Embed Size (px)
Citation preview
Joshua Galanter, HMS IIIGillian Lieberman, MD April 2002
Radiographic Manifestations of ARDS
and its SequelaeJoshua Galanter, HMS III
Gillian Lieberman, MD
22
Joshua Galanter, HMS IIIGillian Lieberman, MD
Patient Presentation: DFDF is 21 year-old female brought in to the ED by EMS for a near drowningWas on her way to a wedding when she drove off a 30-foot high bridgeFell into brackish, fresh waterHad a 10 minute submersion timeUpon extraction, was reported to be vomiting and have an agonal breathing patternEMS was unable to establish an airway
33
Joshua Galanter, HMS IIIGillian Lieberman, MD
DF: Physical ExamVitals
Temperature 91.2, rectallyBP: 109/35Pulse: 100Respiratory Rate: 4O2 Sat: 75% on non-rebreather
HEENT: notable for some lacerationsChest: Coarse breath sounds, bilaterally; no flail chestCV: RRR; pulses 2+ throughoutAbd: NT/NDNeuro: PERRL, 8 → 7 mm, bil. Moving all extremitiesSpine: No tenderness, contusions, or step-offsSkin: Several lacerations
44
Joshua Galanter, HMS IIIGillian Lieberman, MD
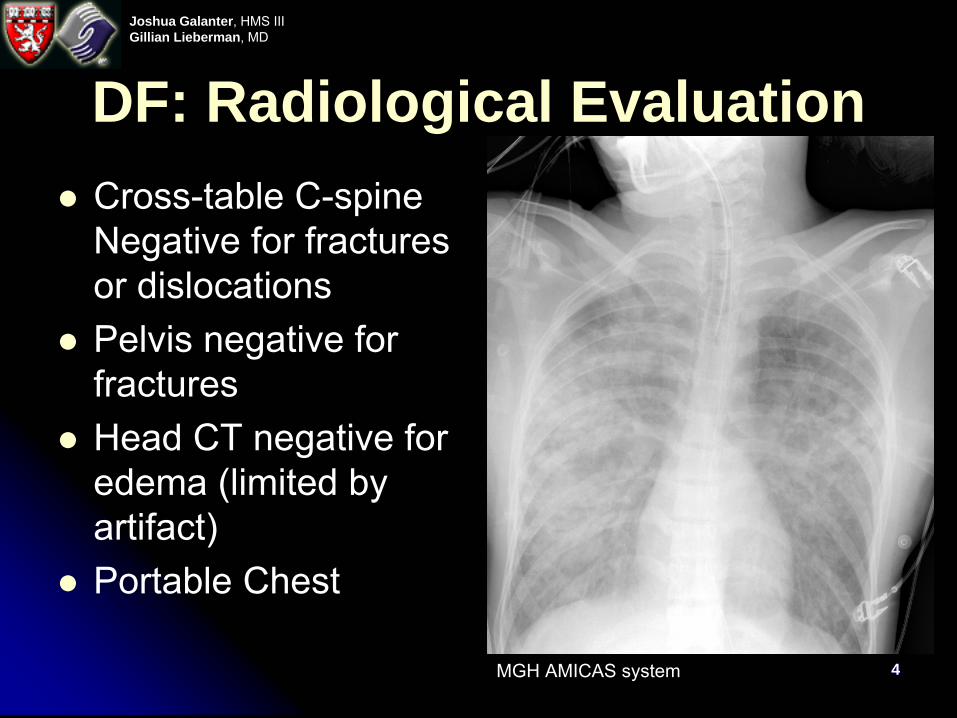
DF: Radiological EvaluationCross-table C-spine Negative for fractures or dislocationsPelvis negative for fracturesHead CT negative for edema (limited by artifact)Portable Chest
MGH AMICAS system
55
Joshua Galanter, HMS IIIGillian Lieberman, MD
AgendaARDS: an introductionNormal pulmonary capillary circulationPathophysiology of ARDSRadiographic appearance of ARDSDifferential diagnosis for diffuse alveolar pulmonary infiltratesSequelae of ARDS on radiographsSummary
66
Joshua Galanter, HMS IIIGillian Lieberman, MD
ARDS: an introductionARDS = Acute Respiratory Distress SyndromeConsensus criteria (Bernard, et. al., 1994):
Acute onsetBilateral Infiltrates on chest radiographyPulmonary artery wedge pressure ≤ 18 mmHg or absence of clinical evidence of left atrial hypertensionPaO2/FiO2 ≤ 200PaO2/FiO2 ≤ 300 = Acute Lung Injury
Incidence between 10 and 75 per 100,000Mortality approx. 35%, down from 50 – 60% over the last 15 years
77
Joshua Galanter, HMS IIIGillian Lieberman, MD
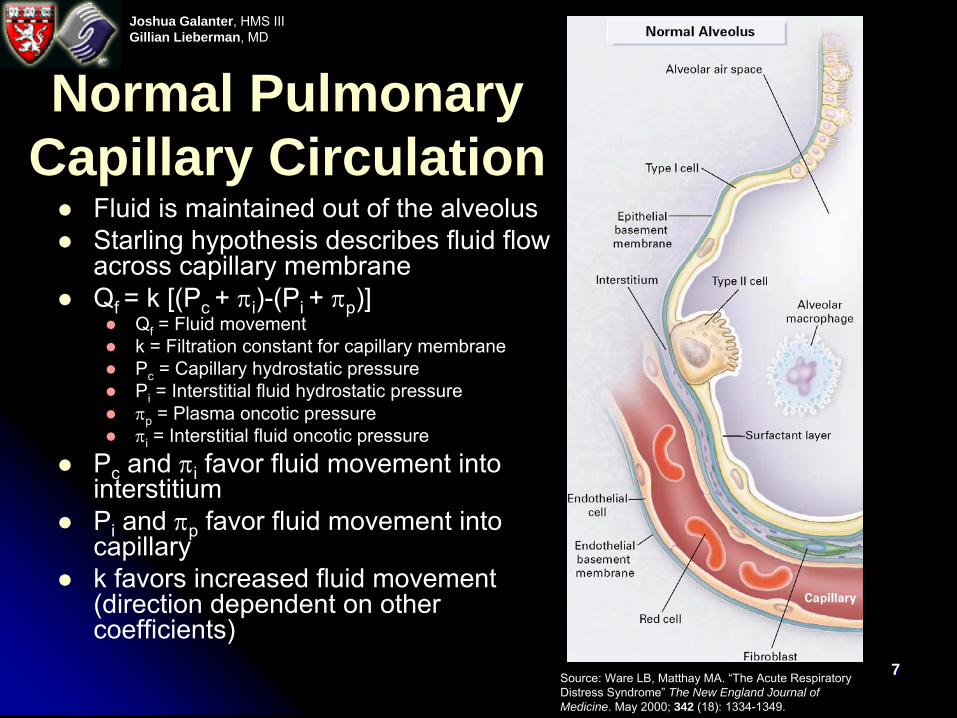
Normal Pulmonary Capillary Circulation
Fluid is maintained out of the alveolusStarling hypothesis describes fluid flow across capillary membraneQf = k [(Pc + πi)-(Pi + πp)]
Qf = Fluid movementk = Filtration constant for capillary membranePc = Capillary hydrostatic pressurePi = Interstitial fluid hydrostatic pressureπp = Plasma oncotic pressureπi = Interstitial fluid oncotic pressure
Pc and πi favor fluid movement into interstitiumPi and πp favor fluid movement into capillaryk favors increased fluid movement (direction dependent on other coefficients)
Source: Ware LB, Matthay
MA. “The Acute Respiratory Distress Syndrome” The New England Journal of Medicine. May 2000; 342 (18): 1334-1349.
