Embed Size (px)
Citation preview
Pulmonary Complications of Sickle Cell Disease
Liz Klings, MD
The Pulmonary Center
Boston University School of Medicine
Why care about a hemoglobinopathy?
0.15% of African Americans are HbSS (250,000 births per year worldwide)
8% have sickle cell trait
Median age at death 42 (males) and 48 (females)
Pulmonary complications – major cause of mortality (20-30% of deaths)
Shortcomings in this Field
• SCD is rare, hard to do large population-based studies
• Difficult patient population to study
• Lack of placebo-controlled randomized trials and outcomes studies
Important Unanswered Questions
• Does screening for PH alter outcomes?• Does PAH of SCD respond to traditional PAH
therapies?• Why do SCD patients develop diastolic
dysfunction and how should we treat this?• What role does VTE play in disease
modulation of SCD?• What is the contribution of airways disease,
OSA and hypoxemia to chronic pulmonary disease?
Acute Chest Syndrome
Occurs in up to 45% of SCD patients; recurrent in up to 80%Clinical presentation differs in kids vs. adultsIncreased incidence in pediatric asthmatics (DeBaun 2006)Defined as a new infiltrate + CP/fever/tachypnea/wheezing/cough
ACS – Diagnostic Work-Up
CXR/Labs – WBC, markers of hemolysis, ABG
V/Q scan
Bronchoscopy/Induced Sputum
Hb S levels
Secretory phospholipase A2/CRP
