Embed Size (px)
Citation preview

Racial-Ethnic Differences in Childhood Asthma Treatment
Eric M. Sarpong and G. Edward Miller
AHRQ Conference September 20, 2011

Introduction
Asthma – chronic, complex and costly health condition – Estimated costs of asthma in the U.S. - $19.7 billion (NHLBI, 2007)
Why childhood asthma medication use?– Recent significant increases in:
Treated prevalence Health care and prescribed asthma drug expenditures (Miller &
Sarpong)– Recent changes in asthma care
Treatment guidelines (NAEPP-EPR3, 2007) - Inhaled corticosteroid (ICS); preferred first-line therapy for persistent asthma
– Changes in use and availability of new pharmacotherapies Increased use of controller medications Decreased use of mono-therapy with relievers
Differences in asthma treatment persists

Pharmaceutical Treatment of Asthma
Recommended treatment depends on asthma severity (NAEPP-EPR3, 2007)
– Controllers (e.g., inhaled corticosteroid) Used in managing asthma symptoms, by
minimizing inflammation and reducing the risk of serious exacerbations
Recommended for all children with persistent asthma
– Relievers (e.g., inhaled short acting beta agonists) Used in managing moderate or severe asthma
attacks by promptly relaxing airway muscles Recommended for all children with intermittent
asthma

Treated Prevalence of Childhood Asthma by Race-Ethnicity, 2005-2008
Source: MEPS, 2005-2008. Estimates for insured children with reported treatment for asthma. Differences from NH Whites significant at p < .05.
All Children NH White NH Black Hispanic0
1
2
3
4
5
6
7
8
9
10
6.47846.2377
8.692
5.834
Per
cent

Use of Controllers Among Children With Treatment for Asthma, 2005-2008
Source: MEPS, 2005-2008. Estimates for insured children with reported treatment for asthma. Differences from NH Whites significant at p < .05.
All Children NH White NH Black Hispanic0
10
20
30
40
50
60
70
80
59.4502
68.6287
44.1524
49.5186
Per
cent

Use of Relievers Only , Among Children with Treatment for Asthma, 2005-2008
Source: MEPS, 2005-2008. Estimates for insured children with reported treatment for asthma. Differences from NH Whites significant at p < .05.
All Children NH White NH Black Hispanic0
5
10
15
20
25
30
35
40
45
30.45
22.9275
42.7624000000001
38.6789
Per
cent
Differences in Treated Prevalence and Use of Asthma Medications
NH Black children - more likely than NH White and Hispanic children to be treated for asthma
NH Black and Hispanic children - less likely than NH White children to use controllers
NH Black and Hispanic children - more likely than NH White children to use relievers only
Previous Research
Large body of literature with mixed evidence on differences in children’s use of asthma medication
Some studies find no differences by race-ethnicity, others do find a difference
Studies differ on a number of dimensions– Time period– Population (e.g., Medicaid, private claims, nationally
representative)– Degree to which they control for differences in underlying
characteristics across groups

Research Objective and Contribution
Research Objective – Examine differential use of asthma medication by race-
ethnicity– Examine extent to which differences in mean predisposing,
enabling and need characteristics explain differences in use
New Contribution – Previous literature limited - Medicaid data, administrative
data or community samples, key variables unavailable– Comprehensive look at differences using nationally
representative data (MEPS)– Provide descriptive information on reasons for differences
and possible approaches to addressing these differences

Analytic Approach
Describe differences in controllers and relievers only use by race-ethnicity
Estimate pooled regression models with binary outcomes (i.e., controllers and relievers only)– Explanatory variables
Predisposing (e.g., socio-demographics, geographic) Enabling (e.g., health insurance, family income/structure
and parental education/employment status) Need (e.g., health status, co-occurring conditions)
Use Oaxaca-Blinder method - decompose differences into:– Explained - differences due to mean differences in
explanatory variables– Unexplained - differences due to differences in
estimated coefficients

Data
Data– 2005-2008 Medical Expenditure Panel Survey (MEPS)
Population studied– Insured children (ages 0-17) with reported treatment for
asthma Treatment = health service use associated with asthma
– Sample size N = 813 NH White children N = 608 NH Black children N = 644 Hispanic children
Drugs – Link MEPS drug data by NDC to the Multum Lexicon– Use generic names to categorize drugs as controllers or
relievers– Measures: any use of controllers and relievers only

