average at about 10 years of age.
Tanner staging of puberty.
TANNER BREAST DEVELOPMENTBreasts (female)
Tanner I no glandular tissue; areola follows the skin contours of the chest (prepubertal)
Tanner II breast bud forms, with small area of surrounding glandular tissue; areola begins to widen
Tanner III breast begins to become more elevated, and extends beyond the borders of the areola, which
continues to widen but remains in contour with surrounding breast[
Tanner IV increased breast size and elevation; areola and papilla form a secondary mound projecting from
the contour of the surrounding breast[
Tanner V breast reaches final adult size; areola returns to contour of the surrounding breast, with a
projecting central papilla[ .
PUBIC HAIRPUBIC HAIR
• second noticeable change in puberty.• usually within a few months of thelarche.• Tanner staging.
TANNER PUBIC STAGINGPubic hair (both male and female)
Tanner I
no pubic hair at all (prepubertal Dominic state) [typically age 10 and younger]
Tanner II
small amount of long, downy hair with slight pigmentation at the base of the penis and scrotum (males) or on the labia majora (females) [10–11.5]
Tanner III
hair becomes more coarse and curly
Tanner IV
adult-like hair quality, extending across pubis but sparing medial thighs [13–15]
UTERINE DEVELOPMENTThe Prepubertal uterus
tear-drop shaped
neck and isthmus accounting for up to 2/3 of the uterine volume.
Craniocaudal direction without the flextion of adult.
then, with the production of estrogens, it becomes pear shaped, with the uterine body increasing in length and thickness proportionately more than the cervix.
Reproductive system maturation
• The mucosal surface of the vagina also changes in becoming thicker and duller pink in color.
• Whitish secretions (physiologic leukorrhea ).
• The ovaries usually contain small follicular cysts visible by ultrasound.
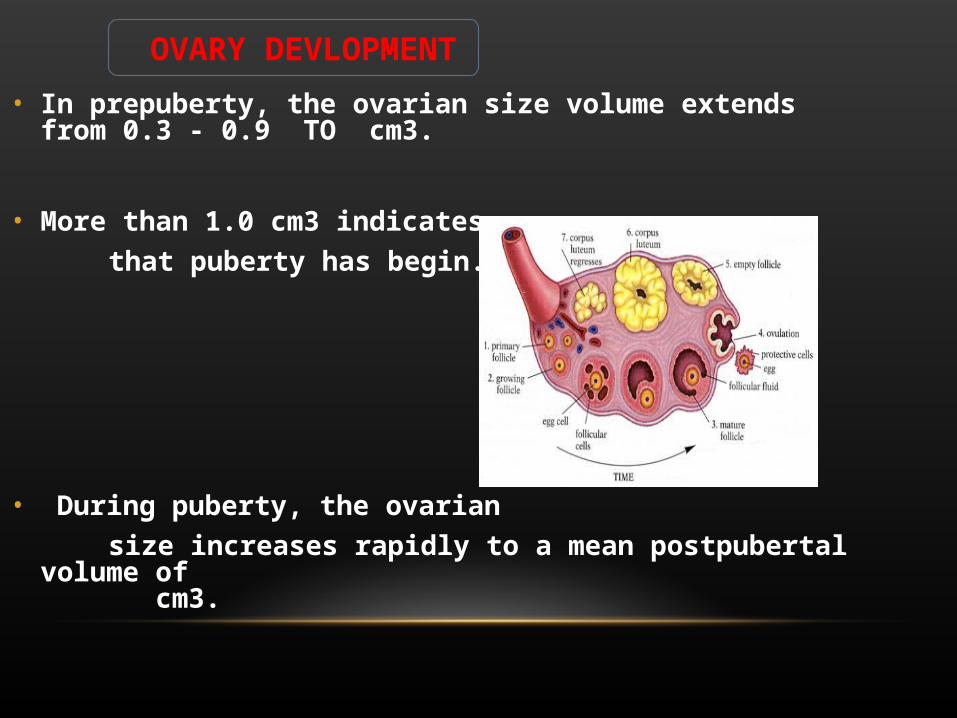
• In prepuberty, the ovarian size volume extends from 0.3 - 0.9 TO cm3.
• More than 1.0 cm3 indicates
that puberty has begin.