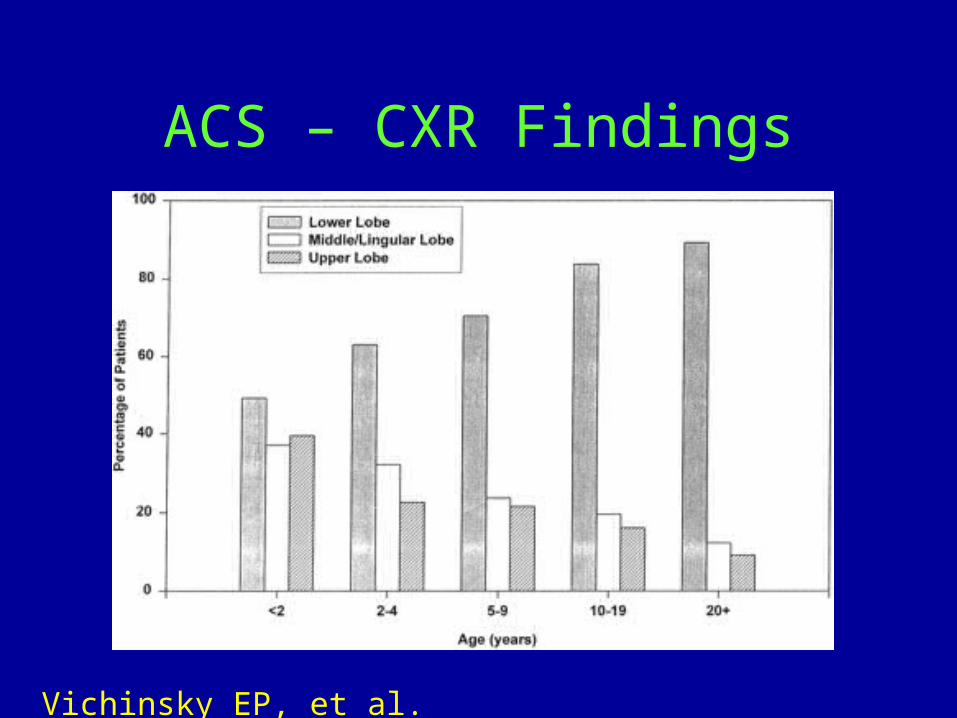
ACS – CXR Findings
Vichinsky EP, et al. Blood 1997
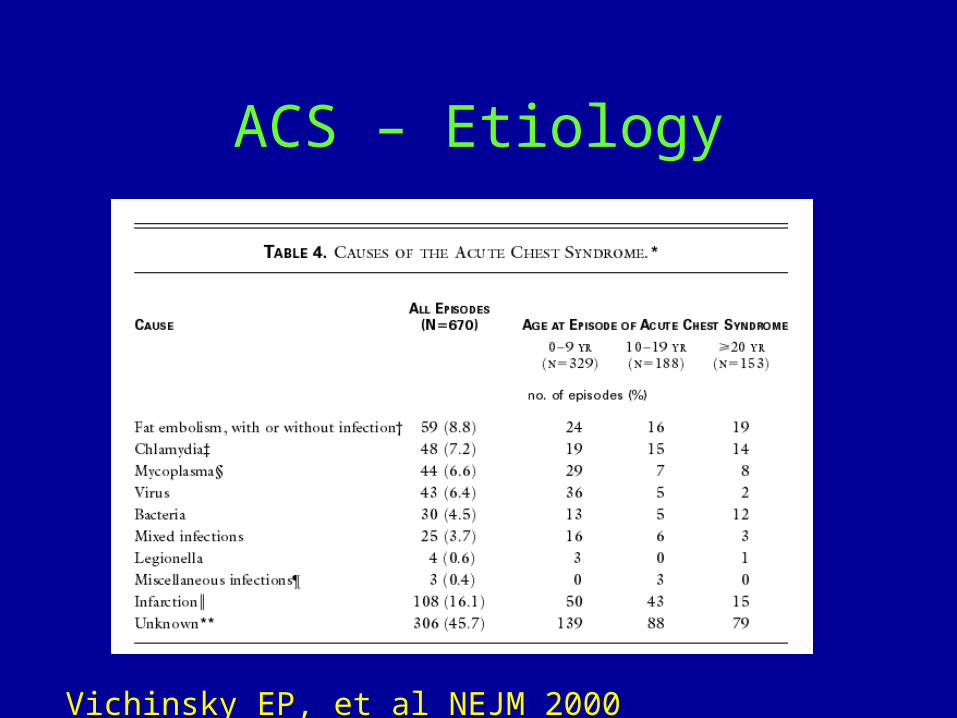
ACS – Etiology
Vichinsky EP, et al NEJM 2000
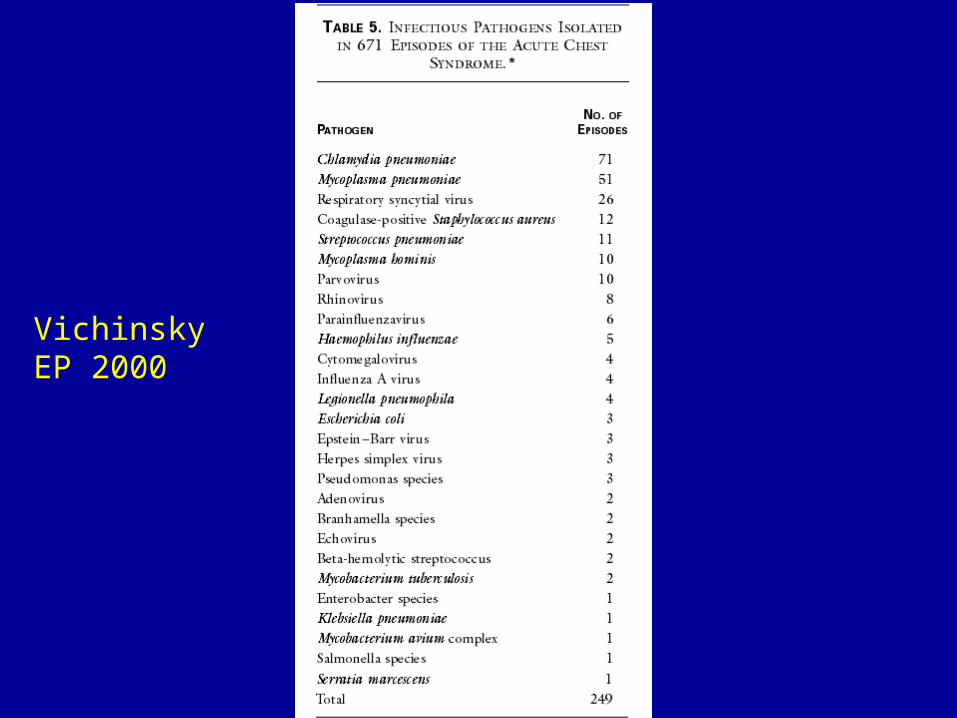
Vichinsky EP 2000
Predictors of Respiratory Failure in ACS
Multi-lobar disease (>4 lobes highest risk)
History of cardiac disease
Thrombocytopenia
Pre-existent pulmonary hypertension
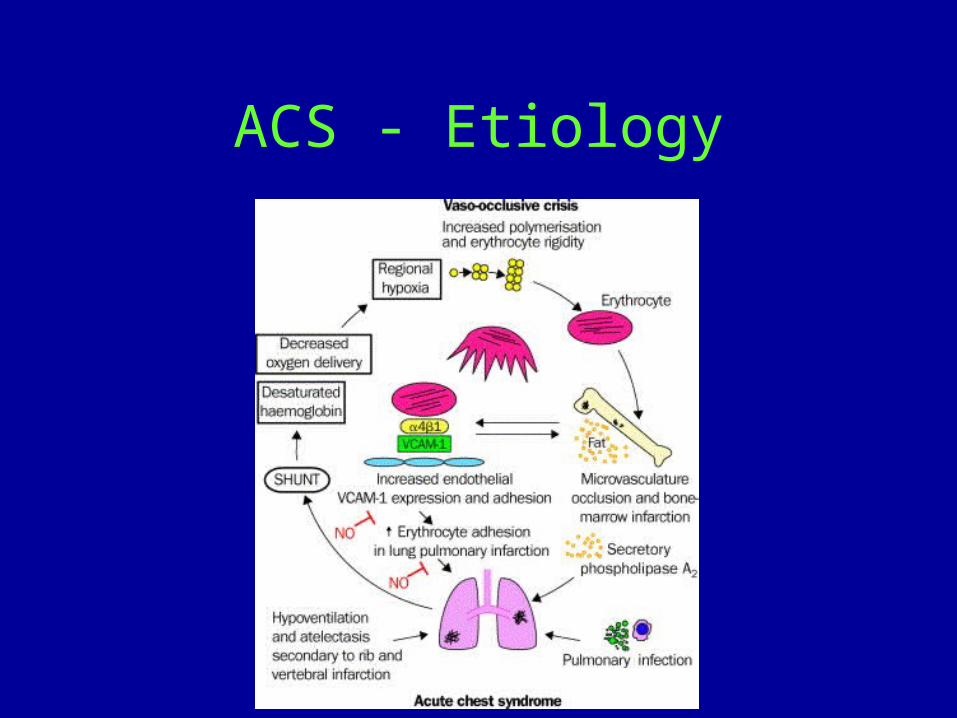
ACS - Etiology
ACS – Treatment Strategies
Pain control/incentive spirometry
Bronchodilators
Antibiotics
Transfusion- Simple or exchange
Anti-coagulation if VTE confirmed
Other agents – inhaled NO, anti-adhesive agents, steroids
Pulmonary HTN in SCDWas for many yrs thought to be part of “Chronic sickle cell lung disease”
Originally defined by a TRV > 2.5 m/sec
Observed in 1/3 of HbSS and 10-25% of HbSC adults
10-22% of HbSS children and adolescents
Overlap in some with LV diastolic dysfunction
Gladwin MT, et al. NEJM 2004; 350:886-95.Castro O, et al. Blood 2003; 4:1257-1261.Kato GJ, et al. Blood Rev 2007; 21:37-47.Klings ES, et al. Am J Hematol 2008; 83 (7):547-553.
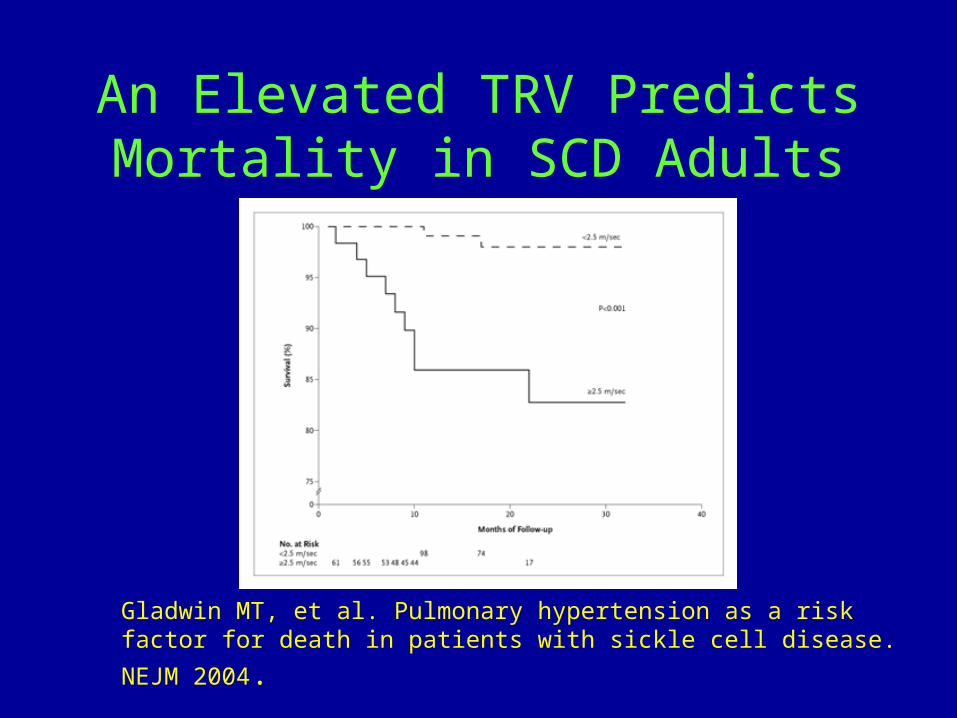
An Elevated TRV Predicts Mortality in SCD Adults
Gladwin MT, et al. Pulmonary hypertension as a risk factor for death in patients
with sickle cell disease. NEJM 2004.
