Embed Size (px)
Citation preview

RADY 403: Ewing Sarcoma

11-year-old with unremarkable past medical history, family history
Presented to pediatrician after one month of right leg pain in lower leg/calf▪ Dull, achy, non-radiating pain
▪ No history of trauma, although is active
▪ No erythema, swelling, gait issues
▪ Afebrile, no overlying skin abrasions or lesions
Diagnosed as muscle strain
Pain continued to worsen▪ Developed new limp with noticeable swelling in right lower leg
▪ Minimally responsive to Tylenol

Local radiographs were performed, in line with the ACR Appropriateness Criteria.

Frontal and lateral radiographs of right tibia and fibula
CT-guided biopsy
MRI of right fibula
CT chest
PET CT

Ill-defined, expansile, lytic lesion of the mid fibula with a moth-eaten appearance and Codman’s triangle
Codman’s Triangle
Medullary involvement and possible soft tissue component

Bony spicules extending horizontally
Tibia, distal femur appear uninvolved
Knee and ankle joints are unremarkable
Poorly defined, expansile, lytic lesion

Lateral approach to the lesion for FNA (x2) and Core Needle Biopsy (x2)
Hair-on-end periosteal reaction


Coronal STIRSagittal T1WI
There is a heterogeneous T2 hyperintense, T1 isointense, enhancing lesion in the diaphysis of the mid fibula.
Axial T2WI
Abnormal signal intensity and enhancement in the tibialis posterior, flexor hallucis longus, peroneus longus/brevis with disruption of the interosseous membrane.

3 mm LUL ground glass opacity, likely atelectasis

No distant sites of abnormal uptake to suggest distant metastases
Right fibula metadiaphyseal osseous lesion with aggressive periosteal reaction and localized muscle invasion
Avid FDG uptake in the tibialis posterior, flexor hallucis longus, peroneus longus and brevis

Second most common primary pediatric bone tumor (osteosarcoma)▪ 3% of all pediatric tumors
Generally occurs in second decade of life (mean age of 11 years)▪ Males > females
Aggressive, small, round, blue-cell tumor
Genetics
▪ Arise from a precursor cell capable of neuroectodermal differentiation
▪ 11;22 translocation
▪ PAS+ and CD99+
Histology slide showing sheets of small, round, uniform cellswith scant clear cytoplasm, divided intoirregular lobules by fibrous strands
Courtesy of https://www.pathologyoutlines.com/topic/boneewing.html
Courtesy of https://www.talkbasket.net/85740-patrick-ewing-michael-jordan-still-trash-talks-me-to-this-day

Most common locations: femur > ilium > tibia > humerus > fibula > ribs > sacrum
▪ Can develop in any bone, although long bones most common
▪ Soft tissue involvement is more common in older patients
Presentation
▪ Pain and swelling of the affected limb
▪ Local findings (warmth and tenderness)
▪ Can present with constitutional signs and symptoms (fever, elevated erythrocyte sedimentation rate, leukocytosis, weight loss)
▪ 10-20% of patients
▪ Associated with advanced disease
20-30% of patients have metastasis at time of presentation
▪ Lung in 50%, bone in 25% and bone marrow in 20%
Differential diagnosis: Osteosarcoma, lymphoma, infection, eosinophilic granuloma
Case courtesy of Dr Hani Makky Al Salam, Radiopaedia.org, rID: 7876

Distribution in the long and flat bones
Centered in the medullary cavity
”Moth-eaten" appearance
Lytic lesions with poorly defined margins and permeative pattern
▪ Can appear predominantly sclerotic in 15% of cases
▪ Bone necrosis can appear radiodense
”Onion skin" periosteum (non-specific)
▪ Extrudes through Haversian Canals, elevating the periosteum in a lamellated fashion
Large soft-tissue component with little calcification
▪ Especially in older patients
▪ Difficult to appreciate on plain radiography
Courtesy of https://radiologyassistant.nl/musculoskeletal/bone-tumors/osteolytic-ill-defined#ewings-sarcoma

Case courtesy of Assoc Prof Frank Gaillard, Radiopaedia.org, rID: 7844
Onion-skinning of periosteum
Long bone distribution
Medullaryinvolvement
Lytic lesions with poorly defined margins and a permeative pattern. They are often located in the diaphysis and metadiaphysis.
Moth eaten appearance