88
Joshua Galanter, HMS IIIGillian Lieberman, MD
Causes of ARDSDirect lung injury
PneumoniaAspiration of gastric contentsPulmonary contusionFat embolusNear-drowningInhalational injuryReperfusion pulmonary edema
Indirect lung injurySepsisSevere trauma with shockCardiopulmonary bypassDrug overdoseAcute pancreatitisTransfusion of blood products
99
Joshua Galanter, HMS IIIGillian Lieberman, MD
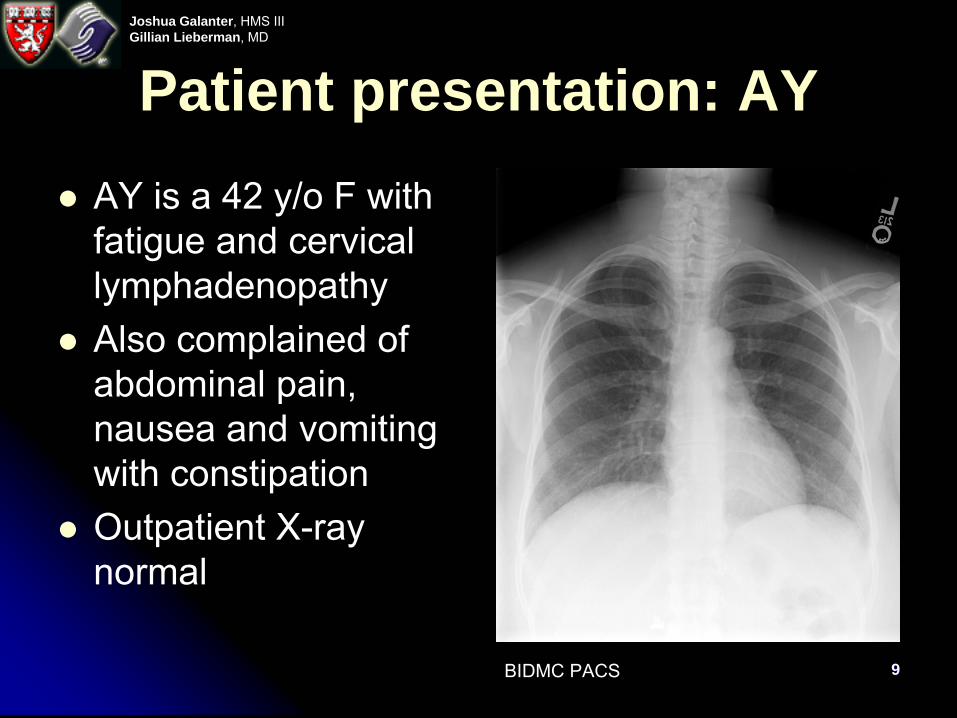
Patient presentation: AYAY is a 42 y/o F with fatigue and cervical lymphadenopathyAlso complained of abdominal pain, nausea and vomiting with constipationOutpatient X-ray normal
BIDMC PACS
1010
Joshua Galanter, HMS IIIGillian Lieberman, MD
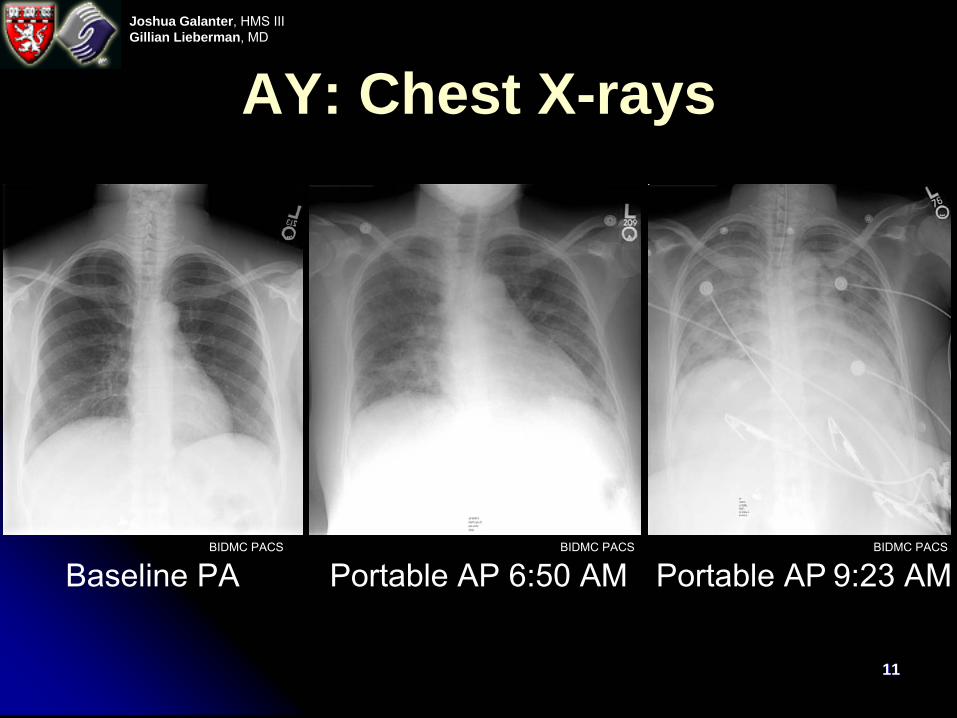
Clinical Course: AYApprox. 3 mo. later, AY presented to the ED with an acute exacerbation of her abdominal pain with radiation to the backIn the interval, she developed fever, night sweats and 45 lb. weight lossCT/MRI revealed extensive lymphadenopathythought to be lymphomaUnderwent an endoscopic biopsyDeveloped acute pancreatitisDeveloped respiratory distress, with resps in the 20’s and O2 sats in the 80’s on a non-rebreather