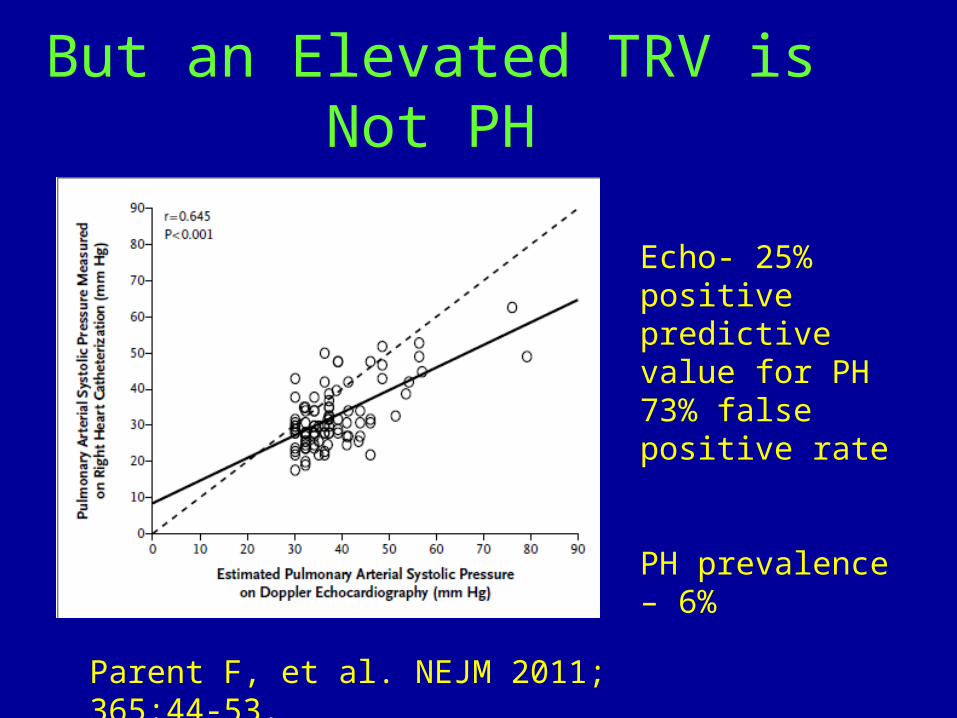
But an Elevated TRV is Not PH
Echo- 25% positive predictive value for PH73% false positive rate
PH prevalence – 6%
Parent F, et al. NEJM 2011; 365:44-53.
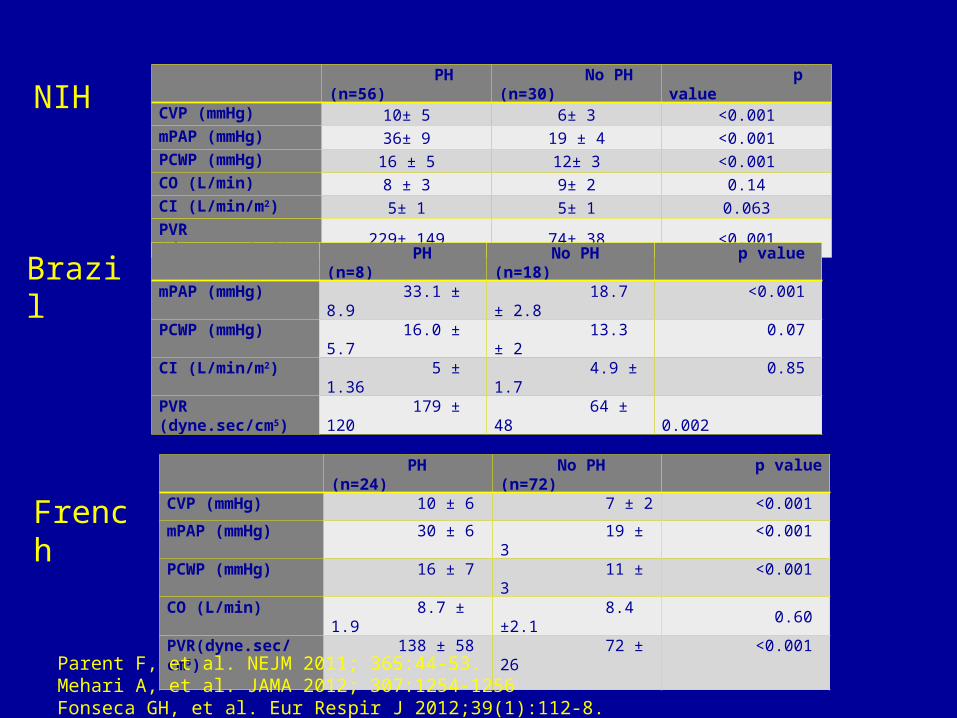
PH (n=56) No PH (n=30) p value
CVP (mmHg) 10± 5 6± 3 <0.001mPAP (mmHg) 36± 9 19 ± 4 <0.001PCWP (mmHg) 16 ± 5 12± 3 <0.001CO (L/min) 8 ± 3 9± 2 0.14CI (L/min/m2) 5± 1 5± 1 0.063PVR (dyne.sec/cm5) 229± 149 74± 38 <0.001
PH (n=24) No PH (n=72) p valueCVP (mmHg) 10 ± 6 7 ± 2 <0.001
mPAP (mmHg) 30 ± 6 19 ± 3 <0.001
PCWP (mmHg) 16 ± 7 11 ± 3 <0.001
CO (L/min) 8.7 ± 1.9 8.4 ±2.1 0.60
PVR(dyne.sec/cm5) 138 ± 58 72 ± 26 <0.001
PH (n=8) No PH (n=18) p value
mPAP (mmHg) 33.1 ± 8.9 18.7 ± 2.8 <0.001
PCWP (mmHg) 16.0 ± 5.7 13.3 ± 2 0.07
CI (L/min/m2) 5 ± 1.36 4.9 ± 1.7 0.85
PVR (dyne.sec/cm5) 179 ± 120 64 ± 48 0.002
NIH
Brazil
French
Parent F, et al. NEJM 2011; 365:44-53.Mehari A, et al. JAMA 2012; 307:1254-1256Fonseca GH, et al. Eur Respir J 2012;39(1):112-8.
