Embed Size (px)
Citation preview

Thorax (1971), 26, 696.
Radiological evaluation of post-tracheostomy lesionsALEXANDER S. MACMILLAN, A. EVERETTE JAMES, JR.,
FREDERICK P. STITIK, and HERMES C. GRILLO
Departments of Radiology, Massachusetts Eye and Ear Infirmary, Boston, Mass. and Johns Hopkins Hospital.Baltimore, Maryland and Division of Thoracic Surgery, Massachusetts General Hospital, Boston, Mass., U.S.A.
Post-tracheostomy lesions are becoming more commonplace and surgical techniques for definitiverepair of these abnormalities are being developed. These lesions, in general, occur at two sites.the proximal lesions at the tracheostomy incision and the distal lesions 15 to 2-5 cm inferior inthe area of the tracheostomy balloon cuff. Granuloma formation, stenosis, tracheomalacia, andperforation of the tracheal wall have been encountered in our experience. Clinical symptomsdepend upon the type and location of the lesion as well as on the patient's awareness and physicalactivity. Radiological evaluation offers an accurate method to depict the anatomical and physio-logical alterations. This radiological assessment should begin with routine postero-anterior andlateral chest radiographs followed by fluoroscopy. Laminograms and special oblique views are
often helpful. Contrast tracheograms using powdered tantalum allow good mucosal detail as wellas excellent delineation of structural and physiological abnormalities.
The more common use of various methods ofassisted respiration coupled with the many modi-fications of tracheostomy tubes has led to anincreased incidence of post-tracheostomy compli-cations. Preoperative evaluation of these lesionsshould include delineation and documentation ofanatomical alterations as well as assessment ofthe significance of the physiological abnormalities.Many of these determinations can be made byradiological methods. This communication ad-dresses itself to the orderly sequence of radio-logical evaluation of these problems, emphasizingthe expected risk and potential value of each typeof examination.
MATERIALS AND METHODS
Because of the particular surgical interest of oneof us (H.C.G.), a large number of patients werereferred to the Massachusetts Eye and EarInfirmary and Massachusetts General Hospitalfor evaluation and definitive repair of post-tracheostomy lesions. We have also been inter-ested in a new contrast agent for radiographicevaluation of post-tracheostomy lesions and oneof us (F.P.S.) has recently engaged in researchand clinical evaluation of the use of powderedtantalum. From this experience (1966-71) aflexible protocol for evaluation of post-trache-ostomy lesions has evolved and is presented.
POST-TRACHEOSTOMY LESIONS
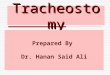
In the radiological evaluation of post-trache-ostomy complications, the expected sequence andpathological alterations must be kept in mind.Proper radiological studies should be requestedaccordingly. Generally, the lesions will occur intwo sites in the trachea at the site of the trache-ostomy incision and in the area of the trache-ostomy balloon cuff. The proximal lesions occur-ring at the tracheostomy incision sites will mostoften involve the anterior and lateral trachealwalls and will consist of stenosis, granulationmass formation, and, occasionally, tracheomal-acia (Meade, 1961; Murphy, MacLean, andDobell. 1966). Those distal post-tracheostomylesions which occur in the area of the ballooncuff consist of (Fig. 1) stenosis, granulation massformation, tracheomalacia, and perforation(Pearson, Goldberg, and da Silva, 1968; Stiles,1965).The histological changes of both proximal and
distal tracheal lesions are comparable and may beconcomitantly discussed. After placement of thetracheostomy tube in the trachea, inflammatoryhistological changes are noted in 24 to 48 hours(Atkins, 1964: Cooper and Grillo, 1969). Thisinflammatory condition leads to a superficialtracheitis and mucosal ulceration within the firstweek (Glas, King, and Lui, 1962). Continued
696
copyright. on A
ugust 30, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.26.6.696 on 1 Novem
ber 1971. Dow
nloaded from

Radiological evaluation of post-tracheostorny lesions
3
1Stenosis
FIG. 1. Distal post-tracheostomy lesions that occur in the area of the balloon cuff.