Descriptive Results - Differences in Mean Characteristics
NH Black children more likely than NH White children to– Be covered by public insurance, live in an MSA and in the south
(predisposing)– Live in families with low levels of family income, low parental
education, unmarried parent and unemployed parent (enabling)– Be in fair/poor physical health (need)
Hispanic children more likely than NH White children to– Be covered by public insurance, live in an MSA, in the west, have
non-native parents and parents with risky attitudes towards health (predisposing)
– Live in families with low levels of family income, low parental education, unmarried parent, unemployed parent and live in a larger family (enabling)
– Be in fair/poor physical health (need)
Multivariate Results - Predictors of Controller and Reliever Only Use
Positive effects on controller use– Age 5-11, native parents, married parent, fair/poor physical
health, and having treatment for allergies
Negative effects on controller use– Female, MSA, western region, low family income, parental
education, and large family
Positive effects on reliever only use– Female, MSA, western region, native parents, low family
income, and large family
Negative effects on reliever only use– Age 5-11, married parent, fair/poor physical health, and
having treatment for allergies
Results are based on coefficient estimates from pooled linear probability models.

Oaxaca-Blinder Decomposition - NH Whites vs. NH Blacks, Controllers
Important variablesEnabling Low income ≤ High school Family of > 4 Unmarried
Source: MEPS, 2005-2008. Estimates for insured children with reported treatment for asthma. Differences from NH Whites, significant at p < .10.
Total Difference in Controller Use = 24.5%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Unexplained; 12.8
Need; 2.2
Enabling; 8.6
Per
cent
con
trib
utio
n to
gap
in u
se Explained

Oaxaca-Blinder Decomposition Results - NH Whites vs. NH Blacks, Relievers Only
Important variablesEnabling Low income Family of > 4 Unmarried
Source: MEPS, 2005-2008. Estimates for insured children with reported treatment for asthma. Differences from NH Whites, significant at p < .10.
Total Difference in Reliever Only Use = 19.8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Unexplained; 12.2
Need; 1.6
Enabling; 5.7
Per
cent
con
trib
utio
n to
gap
in u
se Explained
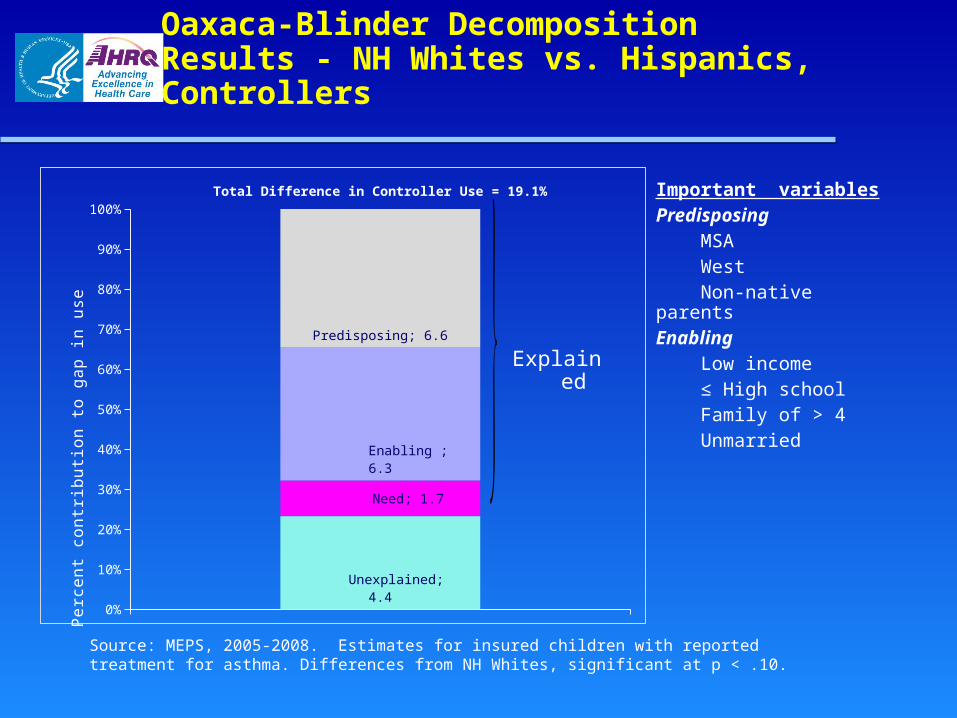
Oaxaca-Blinder Decomposition Results - NH Whites vs. Hispanics, Controllers
Important variablesPredisposing MSA West Non-native parentsEnabling Low income ≤ High school Family of > 4 Unmarried
Source: MEPS, 2005-2008. Estimates for insured children with reported treatment for asthma. Differences from NH Whites, significant at p < .10.
Total Difference in Controller Use = 19.1%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Unexplained; 4.4
Need; 1.7
Enabling ; 6.3
Predisposing; 6.6
Per
cent
con
trib
utio
n to
gap
in u
se Explained