1111
Joshua Galanter, HMS IIIGillian Lieberman, MD
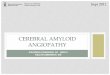
AY: Chest X-rays
Baseline PA Portable AP 6:50 AM Portable AP
9:23 AMBIDMC PACS BIDMC PACSBIDMC PACS
1212
Joshua Galanter, HMS IIIGillian Lieberman, MD
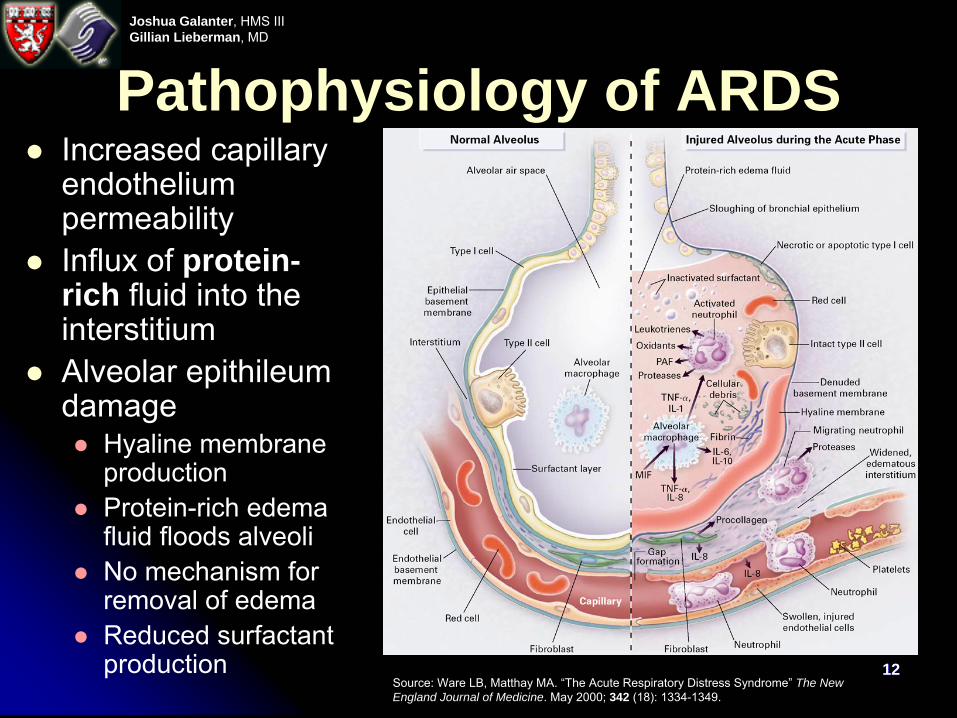
Pathophysiology of ARDSIncreased capillary endothelium permeabilityInflux of protein-rich fluid into the interstitiumAlveolar epithileumdamage
Hyaline membrane productionProtein-rich edema fluid floods alveoliNo mechanism for removal of edemaReduced surfactant production
Source: Ware LB, Matthay
MA. “The Acute Respiratory Distress Syndrome” The New England Journal of Medicine. May 2000; 342 (18): 1334-1349.
1313
Joshua Galanter, HMS IIIGillian Lieberman, MD
Radiographic appearance of ARDSRadiographic latent period
Few or subtle radiographic findingsRapid deterioration: diffuse alveolar pattern pulmonary infiltrateFindings are usually:
Bilateral (92%)Gravity dependent (86%)Worse at the bases (68%)Pleural effusions (50%)
Bilateral (28%)Unilateral (22%)