inflammation and superimposed infection mayresult in deeper mucosal ulcerations and exposureof the underlying cartilage in one to three weeks(Pearson et al., 1968). As the cartilage is exposedchondritis is seen. In two to three weeks this maycause fragmentation and total loss of the carti-lagenous supporting structures. The end resultsare a combination of destructive and reparativeprocesses coexisting in a segment of the trachea(James et al., 1970a).The proximal tracheal lesion probably begins
from the mechanical abrasion of the trachealmucosa by the tracheostomy tube (McLellano,1965). As the tube is inserted the outer convexityrests upon the anterior tracheal wall superiorlyand the posterior tracheal wall inferiorly (Fig.2a,b). When the tracheostomy tube is then attachedto a mechanical breathing apparatus, the rigidityof this placement is enhanced as are the shearingforces between the tracheostomy tube and thetracheal mucosa (Lu, Tamura, and Koobs, 1961;Meade, 1961). Drying of the tracheal mucosa(because the upper respiratory passages that pro-vide moisture are bypassed) and superimposedinfection are undoubtedly contributory (Stiles,1965). Attempts at healing and repair in the areaof the tracheostomy site may be seen as massesof graulation tissue formation, especially on theanterior wall, and asymmetrical or cicatricialstenosis due to fibrous healing (Fraser and Bell,1967).The distal post-tracheostomy lesions most often
occur 1 5 to 3-0 cm distal to the site of trache-ostomy insertion and usually involve a 2-5 to 3 0cm segment of the trachea (Deverall, 1967:Flavell, 1959; Grillo, 1968). The character ofthese lesions is related to the type of ballon cuffused. The rigidity of the balloon wall determinesthe amount of intraluminal pressure necessary toensure an airtight system required for assistedrespiration (Grillo, 1969; Lu et al., 1961). Toprevent air leakage around the balloon cuff, witha thick-walled balloon intraluminal pressures of180 to 250 mmHg must be maintained. Only 10to 30 mmHg pressure is required if a thin-walledballoon is used (Cooper and Grillo, 1969; Jameset al., 1970b). The mechanism by which thick- andthin-walled cuffs attain an airtight seal are alsodifferent. A thick-walled balloon distorts thetrachea to conform to the shape of the balloon.Thin-walled balloons will easily adapt or conformto the irregularly shaped space between thetracheal lumen and the tracheostomy tube (Gib-son, 1967). The lateral pressure of the balloon cuffacting as a right-angle force to the mucosa of thetracheal wall is the major cause of distal post-tracheostomy lesions (Grillo, 1968; Johnston,Wright, and Hercus, 1967). The lateral force ofthe balloon cuff exceeds capillary pressure in thetracheal mucosa and causes necrosis and super-ficial mucosal loss. Disruption of the mucosalbarrier facilitates superimposed infection, chon-dritis, and loss of supporting structures. With lossof the more rigid cartilagenous support, further
697
copyright. on A
ugust 30, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.26.6.696 on 1 Novem
ber 1971. Dow
nloaded from

698 Alexander S. Macmnillan, A. Everette James, Jr., Frederick P. Stitik, and Hermeles C. Grillo
a;;;. z.D
m.j
_-rS w sE
;w jo.X.. . * J,v -A {. f . . , . . - .
* iD -.. ...
- L. ,S! s,
t - ;e /s ,5 -F ,
! .-:,:s5.\. \es Q ,
!l .'t B
I)1
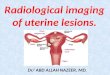
FIG. 2 (a). Anatomical relationship of trachea to cuffedtracheostomy tube. (A) Area of proximal lesion; anteriorlyand superiorly tracheostomy tube rests against anteriortracheal utvall. Posteriorly and inferiorly convexity oftracheostomy tube presses against posterior trachealmucosa. (B) Area of distal lesions at site of balloon cuff.(b). Oblique radiograph demonstrating area of proximallesions. Vertical arrow indicates area of granulomaformation just superior to tracheostomy tube. Large arrow at convexity of tracheostomy tube asto posterior tracheal wall. Row of small horizontal arrows demonstrates distal anterior tracheal wall.
overflation of the balloon cuff is necessary to pro-duce an airtight seal.
Perforation of the tracheal wall is most often aresult of localized pressure necrosis of the distaltracheostomy tube tip (Flege, 1967). The ballooncuff may be placed too proximally, causing theballoon to act as a fulcrum. The distal trache-ostomy tube tip presses into the tracheal wallcausing localized necrosis and perforation. Per-foration may result in a tracheo-oesophagealfistula or, more acutely, mediastinitis.
CLINICAL SYMPTOMS The onset of severity ofclinical symptoms is highly variable and dependsupon the type of lesion present, as well as on thepatient's awareness and physical activity. Patientsare usually removed gradually from the respirator,then the balloon-cuffed tracheostomy tube isreplaced by one without a balloon cuff (sometimesfollowed by a fenestrated type). Later, the tubeis removed and the tracheostomy site is eventuallyclosed (James et al., 1970). However, this sequenceof events may be dramatically altered if post-tracheostomy lesions are present.
............. ..... . . .: -Jp .; ...0 .....: :; :t.,.... i..............