Differences from IPAH
Often a paucity of symptoms
PA pressures/PVR tend to be lower
Preservation of cardiac output
Increased PCWP in some patients
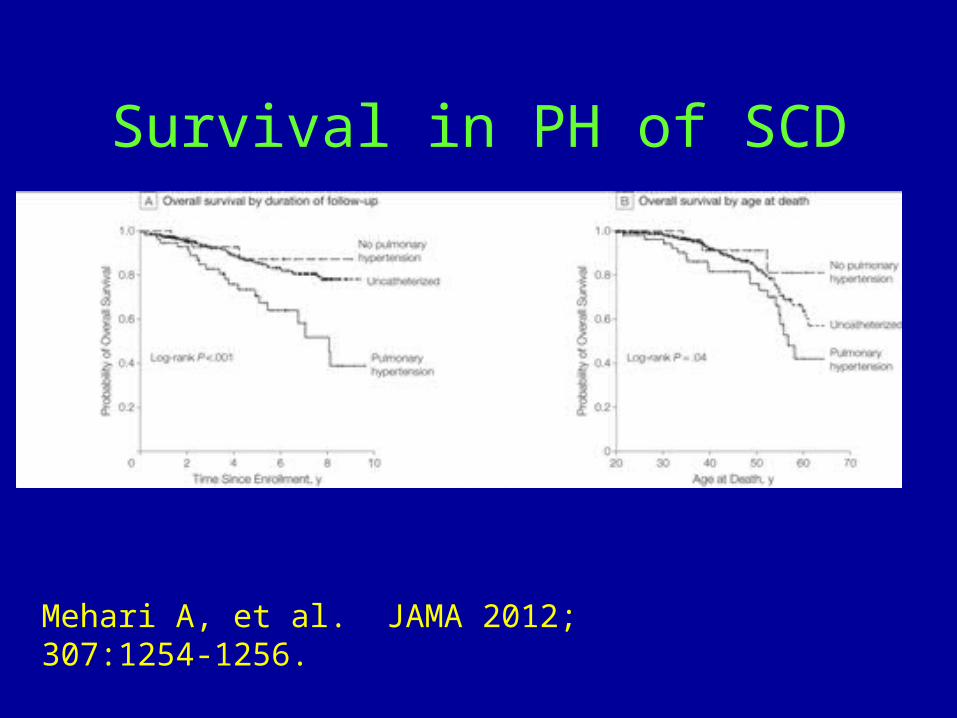
Survival in PH of SCD
Mehari A, et al. JAMA 2012; 307:1254-1256.
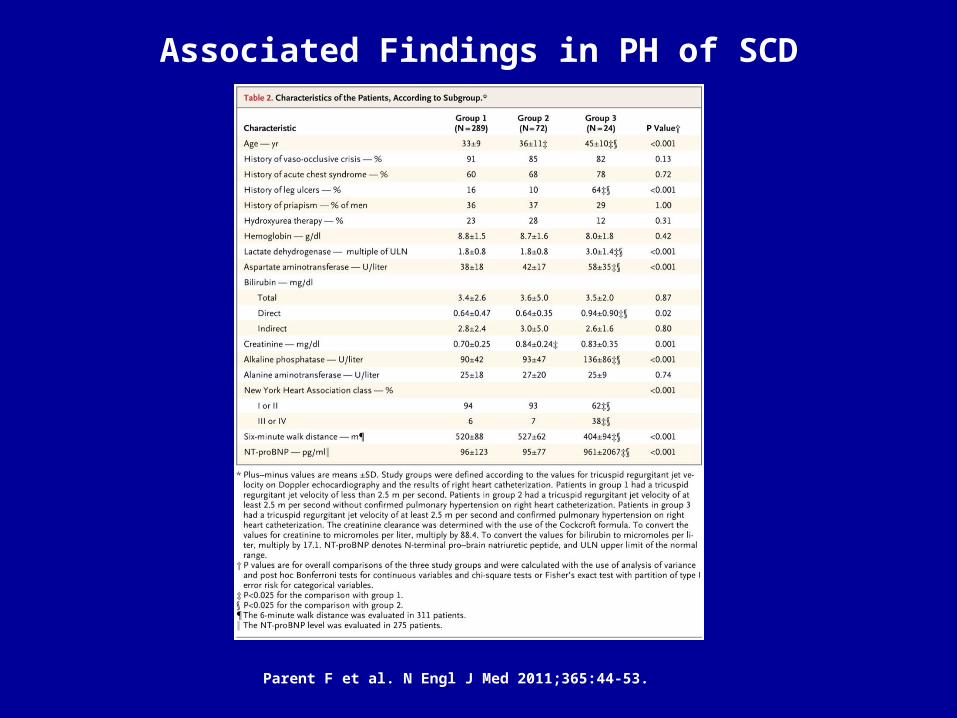
Associated Findings in PH of SCD
Parent F et al. N Engl J Med 2011;365:44-53.
Summary of Hemodynamic Data in PH of SCD
6-10.5% of HbSS adults have PH
Prevalence of PVH – 44-63% of PH patients
Prevalence of PAH in SCD 2.5-5.8%
PA pressures and PVR characteristically lower than IPAH
Parent F, et al. NEJM 2011; 365:44-53.Mehari A, et al. JAMA 2012; 307:1254-1256Fonseca GH, et al. Eur Respir J 2012;39(1):112-8.Klings ES, et al. AJRCCM March 1, 2014 (in press)
Is Screening for PH in SCD Necessary?