Air bronchogramsKerley B lines are uncommonOn CT:
Patchy consolidation (42%)Mixed consolidation/ground glass opacification (33%)Homogenous (25%)
1414
Joshua Galanter, HMS IIIGillian Lieberman, MD
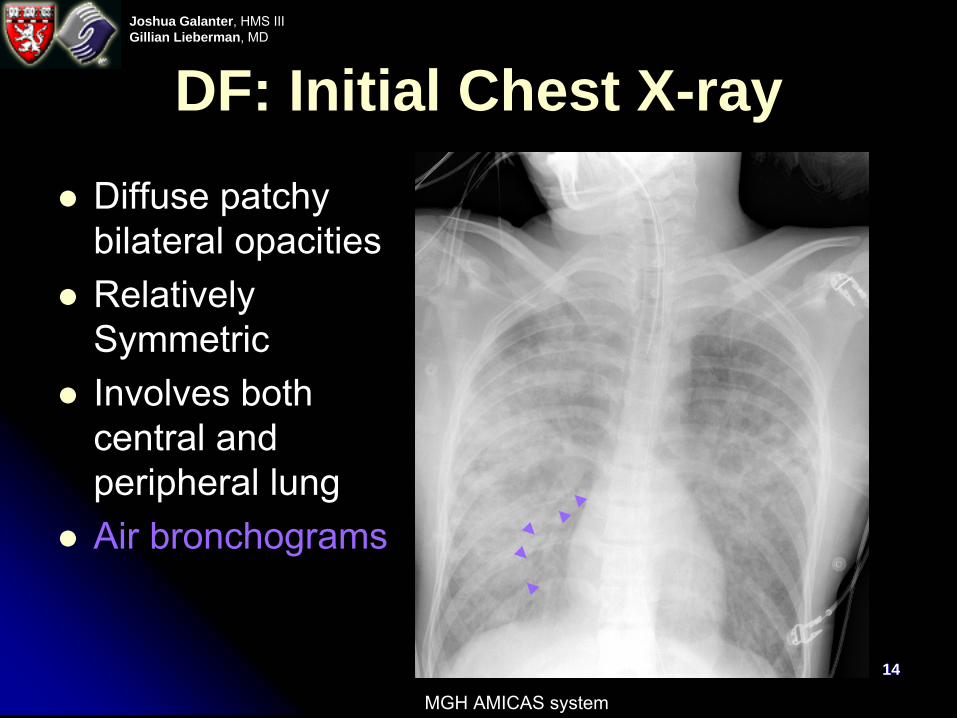
DF: Initial Chest X-rayDiffuse patchy bilateral opacitiesRelatively SymmetricInvolves both central and peripheral lungAir bronchograms
MGH AMICAS system
1515
Joshua Galanter, HMS IIIGillian Lieberman, MD
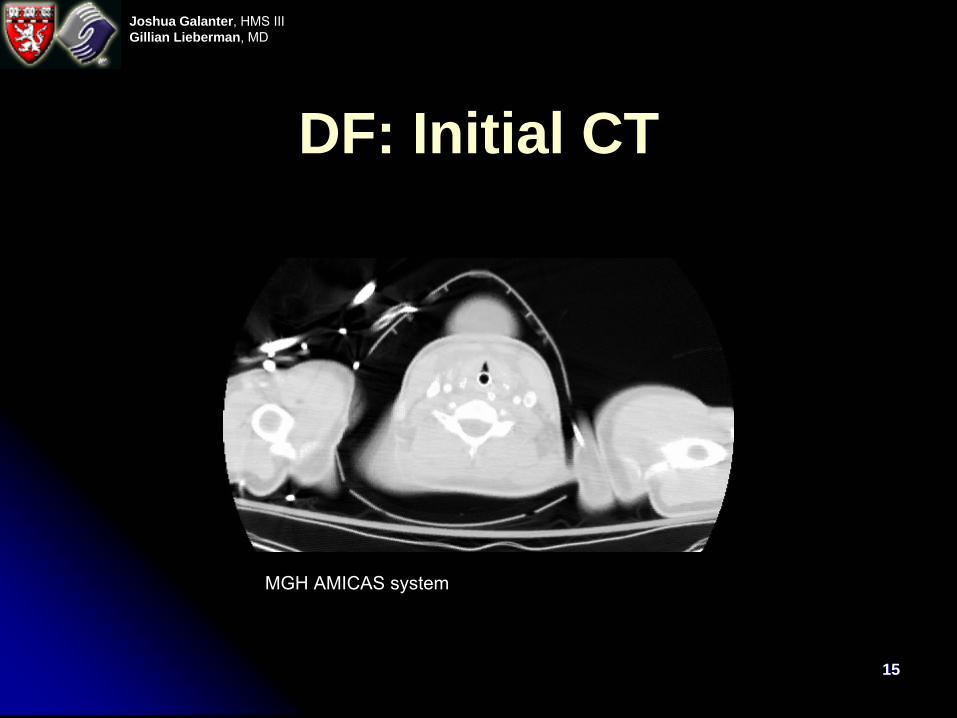
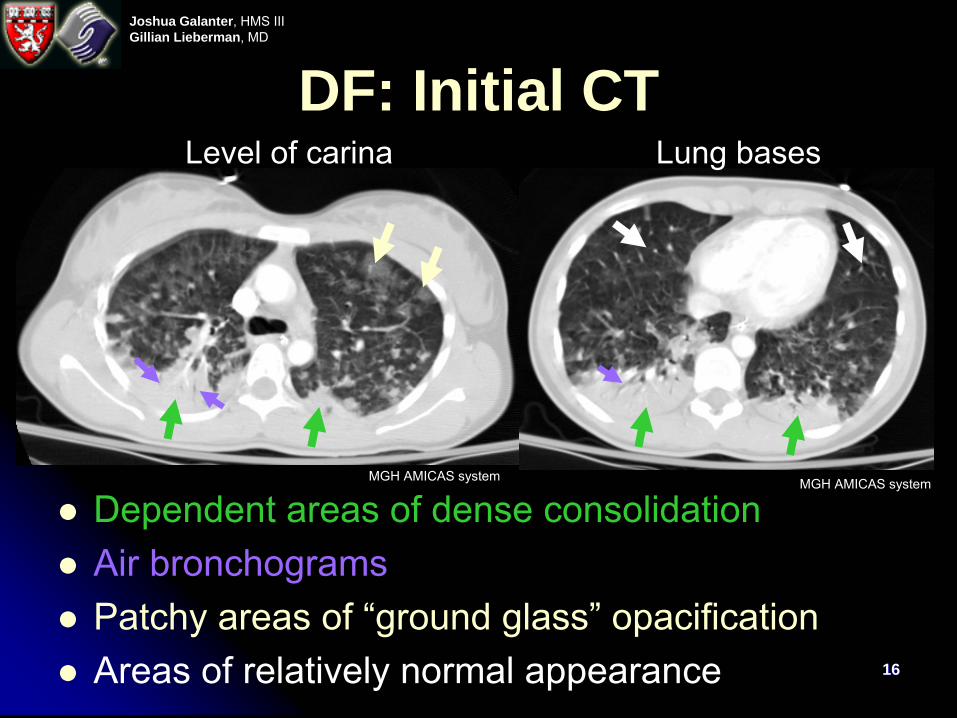
DF: Initial CT
MGH AMICAS system
1616
Joshua Galanter, HMS IIIGillian Lieberman, MD
DF: Initial CT
Dependent areas of dense consolidationAir bronchogramsPatchy areas of “ground glass” opacificationAreas of relatively normal appearance
Level of carina Lung bases
MGH AMICAS system MGH AMICAS system
1717
Joshua Galanter, HMS IIIGillian Lieberman, MD
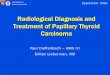
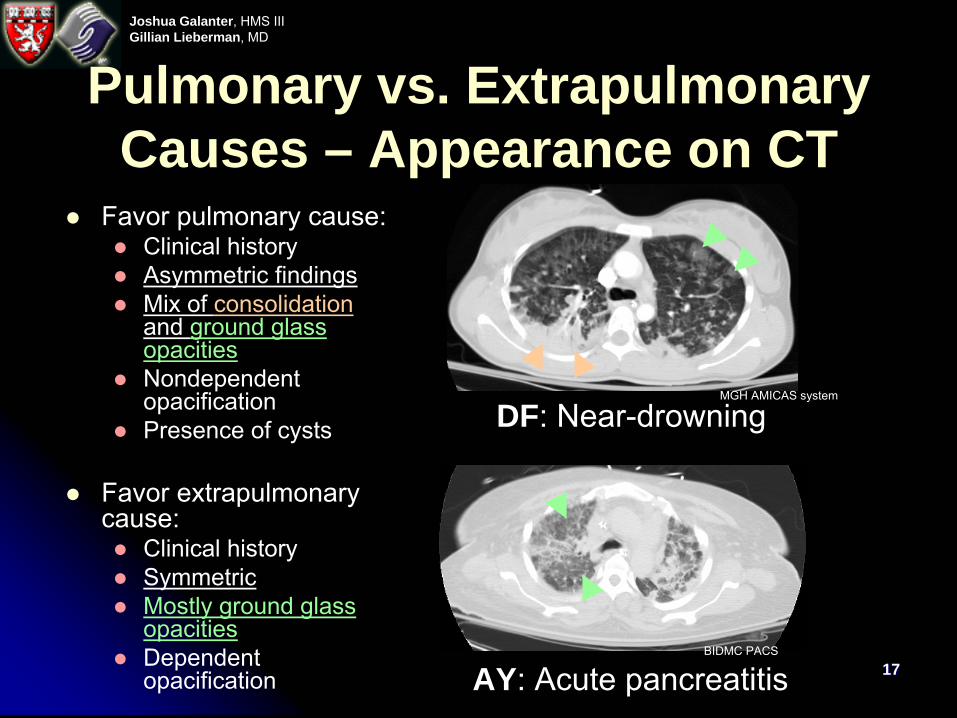
Pulmonary vs. Extrapulmonary Causes – Appearance on CT
Favor pulmonary cause:Clinical historyAsymmetric findingsMix of consolidationand ground glass opacitiesNondependent opacificationPresence of cysts
