Embed Size (px)
Citation preview

Inr. 1. Radialion Oncology Biol. Phys Vol 8, pp. 1055-1057 036~3016/82/06oooo-oo$03.00/00 Printed in the U.S.A. All nghts reserved CopyrIght 0 I982 Pergamon Press Ltd
??Brief Communication
RADIATION THERAPY FOR SMALL BOWEL CARCINOMA: REPORT OF THREE PATIENTS AND REVIEW OF THE LITERATURE
GENE KOPELSON, M.D. AND LEONARD L. GUNDERSON, M.D. Department of Radiation Medicine, Massachusetts General Hospital, Boston, MA 02 I I4
The potential role of radiation therapy in the management of localized small bowel carcinoma is reviewed based upon three patients irradiated at a major referral center and seven previously reported patients in the literature. The one patient irradiated postoperatively for gross residual disease has had local-regional disease control for 1.5 years. The two patients irradiated postoperatively in an adjuvant setting are alive without disease at 3.8 and 0.5 years, respectively. Patients with unresectable disease (initially or at recurrence) have fared poorly. Patterns of tumor spread are reviewed, and recommendations on irradiation dose and volume are suggested.
Small intestinal neoplasms, Radiotherapy.
INTRODUCTION
Although several series of patients’,2,3.4,6.8 and literature reviews7,‘” which discuss carcinoma of the small intestines have been reported over the past 25 years, the role of radiation therapy in the management of these patients remains to be defined. We report here the details and results of the radiotherapeutic management of three patients seen at our hospital. We have also reviewed the literature on previously-reported patients in order to determine the potential value of irradiation for this dis- ease.
METHODS AND MATERIALS
From 1962-1979, five patients with small intestine carcinoma were treated at the Department of Radiation Medicine, Massachusetts General Hospital. Two of these patients, who were given only local palliative irradiation because of known distant metastases, were excluded from further analysis. The clinical characteristics, treatment, and results for the remaining three patients, as well as the seven similar potentially-curative patients previously reported in the literature, appears in Table I. All patients had adenocarcinoma, with the exceptions that in one literature report the specific histology, other than “carci- noma”. was not stated (Patient 3).
RESULTS Patients with unresectable disease (initially or at recur-
rence) did poorly. Local disease status after irradiation was assessed in only two patients, and local in-field failure
occurred in each after 4500 and 4000 rad (Patients 8,9). Results appeared to be better, however, with less pre- irradiation tumor burden. The one patient irradiated for gross residual disease had local-regional disease control for I .5 years, while the two irradiated adjuvantly are alive without disease at 3.8 and 0.5 years.
Distant metastases developed in three patients, two of whom had been irradiated for unresectable recurrent disease. In most of the patients from the literature, however, the pattern of failure after irradiation was often not discussed. As a result. the true incidence of distant failures might be higher, especially for those with unre- sectable disease or for those with resectable disease at an advanced pathologic stage.
Of the four patients alive at least two years after completion of irradiation, there has been no instance of small bowel obstruction due to chronic irradiation compli- cations.
DISCUSSION
Two recent literature reviews of prior series of patients found that about two-thirds to three-quarters of the patients with small intestines carcinoma do undergo curative resections7.” although other series demonstrate a lower resectability rate.’ Five-year survival rates, how- ever, even after curative surgery, are only about 20%.‘,7.‘” Of 34 patients in one review in which the lymph node status was mentioned, 24 patients (71%) had positive nodes.‘” To our knowledge, patterns of failure after cura- tive surgery alone have not been described in much detail.
Reprint requests to: Dr. G. Kopelson, Dept. of Radiation Oncology, Salem Hospital, 81 Highland Ave., Salem, MA 01970. Acknowledgemmts-The authors would like to thank Mindy
and Barry P. Kopelson for their help in the preparation of this manuscript.
Accepted for publication I8 January 1982.