Oaxaca-Blinder Decomposition Results - NH Whites vs. Hispanics, Relievers only
Important variablesEnabling Low income ≤ High school Family of > 4 Unmarried
Source: MEPS, 2005-2008. Estimates for insured children with reported treatment for asthma. Differences from NH Whites, significant at p < .10.
Total Difference in Reliever Only Use = 15.8%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Unexplained; 7.8
Need; 1.2
Enabling ; 4.4
Per
cent
con
trib
utio
n to
gap
in u
se Explained

Interpretation of Oaxaca-Blinder Decomposition Results
Several characteristics in the domains of the behavioral model were associated with – Controller use – Reliever only use
Our model– Explained most differences in:
Controller use for NH Blacks and Hispanics Reliever only use for Hispanics
– Differences in reliever only use for NH Blacks, largely unexplained
Unobservable factors - differences in responses to characteristics, may be important

Limitations and Future Research
Limitations– No measure of asthma severity
Results may change if severity differs across groups
– Non-causal descriptive model Future research
– Depart from linear probability models– Use non-parametric approach
Raking (Pylypchuk and Selden, 2008, JHE)– Follow previous approaches
Kirby et al, 2010 MCRR and Hudson et al, 2007

Conclusions
Non-Hispanic whites: low asthma treated prevalence and reliever only use and, higher controller use
Enabling factors explained some, not all, of the differences in controller and reliever only use for NH Blacks and Hispanics
Predisposing factors explained some of the differences in controller use for Hispanics
Some unobservable characteristics may have also played a role
Results are consistent with studies in other therapeutic classes of drugs and disease areas

References
Miller G.E. and Sarpong E.M. Trends in the Pharmaceutical Treatment of Children’s Asthma, 1997 to 2008. Research Findings No. 31. September 2011. Agency for Healthcare Research and Quality, Rockville, MD. http://meps.ahrq.gov/mepsweb/data_files/publications/
Kirby JB, Hudson J, Miller GE. (2010). Explaining Racial and Ethnic Differences in Antidepressant Use Among Adolescents Med Care Res Rev, 67: 342-363
Crocker D, Brown C, Moolenaar R, Moorman J, Bailey C, Mannino D, Holguin F. (2009). Racial and ethnic disparities in asthma medication usage and health-care utilization: data from the National Asthma Survey. Chest,136(4):1063-71. Epub 2009 Jun 30.
Pylypchuk, Y. and T. M. Selden. (2008). A discrete choice decomposition analysis of racial and ethnic differences in children’s health insurance coverage. Journal of Health Economics 27: 1109-1128.
Chen AY, Escarce JJ. (2008). Family Structure and the Treatment of Childhood Asthma. Medical Care , 46: 174-184 Hudson, J. L., Miller, G. E., & Kirby, J. B. (2007). Explaining racial and ethnic differences in children’s use of stimulant
medications. Medical Care, 45, 1068-1075. National Asthma Education and Prevention Program. Expert Panel Report 3: Guidelines for the Diagnosis and
Management of Asthma: Full Report 2007. Bethesda, MD: National Institutes of Health, US Dept of Health and Human Services, National Heart, Lung, and Blood Institute; 2007.
Shields A, Comstock C, Weiss KB. (2004). Variations in asthma care by race/ethnicity among children enrolled in a state Medicaid program. Pediatrics,113:496 –504.
Finkelstein JA, Lozano P, Farber HJ, et al. (2002). Underuse of controller medications among Medicaid-insured children with asthma. Arch Pediatr Adolesc Med,56(6):562-7.
Lieu TA, Lozano P, Finkelstein J, et al. (2002). Racial/ethnic variation in asthma status and management practices among children in managed Medicaid. Pediatrics,109:857– 865.
Blinder, A. (1973). Wage discrimination: Reduced form and structural estimates. Journal of Human Resources, 8, 436-455.
Oaxaca, R. L. (1973). Male-female wage differentials in urban labor markets. International Economic Review, 14, 693-709.