Favor extrapulmonarycause:
Clinical historySymmetricMostly ground glass opacitiesDependent opacification
DF: Near-drowning
AY: Acute pancreatitisBIDMC PACS
MGH AMICAS system
1818
Joshua Galanter, HMS IIIGillian Lieberman, MD
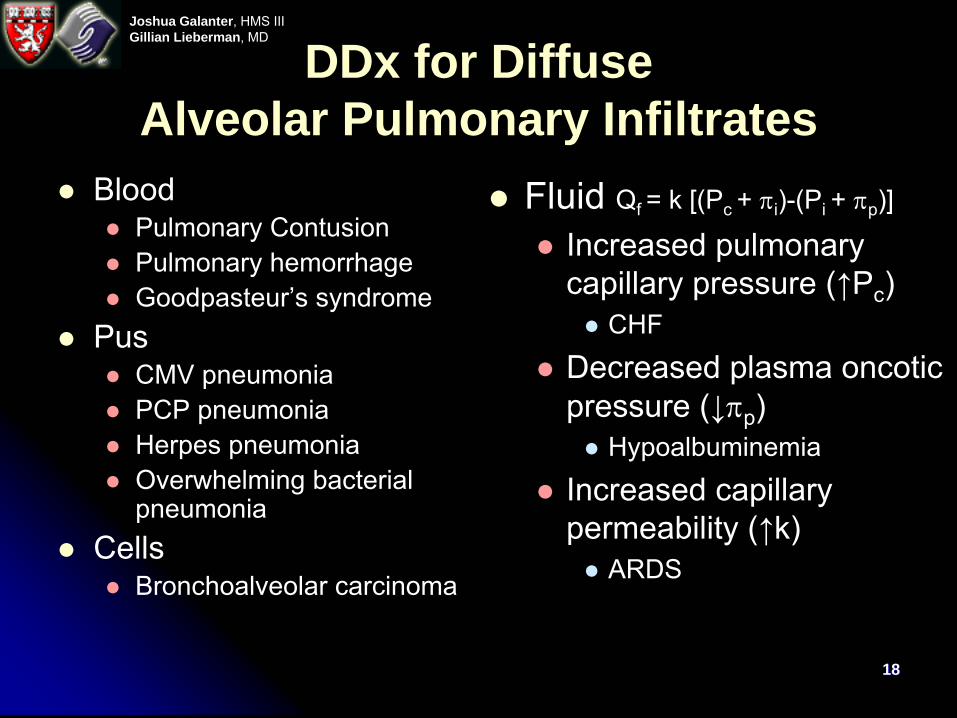
DDx for Diffuse Alveolar Pulmonary Infiltrates
BloodPulmonary ContusionPulmonary hemorrhageGoodpasteur’s syndrome
PusCMV pneumoniaPCP pneumoniaHerpes pneumoniaOverwhelming bacterial pneumonia
CellsBronchoalveolar carcinoma
Fluid Qf = k [(Pc + πi)-(Pi + πp)]
Increased pulmonary capillary pressure (↑Pc)
CHF
Decreased plasma oncoticpressure (↓πp)
Hypoalbuminemia
Increased capillary permeability (↑k)
ARDS
1919
Joshua Galanter, HMS IIIGillian Lieberman, MD
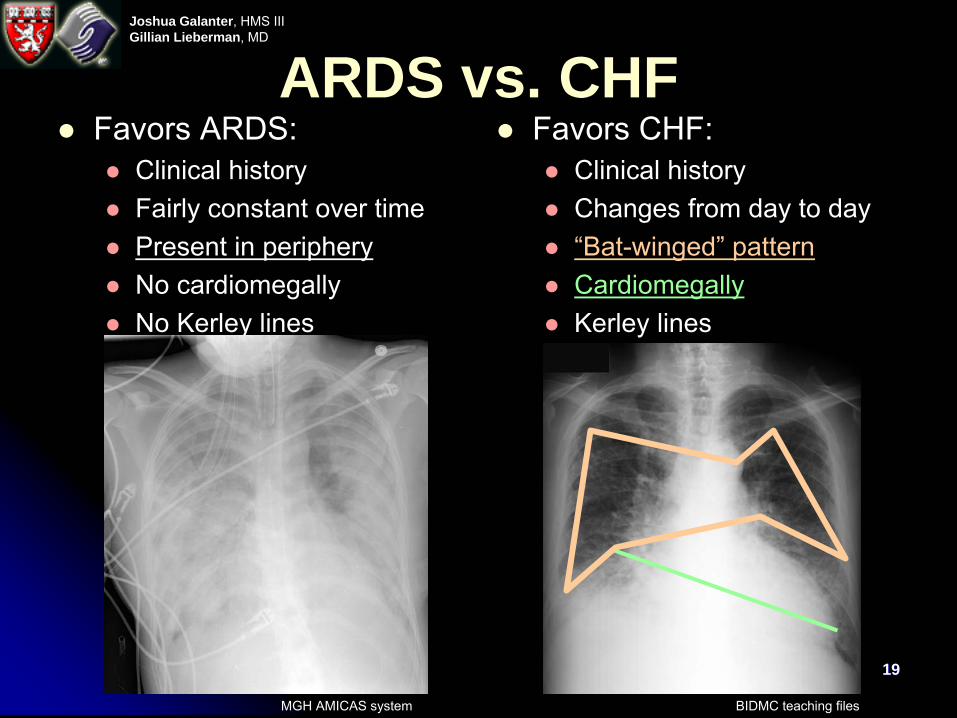
ARDS vs. CHFFavors ARDS:
Clinical historyFairly constant over timePresent in peripheryNo cardiomegallyNo Kerley lines
Favors CHF:Clinical historyChanges from day to day“Bat-winged” patternCardiomegallyKerley lines
MGH AMICAS system BIDMC teaching files
2020
Joshua Galanter, HMS IIIGillian Lieberman, MD