W:i: i;
.... ... .... ..
it lies adjacent
Granulation tissue formation at the trache-ostomy site may effect a ball-valve type of mech-anism causing intermittent obstructive episodes ofacute respiratory distress (James et al., 1970a, b).After removal of the tracheostomy tube, fibroushealing may occur over a period of months, lead-ing to narrowing of the tracheal lumen due tostenosis. This narrowing, in our experience, mayoccur distally or proximally but is most oftenencountered at the site of the balloon cuff. Thepatient may have a variable symptom-free periodafter removal of the tracheostomy tube and laterexperience difficulty in raising secretions (Grillo,1968; Grillo, 1969). As the granulation tissueformation and healing by fibrosis progresses, thepatient may experience respiratory stridor (Pearceand Walsh, 1961).
In patients with significant tracheomalacia, atthe time of removal of the cuffed tracheostomytube, immediate obstructive symptoms may beobserved (Johnston et al., 1967). The loss ofrigidity of the tracheal wall may result in para-doxical motion and apposition of the trachealwalls with respiration. Often the walls are held
copyright. on A
ugust 30, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.26.6.696 on 1 Novem
ber 1971. Dow
nloaded from

Radiological evaluation of post-tracheostomy lesions
open by the balloon cuff. Removal will result incollapse of the tracheal walls and closure of thetracheal lumen. Immediate reinsertion of thetracheostomy tube to restore the airway is neces-sary.
Perforation of the tracheal wall can causeimmediate acute symptoms. Concomitant erosionof a large thoracic vessel or mediastinitis are life-threatening circumstances that require immediatetherapy and do not allow a lengthy pretreatmentevaluation.
RADIOLOGICAL EVALUATION The starting point inany radiological evaluation of the tracheo-bronchial tree is a properly exposed uprightpostero-anterior and lateral chest radiograph. Asurvey examination of this type may not optim-ally demonstrate the tracheal lesion, but willdecrease the probability of overlooking a lesionin other portions of the respiratory tract. The
FIG. 4. Oblique radiograph of area of granulation tissueformation. Anterior tracheal wall is irregular andencroaches upon tracheal ain- column. Minimal inward-leviation of the posterior tracheal wall.
chest radiograph should be followed by fluoro-scopic examination of the trachea and bronchi aswell as evaluation of diaphragmatic and chestwall motion. At fluoroscopy selected radiographsof the particular area of interest can be obtained.Selected fluoroscopic radiographs during inspir-ation and expiration are useful in determiningthe effective tracheal lumen in the area of stenosisor granulation tissue formation. Radiographsduring respiration under fluoroscopic control aremost useful in the assessment of patients withsuspected tracheomalacia (James et al., 1970). Theloss of cartilagenous support causes that trachealsegment to collapse with inspiratory effort (Fig.3). Paradoxical motion of the tracheal wall can beobserved. If the balloon cuff is in place at thebeginning of the evaluation, the patient should befluoroscoped to compare the diameter of the
FIG. 3. Oblique radiograph showing area of tracheomalacia balloon to the width of the tracheal air column.(large double arrows), inward deviation of tracheal walls, This is done to determine if the balloon is over-and narrowing of tracheal lumen with respiration. White inflated and greatly exceeds the diameter of thearrow indicates patient's right side. tracheal lumen and if the balloon is holding the
699
copyright. on A
ugust 30, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.26.6.696 on 1 Novem
ber 1971. Dow
nloaded from

700 Alexander S. Macmillan, A. Everette James, Jr., Frederick P. Stitik, and Hermw1es C. Grillo
trachea open. The balloon cuff is then removedbut only after preparations have been made forimmediate reinsertion.Normally the tracheal walls will appear as thin,
parallel, soft tissue densities. With granulationtissue formation, thick irregular masses may bedetected fluoroscopically and their extent care-fully delineated by appropriate selected radio-graphs (Fig. 4). With fibrosis the tracheal wallswill be seen to deviate inward, narrowing theeffective tracheal lumen. At fluoroscopy thisnarrowing of the lumen will not appear to changedramatically with respiration. If tracheomalaciais present, the air column within the trachea willchange markedly with respiration and the softtissue of the tracheal walls will move outwardand inward.
Following fluoroscopic evaluation of thetracheobronchial tree selected radiographs of theabnormal areas should be obtained. For proximallesions at the tracheostomy site a lateral neckradiograph using soft tissue technique is often themost useful projection (Fig. 5). Lesions involvingthe lateral wall are often depicted only on theanteroposterior radiograph, however. With thetypical granulation mass formation, often referredto as a 'granuloma ball', the amount of air spacein the trachea posterior to this lesion should be
e........