• During puberty, the ovarian
size increases rapidly to a mean postpubertal volume of cm3.
OVARY DEVLOPMENT

MENSTRUATION+ FERTILITY
• menarche, and typically occurs about two years after thelarche
• The average age of menarche in girls is 11. years• The time between menstrual periods (menses) is not
always regular in the first two years after menarche• Ovulation is necessary for fertility, but may or may not
accompany the earliest menses• Starting of ovulation? By production of progesteron
• 6-9 month after thelarche• 11.5 y at Ts 2-3• BMDPeak menerlization 14-16 y.Influence by Genetic ExcersiseGH.
Bone mineral density
HORMONAL CHANGES OF PUBERTY
• Gonadotropin-Releasing Hormone• •Gonadotropins• •Adrenal steroids
GONADOTROPIN-RELEASING HORMONE
• GnRH is synthesized and released from neurons within the hypothalamus.
• Chromosome8.• GnRH stimulates the synthesis and
secretion of the gonadotropins .• GnRH is secreted in pulses .• LH ,FSH
ROLE OF GONADOTROPINSFSHStimulates the ovaryInvolved in spermatogenesis in the testesInduces receptors for LH
LHUses as substrate to produce estradiol in theca cellsStimulates testosterone synthesis by Leydig cells
FSH is usually higher than LH in prepubertal stages, and this reverses in pubertal stages
SEX STEROIDSTESTOSTERONE EXTERNAL GENITALIA.MUSCLE GROWTH
ESTROGENBREAST UTERINEADIPOSE TISSUEBONE MINERALIZATION EPIPHYSIEL PLATE
Precocious puberty.
Delayed puberty
ABNORMAL PUBERTY
PRECOCIOUS PUBERTY
the appearance of physical and hormonal signs of pubertal development at an earlier age than is considered normal.
girls < 7 years.
black girls 6-8 years.
boys< 8 years
PRECOCIOUS PUBERTY CAN BE DIVIDED INTO 2 PRECOCIOUS PUBERTY CAN BE DIVIDED INTO 2 DISTINCT CATEGORIESDISTINCT CATEGORIES . .
gonadotropin-dependent gonadotropin-dependent precocious pubertyprecocious puberty
involves the premature involves the premature activation of the activation of the
hypothalamic-pituitary-hypothalamic-pituitary-gonadal (HPG) axis.gonadal (HPG) axis.
GDPPGDPP
gonadotropin-independent gonadotropin-independent precocious puberty precocious puberty
in which the presence of in which the presence of sex steroids is independent of sex steroids is independent of pituitary gonadotropin releasepituitary gonadotropin release..
GIPPGIPP
CAUSESCAUSES
1.Constitutional or idiopathic: • In most cases of precocious puberty (90%) , no
cause is found. • For some unknown reason the hypothalamus
stimulates the pituitary gland to secrete its gonadotrophic hormones.
• There is normal menstruation and ovulation. • Pregnancy can occur at young age.
CAUSESCAUSES
2. Organic lesions of the brain:
• The next common cause.
• Organic lesions affecting the midbrain, hypothalamus, pineal body, or pituitary gland may lead to premature release of pituitary gonadotrophins.
• Examples include traumatic brain injury, meningitis, encephalitis, brain abscess, brain tumor as glioma, craniopharyngioma, and hamartomas.
CAUSESCAUSES
3. McCune-Albright syndrome.
4. Adrenal causes:
(a) Hyperplasia, adenoma, or carcinoma of suprarenal cortex.
Congenital adrenal hyperplasia and lead to precocious puberty in the male direction, i.e.
heterosexual precocious puberty;
(b) Estrogen secreting adrenal tumor which is very rare.
CAUSESCAUSES
5. Ovarian causes :(a) Estrogen producing tumors as granulosa and theca cell
tumor;
(b) Androgen producing tumors as androblastoma;
(c) Choriocarcinoma because it secretes human chorionic gonadotrophin (HCG) which may stimulate the ovaries to secrete estrogen;
(d) Dysgerminoma if it secretes HCG.
6. Juvenile hypothyroidism:
Lack of thyroxine leads to increased production of thyroid stimulating hormone and the secretion of pituitary gonadotrophins may also be increased.