Sequelae of ARDSLines and tubesPneumothorax from barotraumaPneumomediastinum from barotraumaSubcutaneous emphysema from barotraumaPleural effusionAtelectasis and collapse from malpositioned ET tubeNosocomial pneumoniaPulmonary fibrosis
2121
Joshua Galanter, HMS IIIGillian Lieberman, MD
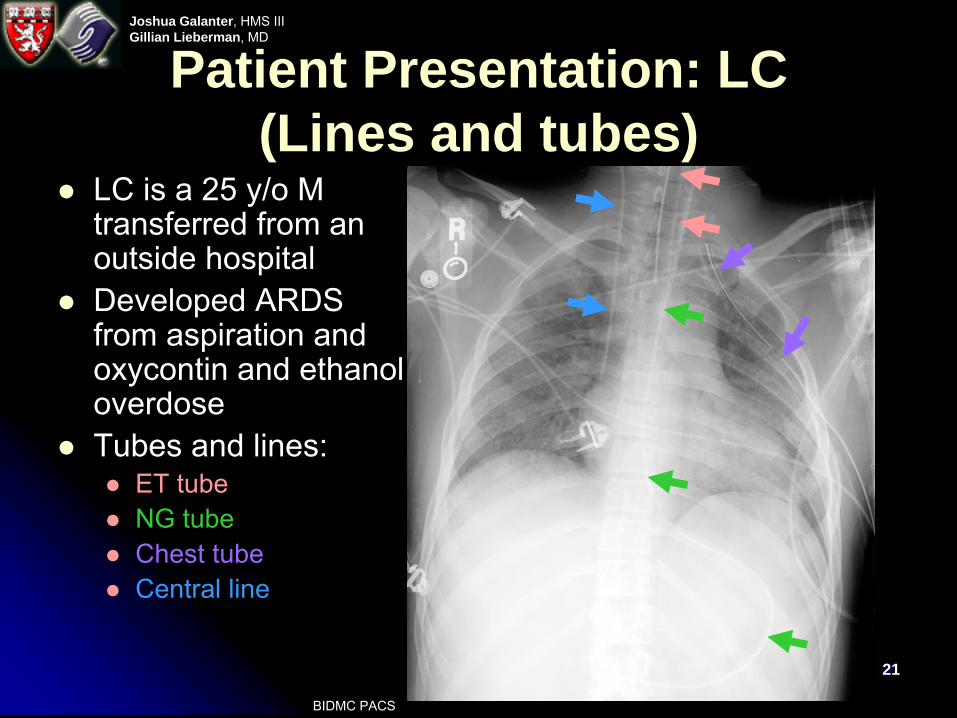
Patient Presentation: LC (Lines and tubes)
LC is a 25 y/o M transferred from an outside hospitalDeveloped ARDS from aspiration and oxycontin and ethanol overdoseTubes and lines:
ET tubeNG tubeChest tubeCentral line
BIDMC PACS
2222
Joshua Galanter, HMS IIIGillian Lieberman, MD
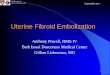
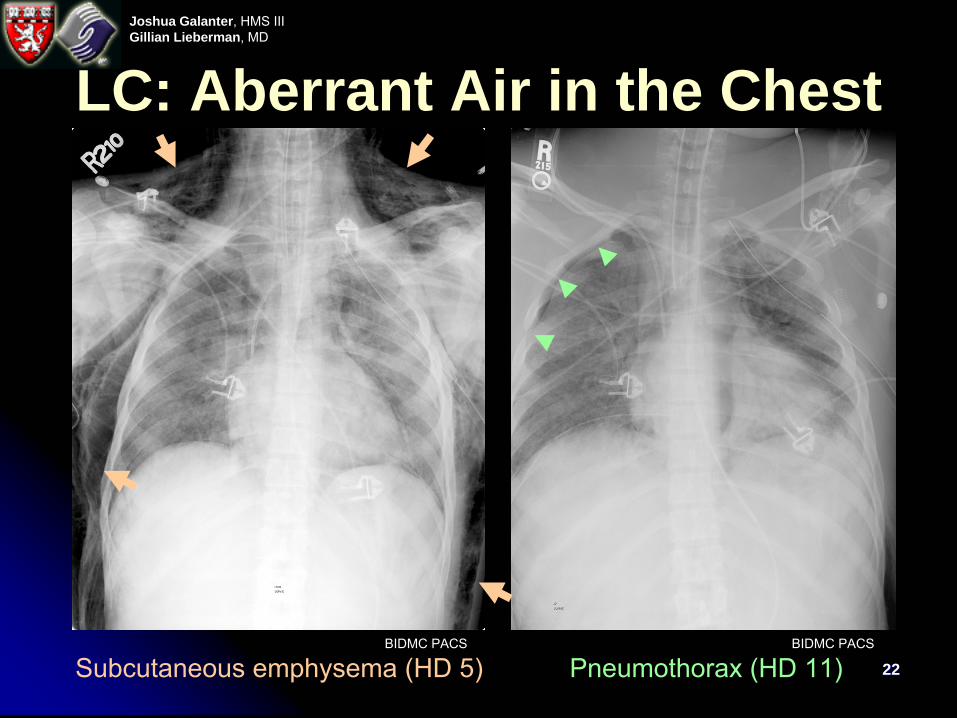
LC: Aberrant Air in the Chest
Subcutaneous emphysema (HD 5) Pneumothorax
(HD 11)BIDMC PACS BIDMC PACS
2323
Joshua Galanter, HMS IIIGillian Lieberman, MD
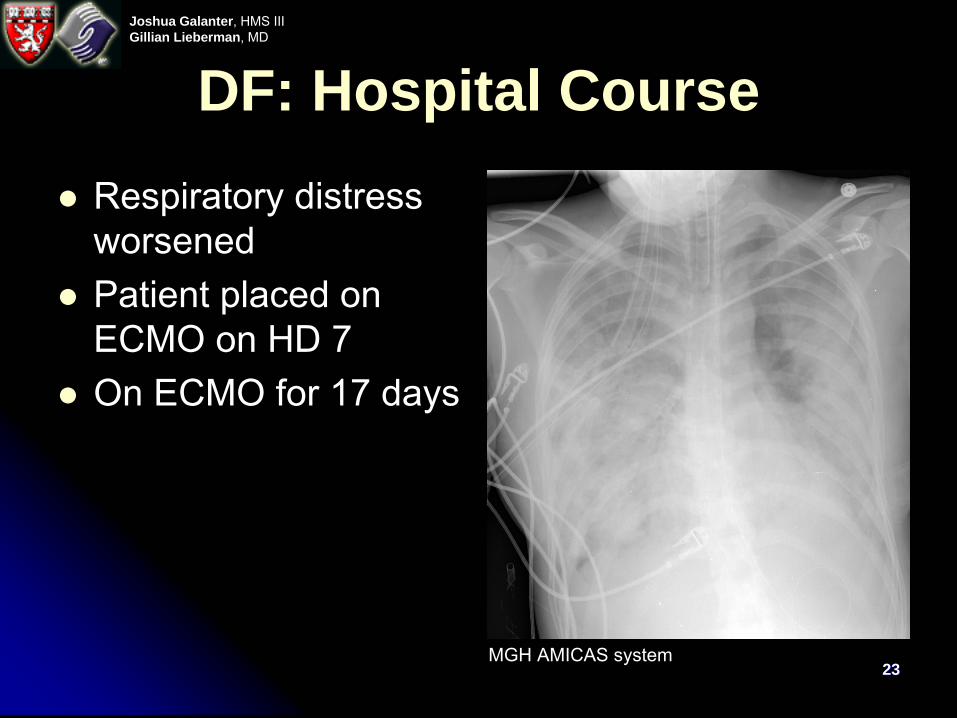
DF: Hospital CourseRespiratory distress worsenedPatient placed on ECMO on HD 7On ECMO for 17 days
MGH AMICAS system
2424
Joshua Galanter, HMS IIIGillian Lieberman, MD
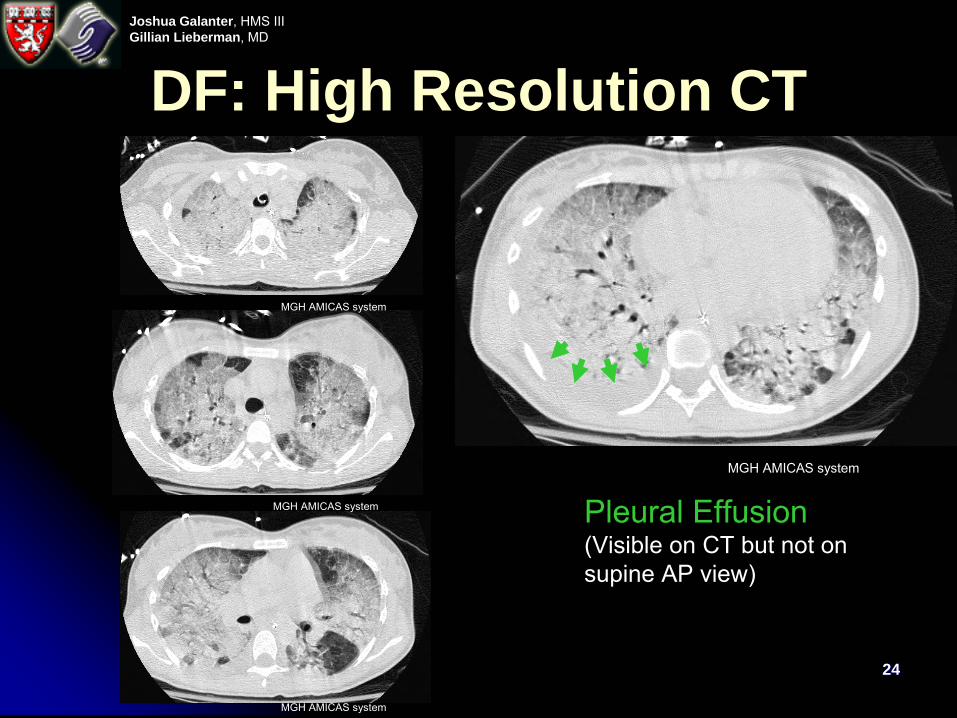
DF: High Resolution CT