1055
1056 Radiation Oncology 0 Biology 0 Physics June 1982, Volume 8, Number 6
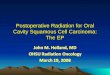
Table I. Radiation therapy results for small bowel carcinoma
Patient no. Age Sex
Postoperative. adjuvant I (present report) 40
M 2’ 46
F
Postoperatwe. gross residual 3’ 51
F
Initially unresectable 4x 0
0 sp 48
M 69 37
M 7’ 74
F
Recurrent. unresectable 8 (present report) 58
M 9 (present report) 52
M I o4 45
M
Irradiation details Follow-up status
Site Rad/
Modality fractions Technique Chemo.
J IOX 5.040/28 Tumor bed + 5-FU (proximal) nodes(4-held) CCNU
D 0 3.900/o 0 None
D 60,” 5,000/30 AP-PA 5-FU I .5y LC No- A.NED
D 0 O/O 0 None
D 0 O/O 0 None
D 0 O/O 0 None
D 0 5.000/0 0 5-FU
2X 4,500/23 AP-PA to 5-FU tumor bed
2X 4,000/ 20 AP-PA to 5-FU tumor bed
0 O/O Radium None implant
Local Survival* disease status
.-___
Distant metastases’!
3y9m LC No- A.NED
6m LC No- A,NED
4.5y 0
lylm 0
9m 0
2Y 0
2ylOm LF-reexplored Yes
3m LF-post Yes
lY 0 0
J = Jejunum; D = Duodenum; LF = Local failure; LC = Local control; A,NED = Alive. no evidence of disease; AP-PA = Anterior-posterior parallel-opposed; IOX = IO MeV linear accelerator; 2X = 2 MeV Van de Graaf generator; 0 = Data unavailable.
*After completion of irradiation. Note: Patient No. I had a Cz primary, and Patient No. 2 had a B, primary.
The only clinicopathologic series’ reported that the inci- dence of death due to disease rose from 40% of those five patients with disease confined to the bowel wall, to 60% of 38 patients with disease extending beyond the serosa. Similarly, 45% of 22 patients with negative nodes died of disease, as compared to 88% of eight with positive nodes.’
Of the 10 irradiated patients in Table 1, four survived at least two years after completion of irradiation. This rate appears to compare favorably to the 33% two-year survival rate after curative surgery alone in one series.’ This is especially true considering the advanced disease status of most of the patients who received irradiation.
Although patient numbers are too small to make definite conclusions, local disease control after irradiation appeared to be related, as expected, to the pre-irradiation tumor volume. The two patients with unresectable disease who had their local disease assessed after irradiation (Patients 8,9) each developed in-field failure after 4500 and 4000 rad, respectively. Local disease was controlled, however, for varying follow-up times after irradiation for gross-residual disease in one patient (Patient 3) and for adjuvant irradiation in two others (Patients 1,2).
DoselJield recommendations When there is unresectable disease or gross residual
disease in the small bowel mesentery or adjacent struc-
tures, the radiation tolerance of the small bowel would usually preclude delivering a tumoricidal irradiation dose. For select patients with residual disease after resection, a boost dose could possibly be delivered via specialized techniques, such as with an implant or with intraoperative irradiation, where the small bowel would be out of the boost field. For unresectable disease one approach might be preoperatic irradiation followed by total or subtotal resection k intraoperative irradiation.
The major role of radiation therapy appears to be that of adjuvant treatment. The doses required to sterilize microscopic adenocarcinoma elsewhere (ie 4500-5000 rad in 180-200 rad fractions) approach tolerance of the small bowel. We would recommend carefully defined postoperative irradiation to high risk patients.
Patients with positive lymph nodes close to the proxi- mal vessel ligation point, or those with many positive peri-tumor nodes in which the next echelon nodes have not been assessed, should probably receive postoperative irradiation to the proximal draining nodes. For proximal d,uodenal primaries, which drain via the superior and inferior pancreaticuoduodenal systems, the celiac, superior mesenteric and probably porta hepatic nodes should be included. For lesions distal to the second part of the duodenum, drainage is to the superior mesenteric chain.