• Evidence is stronger in adults
• Pediatric population – No associated mortality, may be reversible, and may predict worse exercise capacity
• No outcomes studies to predict benefit
• But, this may be the only way to identify PH patients early in disease course
Etiology of PH in SCD
Unknown, likely multi-factorial
Historically, related to recurrent episodes of ACS, but this is not true
Endothelial dysfunction- pro-constrictive and pro-adhesive
Oxidant stress and decreased NO bioavailability
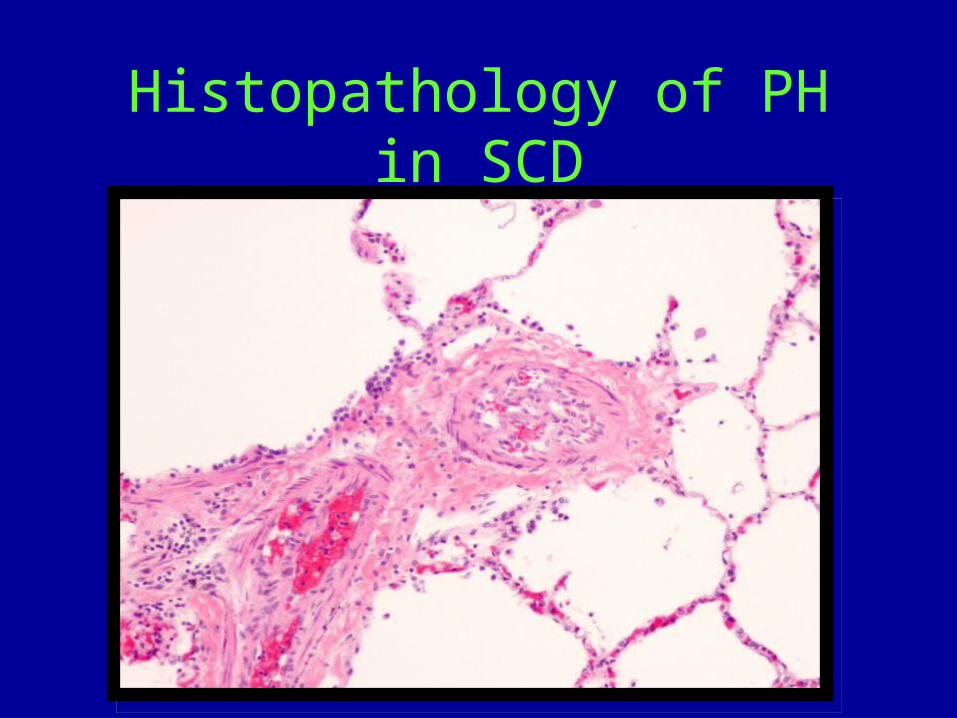
Histopathology of PH in SCD
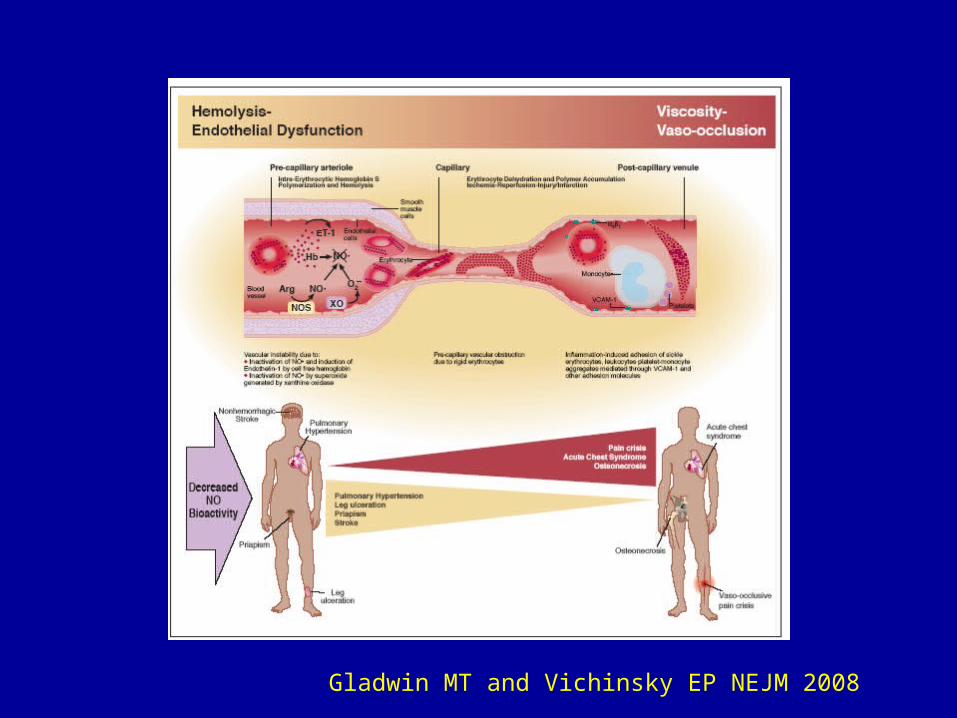
Gladwin MT and Vichinsky EP NEJM 2008
Hemolysis-related PH
PH associated with other hemolytic diseases:
1) Post-splenectomy2) β-thalassemia3) Hereditary spherocytosis4) Pyruvate kinase deficiency
May be a mechanism of decreased NO bioavailability
Decreased NO Bioavailability
Decreased NO production
Increased NO consumption
a) Scavenging by free Hb
b) Oxidant consumption
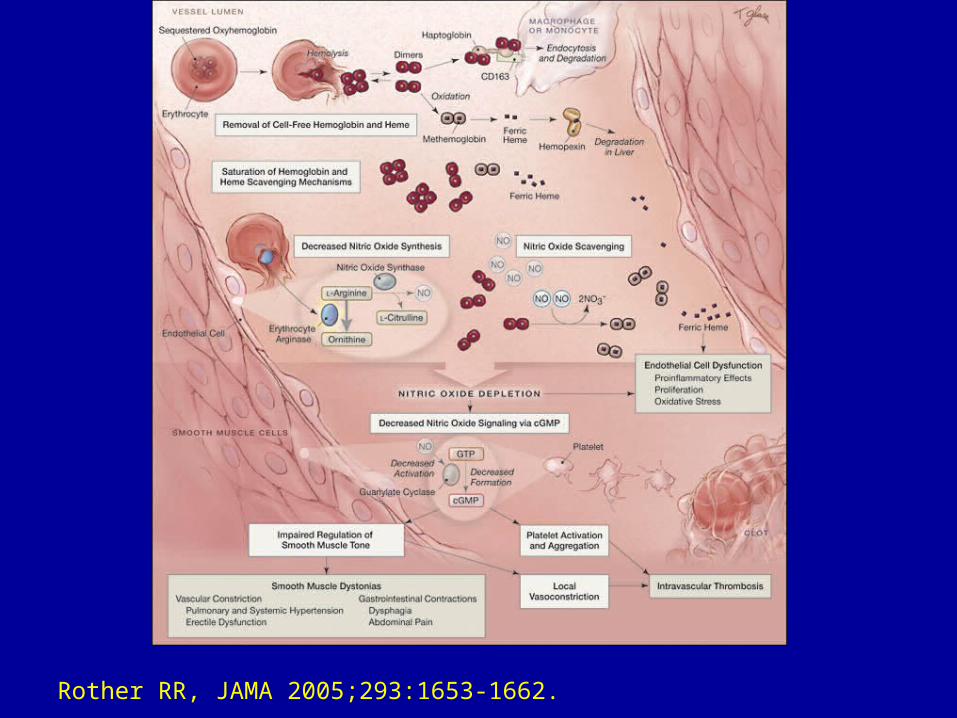
Rother RR, JAMA 2005;293:1653-1662.