Pleural Effusion(Visible on CT but not on supine AP view)
MGH AMICAS system
MGH AMICAS system
MGH AMICAS system
MGH AMICAS system
2525
Joshua Galanter, HMS IIIGillian Lieberman, MD
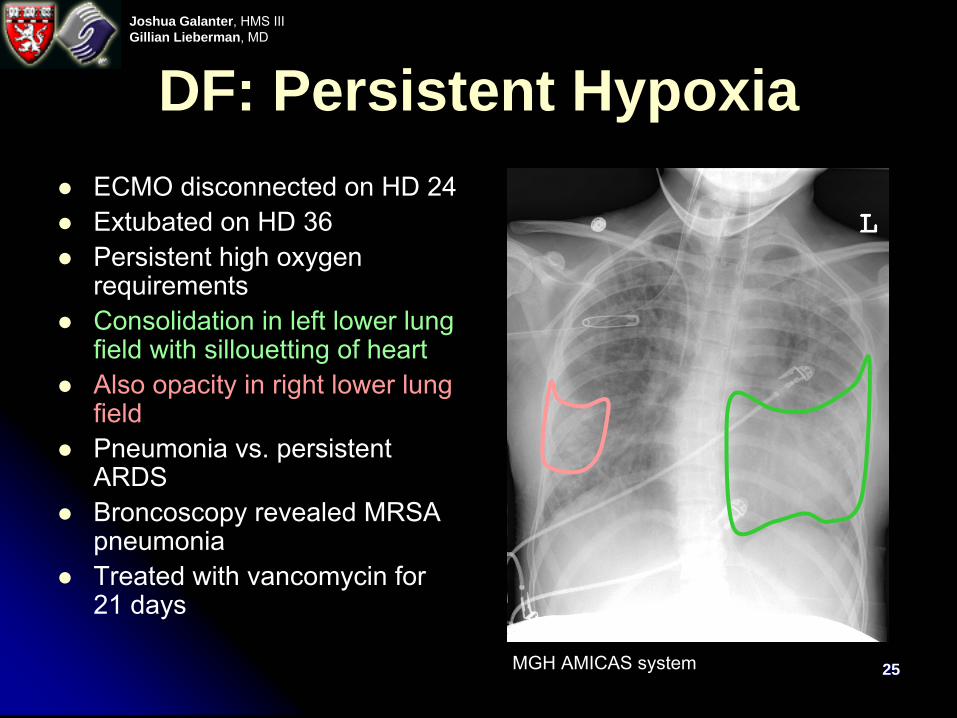
DF: Persistent Hypoxia ECMO disconnected on HD 24Extubated on HD 36Persistent high oxygen requirementsConsolidation in left lower lung field with sillouetting of heartAlso opacity in right lower lung fieldPneumonia vs. persistent ARDSBroncoscopy revealed MRSA pneumoniaTreated with vancomycin for 21 days
MGH AMICAS system
2626
Joshua Galanter, HMS IIIGillian Lieberman, MD
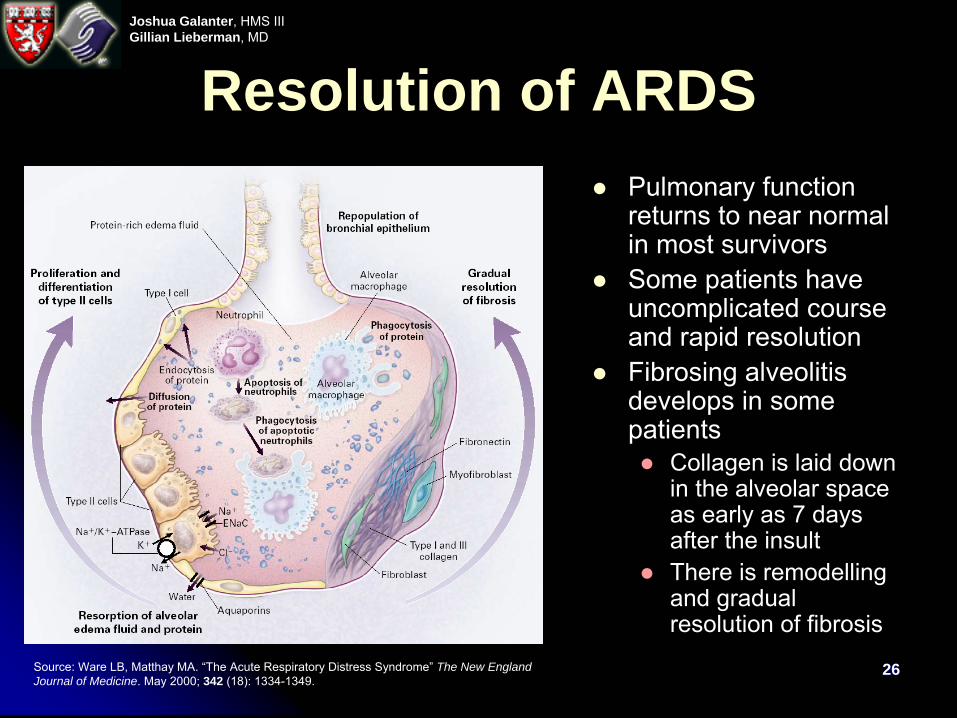
Resolution of ARDSPulmonary function returns to near normal in most survivorsSome patients have uncomplicated course and rapid resolutionFibrosing alveolitisdevelops in some patients
Collagen is laid down in the alveolar space as early as 7 days after the insultThere is remodellingand gradual resolution of fibrosis
Source: Ware LB, Matthay
MA. “The Acute Respiratory Distress Syndrome” The New England Journal of Medicine. May 2000; 342 (18): 1334-1349.