7. Drugs:
• latrogenic may follow oral or local administration of estrogen.
• A long course of estrogen cream used for treatment of vulvovaginitis of children may lead to breast development or withdrawal bleeding.
8. Silver syndrome: Small stature, retarded bone age and increased Gonadotrophin levels.
SYMPTOMSSYMPTOMS
Girls.*breast enlargement, unilateral.*Pubic and axillary hair.*Axillary odor *Menarche until 2-3 years after onset of breast enlargement.*The pubertal growth spurt occurs early in female puberty.
boysboys*testicular enlargement*Growth of the penis and scrotum + appearance of pubic hair typically occur at least a year after testicular enlargement.*Accelerated linear growth (the pubertal growth spurt) occurs later in the course of male puberty than in female puberty

SIGNSSIGNS *breast enlargement*breast diameter inc*areola darkens + thickens*nipple becomes more prominent*enlargement of the clitoris *pubic hair*deep-red color of vaginal mucosa *Mild acne
*enlargement of the testes*penis growth, *reddening+thinning of the scrotum *increased pubic hair*the pubertal growth spurt, acne, *voice change, *facial hair.
DIAGNOSIS OF PRECOCIOUS PUBERTY
1. History:
• It excludes iatrogenic source of estrogen or androgen.
• It differentiates between isosexual and heterosexual precocious puberty.
2. Physical examination:
• It diagnoses McCune-Albright syndrome.
• Neurologic and ophthalmologic examinations exclude organic lesions of the brain.
FEMALE PRECOCIOUS PUBERTY
3. Special investigations:
These are done according to the history and clinical findings and include:
DIAGNOSIS
a. X-ray examination of the hand and wrist
to determine bone age.
• Estrogen stimulates growth of bone but causes early fusion of the epiphysis.
• So the child is taller than her peers during childhood, but she is short during adult life.
DIAGNOSIS
DIAGNOSIS
c. Ultrasonography
to diagnose ovarian or adrenal tumor.
d. CT or MRI :
to diagnose an organic lesion of the brain, or adrenal tumor.
Hypothyroidism
retards bone age, and is the only condition of precocious puberty in
which bone age is retarded
IDIOPATHIC PRECOCIOUS IDIOPATHIC PRECOCIOUS PUBERTYPUBERTY::
is diagnosed after excluding all other causes.
TREATMENT OF PRECOCIOUS PUBERTY
1. Treatment of the cause, e.g., thyroxin for hypothyroidism, removal of ovarian and adrenal tumors.
2. Incomplete forms of precocious puberty do not require treatment, as estrogen production is not increased.
3 .MCCUNE-ALBRIGHT SYNDROME
• is treated with testolactone oral tablets.
• The drug inhibits the formation of estrogen from its precursors, so reduces estrogen level.
• The dose is 20 mg/kg body weight in 4 divided doses and increased to 40 mg/kg body weight during a 3 week interval.
4 .IDIOPATHIC TYPEis treated by explanation and reassurance and by giving one of
the following drugs which inhibit the secretion of gonadotrophins:
(a)Gonadotrophin releasing hormone analogues
(b)Medroxyprogesterone acetate tablets (Provera tablets)
(c) Danazol capsules
(d) Cyproterone acetate tablets
Treatment is given till the age of 12 years (mean age of pubertal development).
MCCUNE-ALBRIGHT SYNDROME:
• The disease is found more frequently in girls.
• It consists of a triad of :
1. Precocious puberty,
2. Cystic changes in bones, and
3. Cafe-au lait patches of the skin.
• The cause of precocious puberty is autonomous production of estrogen by the ovaries.
• FSH and LH levels are low.
• The treatment is testolactone oral tablets which inhibit ovarian steroidogenesis.
DELAYED PUBERTY
Delayed puberty is indicated if no signs of puberty are observed in a girl by14 years in age and in a boy by 15 years in age
Evaluation also indicated of an arrest of pubertyal maturation occurs
ETIOLOGY OF DELAYED PUBERTY
1 - Constitutional
with +ve family history , short stature & normal fertility .
2 - Hypergonadotropic hypogonadism
Gonadal damage secondary to chemotherapy/radiation
Enzyme defects in the gonads
Androgen insensitivity
Ovarian/testicular dysgenesis
3 - Hypogonadtropic hypogonadism
A male has abnormal testicles that do not produce normal levels of the sex hormone, testosterone.