FIG. 5. Late, al neck radiograph: soji tissue detail optimizesdemonstration of the granutloma mass (obliquie arrow)and slight inward deviation of'the posterior tr-acheal wtaIl(horizontal arrows).
FIG. 6. Oblique radiograph demonstrates relation ofgranuloma mass to posterior tracheal itall. Small liumenis indicated (arrow).
FIG. 7. Oblique radiograph eliniinates overlying osseousstructures and optimally demolistrates minimal inwarddeviation of tracheal walls.
copyright. on A
ugust 30, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.26.6.696 on 1 Novem
ber 1971. Dow
nloaded from

Radiological evaluation of post-tracheostomy lesions
determined (Fig. 6). Occasionally, oblique viewsmust be obtained to radiograph the 'granulomaball' and posterior tracheal air column tangen-tially. Also the presence of associated stenosis ortracheomalacia must be recognized to decidewhether or not transtracheal removal of thegranulation mass will provide definitive therapy(Pearson et al., 1968).
Distal tracheal lesions in the area of the ballooncuff are often obscured by overlying osseous andsoft tissue structures. Oblique radiographs pro-vide optimum delineation of the lesions (Fig. 7)which may not be apparent with postero-anteriorand lateral radiographs even using a high kilo-voltage technique.
Laminography is a very useful radiographicmodality to enhance anatomical detail at aselected depth and location. Multiple radiographsat depths of optimal resolution in more than oneplane often provide an accurate assessment ofthe size, configuration, and location of a lesion(Fig. 8). Laminograms are useful in depicting the'mass-like' nature of granulation tissue formation(James et al., 1970). Occasionally, dystrophiccalcification may be seen by laminography whenit is not seen on plain radiographs.We have been very conservative in our attitude
towards the use of contrast media in the radio-graphic evaluation of tracheal lesions (James etal., 1970). Positive contrast compounds that con-
tain iodine or barium may, at times, causedeleterious effects on the respiratory function ofpatients with post-tracheostomy lesions. Large
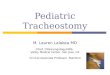
FIG. 8. Laminogram optimizes visualization of the tracheallumen in the plane offocus.
oIG. 9. Oblique fluoroscopic radiograph with tantalum obtained duringinspiration. There was increased mobility of the posterior trachealwall indicating tracheomalacia (after open heart surgery).
701
copyright. on A
ugust 30, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.26.6.696 on 1 Novem
ber 1971. Dow
nloaded from

702 Alexander S. Macmiiillan, A. Everetle James, Jr., Frederick P. Stitik, and Hermes C. Grillo
amounts of radiographic contrast will severelycompromise the airway in these patients withdisastrous results. In addition, oily contrastagents coat the mucosa poorly and may induceacute inflammation locally. Therefore, we havein the past recommended their use only whenother methods have failed and then in very smallamounts. Because of these objections to iodineand barium contrast agents we, among others,have investigated the use of powdered metallictantalum (Hinchcliffe et al., 1970).Tantalum is chemically inert, non-toxic, and
very radiodense. The finely powdered tantalum(0.5 ,u particle size) coats the mucosa and adheresto its surface despite forceful respiratory move-ments (Nadel, Wolfe, and Graf, 1968). The lackof toxicity as well as the small volume necessaryfor a tracheogram (0.2 to 0.5 ml) has resulted inno adverse effect in any patient we have examined.Tantalum is cleared rapidly via mucociliary
action (Nadel et al., 1970). Delayed radiographstaken six hours after the tracheogram have shownno residual tantalum. After proper premedication
FIG. 10. Oblique radiograph demonstrates a sharplydefined area of tracheal stenosis. The granular appearanceof the tantalum in the area of stenosis represents markedirregularity oJ the mucosa with leucoplakia (after openheart surgery).
and local anaesthesia, tantalum is insufflated intothe trachea through a catheter. The deposition oftantalum is controlled fluoroscopically. Fluor-oscopic and conventional radiographs includingoblique, frontal, and lateral views are obtained.Fluoroscopic radiographs during respiratorymovements have shown increased mobility ofsegments with tracheomalacia (Fig. 9). This hasalso been documented by cine examination. Thedelineation of the structural abnormality as wellas the fine mucosal detail have been excellent (Fig.10).