Case courtesy of Dr Benoudina Samir, Radiopaedia.org, rID: 84751
Onion-skinning of periosteum
Lytic lesions with poorly defined margins and a permeative pattern. They are often located in the diaphysis and metadiaphysis.
Moth eaten appearance
Courtesy of https://pediatricimaging.org/diseases/ewing-sarcoma/

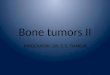
MRI
▪ Demonstrates extent of primary osseous lesion and soft tissue, bone marrow involvement
▪ Informs the therapeutic approach
▪ T1WI: homogenous, intermediate signal intensity
▪ T2WI: homogenous, low-intermediate signal intensity
▪ High signal intensity predominates in 32% of Ewing sarcomas of bone on T2-weighted images
▪ Contrast enhancement is usually seen, and is usually either diffuse or peripheral nodular in pattern
CT
▪ Chest CT often performed for detection of metastatic disease
▪ Similar appearance of radiography, with aggressive bone destruction and a large associated soft-tissue mass
FDG PET/PET-CT
▪ Demonstrate extent of disease and evaluate treatment response
▪ Up to 100% sensitivity for detecting sites of disease at staging and recurrence▪ Specificity 81%, accuracy 96%
Axial T1WI with heterogeneously intermediate signal intensity
Lesion centered in marrow canal (M) with soft tissue extension (S)
Axial contrast enhanced T1WI with diffuse contrast enhancement
Axial T2WI with intermediate intensity
White arrowheads demonstrate cortical involvement as intermediate-intensity channels extending through low-signal-intensity cortex.

5-year survival is 70% for localized disease and 30% for metastatic disease
▪ Historically, even in localized lesions with adequate tumor resection, 5-year survival was only 10%
▪ Began to assume that all patients with Ewing Sarcoma have micrometastases and treat as such
The most favorable prognostic factors at the time of initial diagnosis are tumor responsiveness to preoperative chemotherapy, and the presence of the most common type of Ewing sarcoma fusion transcript (EWS-FLI1)
Adverse prognostic indicators at the time of initial diagnosis include:
▪ Metastatic disease
▪ Eight year survival rate of 30%
▪ Flat bone involvement (pelvis)
▪ Large tumor size (>8 cm)
▪ Older patient age (>15 years) at presentation
▪ Elevated LDH
▪ Poor tumor response to preoperative chemotherapy
Case courtesy of Dr Mahmoud Yacout Alabd, Radiopaedia.org, rID: 41035

Multidisciplinary management is key▪ Multi-drug induction chemotherapy
▪ 4-8 cycles
▪ Local treatment of primary tumor▪ Surgery, radiotherapy, or both
▪ Goal of surgery: wide surgical margin with attempt at limb salvage
▪ Limb reconstruction with bone allograft or metallic implant; joint prosthesis if epiphysis is involved in resection
▪ Consolidation chemotherapy
Favorable findings on follow up radiographs:▪ Maturation of periosteal reaction
▪ Coarsening of the bone trabeculae
▪ Reconstitution of the cortex
▪ Increasing osseous sclerosis and progressive mineralization
▪ Decrease in the size of the soft-tissue component of the lesionCourtesy of https://pediatricimaging.org/diseases/ewing-sarcoma/

32 months s/p completion of therapy
Followed up every three months with leg and chest radiographs and leg MRI▪ Post-treatment imaging is important
No evidence of recurrence
Doing well clinically
Surgical clip
Surgical clip
Dystrophic calcification
Dystrophic calcification

More common in males
At radiography, Ewing sarcoma of bone reveals aggressive features, reflecting its high-grade nature
Initial imaging of choice is plain radiograph of area of interest▪ Moth-eaten lytic lesion in long bones
▪ Diaphyseal/metadiaphyseal involvement
▪ “Onion-skin” appearance
30% metastatic at presentation with significantly worse outcomes
▪ Commonly metastasizes to lungs and bone marrow
▪ Assess with chest CT and PET scan
Management includes chemo, then surgery/radiation, then consolidation chemo