Treatment of PH in SCD
Treatment Issues Specific to SCD
Multiple co-morbiditiesAnemia produces an elevated CO and symptoms can be delayedIncreased risk of bleeding and possibly infectionNot all PH in SCD is PAHNo randomized trials completed in this populationRecommend referral to PH center with expertise in SCD
SCD Specific Therapies and Co-Morbidities
• Hydroxyurea
• Chronic Transfusions
• Treatment of associated conditions: OSA, VTE, hypoxemia
HydroxyureaOnly FDA approved medication for SCD, under-utilized
Reduces VOC, ACS and need for transfusion in HbSS
Primary action – induction of HbF
Long-term studies – improved survival
at 17.5 yrs
Benefits in PH of SCD theoretical, not studied
Steinberg MH, et al. JAMA 2003;285;1645-1651.Steinberg MH, et al. Am J Hematol 2010; 85:403-408.
Chronic Transfusions• Best studied in pediatric patients for stroke
prevention – STOP 1 and 2
• May reduce frequency of VOC/ACS
• No effects on mortality
• In a small case series, lowered PASP by echo
• Risk of iron overload and allo-immunization
Lee MT, et al. Blood 2006; 108:847-852.Wang WC, et al. J Pediatr 2005; 147:244-247
The Link Between VTE and PH
2-4% of patients with PE will develop CTEPHAutopsy studies of IPAH patients – in situ thrombosisSCD is a hyper-coagulable statePatients with PH of SCD – thrombotic arteriopathy of small PA’sBut the link between DVT/PE and PH in SCD is unclear
Haque AK, et al.Hum Pathol 2002; 33(10):1037-1043.
Graham JK, et al. Am J Forensic Med Pathol 2007; 28(2):168-172.van Beers EJ, et al. Haematologica 2008; 93(5):e42-e44.Ataga KI, et al. Haematologica 2008; 93(1):20-26.Wilkins H, et al. Int J Cardiol 2011; 154S1: S54-S60.
Risk of VTE in SCD Patients with an Elevated TRV
Used clinical data from patients recruited as part of the PH in SCD study at Boston University (n=162) Prospective observational study conducted from 2004-2010Enrolled all SCD patients > 12 yrsAll subjects underwent a screening questionnaire, echocardiogram and procurement of a blood sample
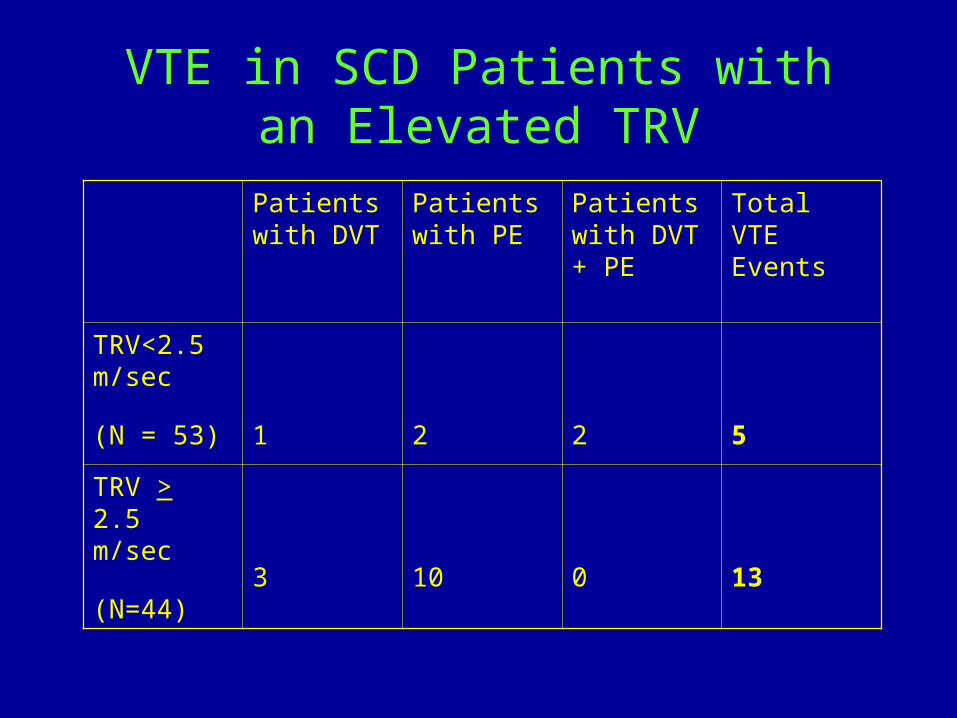
VTE in SCD Patients with an Elevated TRV
Patients with DVT
Patients with PE
Patients with DVT + PE
Total VTE Events
TRV<2.5 m/sec
(N = 53) 1 2 2 5
TRV > 2.5 m/sec
(N=44) 3 10 0 13
Increased Risk of VTE in SCD Patients with an Elevated TRV
18.5% of SCD patients had a history of VTE5/53 patients (9.4%) with a normal echo had a history of VTE, compared with 13/44 (29.5%) in the elevated TRV group. SCD patients with an elevated TRV were four times more likely to have a history of VTE compared to those with a normal echo(OR: 4.03, 95% CI 1.31-12.41, p=0.01).