CONCLUSION
Decisions regarding the proper therapy for post-tracheostomy lesions depend upon proper assess-ment of the alterations of anatomy and physi-ology. Pulmonary function studies and bronch-oscopy are mandatory and provide valuableinformation. Many functional and structuraldeterminations may be made by proper use ofradiological techniques. Static radiographs,laminograms, and contrast tracheograms withfluoroscopic monitoring allow anatomical andphysiological assessment using the same diag-nostic technique. A three-dimensional delineationof the abnormalities is possible, thus allowing forproper planning of the surgical approach. Com-munication between the physician primarilyresponsible for the care of the patient and hisradiological consultant will add greatly to theaccuracy of this evaluation.
REFERENCESAtkins, J. P. (1964). Tracheal reactions following the use of
cuffed tracheotomy tubes. Ann. Otol. (St. Louis), 73,1124.
Cooper, J. D., and Grillo, H. C. (1969). The evolution oftracheal injury due to ventilatory assistance throughcuffed tubes: a pathologic study. Ann. Surg., 169, 334.
Deverall, P. B. (1967). Tracheal stricture following tracheos-tomy. Thorax, 22, 572.
Flavell, G. (1959). Resection of tracheal stricture followingtracheotomy, with primary anastomosis. Proc. roY.Soc. Med., 52, 143.
Flege, J. B., Jr. (1967). Tracheoesophageal fistula caused bycuffed tracheostomy tube. Ann. Surg., 166, 153.
Fraser, K., and Bell, P. R. F. (1967). Distal tracheal stenosisfollowing tracheostomy. Brit. J. Surg., 54, 302.
Gibson, P. (1967). Aetiology and repair of tracheal stenosisfollowing tracheostomy and intermittent positivepressure respiration. Thorax, 22, 1.
Glas, W. W., King, 0. J., Jr., and Lui, A. (1962). Complica-tions of tracheostomy. Arch. Surg., 85, 56.
copyright. on A
ugust 30, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.26.6.696 on 1 Novem
ber 1971. Dow
nloaded from

Radiological evaluation of post-tracheostomy lesions
Grillo, H. C. (1968). The management of tracheal stenosisfollowing assisted respiration. J. thorac. cardiovasc.Surg., 57, 52.(1969). Surgical approaches to the trachea. Surg.
Gynec. Obstet., 129, 347.Hinchcliffe, W. A., Zamel, N., Fishman, N. H., Dedo, H. H.,
Greenspan, R. H., and Nadel, J. (1970). Roentgeno-graphic study of the human trachea with powderedtantalum. Radiology, 97, 327.
James, A. E., Jr., Macmillan, A. S., Eaton, S. B., Grillo, H. C.(1970a). Roentgenology of tracheal stenosis resultingfrom cuffed tracheostomy tubes. Amer. J. Roentgenol.,109, 455., MacMillan, A. S., Jr., Eaton, S. B., Janower, M. L.,and Grillo, H. C. (1970b). Radiological considerationsof stenosis and granuloma at the site of tracheostomy.Radiology, 96, 513.
Johnston, J. B., Wright, J. S., and Hercus, V. (1967). Trachealstenosis following tracheostorny. J. thorac. cardiovasc.Surg., 53, 206.
Lu, A. T., Tamura, Y., and Koobs, D. H. (1961). The path-ology of laryngotracheal complications. Arch. Otolaryng.,74, 323.
McLellano, R. M. (1965). Complications of tracheostomy.Brit. med. J., 2, 567.
Meade, J. W. (1961). Tracheotomy-its complications andtheir management. A study of 212 cases. New Engi. J.
Med., 265, 519.Murphy, D. A., MacLean, L. D., and Dobell, A. R. C.
(1966). Tracheal stenosis as a complication of tracheos-tomy. Ann. thoracic Surg., 2, 44.
Nadel, J. A., Wolfe, W. G., Graf, P. D. (1968). Powderedtantalum as a medium for bronchography in canine andhuman lungs. Invest. Radiol., 3, 229.
Youker, J. E., Zamel, N., Austin, J. H. M.,Hinchcliffe, W. A., Greenspan, R. H. and Wright, R. R.(1970). Powdered tantalum: a new contrast medium forroentgenographic examination of human airways. Newt-Engl. J. Med., 283, 281.
Pearce, D. J., and Walsh, R. S. (1961). Respiratory obstruc-tion due to tracheal granuloma after tracheostomy.Lancet, 2, 135.
Pearson, F. G., Goldberg, M., and da Silva, A. J. (1968).Tracheal stenosis complicating tracheostomy withcuffed tubes. Arch. Surg., 97, 380.
Stiles, P. J. (1965). Tracheal lesions after tracheostomy.Thorax, 20, 517.
703
copyright. on A
ugust 30, 2020 by guest. Protected by
http://thorax.bmj.com
/T
horax: first published as 10.1136/thx.26.6.696 on 1 Novem
ber 1971. Dow
nloaded from