A female has abnormal ovaries that do not produce normal levels of sex hormone, estrogen.
4 -Gonadal Failure (bilateral)
In these cases, circulating levels of LH & FSH are high (hypergonadotropic hypogonadism)
*CongenitalTurner Syndrome
Klinefelter’s Syndrome
Complete androgen insensitivity
*AcquiredChemotherapy/Radiation/Surgery
Postinfectious (ie. mumps orchitis, coxsackievirus infection, dengue, shigella, malaria, varicella)
Testicular torsion
Autoimmune/metabolic (autoimmune polyglandular syndromes)
“Vanishing Testes syndrome”
“Resistant Ovaries syndomre” (gonadatropin receptor problems)
5 -Eugonadotropic pubertal delay*Congenital Anatomic Anomalies
Imperforate hymen
Vaginal atresia
Vaginal aplasia
*PCOS
*Hyperprolactinemia
6-Other Endocrine Causes
*Hypothyroidism
Interferes with gonadotropin secretion
*Hyperprolactinemia
Interfere with gonadotropin production7 -other causes
MalnutritionGrowth Hormone DeficiencyBrain tumors
Craniopharyngioma, astrocytomas, gliomas, histiocytosis X, germinomas, prolactinomas
Iron overload (pituitary damage)GnRH receptor abnormalities
INVESTIGATING DELAYED PUBERTY
History :
1 - Family history , nutritional history , any systemic diseases
(e.g. history of endocrinal disturbance).
2 - Clinical picture of space occupying lesion in the ovary , adrenal, pituitary & hypothalamus.
3 - Periodic pain and +ve 2ry sexual characteristics in imperforate hymen .
INVESTIGATING DELAYED PUBERTY
Examination :
(A) Body measurement for causes of amenorrhea + ↑or ↓weight, short or tall stature , proportions (upper / lower segment ratio & arm span / height ratio).
(B) Tanner staging of breast,testes, pubic & axillary hair if present.
(C) Neurological examination for smell sense (Kallman's syndrome), visual field & other cranial nerve lesions .
1-Primary investigationsRoutine first-line:FBC and CRP or ESR to exclude anaemia, iron deficiency, malnutrition and hidden inflammatory disease.
RFT and LFT to exclude renal and liver diseases.
Bone profile.
TSH and free T4 to exclude hypothyroidism (central hypothyroidism cannot be excluded on TSH alone)
Second-line (endocrine):FSH and LH - low levels are associated with central or constitutional delay. Elevated levels are associated with primary testicular or ovarian disorder.
Prolactin - significant elevation is suggestive of pituitary microadenoma.
Early morning estradiol (girls) - low but detectable levels suggest pubertal development is imminent.
Early morning testosterone (boys) - low but detectable levels suggest pubertal development is imminent.
Elevated testosterone (female range) and LH:FSH ratio is suggestive of PCOS in girls.
2 -secondary investigations
Chromosomal study if short stature or hypergonadotropic type .
Radiological bone age study & radiologic study for pituitary adenoma
INVESTIGATING DELAYED PUBERTY
TREATMENT OF DELAYED PUBERTYExclusion of a serious organic disease or a chromosome variation is the primary goal in an adolescent presenting with true delayed sexual development.
If all is normal, and puberty is just late, simple reassurance is all that is needed.
Delay, especially when accompanied by short stature, can produce anxiety, depression and low self-esteem, isolation and school refusal.
As this is almost always a problem for boys due to the difference in physiological timing of events, a short-term course of around three to 12 months' treatment with low-dosage testosterone can boost growth, pubertal progress and morale.
Treatment options include monthly depot testosterone esters or daily oral capsules .
TREATMENT OF DELAYED PUBERTY
Testosterone is usually continued until there is clear evidence of spontaneous puberty (testicular growth).
The duration and dosage of therapy should be monitored by a paediatric endocrinologist as overdosage or excessively long courses can reduce the period of pubertal growth.
Growth hormone is not necessary unless there is a proven deficiency.
Therapeutic management of simple delayed puberty is rarely required in girls, but very low doses of ethinyl estradiol are the mainstay of treatment.
Thank you