ASSET-1 and 2: Bosentan in PH of SCD
• Randomized placebo controlled trials of bosentan in PAH or PVH of SCD
• Industry sponsored
• Difficulties with site initiation and enrollment led to sponsor withdrawal
• 26 subjects enrolled, efficacy endpoints not analyzed
Barst RJ, et al. Br J Haematol 2010;149(3):426-35
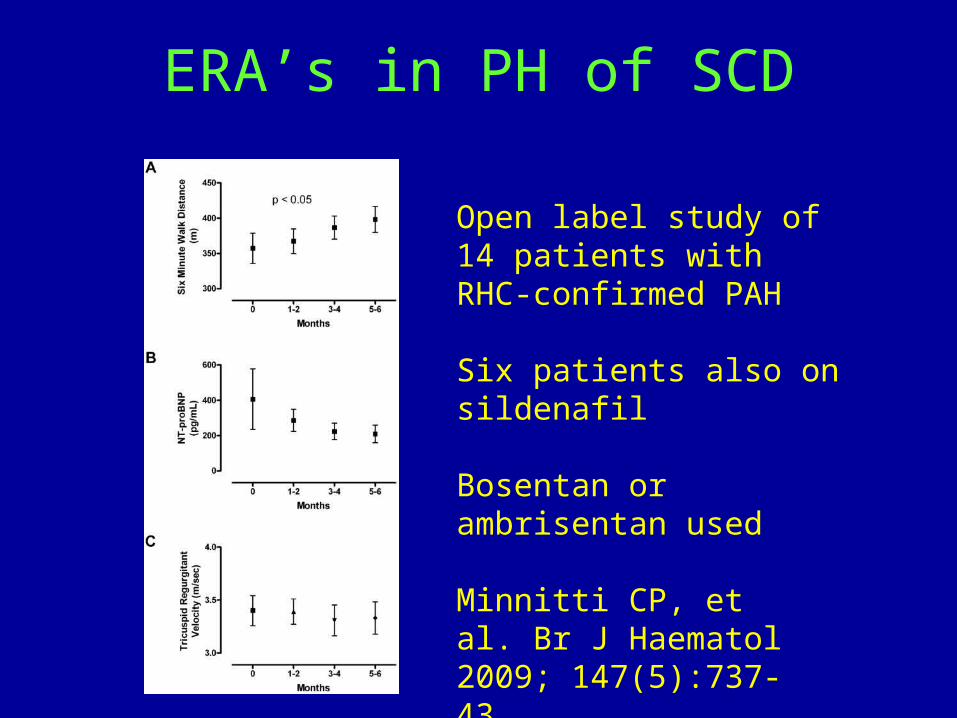
ERA’s in PH of SCD
Open label study of 14 patients with RHC-confirmed PAH
Six patients also on sildenafil
Bosentan or ambrisentan used
Minnitti CP, et al. Br J Haematol 2009; 147(5):737-43.
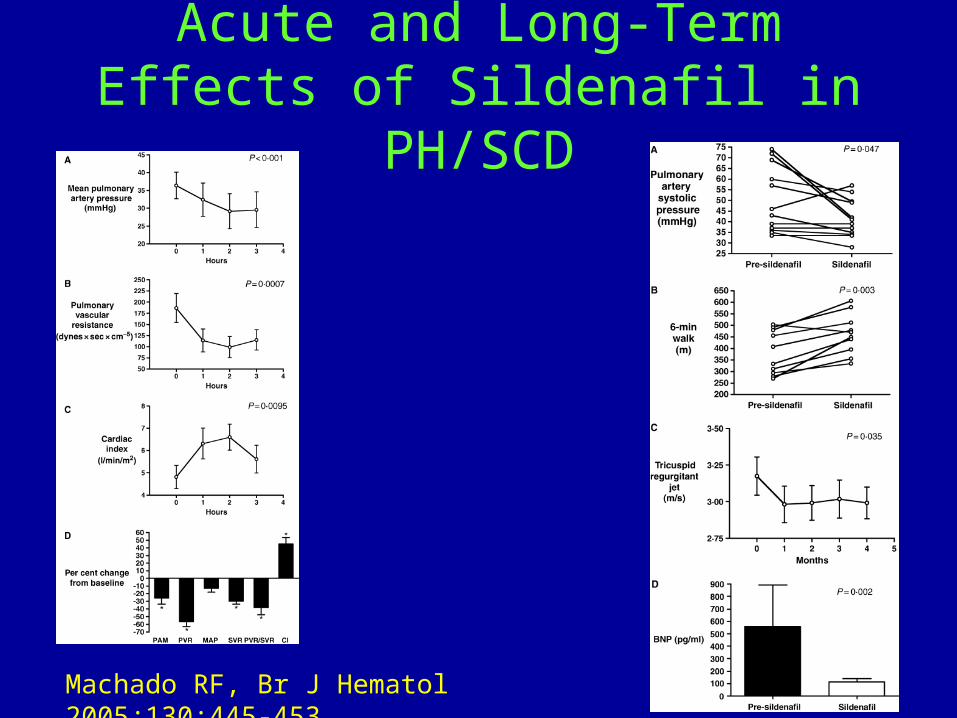
Acute and Long-Term Effects of Sildenafil in PH/SCD
Machado RF, Br J Hematol 2005;130:445-453.
Walk-PHaSST – Sildenafil for PH of SCD
Used echo definition of PH (TRV > 2.7 m/sec)
Primary outcome: improved 6MWD
Planned to enroll 132 subjects
Study stopped prematurely after 74 were randomized
Increased SAE’s in sildenafil group – primarily VOC
Questions about efficacy
Machado RF, et al. Blood 2011;118(4):855-64.