ACR Appropriateness Criteria. (2021). Retrieved June 11, 2021, from https://www.acr.org/Clinical-Resources/ACR-Appropriateness-Criteria
Clinical presentation, staging, and prognostic factors of the Ewing sarcoma family of tumors – UpToDate. Accessed June 11, 2021. https://www.uptodate.com/contents/clinical-presentation-staging-and-prognostic-factors-of-the-ewing-sarcoma-family-of-tumors?search=ewing%20sarcoma&source=search_result&selectedTitle=1~95&usage_type=default&display_rank=1#H4
Saeter G, European Society for Medical Oncology. ESMO Minimum Clinical Recommendations for diagnosis, treatment and follow-up of Ewing’s sarcoma of bone. Ann Oncol. 2003;14(8):1167-1168. doi:10.1093/annonc/mdg335
Ewing Sarcoma | Pediatric Radiology Reference Article | PediatricImaging.org | @pedsimaging. Pediatric Imaging. Published November 16, 2019. Accessed June 12, 2021. https://pediatricimaging.org/diseases/ewing-sarcoma/
Gaillard F. Ewing sarcoma | Radiology Reference Article | Radiopaedia.org. Radiopaedia. Accessed June 11, 2021. https://radiopaedia.org/articles/ewing-sarcoma?lang=us
Charest M, Hickeson M, Lisbona R, Novales-Diaz J-A, Derbekyan V, Turcotte RE. FDG PET/CT imaging in primary osseous and soft tissue sarcomas: a retrospective review of 212 cases. Eur J Nucl Med Mol Imaging. 2009;36(12):1944-1951. doi:10.1007/s00259-009-1203-0
Meyer JS, Nadel HR, Marina N, et al. Imaging guidelines for children with Ewing sarcoma and osteosarcoma: a report from the Children’s Oncology Group Bone Tumor Committee. Pediatr Blood Cancer. 2008;51(2):163-170. doi:10.1002/pbc.21596
Imaging guidelines for children with Ewing sarcoma and osteosarcoma: a report from the Children’s Oncology Group Bone Tumor Committee. - Google Search. Accessed June 11, 2021. https://www.google.com/search?q=Imaging+guidelines+for+children+with+Ewing+sarcoma+and+osteosarcoma%3A+a+report+from+the+Children%27s+Oncology+Group+Bone+Tumor+Committee.&oq=Imaging+guidelines+for+children+with+Ewing+sarcoma+and+osteosarcoma%3A+a+report+from+the+Children%27s+Oncology+Group+Bone+Tumor+Committee.&aqs=chrome..69i57.253j0j7&sourceid=chrome&ie=UTF-8
Jaramillo D, Laor T, Gebhardt MC. Pediatric musculoskeletal neoplasms. Evaluation with MR imaging. Magn Reson Imaging Clin N Am. 1996;4(4):749-770.
Pediatric Radiology. Accessed June 15, 2021. https://www.med-ed.virginia.edu/courses/rad/peds/ms_webpages/ms6eewing.html
Bacci G, Ferrari S, Bertoni F, et al. Prognostic factors in nonmetastatic Ewing’s sarcoma of bone treated with adjuvant chemotherapy: analysis of 359 patients at the Istituto Ortopedico Rizzoli. J Clin Oncol. 2000;18(1):4-11. doi:10.1200/JCO.2000.18.1.4
Jain N, Sah M, Chakraverty J, Evans A, Kamath S. Radiological approach to a child with hip pain. Clinical Radiology. 2013;68(11):1167-1178. doi:10.1016/j.crad.2013.06.016
Jain et al. - 2013 - Radiological approach to a child with hip pain.pdf. Accessed June 12, 2021. https://msrads.web.unc.edu/wp-content/uploads/sites/15695/2018/04/Child-with-a-Limp-Clinical-Rad-2013.pdf
The Radiology Assistant : Osteolytic - ill defined. Accessed June 11, 2021. https://radiologyassistant.nl/musculoskeletal/bone-tumors/osteolytic-ill-defined#ewings-sarcoma
Mar WA, Taljanovic MS, Bagatell R, et al. Update on imaging and treatment of Ewing sarcoma family tumors: what the radiologist needs to know. J Comput Assist Tomogr. 2008;32(1):108-118. doi:10.1097/RCT.0b013e31805c030f
Murphey MD, Senchak LT, Mambalam PK, Logie CI, Klassen-Fischer MK, Kransdorf MJ. From the Radiologic Pathology Archives: Ewing Sarcoma Family of Tumors: Radiologic-Pathologic Correlation. RadioGraphics. 2013;33(3):803-831. doi:10.1148/rg.333135005