Tumor bed inclusion is recommended for many

Radiation therapy for small bowel carcinoma ??G. KOPELSO~ AYD L. L. GIJWDtRSol 1057
patients with other gastrointestinal adenocarcinomas in whom the tumor has extended through the wall (B2,3 or C?,,), especially for lesions which are infra- or retro- peritoneal. The second and third portions of the duode- num are retroperitoneal. A tumor bed boost alone might be considered for these patients if their primaries extend through the wall. Because the small bowel is mainly intra-peritoneal, extension through the small bowel wall probably places the entire abdomen at risk. In institutions studying whole abdominal irradiation for gastrointestinal adenocarcinomas which extend through the wall for intra-peritoneal primaries (e.g. Bz,l or C,,, lesions of the transverse colon), such a treatment policy might be instituted for patients whose small bowel carcinomas extend through the wall to a peritoneal surface.
It should be emphasized that these dose/volume rec- ommendations can only be considered speculative since these data arc based on few patients.
Chemotherapy was given to five patients in Table I. Although chemotherapy results have not been reported in
any detail for these patients,‘.’ one could make an analogy to adenocarcinomas elsewhere in the gastrointesinal tract and consider concomitant S-Flouorouracil for patients with unresectable or residual disease in whom radiation doses are compromised as previously discussed.
CONCLUSION
Based upon very few reported patients, the major role of irradiation in this clinical setting appears to be that of postoperative treatment to those patients who have a high risk for failing. Therefore patients with positive nodes (many nodes close to the tumor in which next echelon nodes are not assessed, or positive nodes close to the vessel ligation site) should probably bc treated to the next echelon site(s). For retroperitoneal primaries. the tumor
bed should probably be included for lesions which extend through the wall. Whole abdomen irradiation might be considered for most other lesions if they extend through the entire wall to a peritoneal surface.
REFERENCES 1.
2.
3.
4.
5.
6.
Almwark, A., Andersson. A., Lasson, A.: Primary carci- noma of the duodenum. Ann. Surg. 191: 13-18, 1980. Bridge, M.F., Pet%, K.H.: Primary adenocarcinoma of the jejunum and ileum. Cancer 36: 1876-I 887, 1975. Darling, R.C.. Welch, C.E.: Tumors of the small intestine. N. Eng. J. Med. 260: 397-408. 1959. Dunhill. T.: Carcinoma of the third part of the duodenum. Brit. J. S’urg. 40: I3-- 18, 1952. Edman. P.: Duodenal cancer. Acta. C‘hir. Sumd. 139: 759 762. 1973. Moss, W.M.. McCart. P.M. Juler. G., Miller, D.R.: Pri-
7.
8.
9.
IO.
mary adenocarcinoma of the duodenum. ,-frch. .S’urg. 108: x05- x07, 1974.
Sakker. S.. Ware, C.C.: Carcinoma of the duodenum. Hrir J. Surg. 60: X67 872. 1973.
Serrano. J.F., McPeak. C‘J.: Primary neoplasma of the duodenum. Surgrrj, 59: I99 202, 1966
SpinnaT&. A.J., Gillesbby, W.J.. Primary malignant nco- plasms of the duodenum. .-lnr. .Vurg. 29: 405 4 12, 1963.
Spira, IA., Ghazi. A.. Wolff. W I.: Primary adenocarci- noma of the duodenum. C’anwr 39: I72 I 1726. 1977.

















![CARCINOMA ERYSIPELOIDES MIMICKING RADIATION … · Carcinoma erysipeloides (CE) is an uncommon cutaneous metastasis arising from visceral carcinoma [1]. It is the result of spread](https://img.pdfslide.net/doc/110x75/5feca92ebacb9554d41ee682/carcinoma-erysipeloides-mimicking-radiation-carcinoma-erysipeloides-ce-is-an-uncommon.jpg)