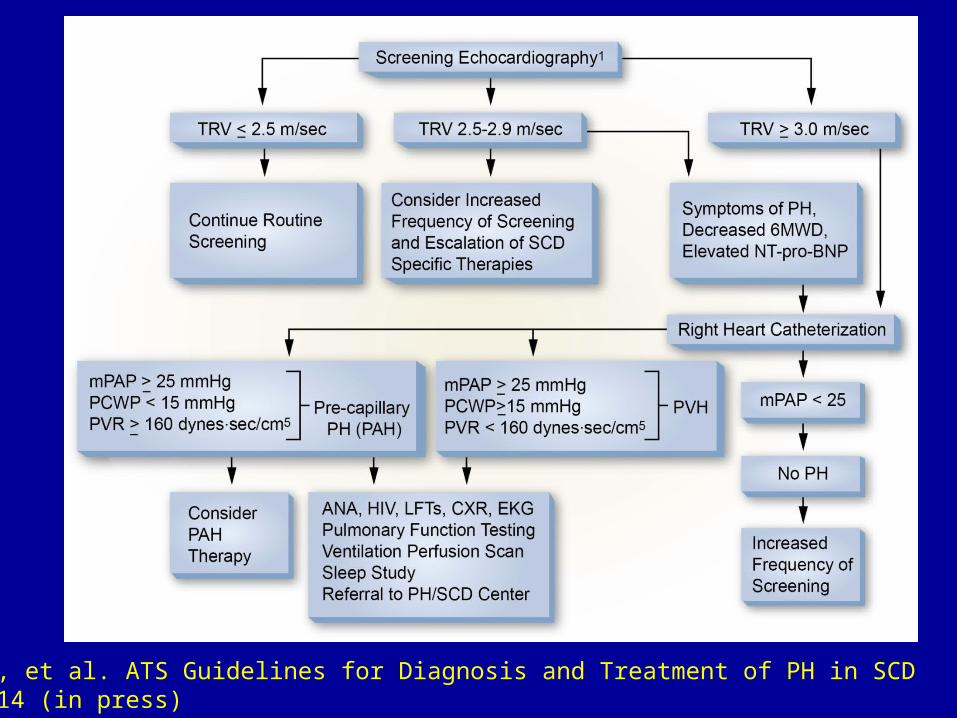
Klings ES, et al. ATS Guidelines for Diagnosis and Treatment of PH in SCD AJRCCM 2014 (in press)
But wait, there’s more
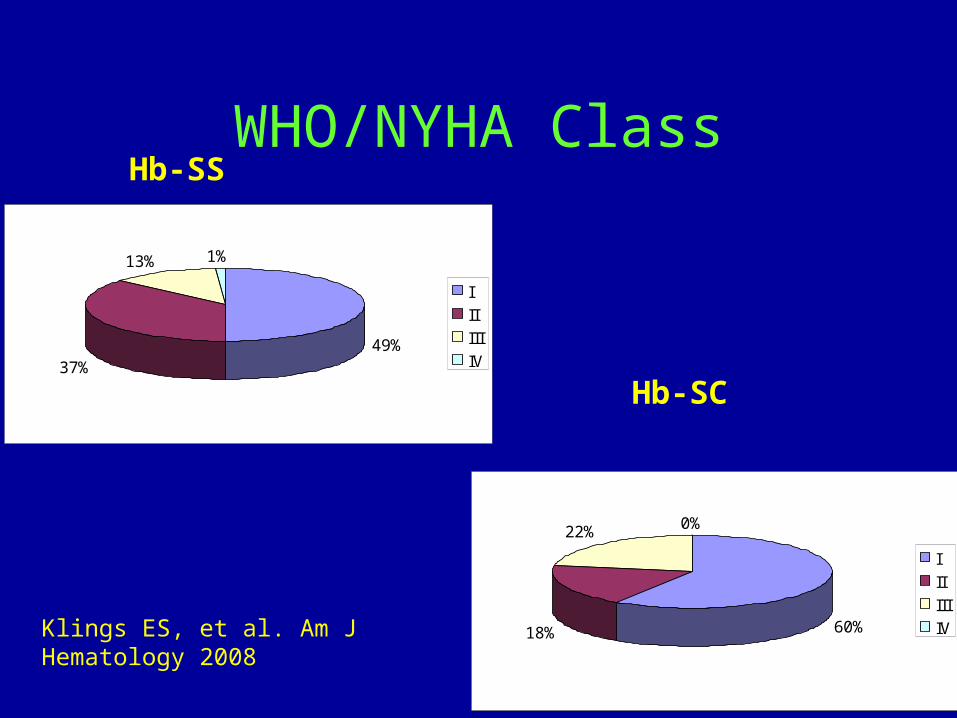
WHO/NYHA ClassHb-SS
Hb-SC
60%18%
22% 0%
I
II
III
IV
49%37%
13% 1%
I
II
III
IV
Klings ES, et al. Am J Hematology 2008
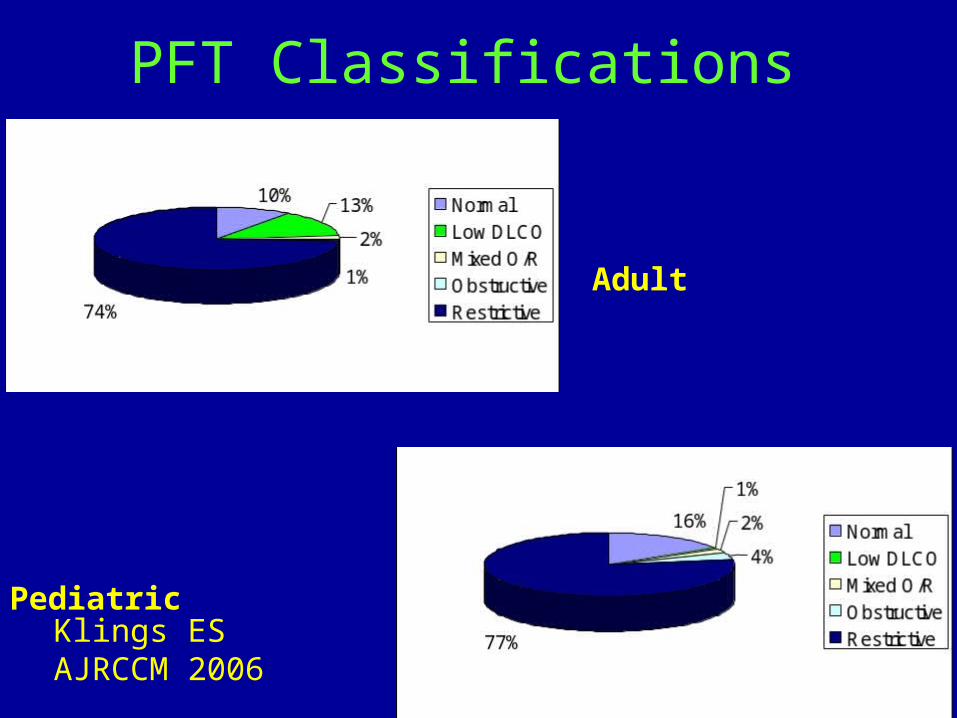
PFT Classifications
Adult
Pediatric
Klings ES AJRCCM 2006
Sleep-Disordered Breathing and SCD
Multiple small studies in kids and adolescents – nocturnal desats in up to 79%Prevalence of OSA – 10-20%Upper airway obstruction related to lymphoid hyperplasiaAdenoidectomy/tonsillectomy- curative in some, but impact on cardiopulmonary outcomes unclearMay be associated with daytime hypoxemia Risk for adults - unknown
Linking Adult And Pediatric SCD-Related Lung Disease
• Link between asthma/ACS in pediatric patients and restrictive disease in adults
• Changes in cardiopulmonary physiology in early adulthood
• Can early intervention prevent PH in SCD?
Pulmonary Fibrosis and SCD
Thought to be part of the spectrum of chronic sickle cell lung disease
Mechanism unknown, may be long-term effect of recurrent episodes of ACS
CT scan – Ground glass infiltrates with mild fibrotic changes
May be associated with PH
Summary
Pulmonary disease is an important cause of morbidity and mortality in SCD
Dyspnea is very common in SCD population, not all of this is due to PH
All SCD adults should be screened annually for PH
Lots of work still needs to be done