2727
Joshua Galanter, HMS IIIGillian Lieberman, MD
DF: ConclusionDF was discharged on hospital day 52Her O2 saturation at discharge was 100% at room air
On her presentation at Grand Rounds two months later, she reported some exhertionaldyspnea but no other long-term symptomsReturned to work as an administrative assistant
2828
Joshua Galanter, HMS IIIGillian Lieberman, MD
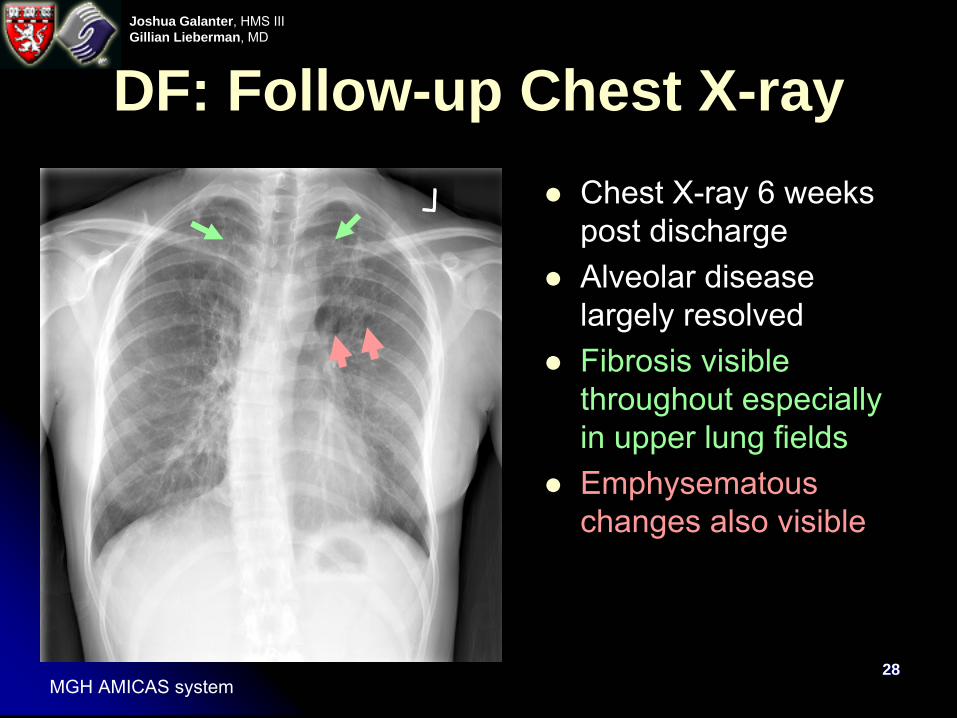
DF: Follow-up Chest X-rayChest X-ray 6 weeks post dischargeAlveolar disease largely resolvedFibrosis visible throughout especially in upper lung fieldsEmphysematous changes also visible
MGH AMICAS system
2929
Joshua Galanter, HMS IIIGillian Lieberman, MD
Summary
Normal pulmonary fluid balance dictated by the Starling hypothesisIn ARDS, a pulmonary or extrapulmonaryinsult results in a breakdown of capillary endothelium and alveolar epitheliumThere is an influx of protein rich edema fluid into the alveolusHypoxia and respiratory distress result
3030
Joshua Galanter, HMS IIIGillian Lieberman, MD
SummaryRadiographically ARDS typically presents with a bilateral, diffuse, symmetric alveolar pattern with air bronchograms, worse at the bases (initially)On CT, patchy consolidation and/or ground glass opacifications is seen; a homogenous appearance is suggestive of an extrapulmonary etiologyThe DDx is large, and includes blood, pus, cells, and fluidComplications of ARDS visible on chest X-ray include:
Pleural effusionAtelectasis and collapsePneumothorax, pneumomediastinum, and subcutaneous emphysemaPneumoniaPulmonary fibrosis
3131
Joshua Galanter, HMS IIIGillian Lieberman, MD
ReferencesBernard GR, Artigas A, Brigham KL, et al. “The American-European Consensus Conference of ARDS”. Am J Respir Crit Care Med. 1994; 149: 818-824.Desai SR, Wells AU, Suntharalingam G, Rubens MB, Evans TW, Hansell DM. “Acute Respiratory Distress Syndrome Caused by Pulmonary and Extrapulmonary Injury: a Comparative CT Study.” Radiology Mar 2001; 218 (3): 689-93.Goodman LR. “Congestive Heart Failure and Adult Respiratory Distress Syndrome: New Insights Using Computed Tomography” The Radiologic Clinics of North America Jan 1996; 34 (1): 33-46.Goodman LR, Fumagalli R, Tagliabue P, Tagliabue M, Ferrario M, Gattinoni L, Pesenti A. “Adult Respiratory Distress Syndrome Due to Pulmonary and Extrapulmonary Causes: CT, Clinical, and Functional Correlations”. Radiology Nov 1999; 213 (2): 545-52.Goodman PC “Radiographic Findings in Patients with Acute Respiratory Distress Syndrome”. Clinics in Chest Medicine Sept 2000; 21 (3)Greene R, Janisca H, Boggis C, Straups W, Lowenstein E. “Respiratory Distress Syndrome with New Considerations” The Radiologic Clinics of North America Dec 1983; 21 (4): 699-708.Kollef MH, Schuster DP. “The Acute Respiratory Distress Syndrome” The New England Journal of Medicine. Jan 1995; 332 (1): 27-36.Miller WT Sr. “The Chest Radiograph in the Intensive Care Unit” Seminars in Roentgenology.Apr 1997; 32 (2): 89-101.Novelline RA. Squire’s Fundamentals of Radiology Fourth Edition. Harvard University Press, Cambridge, MA 1997.Ware LB, Matthay MA. “The Acute Respiratory Distress Syndrome” The New England Journal of Medicine. May 2000; 342 (18): 1334-1349.Weinberger SE. Principles of Pulmonary Medicine Third Edition. W. B. Saunders Company, Philadelphia, 1998.
3232
Joshua Galanter, HMS IIIGillian Lieberman, MD
AcknowledgementsChristopher Taylor, MDPhillip Boiselle, MDDavid Sher, HMS IIILarry Barbaras and Cara Lyn D’amour, our WebmastersGillian Lieberman, MD Pamela Lepkowski
3333
Joshua Galanter, HMS IIIGillian Lieberman, MD
Thank youHMS Core radiology clerkship, April/May 2002